
A Real-Life Action toward the End of HIV Pandemic: Surveillance of Mother-to-Child HIV Transmission in a Center from Southeast Romania

 , ,
, ,
Abstract
:1. Introduction
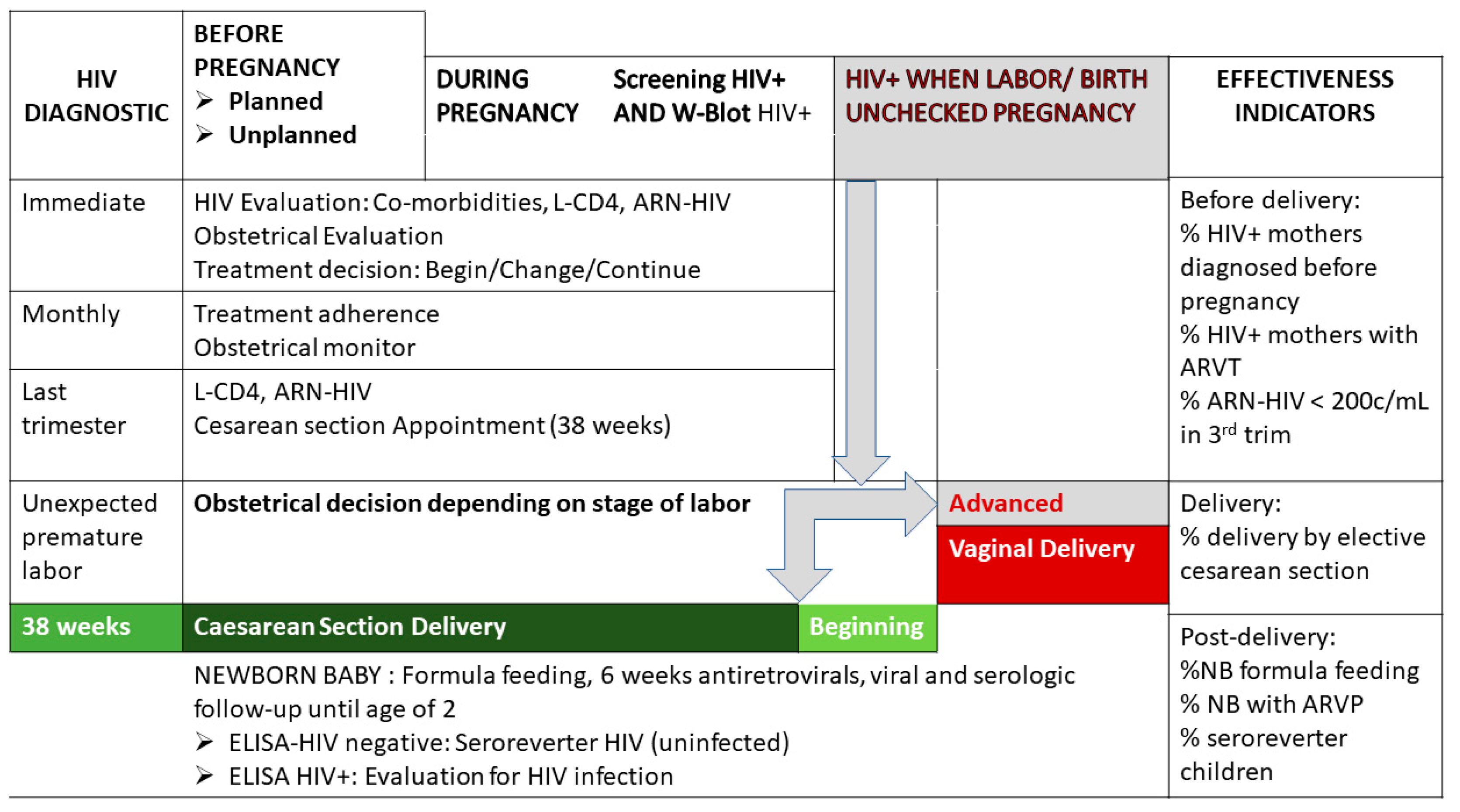
2. Materials and Methods
- Prenatal interventions for mother HIV diagnosis, evaluation and treatment.
