
Clinical Outcome of Intraoperative Recurrent Laryngeal Nerve Monitoring during Thoracoscopic Esophagectomy and Mediastinal Lymph Node Dissection for Esophageal Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Intubation and Anesthesia
2.3. Surgical Procedure
2.4. Intraoperative Monitoring for RLN
2.5. Follow-up and Data Collection
2.6. Statistical Analysis
3. Results
3.1. Patient Clinical Data
3.2. Surgical Outcomes
3.3. Postoperative Morbidity and Survival Outcome
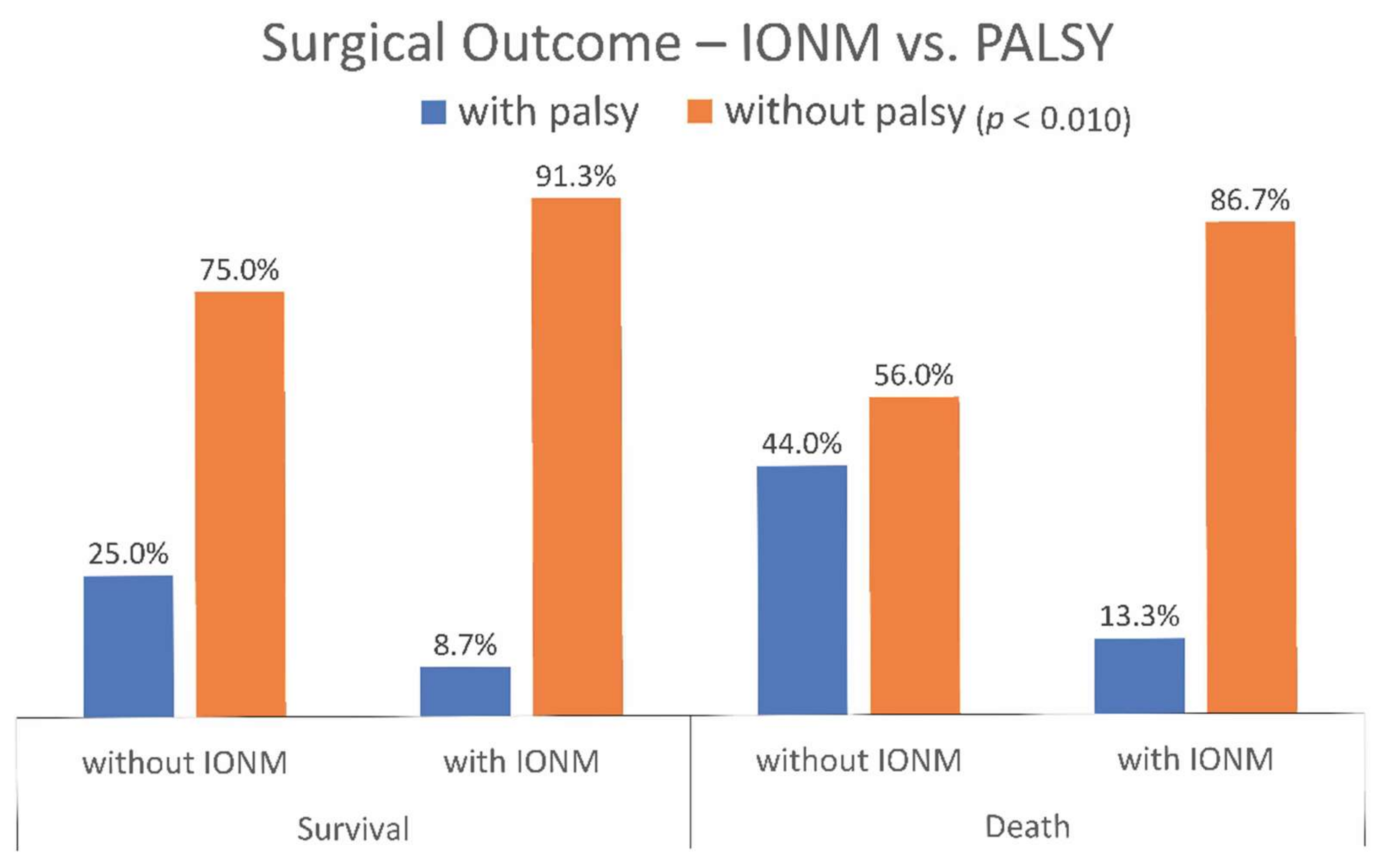
Survival Outcome
3.4. Postoperative Vocal Cord Palsy Predictors and Influence of OS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Demarest, C.T.; Chang, A.C. The Landmark Series: Multimodal Therapy for Esophageal Cancer. Ann. Surg. Oncol. 2021, 28, 3375–3382. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, H.; Tsurumaru, M.; Udagawa, H.; Kajiyama, Y. Radical lymph node dissection for cancer of the thoracic esophagus. Ann Surg. 1994, 220, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Bona, D.; Lombardo, F.; Matsushima, K.; Cavalli, M.; Lastraioli, C.; Bonitta, G.; Cirri, S.; Danelli, P.; Aiolfi, A. Three-field versus two-field lymphadenectomy for esophageal squamous cell carcinoma: A long-term survival meta-analysis. Surgery 2022, 171, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.H.; Kim, Y.T.; Jeon, S.H.; Sung, S.W.; Kim, J.H. Lymphadenectomy extent is closely related to long-term survival in esophageal cancer. Eur. J. Cardiothorac. Surg. 2007, 31, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.Y.; Wang, Z.Q.; Wang, Y.C.; Li, G.; Luo, J.; Chen, L.Q.; Liu, L.X.; Zhou, Q.H.; Lin, Y.D. Oesophageal adenocarcinoma has a higher risk of lymph node metastasis than squamous cell carcinoma: A propensity score-matched study. Eur. J. Cardiothorac. Surg. 2017, 52, 958–962. [Google Scholar] [CrossRef] [PubMed]
- Mine, S.; Sano, T.; Hiki, N.; Yamada, K.; Kosuga, T.; Nunobe, S.; Shigaki, H.; Yamaguchi, T. Thoracic lymph node involvement in adenocarcinoma of the esophagogastric junction and lower esophageal squamous cell carcinoma relative to the location of the proximal end of the tumor. Ann. Surg. Oncol. 2014, 21, 1596–1601. [Google Scholar] [CrossRef]
