
Multiparametric Dual-Time-Point [18F]FDG PET/MRI for Lymph Node Staging in Patients with Untreated FIGO I/II Cervical Carcinoma

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. PET/MRI Protocol
2.2. SLN SPECT/CT
2.3. Histological Validation
2.4. Image Evaluation and Data Quantification
2.5. Statistical Analysis
3. Results
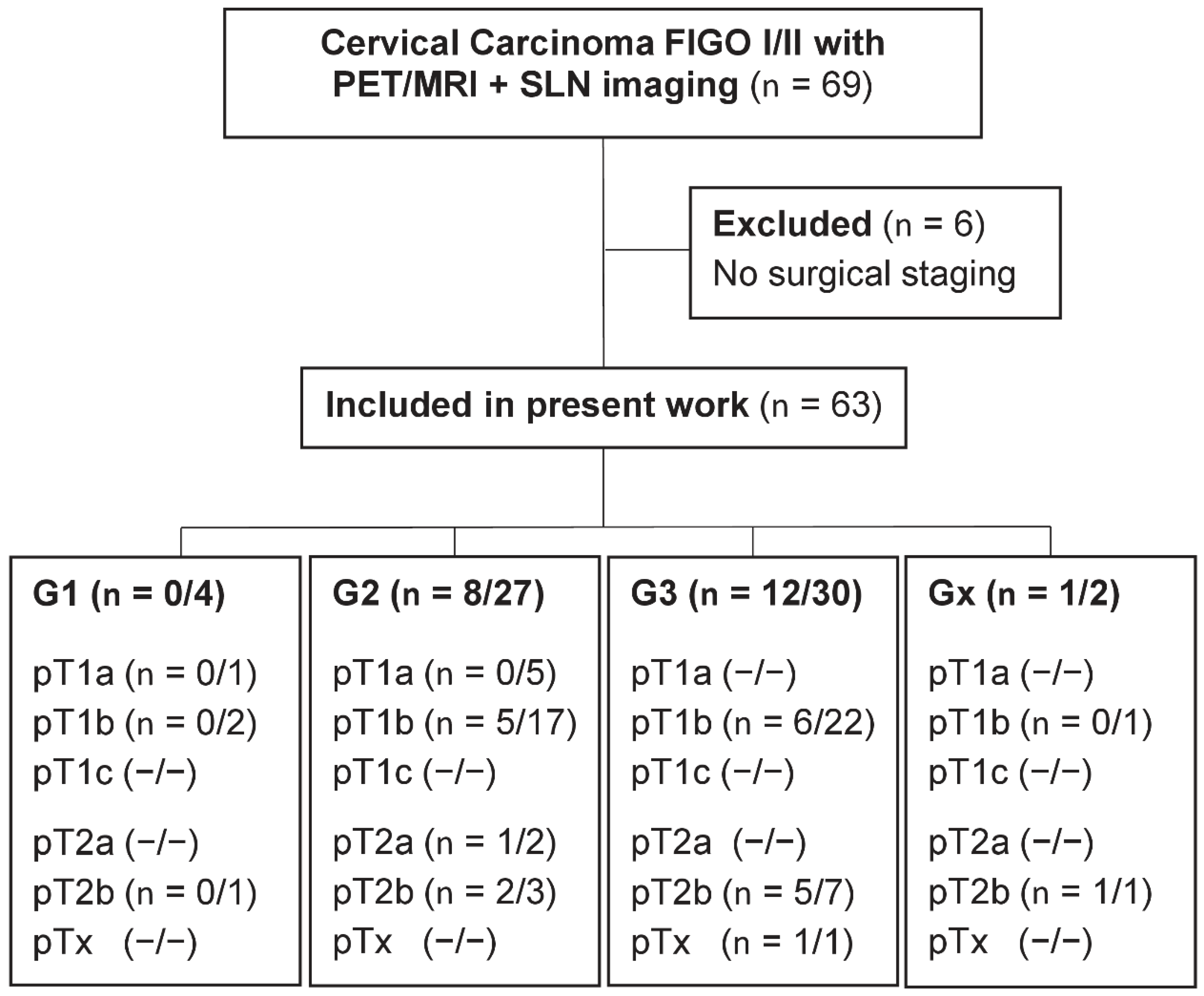
3.1. Patient Cohort
3.2. Prevalence of LNM Dependent on Stage and Grade of Primary Tumors
3.3. Interrelationships of Histology and PET/MRI Parameters
3.4. PET/MRI Parameter Evaluation
3.5. Multiparametric Approach
3.6. Additional Value of Dual-Time-Point [18F]FDG Kinetic
3.7. Visual vs. Multiparametric Evaluation
4. Discussion
4.1. Impact of Tumor Grade
4.2. Dual-Time-Point [18F]FDG PET
4.3. Experts vs. Malignancy Score
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arbyn, M.; Weiderpass, E.; Bruni, L.; de Sanjose, S.; Saraiya, M.; Ferlay, J.; Bray, F. Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob. Health 2020, 8, e191–e203. [Google Scholar] [CrossRef]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): S3-Leitlinie Diagnostik, Therapie und Nachsorge der Patientin mit Zervixkarzinom, Langversion, 2.2, 2022, AWMF-Registernummer: 032/033OL. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/zervixkarzinom/ (accessed on 15 August 2022).