- Birth decision for procedures of vaginal or caesarean section.
- After birth intervention for the clinical evaluation of newborns, feed them with formula, antiretroviral medication for six weeks, subject them to virologic and serologic monitoring for at least 18 months.
3. Results
4. Discussion
4.1. Local Condition of Perinatal Transmission
4.2. Peculiarities of HIV-Positive Mother Survivors from the Pediatric Cohort
4.3. The Impact of HIV on Maternal and Neonatal Mortality
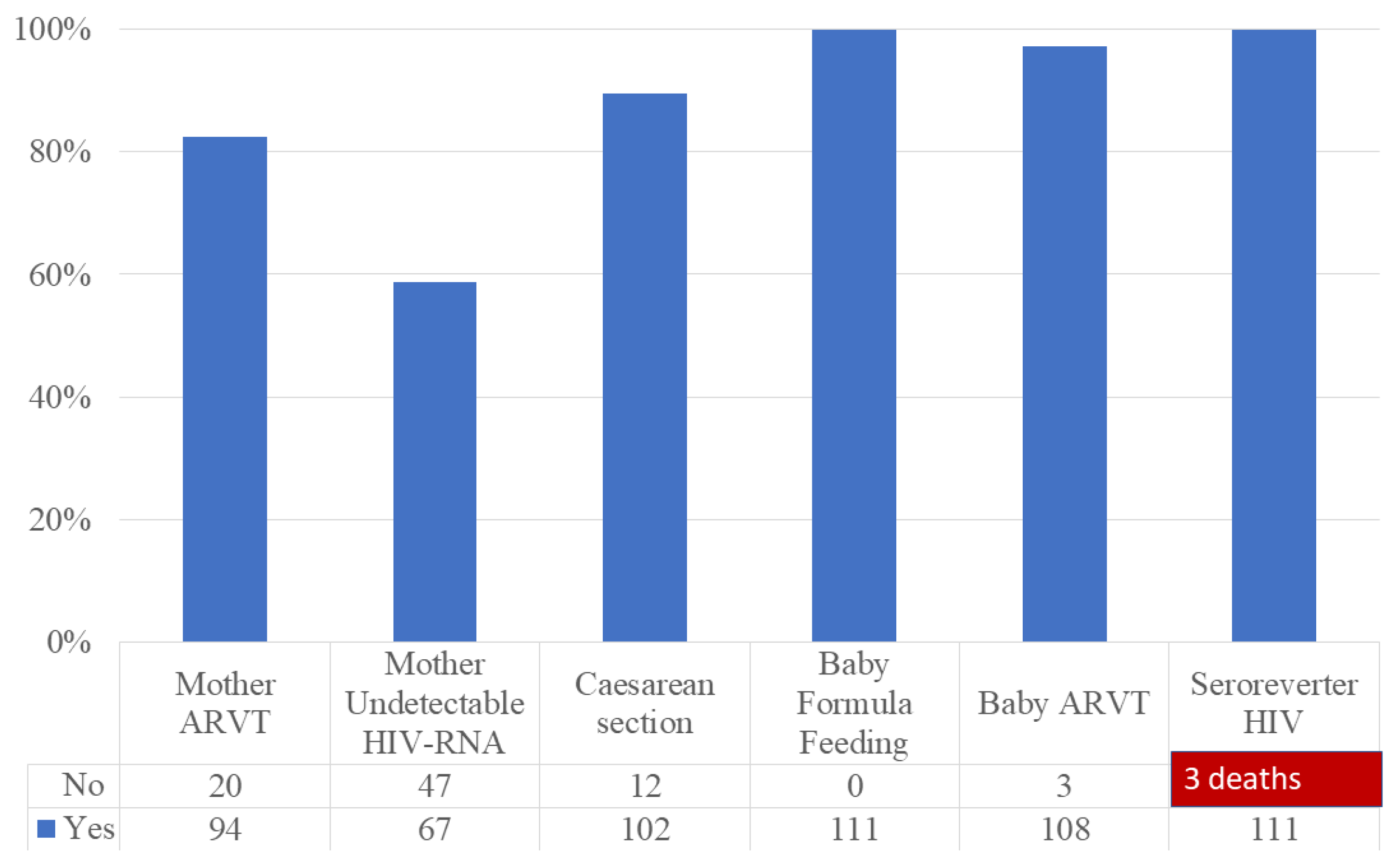
4.4. The Impact of Preventive Interventions on HIV-Exposed Children
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Arv Structure | Combinations | No. |
|---|---|---|
| 2INRT + INNRT | CBV + EFV | 1 |
| CBV + NVP | 1 | |
| KVX + NVP | 2 | |
| EMC/TDF + NVP | 1 | |
| 2INRT + IP | CBV + INV/R | 9 |
| CBV + NFV | 2 | |
| CBV + KAL | 29 | |
| CBV + DRV/r | 1 | |
| CBV + TEL/r | 2 | |
| KVX + ATV/r | 4 | |
| KVX + DRV/R | 2 | |
| KVX + INV/r | 4 | |
| KVX + KAL | 10 | |
| KVX + TEL/r | 1 | |
| EMC/TDF + KAL | 4 | |
| EMC/TDF + ATV/r | 4 | |
| EMC/TDF + DRV/r | 1 | |
| 2INRT + II | CBV + RLG | 4 |
| KVX + RLG | 1 | |
| EMC/TDF + RLG | 1 | |
| KVX + DLG | 1 | |
| Other | TZV + DRV/r | 2 |
| TZV + KAL | 1 | |
| TDF + EVR + DRV/r | 1 | |
| EVR + RLG + DRV/R | 4 |
| ARV | No |
|---|---|
| AZT | 4 |
| AZT + 3TC | 94 |
| AZT + 3TC + NVP | 11 |
| None | 5 |
| Anomaly Group | n | % | Findings at Birth | N | % |
|---|---|---|---|---|---|
| Skin | 36 | 31.57% | Angioma | 31 | 27.19% |
| Pigmented lesions | 4 | 3.50% | |||
| Ear | 1 | 0.87% | Microtia | 1 | 0.87% |
| Abdominal wall | 1 | 0.87% | Umbilical hernia | 1 | 0.87% |
| Muscles and bones findings | 24 | 21.05% | Dermal sinus | 1 | 0.87% |
| Hip dysplasia | 2 | 1.75% | |||
| Hip Dislocation | 4 | 3.50% | |||
| Varus equines | 14 | 12.28% | |||
| Metatarsus valgus | 3 | 2.63% | |||
| Congenital torticollis | 1 | 0.87% | |||
| Neurologic | 9 | 7.89% | Spina bifida oculta | 1 | 0.87% |