- Mine, S.; Watanabe, M.; Kumagai, K.; Okamura, A.; Yuda, M.; Hayami, M.; Yamashita, K.; Imamura, Y.; Ishizuka, N. Comparison of mediastinal lymph node metastases from adenocarcinoma of the esophagogastric junction versus lower esophageal squamous cell carcinoma with involvement of the esophagogastric junction. Dis. Esophagus 2019, 32, doz002. [Google Scholar] [CrossRef]
- Kanemura, T.; Makino, T.; Miyazaki, Y.; Takahashi, T.; Kurokawa, Y.; Yamasaki, M.; Nakajima, K.; Takiguchi, S.; Mori, M.; Doki, Y. Distribution patterns of metastases in recurrent laryngeal nerve lymph nodes in patients with squamous cell esophageal cancer. Dis. Esophagus 2017, 30, 1–7. [Google Scholar] [CrossRef]
- Ma, L.; Xiang, J.; Zhang, Y.; Hu, H.; Shao, R.; Lin, D. Characteristics and clinical significance of recurrent laryngeal nerve lymph node metastasis in esophageal squamous cell carcinoma. J. BUON 2017, 22, 1533–1539. [Google Scholar]
- Jang, H.J.; Lee, H.S.; Kim, M.S.; Lee, J.M.; Zo, J.I. Patterns of lymph node metastasis and survival for upper esophageal squamous cell carcinoma. Ann. Thorac. Surg. 2011, 92, 1091–1097. [Google Scholar] [CrossRef] [PubMed]
- Baba, M.; Natsugoe, S.; Shimada, M.; Nakano, S.; Noguchi, Y.; Kawachi, K.; Kusano, C.; Aikou, T. Does hoarseness of voice from recurrent nerve paralysis after esophagectomy for carcinoma influence patient quality of life? J. Am. Coll. Surg. 1999, 188, 231–236. [Google Scholar] [CrossRef]
- Shimizu, H.; Shiozaki, A.; Fujiwara, H.; Konishi, H.; Kosuga, T.; Komatsu, S.; Ichikawa, D.; Okamoto, K.; Otsuji, E. Short- and Long-term Progress of Recurrent Laryngeal Nerve Paralysis After Subtotal Esophagectomy. Anticancer Res. 2017, 37, 2019–2023. [Google Scholar] [CrossRef] [PubMed]
- Oshikiri, T.; Takiguchi, G.; Hasegawa, H.; Yamamoto, M.; Kanaji, S.; Yamashita, K.; Matsuda, T.; Nakamura, T.; Suzuki, S.; Kakeji, Y. Postoperative recurrent laryngeal nerve palsy is associated with pneumonia in minimally invasive esophagectomy for esophageal cancer. Surg. Endosc. 2021, 35, 837–844. [Google Scholar] [CrossRef]
- Wright, C.D.; Zeitels, S.M. Recurrent laryngeal nerve injuries after esophagectomy. Thorac. Surg. Clin. 2006, 16, 23–33. [Google Scholar] [CrossRef]
- Yang, S.; Zhou, L.; Lu, Z.; Ma, B.; Ji, Q.; Wang, Y. Systematic review with meta-analysis of intraoperative neuromonitoring during thyroidectomy. Int. J. Surg. 2017, 39, 104–113. [Google Scholar] [CrossRef]