- Marchiole, P.; Buenerd, A.; Benchaib, M.; Nezhat, K.; Dargent, D.; Mathevet, P. Clinical significance of lympho vascular space involvement and lymph node micrometastases in early-stage cervical cancer: A retrospective case-control surgico-pathological study. Gynecol. Oncol. 2005, 97, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Bats, A.S.; Mathevet, P.; Buenerd, A.; Orliaguet, I.; Mery, E.; Zerdoud, S.; Le Frere-Belda, M.A.; Froissart, M.; Querleu, D.; Martinez, A.; et al. The sentinel node technique detects unexpected drainage pathways and allows nodal ultrastaging in early cervical cancer: Insights from the multicenter prospective SENTICOL study. Ann. Surg. Oncol. 2013, 20, 413–422. [Google Scholar] [CrossRef]
- Kim, S.M.; Choi, H.S.; Byun, J.S. Overall 5-year survival rate and prognostic factors in patients with stage IB and IIA cervical cancer treated by radical hysterectomy and pelvic lymph node dissection. Int. J. Gynecol. Cancer 2000, 10, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Sawada, S.; Murata, T. Relationship between lymph node metastases and prognosis in patients irradiated postoperatively for carcinoma of the uterine cervix. Acta. Radiol. Oncol. 1984, 23, 455–459. [Google Scholar] [CrossRef]
- Koh, W.J.; Abu-Rustum, N.R.; Bean, S.; Bradley, K.; Campos, S.M.; Cho, K.R.; Chon, H.S.; Chu, C.; Clark, R.; Cohn, D.; et al. Cervical Cancer, Version 3.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 64–84. [Google Scholar] [CrossRef]
- Bhatla, N.; Berek, J.S.; Cuello Fredes, M.; Denny, L.A.; Grenman, S.; Karunaratne, K.; Kehoe, S.T.; Konishi, I.; Olawaiye, A.B.; Prat, J.; et al. Revised FIGO staging for carcinoma of the cervix uteri. Int. J. Gynaecol. Obstet. 2019, 145, 129–135. [Google Scholar] [CrossRef]
- Marth, C.; Landoni, F.; Mahner, S.; McCormack, M.; Gonzalez-Martin, A.; Colombo, N.; Committee, E.G. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv262. [Google Scholar] [CrossRef]
- van de Lande, J.; Torrenga, B.; Raijmakers, P.G.; Hoekstra, O.S.; van Baal, M.W.; Brolmann, H.A.; Verheijen, R.H. Sentinel lymph node detection in early stage uterine cervix carcinoma: A systematic review. Gynecol. Oncol. 2007, 106, 604–613. [Google Scholar] [CrossRef]
- Niikura, H.; Tsuji, K.; Tokunaga, H.; Shimada, M.; Ishikawa, M.; Yaegashi, N. Sentinel node navigation surgery in cervical and endometrial cancer: A review. Jpn. J. Clin. Oncol. 2019, 49, 495–500. [Google Scholar] [CrossRef]
- Tax, C.; Rovers, M.M.; de Graaf, C.; Zusterzeel, P.L.; Bekkers, R.L. The sentinel node procedure in early stage cervical cancer, taking the next step; a diagnostic review. Gynecol. Oncol. 2015, 139, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Echt, M.L.; Finan, M.A.; Hoffman, M.S.; Kline, R.C.; Roberts, W.S.; Fiorica, J.V. Detection of sentinel lymph nodes with lymphazurin in cervical, uterine, and vulvar malignancies. South Med. J. 1999, 92, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Balaya, V.; Bresset, A.; Guani, B.; Magaud, L.; Montero Macias, R.; Delomenie, M.; Bonsang-Kitzis, H.; Ngo, C.; Bats, A.S.; Mathevet, P.; et al. Risk factors for failure of bilateral sentinel lymph node mapping in early-stage cervical cancer. Gynecol. Oncol. 2020, 156, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Sahbai, S.; Taran, F.A.; Staebler, A.; Wallwiener, D.; la Fougere, C.; Brucker, S.; Dittmann, H. Sentinel lymph node mapping using SPECT/CT and gamma probe in endometrial cancer: An analysis of parameters affecting detection rate. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1511–1519. [Google Scholar] [CrossRef]
