
Influence of Bone Morphology on In Vivo Tibio-Femoral Kinematics in Healthy Knees during Gait Activities
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
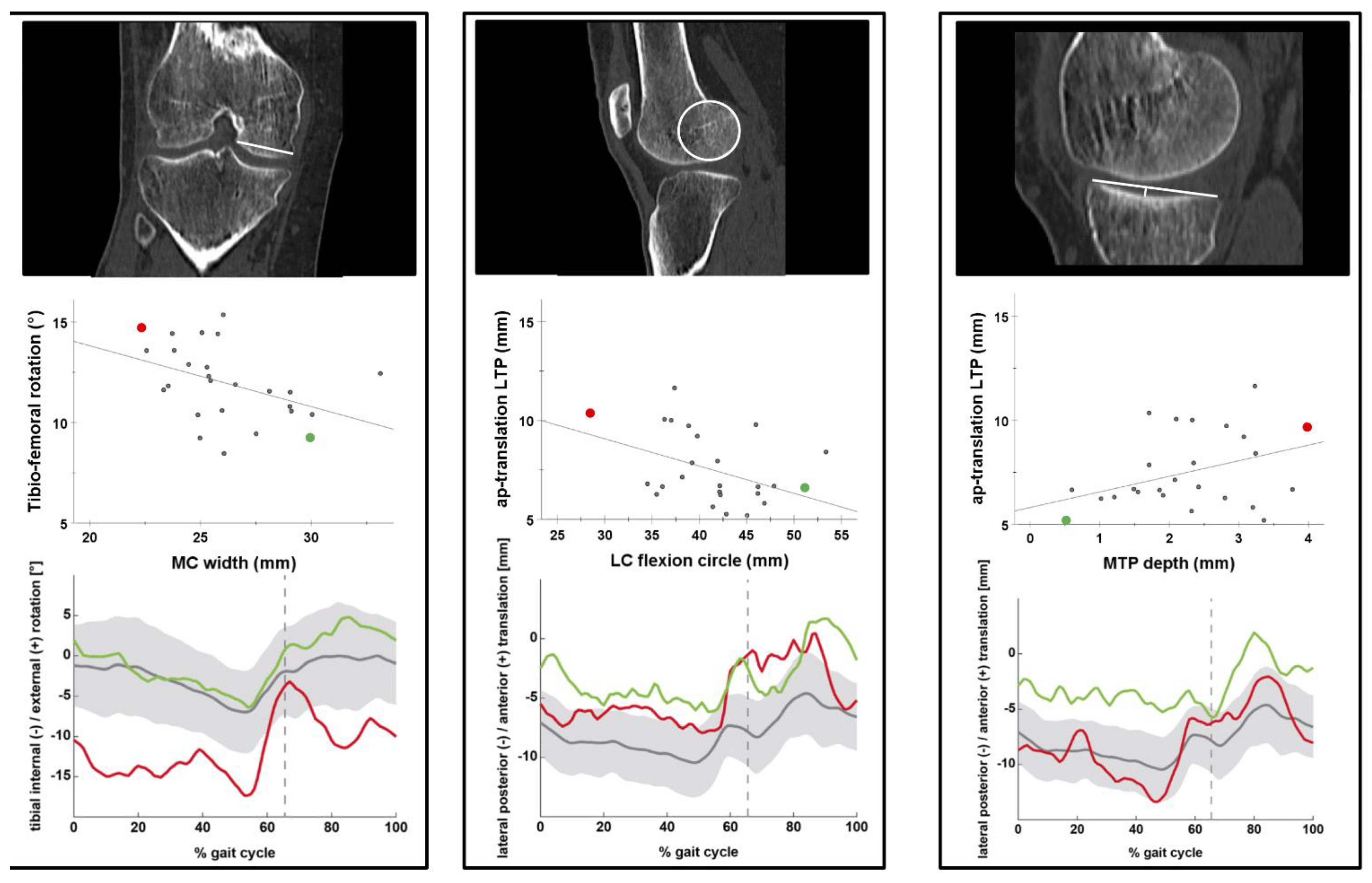
2.2. Femoral and Tibial Bone Morphology
- -
- Femoral bone morphology:
- -
- Tibial bone morphology:
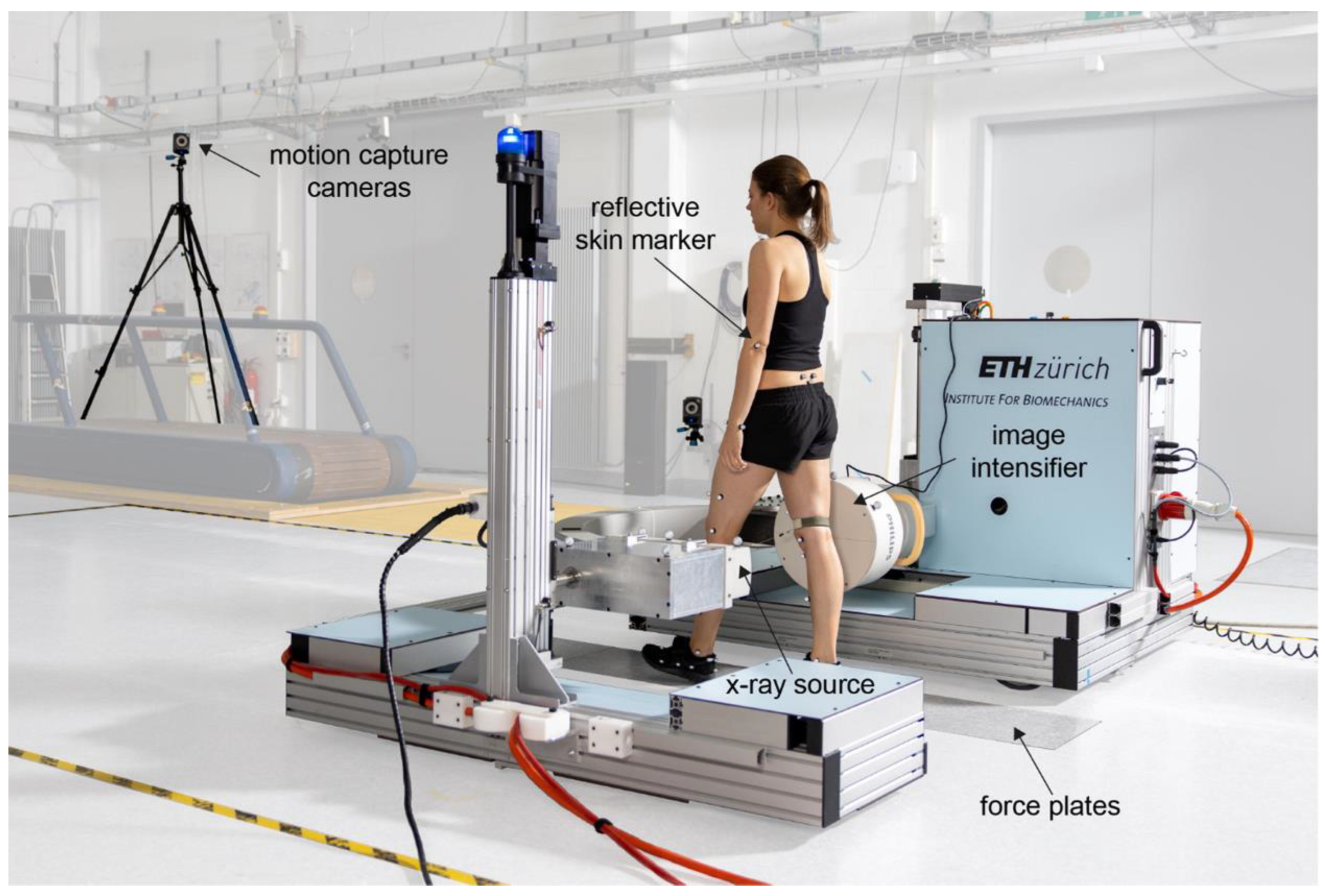
2.3. Video-Fluoroscopy Set-Up and Motion Tasks
2.4. Tibio-Femoral Kinematic Analysis
2.5. Statistical Analysis
3. Results
3.1. Tibio-Femoral Kinematics
3.2. Influence of Bone Morphology, Frontal, Axial Limb Alignment, and Demographics on Tibio-femoral Kinematics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Andriacchi, T.P.; Alexander, E.J.; Toney, M.K.; Dyrby, C.; Sum, J. A Point Cluster Method for In Vivo Motion Analysis: Applied to a Study of Knee Kinematics. J. Biomech. Eng. 1998, 120, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Smoger, L.M.; Fitzpatrick, C.K.; Clary, C.W.; Cyr, A.J.; Maletsky, L.P.; Rullkoetter, P.J.; Laz, P.J. Statistical modeling to characterize relationships between knee anatomy and kinematics. J. Orthop. Res. 2015, 33, 1620–1630. [Google Scholar] [CrossRef] [PubMed]
- Hill, P.F.; Vedi, V.; Williams, A.; Iwaki, H.; Pinskerova, V.; Freeman, M.A.R. Tibiofemoral movement 2: The loaded and unloaded living knee studied by MRI. J. Bone Jt. Surgery. Br. Vol. 2000, 82, 1196–1198. [Google Scholar] [CrossRef]
- Iwaki, H.; Pinskerova, V.; Freeman, M.A.R. Tibiofemoral movement 1: The shapes and relative movements of the femur and tibia in the unloaded cadaver knee. J. Bone Jt. Surgery. Br. Vol. 2000, 82, 1189–1195. [Google Scholar] [CrossRef]
- Hashemi, J.; Chandrashekar, N.; Mansouri, H.; Gill, B.; Slauterbeck, J.R.; Schutt, R.C.; Dabezies, E.; Beynnon, B.D. Shallow Medial Tibial Plateau and Steep Medial and Lateral Tibial Slopes: New Risk Factors for Anterior Cruciate Ligament Injuries. Am. J. Sports Med. 2010, 38, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Hodel, S.; Kabelitz, M.; Tondelli, T.; Vlachopoulos, L.; Sutter, R.; Fucentese, S.F. Introducing the Lateral Femoral Condyle Index as a Risk Factor for Anterior Cruciate Ligament Injury. Am. J. Sports Med. 2019, 47, 2420–2426. [Google Scholar] [CrossRef]