| Dysgenesis corpus callosum syndrome | 1 | 0.87% | |||
| Microcephalia | 1 | 0.87% | |||
| Retro cerebellar arachnoid cysts | 1 | 0.87% | |||
| Subarachnoid cyst | 1 | 0.87% | |||
| Choroid plexus cyst | 2 | 1.75% | |||
| Lenticulostriate vasculopathy | 2 | 1.75% | |||
| Cardiac | 9 | 7.89% | Persistent arterial duct | 4 | 3.50% |
| Unspecified non cyanogen cardiopathy | 2 | 1.75% | |||
| Interatrial septum aneurysm | 1 | 0.87% | |||
| Cardiomyopathy | 1 | 0.87% | |||
| Situs solitus | 1 | 0.87% | |||
| Urogenital | 9 | 7.89% | Pyelocaliceal ectasia | 3 | 2.63% |
| Hydrocele | 4 | 3.50% | |||
| Cryptorchidy | 2 | 1.75% |
| Birth Defects Absent | Birth Defects Present | Chi-Square Test | ||
|---|---|---|---|---|
| Nelfinavir | Yes | 2 | 0 | p = 0.676 |
| No | 103 | 9 | ||
| Lopinavir/r | Yes | 40 | 3 | p = 0.777 |
| No | 65 | 6 | ||
| Darunavir/r | Yes | 9 | 1 | p = 0.796 |
| No | 96 | 8 | ||
| Invirase/r | Yes | 11 | 2 | p = 0.287 |
| No | 94 | 7 | ||
| Atazanavir/r | Yes | 8 | 0 | p = 0.390 |
| No | 97 | 9 | ||
| Fosamprenavir/r | Yes | 2 | 1 | p = 0.097 |
| No | 103 | 8 | ||
| Nevirapine | Yes | 4 | 0 | p = 0.551 |
| No | 101 | 9 | ||
| Efavirenz | Yes | 1 | 0 | p = 0.768 |
| No | 104 | 9 | ||
| Etravirine | Yes | 3 | 1 | p = 0.196 |
| No | 102 | 8 | ||
| Combivir | Yes | 47 | 5 | p = 0.532 |
| No | 58 | 4 | ||
| Kivexa | Yes | 21 | 1 | p = 0.516 |
| No | 84 | 8 | ||
| Emtricitabine/Tenofovirum | Yes | 12 | 0 | p = 0.283 |
| No | 93 | 9 | ||

References
- UNAIDS Joint United Nations Programme on HIV/AIDS. UNAIDS DATA 2019. Available online: https://www.unaids.org/sites/default/files/media_asset/2019-UNAIDS-data_en.pdf (accessed on 12 January 2022).
- WHO. Consolidated HIV Strategic Information Guidelines: Driving Impact through Programme Monitoring and Management; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/9789240000735 (accessed on 12 January 2022).