- Weissinger, M.; Taran, F.A.; Gatidis, S.; Kommoss, S.; Nikolaou, K.; Sahbai, S.; Fougere, C.; Brucker, S.Y.; Dittmann, H. Lymph Node Staging with a Combined Protocol of (18)F-FDG PET/MRI and Sentinel Node SPECT/CT: A Prospective Study in Patients with FIGO I/II Cervical Carcinoma. J. Nucl. Med. 2021, 62, 1062–1067. [Google Scholar] [CrossRef]
- Sakuragi, N.; Satoh, C.; Tanaka, T.; Horikawa, I.; Nishiya, M.; Ohkubo, H.; Hirahatake, K.; Ohkochi, T.; Iwakawa, Y.; Fujimoto, S. The incidence and clinical significance of paraaortic lymph node metastases in patients with uterine cervical cancer. Nihon Sanka Fujinka Gakkai Zasshi 1990, 42, 60–66. [Google Scholar]
- Tsunoda, A.T.; Marnitz, S.; Soares Nunes, J.; de Cunha Andrade, C.E.M.; Scapulatempo Neto, C.; Blohmer, J.U.; Herrmann, J.; Kerr, L.M.; Martus, P.; Schneider, A.; et al. Incidence of Histologically Proven Pelvic and Para-Aortic Lymph Node Metastases and Rate of Upstaging in Patients with Locally Advanced Cervical Cancer: Results of a Prospective Randomized Trial. Oncology 2017, 92, 213–220. [Google Scholar] [CrossRef]
- Diaz-Feijoo, B.; Perez-Benavente, M.A.; Cabrera-Diaz, S.; Gil-Moreno, A.; Roca, I.; Franco-Camps, S.; Fernandez, M.S.; Garcia-Jimenez, A.; Xercavins, J.; Martinez-Palones, J.M. Change in clinical management of sentinel lymph node location in early stage cervical cancer: The role of SPECT/CT. Gynecol. Oncol. 2011, 120, 353–357. [Google Scholar] [CrossRef]
- Wang, X.; Zhong, X.; Lei, H.; Yang, N.; Gao, X.; Cheng, L. Tumor microenvironment-responsive contrast agents for specific cancer imaging: A narrative review. J. Bio-X Res. 2020, 3, 144–156. [Google Scholar] [CrossRef]
- Liu, B.; Gao, S.; Li, S. A Comprehensive Comparison of CT, MRI, Positron Emission Tomography or Positron Emission Tomography/CT, and Diffusion Weighted Imaging-MRI for Detecting the Lymph Nodes Metastases in Patients with Cervical Cancer: A Meta-Analysis Based on 67 Studies. Gynecol. Obstet. Investig. 2017, 82, 209–222. [Google Scholar] [CrossRef]
- Sarabhai, T.; Schaarschmidt, B.M.; Wetter, A.; Kirchner, J.; Aktas, B.; Forsting, M.; Ruhlmann, V.; Herrmann, K.; Umutlu, L.; Grueneisen, J. Comparison of (18)F-FDG PET/MRI and MRI for pre-therapeutic tumor staging of patients with primary cancer of the uterine cervix. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Cysouw, M.C.F.; Kramer, G.M.; Hoekstra, O.S.; Frings, V.; de Langen, A.J.; Smit, E.F.; van den Eertwegh, A.J.; Oprea-Lager, D.E.; Boellaard, R. Accuracy and Precision of Partial-Volume Correction in Oncological PET/CT Studies. J. Nucl. Med. 2016, 57, 1642–1649. [Google Scholar] [CrossRef] [PubMed]
- German Clinical Trials Register (DRKS). Available online: https://www.drks.de/drks_web/setLocale_EN.do (accessed on 27 August 2020).