- Hudek, R.; Schmutz, S.; Regenfelder, F.; Fuchs, B.; Koch, P.P. Novel Measurement Technique of the Tibial Slope on Conventional MRI. Clin. Orthop. Relat. Res. 2009, 467, 2066–2072. [Google Scholar] [CrossRef] [PubMed]
- Musahl, V.; Ayeni, O.R.; Citak, M.; Irrgang, J.J.; Pearle, A.D.; Wickiewicz, T.L. The influence of bony morphology on the magnitude of the pivot shift. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 1232–1238. [Google Scholar] [CrossRef]
- Kujala, U.M.; Nelimarkka, O.; Koskinen, S.K. Relationship between the pivot shift and the configuration of the lateral tibial plateau. Arch. Orthop. Trauma. Surg. 1992, 111, 228–229. [Google Scholar] [CrossRef]
- Schütz, P.; Postolka, B.; Gerber, H.; Ferguson, S.J.; Taylor, W.R.; List, R. Knee implant kinematics are task-dependent. J. R. Soc. Interface 2019, 16, 20180678. [Google Scholar] [CrossRef]
- Gray, H.A.; Guan, S.; Thomeer, L.T.; Schache, A.G.; De Steiger, R.; Pandy, M.G. Three-dimensional motion of the knee-joint complex during normal walking revealed by mobile biplane x-ray imaging. J. Orthop. Res. 2019, 37, 615–630. [Google Scholar] [CrossRef] [PubMed]
- Gale, T.; Anderst, W. Knee Kinematics of Healthy Adults Measured Using Biplane Radiography. J. Biomech. Eng. 2020, 142, 101004. [Google Scholar] [CrossRef] [PubMed]
- Postolka, B.; Schütz, P.; Fucentese, S.F.; Freeman, M.A.; Pinskerova, V.; List, R.; Taylor, W.R. Tibio-femoral kinematics of the healthy knee joint throughout complete cycles of gait activities. J. Biomech. 2020, 110, 109915. [Google Scholar] [CrossRef]
- Kozanek, M.; Hosseini, A.; Liu, F.; Van de Velde, S.K.; Gill, T.J.; Rubash, H.E.; Li, G.; Kozanek, M.; Hosseini, A.; Liu, F.; et al. Tibiofemoral kinematics and condylar motion during the stance phase of gait. J. Biomech. 2009, 42, 1877–1884. [Google Scholar] [CrossRef]