- Ratner, B. Variable selection methods in regression: Ignorable problem, outing notable solution. J. Target Meas. Anal. Mark. 2010, 18, 65–75. [Google Scholar] [CrossRef]
- Zhong, D.; Zhou, Y.; Li, Y.; Wang, Y.; Zhou, W.; Cheng, Q.; Chen, L.; Zhao, J.; Li, X.; Yan, X. Intraoperative recurrent laryngeal nerve monitoring: A useful method for patients with esophageal cancer. Dis. Esophagus 2014, 27, 444–451. [Google Scholar] [CrossRef]
- Hikage, M.; Kamei, T.; Nakano, T.; Abe, S.; Katsura, K.; Taniyama, Y.; Sakurai, T.; Teshima, J.; Ito, S.; Niizuma, N.; et al. Impact of routine recurrent laryngeal nerve monitoring in prone esophagectomy with mediastinal lymph node dissection. Surg. Endosc. 2017, 31, 2986–2996. [Google Scholar] [CrossRef]
- Takeda, S.; Iida, M.; Kanekiyo, S.; Nishiyama, M.; Tokumitsu, Y.; Shindo, Y.; Yoshida, S.; Suzuki, N.; Yoshino, S.; Nagano, H. Efficacy of intraoperative recurrent laryngeal neuromonitoring during surgery for esophageal cancer. Ann. Gastroenterol. Surg. 2021, 5, 83–92. [Google Scholar] [CrossRef]
- Fan, N.; Yang, H.; Zheng, J.; Chen, D.; Wang, W.; Tan, Z.; Huang, Y.; Lin, P. Comparison of short- and long-term outcomes between 3-field and modern 2-field lymph node dissections for thoracic oesophageal squamous cell carcinoma: A propensity score matching analysis. Interact. Cardiovasc. Thorac. Surg. 2019, 29, 434–441. [Google Scholar] [CrossRef]
- Hemmerling, T.M.; Schmidt, J.; Jacobi, K.E.; Klein, P. Intraoperative monitoring of the recurrent laryngeal nerve during single-lung ventilation in esophagectomy. Anesth. Analg. 2001, 92, 662–664. [Google Scholar] [CrossRef]
- Schmidt, J.; Irouschek, A.; Heinrich, S.; Oster, O.; Klein, P.; Birkholz, T. Recurrent laryngeal nerve monitoring during esophagectomy and mediastinal lymph node dissection: A novel approach using a single-lumen endotracheal EMG tube and the EZ-blocker. World J. Surg. 2012, 36, 2946–2947. [Google Scholar] [CrossRef]
- Gelpke, H.; Grieder, F.; Decurtins, M.; Cadosch, D. Recurrent laryngeal nerve monitoring during esophagectomy and mediastinal lymph node dissection. World J. Surg. 2010, 34, 2379–2382. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| IONM (n = 38) | Non-IONM (n = 37) | p-Value | |||