- WHO. Guidelines: Updated Recommendations on HIV Prevention, Infant Diagnosis, Antiretroviral Initiation and Monitoring: March 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Yan, H.; Peters, H.; Thorne, C. Neonatal deaths among infants born to women living with HIV in the UK and Ireland. AIDS 2022, 36, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.S.; Chen, Y.Q.; McCauley, M.; Gamble, T.; Hosseinipour, M.C.; Kumarasamy, N.; Hakim, J.G.; Kumwenda, J.; Grinsztejn, B.; Pilotto, J.H.; et al. Antiretroviral Therapy for the Prevention of HIV-1 Transmission. N. Engl. J. Med. 2016, 375, 830–839. [Google Scholar] [CrossRef]
- Cohen, M.S.; Gamble, T.; McCauley, M. Prevention of HIV Transmission and the HPTN 052 Study. Annu. Rev. Med. 2020, 71, 347–360. [Google Scholar] [CrossRef] [PubMed]
- NAM Aidsmap NAM Endorses Undetectable Equals Untransmittable (U=U) Consensus Statement. 2017. Available online: http://www.aidsmap.com/news/feb-2017/nam-endorses-undetectable-equals-untransmittable-uu-consensus-statement#_ednref1 (accessed on 25 July 2022).
- Panel on Treatment of HIV during Pregnancy and Prevention of Perinatal Transmission. Recommendations for Use of Antiretroviral Drugs in Transmission in the United States. Available online: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/Perinatal_GL.pdf (accessed on 19 January 2022).
- Ministerul Sanatatii. Ordinul nr. 1241 din 9 August 2019. Ghid Privind Infectia HIV in Sarcina. Monitorul Oficial al Romaniei Partea I, nr. 738 bis din 10 Septembrie 2019. Available online: https://legislatie.just.ro/Public/DetaliiDocumentAfis/218537 (accessed on 11 January 2022).
- Comisia Natională de Luptă Anti-SIDA—Date Statistice. Available online: http://cnlas.ro/com_jce/date-statistice.html (accessed on 28 June 2021).
- Panel on Antiretroviral Therapy and Medical Management of Children Living with HIV. Guidelines for the Use of Antiretroviral Agents in Pediatric HIV Infection. Available online: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/Diagnosis_of_HIV_in_Infants.pdf (accessed on 18 January 2022).