- Koo, S.; Andriacchi, T.P. The knee joint center of rotation is predominantly on the lateral side during normal walking. J. Biomech. 2008, 41, 1269–1273. [Google Scholar] [CrossRef]
- Liu, F.; Kozanek, M.; Hosseini, A.; Van de Velde, S.K.; Gill, T.J.; Rubash, H.E.; Li, G. In vivo tibiofemoral cartilage deformation during the stance phase of gait. J. Biomech. 2010, 43, 658–665. [Google Scholar] [CrossRef]
- Hu, X.; Pickle, N.T.; Grabowski, A.M.; Silverman, A.K.; Blemker, S.S. Muscle Eccentric Contractions Increase in Downhill and High-Grade Uphill Walking. Front. Bioeng. Biotechnol. 2020, 8, 573666. [Google Scholar] [CrossRef]
- Postolka, B. Tibio-femoral kinematics of natural versus replaced knees—A comparison using dynamic videofluoroscopy. Clin. Biomech. 2022, 96, 105667. [Google Scholar] [CrossRef]
- Balcarek, P.; Terwey, A.; Jung, K.; Walde, T.A.; Frosch, S.; Schüttrumpf, J.P.; Wachowski, M.M.; Dathe, H.; Stürmer, K.M. Influence of tibial slope asymmetry on femoral rotation in patients with lateral patellar instability. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2155–2163. [Google Scholar] [CrossRef] [PubMed]
- Folinais, D.; Thelen, P.; Delin, C.; Radier, C.; Catonne, Y.; Lazennec, J. Measuring femoral and rotational alignment: EOS system versus computed tomography. Orthop. Traumatol. Surg. Res. 2013, 99, 509–516. [Google Scholar] [CrossRef] [Green Version]
- List, R.; Postolka, B.; Schütz, P.; Hitz, M.; Schwilch, P.; Gerber, H.; Ferguson, S.J.; Taylor, W.R. A moving fluoroscope to capture tibiofemoral kinematics during complete cycles of free level and downhill walking as well as stair descent. PLoS ONE 2017, 12, e0185952. [Google Scholar] [CrossRef]
- Pauchard, Y.; Fitze, T.; Browarnik, D.; Eskandari, A.; Pauchard, I.; Enns-Bray, W.; Pálsson, H.; Sigurdsson, S.; Ferguson, S.J.; Harris, T.B.; et al. Interactive graph-cut segmentation for fast creation of finite element models from clinical ct data for hip fracture prediction. Comput. Methods Biomech. Biomed. Eng. 2016, 19, 1693–1703. [Google Scholar] [CrossRef] [PubMed]