|---|---|---|---|---|---|
| n (%) | n (%) | ||||
| Age (mean ± SD) | 60.18 ± 8.99 | 56.16 ± 9.78 | 0.068 | ||
| Gender | |||||
| Male | 34 | 89% | 34 | 92% | 0.719 |
| Female | 4 | 11% | 3 | 8% | |
| History of H and N cancer | |||||
| No | 34 | 89% | 30 | 81% | 0.304 |
| Yes | 4 | 11% | 7 | 19% | |
| Neoadjuvant CCRT | |||||
| No | 23 | 61% | 17 | 46% | 0.206 |
| Yes | 15 | 39% | 20 | 54% | |
| cT stage | |||||
| 1 | 6 | 16% | 2 | 5% | 0.038 |
| 2 | 9 | 24% | 21 | 57% | |
| 3 | 21 | 55% | 13 | 35% | |
| 4 | 2 | 5% | 1 | 3% | |
| cN stage | |||||
| 0 | 16 | 42% | 9 | 24% | 0.331 |
| 1 | 12 | 32% | 15 | 41% | |
| 2 | 6 | 16% | 10 | 27% | |
| 3 | 4 | 11% | 3 | 8% | |
| Tumor location | |||||
| Upper thoracic/middle thoracic | 27 | 71% | 24 | 65% | 0.566 |
| Lower thoracic/EG junction | 11 | 29% | 13 | 35% | |
| Cell type | |||||
| Squamous cell carcinoma | 33 | 87% | 34 | 92% | 0.716 |
| Adenocarcinoma | 4 | 11% | 2 | 5% | |
| Others | 1 | 3% | 1 | 3% | |
| IONM | Non-IONM | p-Value | ||||
|---|---|---|---|---|---|---|
| n = 38 | % | n = 37 | % | |||
| Operation time, minutes | Median (IQR) | 570 | (533–644) | 633 | (586–688) | 0.007 |
| Blood loss, ml | Median (IQR) | 100 | (50–150) | 150 | (100–200) | 0.019 |
| ICU LOS, days | Mean ± SD | 4.6 ± 2.6 | 5.9 ± 4.2 | 0.096 | ||
| Hospital LOS, days | Mean ± SD | 21.1 ± 9.7 | 19.8 ± 7.7 | 0.515 | ||
| pT stage | ||||||
| 0 | 6 | 16% | 10 | 27% | 0.624 | |
| Tis | 0 | 0% | 1 | 3% | ||
| 1 | 7 | 18% | 4 | 11% | ||
| 2 | 8 | 21% | 5 | 14% | ||
| 3 | 16 | 42% | 16 | 43% | ||
| 4 | 1 | 3% | 1 | 3% | ||
| pN stage | ||||||
| 0 | 19 | 50% | 17 | 46% | 0.337 | |
| 1 | 8 | 21% | 13 | 35% | ||
| 2 | 11 | 29% | 7 | 19% | ||
| Harvested MLN | 30.0 ± 12.9 | 28.9 ± 8.7 | 0.670 | |||
| Positive MLN | 1.0 ± 1.6 | 0.7 ± 1.0 | 0.391 | |||
| Ratio of positive MLN | 2.97% | 2.53% | ||||
| Harvested TLN | 41.9 ± 13.9 | 41.5 ± 11.7 | 0.898 | |||
| Positive TLN | 1.4 ± 1.8 | 1.3 ± 1.7 | 0.710 | |||
| Ratio of positive TLN | 3.23% | 3.01% | ||||
| Harvested right RLN LN | 3.6 ± 2.4 | 3.3 ± 2.3 | 0.572 | |||
| Harvested left RLN LN | 3.1 ± 3.2 | 1.8 ± 2.0 | 0.043 | |||
| IONM | non-IONM | p-Value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Vocal cord palsy | 4 | 10.5% | 14 | 37.8% | 0.006 |