- Pinto, F.; Fernandes, E.; Virella, D.; Abrantes, A.; Neto, M.T. Born Preterm: A Public Health Issue. Port. J. Public Health 2019, 37, 38–49. [Google Scholar] [CrossRef]
- European Network of Population-Based Registries for the Epidemiological Surveillance of Congenital Anomalies. Available online: https://eu-rd-platform.jrc.ec.europa.eu/eurocat/eurocat-data/prevalence_en (accessed on 4 March 2022).
- European Surveillance of Congenital Anomalies (EUROCAT). Guide 1.4. Chapter 3.2. 2020. Available online: https://eu-rd-platform.jrc.ec.europa.eu/sites/default/files/JRC-EUROCAT-Section-3.2-23-9-2020.pdf (accessed on 12 February 2021).
- Arbune, M.; Cojocaru, M.E.; Stefanescu, V. Neurological Malformation Related to Human Immunodeficiency Virus: Case Report. Acta Med. Transilv. 2017, 22, 26–27. Available online: http://www.amtsibiu.ro/Arhiva/2017/Nr3-en/Arbune.pdf (accessed on 12 February 2022).
- Marcu, E.-A.; Dinescu, S.-N.; Pădureanu, V.; Dumitrescu, F.; Diaconu, R. Perinatal Exposure to HIV Infection: The Experience of Craiova Regional Centre, Romania. Healthcare 2022, 10, 308. [Google Scholar] [CrossRef]
- Cambrea, S.-C.; Pinzaru, A.-D. Value of Caesarian Section in HIV-Positive Women, Caesarean Section, Georgios Androutsopoulos, IntechOpen. Available online: https://www.intechopen.com/chapters/61216 (accessed on 26 September 2018).
- Jianu, C.; Bolboacă, S.D.; Topan, A.V.; Filipescu, I.; Jianu, M.E.; Itu-Mureşan, C. A View of Human Immunodeficiency Virus Infections in the North-West Region of Romania. Medicina 2019, 55, 765. [Google Scholar] [CrossRef]
- World Health Organization. Trends in Maternal Mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division; World Health Organization: Geneva, Switzerland, 2019; Available online: https://cdn.who.int/media/docs/default-source/gho-documents/maternal-health-countries/maternal_health_rou_en.pdf (accessed on 20 December 2021).
- Calvert, C.; Marston, M.; Slaymaker, E.; Crampin, A.C.; Price, A.J.; Klein, N.; Herbst, K.; Michael, D.; Urassa, M.; Clark, S.J.; et al. Direct maternal deaths attributable to HIV in the era of antiretroviral therapy: Evidence from three population-based HIV cohorts with verbal autopsy. AIDS 2020, 34, 1397–1405. [Google Scholar] [CrossRef]
- Lathrop, E.; Jamieson, D.J.; Danel, I. HIV and maternal mortality. Int. J. Gynecol. Obstet. 2014, 127, 213–215. [Google Scholar] [CrossRef]
- Remera, E.; Chammartin, F.; Nsanzimana, S.; Forrest, J.I.; Smith, E.G.; Mugwaneza, P.; Malamba, S.S.; Semakula, M.; Condo, J.U.; Ford, N.; et al. Child mortality associated with maternal HIV status: A retrospective analysis in Rwanda, 2005-2015. BMJ Glob. Health 2021, 6, e004398. [Google Scholar] [CrossRef]
- Trahan, M.-J.; Boucher, M.; Renaud, C.; Karatzios, C.; Metras, M.-E.; Valois, S.; Ransy, D.G.; Lamarre, V.; Kakkar, F. Pregnancies Among the First Generation of Survivors of Perinatal HIV Infection. J. Obstet. Gynaecol. Can. 2020, 42, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Aagaard-Tillery, K.M.; Lin, M.G.; Lupo, V.; Buchbinder, A.; Ramsey, P.S. Preterm premature rupture of membranes in human immunodeficiency virus-infected women: A novel case series. Infect. Dis. Obstet. Gynecol. 2006, 2006, 53234. [Google Scholar] [CrossRef] [PubMed]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef]