- Foresti, M. In Vivo Measurement of Total Knee Joint Replacement Kinematics and Kinetics during Stair Descent. Ph.D. Thesis, ETH Zurich, Zurich, Switzerland, 2009. [Google Scholar]
- Postolka, B.; List, R.; Thelen, B.; Schütz, P.; Taylor, W.R.; Zheng, G. Evaluation of an intensity-based Algorithm for 2D/3D Registration of Natural Knee Videofluoroscopy. Med. Eng. Phys. 2020, 77, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Grood, E.S.; Suntay, W.J. A Joint Coordinate System for the Clinical Description of Three-Dimensional Motions: Application to the Knee. J. Biomech. Eng. 1983, 105, 136–144. [Google Scholar] [CrossRef]
- Ehrig, R.M.; Taylor, W.R.; Duda, G.N.; Heller, M.O. A survey of formal methods for determining functional joint axes. J. Biomech. 2007, 40, 2150–2157. [Google Scholar] [CrossRef]
- Ehrig, R.M.; Taylor, W.R.; Duda, G.N.; Heller, M.O. A survey of formal methods for determining the centre of rotation of ball joints. J. Biomech. 2006, 39, 2798–2809. [Google Scholar] [CrossRef]
- Fleiss, J. Design and Analysis of Clinical Experiments; John Wiley & Sons: Hoboken, NJ, USA, 1986. [Google Scholar]
- Pinskerova, V.; Johal, P.; Nakagawa, S.; Sosna, A.; Williams, A.; Gedroyc, W.; Freeman, M.A.R. Does the femur roll-back with flexion? J. Bone Jt. Surg. Br. Vol. 2004, 86, 925–931. [Google Scholar] [CrossRef]
- Shimokochi, Y.; Shultz, S.J. Mechanisms of Noncontact Anterior Cruciate Ligament Injury. J. Athl. Train. 2008, 43, 396–408. [Google Scholar] [CrossRef]
- Schütz, P.; Taylor, W.R.; Postolka, B.; Fucentese, S.F.; Koch, P.P.; Freeman, M.A.; Pinskerova, V.; List, R. Kinematic Evaluation of the GMK Sphere Implant During Gait Activities: A Dynamic Videofluoroscopy Study. J. Orthop. Res. 2019, 37, 2337–2347. [Google Scholar] [CrossRef]
- Shin, C.S.; Chaudhari, A.M.; Andriacchi, T.P. Valgus Plus Internal Rotation Moments Increase Anterior Cruciate Ligament Strain More Than Either Alone. Med. Sci. Sports Exerc. 2011, 43, 1484–1491. [Google Scholar] [CrossRef] [PubMed]