| Right/left/bilateral | 2/2/0 | 3/10/1 | |||
| Pneumonia | 5 | 13.2% | 14 | 37.8% | 0.014 |
| Other complications | |||||
| Anastomosis leakage | 5 | 28% | 3 | 14% | 0.298 |
| Pneumothorax/air leak | 1 | 6% | 1 | 5% | 0.911 |
| Chylothorax | 2 | 11% | 0 | 0% | 0.117 |
| Chyloabdomen | 1 | 6% | 1 | 5% | 0.911 |
| Loculated pleural effusion | 3 | 17% | 2 | 10% | 0.506 |
| Respiratory failure | 0 | 0% | 1 | 5% | 0.348 |
| HR | 95.0% CI | p-Value | |
|---|---|---|---|
| Vocal cord palsy (with) | 2.98 | (1.32–6.71) | 0.008 |
| Age (year) | 1.05 | (1.01–1.08) | 0.016 |
| pT(Tis + T1a/b + T2) | 7.25 | (2.09–25.17) | 0.002 |
| pT(T3 + T4) | 12.53 | (3.62–43.35) | 0.000 |
| Neoadjuvant CCRT | 8.37 | (3.59–19.52) | 0.000 |
| ICU duration (day) | 1.11 | (1.00–1.22) | 0.040 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-L.; Chen, C.-M.; Hung, W.-H.; Cheng, Y.-F.; Hong, R.-P.; Wang, B.-Y.; Cheng, C.-Y. Clinical Outcome of Intraoperative Recurrent Laryngeal Nerve Monitoring during Thoracoscopic Esophagectomy and Mediastinal Lymph Node Dissection for Esophageal Cancer. J. Clin. Med. 2022, 11, 4949. https://doi.org/10.3390/jcm11174949
Huang C-L, Chen C-M, Hung W-H, Cheng Y-F, Hong R-P, Wang B-Y, Cheng C-Y. Clinical Outcome of Intraoperative Recurrent Laryngeal Nerve Monitoring during Thoracoscopic Esophagectomy and Mediastinal Lymph Node Dissection for Esophageal Cancer. Journal of Clinical Medicine. 2022; 11(17):4949. https://doi.org/10.3390/jcm11174949
Chicago/Turabian StyleHuang, Chang-Lun, Chun-Min Chen, Wei-Heng Hung, Ya-Fu Cheng, Ruei-Ping Hong, Bing-Yen Wang, and Ching-Yuan Cheng. 2022. "Clinical Outcome of Intraoperative Recurrent Laryngeal Nerve Monitoring during Thoracoscopic Esophagectomy and Mediastinal Lymph Node Dissection for Esophageal Cancer" Journal of Clinical Medicine 11, no. 17: 4949. https://doi.org/10.3390/jcm11174949
APA StyleHuang, C.-L., Chen, C.-M., Hung, W.-H., Cheng, Y.-F., Hong, R.-P., Wang, B.-Y., & Cheng, C.-Y. (2022). Clinical Outcome of Intraoperative Recurrent Laryngeal Nerve Monitoring during Thoracoscopic Esophagectomy and Mediastinal Lymph Node Dissection for Esophageal Cancer. Journal of Clinical Medicine, 11(17), 4949. https://doi.org/10.3390/jcm11174949