- Nogami, Y.; Banno, K.; Irie, H.; Iida, M.; Masugi, Y.; Murakami, K.; Aoki, D. Efficacy of 18-FDG PET-CT dual-phase scanning for detection of lymph node metastasis in gynecological cancer. Anticancer Res. 2015, 35, 2247–2253. [Google Scholar] [PubMed]
- Minig, L.; Fagotti, A.; Scambia, G.; Salvo, G.; Patrono, M.G.; Haidopoulos, D.; Zapardiel, I.; Domingo, S.; Sotiropoulou, M.; Chisholm, G.; et al. Incidence of Lymph Node Metastases in Women with Low-Risk Early Cervical Cancer (<2 cm) without Lymph-Vascular Invasion. Int. J. Gynecol. Cancer 2018, 28, 788–793. [Google Scholar] [CrossRef]
- Collarino, A.; Garganese, G.; Valdes Olmos, R.A.; Stefanelli, A.; Perotti, G.; Mirk, P.; Fragomeni, S.M.; Ieria, F.P.; Scambia, G.; Giordano, A.; et al. Evaluation of Dual-Timepoint (18) F-FDG PET/CT Imaging for Lymph Node Staging in Vulvar Cancer. J. Nucl. Med. 2017, 58, 1913–1918. [Google Scholar] [CrossRef]
- Ma, S.Y.; See, L.C.; Lai, C.H.; Chou, H.H.; Tsai, C.S.; Ng, K.K.; Hsueh, S.; Lin, W.J.; Chen, J.T.; Yen, T.C. Delayed (18) F-FDG PET for detection of paraaortic lymph node metastases in cervical cancer patients. J. Nucl. Med. 2003, 44, 1775–1783. [Google Scholar]
- Peppicelli, S.; Andreucci, E.; Ruzzolini, J.; Bianchini, F.; Calorini, L. FDG uptake in cancer: A continuing debate. Theranostics 2020, 10, 2944–2948. [Google Scholar] [CrossRef]
- Stecco, A.; Buemi, F.; Cassara, A.; Matheoud, R.; Sacchetti, G.M.; Arnulfo, A.; Brambilla, M.; Carriero, A. Comparison of retrospective PET and MRI-DWI (PET/MRI-DWI) image fusion with PET/CT and MRI-DWI in detection of cervical and endometrial cancer lymph node metastases. Radiol. Med. 2016, 121, 537–545. [Google Scholar] [CrossRef]
- Kim, S.K.; Choi, H.J.; Park, S.Y.; Lee, H.Y.; Seo, S.S.; Yoo, C.W.; Jung, D.C.; Kang, S.; Cho, K.S. Additional value of MR/PET fusion compared with PET/CT in the detection of lymph node metastases in cervical cancer patients. Eur. J. Cancer 2009, 45, 2103–2109. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Average ± SD | Range | |
| Age at PET/MR (years) | 46.8 ± 11.5 | 28–72 |
| Patient height (cm) | 166 ± 6.6 | 152–187 |
| Patient weight (kg) | 71.0 ± 16.2 | 44–117 |
| BMI (kg/m²) | 25.7 ± 5.4 | 15–40 |
| Time between PET/MR and LN histology (days) | 22.4 ± 16.7 | 1–89 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weissinger, M.; Kommoss, S.; Jacoby, J.; Ursprung, S.; Seith, F.; Hoffmann, S.; Nikolaou, K.; Brucker, S.Y.; La Fougère, C.; Dittmann, H. Multiparametric Dual-Time-Point [18F]FDG PET/MRI for Lymph Node Staging in Patients with Untreated FIGO I/II Cervical Carcinoma. J. Clin. Med. 2022, 11, 4943. https://doi.org/10.3390/jcm11174943
Weissinger M, Kommoss S, Jacoby J, Ursprung S, Seith F, Hoffmann S, Nikolaou K, Brucker SY, La Fougère C, Dittmann H. Multiparametric Dual-Time-Point [18F]FDG PET/MRI for Lymph Node Staging in Patients with Untreated FIGO I/II Cervical Carcinoma. Journal of Clinical Medicine. 2022; 11(17):4943. https://doi.org/10.3390/jcm11174943
Chicago/Turabian StyleWeissinger, Matthias, Stefan Kommoss, Johann Jacoby, Stephan Ursprung, Ferdinand Seith, Sascha Hoffmann, Konstantin Nikolaou, Sara Yvonne Brucker, Christian La Fougère, and Helmut Dittmann. 2022. "Multiparametric Dual-Time-Point [18F]FDG PET/MRI for Lymph Node Staging in Patients with Untreated FIGO I/II Cervical Carcinoma" Journal of Clinical Medicine 11, no. 17: 4943. https://doi.org/10.3390/jcm11174943
APA StyleWeissinger, M., Kommoss, S., Jacoby, J., Ursprung, S., Seith, F., Hoffmann, S., Nikolaou, K., Brucker, S. Y., La Fougère, C., & Dittmann, H. (2022). Multiparametric Dual-Time-Point [18F]FDG PET/MRI for Lymph Node Staging in Patients with Untreated FIGO I/II Cervical Carcinoma. Journal of Clinical Medicine, 11(17), 4943. https://doi.org/10.3390/jcm11174943