- Tudor, A.M.; Mardarescu, M.; Petre, C.; Drăghicenoiu, R.N.; Ungurianu, R.; Tiliscan, C.; Otelea, D.; Cambrea, S.C.; Tănase, D.E.; Schweitzer, A.M.; et al. Birth outcome in HIV vertically-exposed children in two Romanian centers. Germs 2015, 5, 116–124. [Google Scholar] [CrossRef]
- d’Arminio Monforte, A.; Galli, L.; Lo Caputo, S.; Lichtner, M.; Pinnetti, C.; Bobbio, N. Pregnancy outcomes among ART-naive and ART-experienced HIV-positive women: Data from the ICONA foundation study group, years 1997–2013. JAIDS J. Acquir. Immune Defic. Syndr. 2014, 67, 258–267. [Google Scholar] [CrossRef]
- Piske, M.; Qiu, A.Q.; Maan, E.J.; Sauvé, L.J.; Forbes, J.C.; Alimenti, A.; Janssen, P.A.; Money, D.M.; Côté, H.C.; for the CIHR Team Grant on Cellular Aging and HIV Comorbidities in Women and Children. Preterm Birth and Antiretroviral Exposure in Infants HIV-exposed Uninfected. Pediatr. Infect. Dis. J. 2021, 40, 245–250. [Google Scholar] [CrossRef]
- Delicio, A.M.; Lajos, G.J.; Amaral, E.; Cavichiolli, F.; Polydoro, M.; Milanez, H. Adverse effects in children exposed to maternal HIV and antiretroviral therapy during pregnancy in Brazil: A cohort study. Reprod. Health 2018, 15, 76. [Google Scholar] [CrossRef]
- APR. Antiretroviral Pregnancy Registry Interim Report 1 January 1989 through 31 July 2021. Available online: http://www.apregistry.com/forms/appendix_c.pdf (accessed on 20 January 2022).
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Watts, D.H.; Li, D.; Handelsman, E.; Tilson, H.; Paul, M.; Foca, M.; Vajaranant, M.; Diaz, C.; Tuomala, R.; Thompson, B. Assessment of Birth Defects according to Maternal Therapy Among Infants in the Women and Infants Transmission Study. JAIDS J. Acquir. Immune Defic. Syndr. 2007, 44, 299–305. [Google Scholar] [CrossRef]
- Brogly, S.B.; Abzug, M.J.; Watts, D.H.; Cunningham, C.K.; Williams, P.L.; Oleske, J.; Conway, D.; Sperling, R.S.; Spiegel, H.; Van Dyke, R.B. Birth Defects Among Children Born to Human Immunodeficiency Virus-Infected Women: Pediatric AIDS clinical trials protocols 219 and 219C. Pediatr. Infect. Dis. J. 2010, 29, 721–727. [Google Scholar] [CrossRef]
- Sibiude, J.; Mandelbrot, L.; Blanche, S.; Le Chenadec, J.; Boullag-Bonnet, N.; Faye, A.; Dollfus, C.; Tubiana, R.; Bonnet, D.; Lelong, N.; et al. Association between Prenatal Exposure to Antiretroviral Therapy and Birth Defects: An Analysis of the French Perinatal Cohort Study (ANRS CO1/CO11). PLoS Med. 2014, 11, e1001635. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Data | Categories | N | % |
|---|---|---|---|
| Living area | Urban | 56 | 49% |
| Rural | 58 | 51% | |
| Formal education level | Illiteracy | 14 | 12.28% |
| 4 years | 21 | 18.42% | |
| 8 years | 62 | 54.38% | |
| ≥12 years | 17 | 14.91% | |
| Smoking | Yes | 76 | 66.66% |
| No | 38 | 33.33% | |
| Civil status | Single | 16 | 14% |
| Unmarried couple | 46 | 40% | |
| Married | 52 | 46% | |
| Father HIV status | Positive | 39 | 34% |
| Negative | 61 | 54% | |
| Unknown | 14 | 12% | |
| HIV Diagnostic HIV related to pregnancy | Before pregnancy | 92 | 81% |
| During pregnancy | 12 | 10% | |
| At birth | 10 | 9% | |
| The rank of birth | First birth | 73 | 65% |
| Second birth | 27 | 24% | |
| ≥3 births | 10 | 9% | |
| Twins (2 pairs) | 2 | 2% | |
| Hepatitis B virus co-infection | Yes | 32 | 28% |
| No | 82 | 72% | |
| AIDS | Yes | 64 | 57% |
| No | 49 | 43% | |
| RNA-HIV(cut-off for detection 400 copies/mL) | Detectable | 39 | 34% |
| Undetectable | 67 | 59% | |
| Unavailable | 8 | 7% | |
| Antiretrovirals during pregnancy | Yes | 94 | 82.45% |
| All the pregnancy | 70 | 61.40% | |
| After the 1st trimester | 24 | 21.05% | |
| No | 20 | 17.54% |
| Average | SD | Median | Max | Min | CI 0.95 | p * | |
|---|---|---|---|---|---|---|---|
| Gestational age (weeks) | 37.21 | 2.20 | 38 | 41 | 29 | 36.8; 37.6 | <0.001 |
| Apgar score | 8 | 1.02 | 8 | 10 | 4 | 7.80; 8.19 | <0.001 |
| Weight (grams) | 2739 | 512.03 | 2800 | 3800 | 1300 | 2635; 2830 | <0.001 |
| Length (cm) | 47.91 | 3.32 | 49 | 54 | 33 | 47.2; 48.5 | <0.001 |
| Cranial circumference (cm) | 32.60 | 2.31 | 33 | 48 | 25 | 32.0; 33.0 | <0.001 |
| Anomaly Group | Findings at Birth | N | Study Prevalence % | EUROCAT Prevalence per 10,000 Births All Registries |
|---|---|---|---|---|
| Cardio-vascular | Atrial septal defect | 4 | 3.50% | 14.68 |
| Ventricular septal defect | 3 | 2.63% | 35.83 | |
| Urogenital | Hydronephrosis | 1 | 0.87% | 11.76 |
| Hypospadias | 1 | 0.87% | 16.18 | |
| Abdominal wall | Gastroschisis | 1 | 0.87% | 1.14 |
| Overall | 10 | 8.7% | 188.23 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arbune, M.; Calin, A.M.; Iancu, A.V.; Dumitru, C.N.; Arbune, A.A. A Real-Life Action toward the End of HIV Pandemic: Surveillance of Mother-to-Child HIV Transmission in a Center from Southeast Romania. J. Clin. Med. 2022, 11, 5020. https://doi.org/10.3390/jcm11175020
Arbune M, Calin AM, Iancu AV, Dumitru CN, Arbune AA. A Real-Life Action toward the End of HIV Pandemic: Surveillance of Mother-to-Child HIV Transmission in a Center from Southeast Romania. Journal of Clinical Medicine. 2022; 11(17):5020. https://doi.org/10.3390/jcm11175020
Chicago/Turabian StyleArbune, Manuela, Alina Mihaela Calin, Alina Viorica Iancu, Caterina Nela Dumitru, and Anca Adriana Arbune. 2022. "A Real-Life Action toward the End of HIV Pandemic: Surveillance of Mother-to-Child HIV Transmission in a Center from Southeast Romania" Journal of Clinical Medicine 11, no. 17: 5020. https://doi.org/10.3390/jcm11175020
APA StyleArbune, M., Calin, A. M., Iancu, A. V., Dumitru, C. N., & Arbune, A. A. (2022). A Real-Life Action toward the End of HIV Pandemic: Surveillance of Mother-to-Child HIV Transmission in a Center from Southeast Romania. Journal of Clinical Medicine, 11(17), 5020. https://doi.org/10.3390/jcm11175020