- Jacquet, C.; Pioger, C.; Seil, R.; Khakha, R.; Parratte, S.; Steltzlen, C.; Argenson, J.-N.; Pujol, N.; Ollivier, M. Incidence and Risk Factors for Residual High-Grade Pivot Shift After ACL Reconstruction With or Without a Lateral Extra-articular Tenodesis. Orthop. J. Sports Med. 2021, 9, 23259671211003590. [Google Scholar] [CrossRef] [PubMed]
- Kraeutler, M.J.; Welton, K.L.; Chahla, J.; Laprade, R.F.; Mccarty, E.C. Current Concepts of the Anterolateral Ligament of the Knee: Anatomy, Biomechanics, and Reconstruction. Am. J. Sports Med. 2018, 46, 1235–1242. [Google Scholar] [CrossRef]
- Getgood, A.; ALC Consensus Group; Brown, C.; Lording, T.; Amis, A.; Claes, S.; Geeslin, A.; Musahl, V. The anterolateral complex of the knee: Results from the International ALC Consensus Group Meeting. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 166–176. [Google Scholar] [CrossRef]
- Hodel, S.; Torrez, C.; Flury, A.; Fritz, B.; Steinwachs, M.R.; Vlachopoulos, L.; Fucentese, S.F. Tibial internal rotation in combined anterior cruciate ligament and high-grade anterolateral ligament injury and its influence on ACL length. BMC Musculoskelet Disord. 2022, 23, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wada, K.; Hamada, D.; Takasago, T.; Nitta, A.; Goto, T.; Tonogai, I.; Tsuruo, Y.; Sairyo, K. The medial constrained insert restores native knee rotational kinematics after bicruciate-retaining total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1621–1627. [Google Scholar] [CrossRef] [PubMed]
- Nasab, S.H.; Smith, C.; Postolka, B.; Schütz, P.; List, R.; Taylor, W. In Vivo Elongation Patterns of the Collateral Ligaments in Healthy Knees During Functional Activities. J. Bone Jt. Surg. 2021, 103, 1620–1627. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| 26 Subjects (26 Knees) | |
|---|---|
| Age (years) | 27.3 ± 10.5 (20 to 67) |
| Male | 13 |
| Female | 13 |
| BMI (kg/m2) | 21.3 ± 2.2 (17 to 26) |
| 177.6 ± 9.3 (162.0 to 195.2) |
| 67.3 ± 11.0 (50.8 to 93.6) |
| HKA (°) | +1.4 ± 4.1 (−8.0 to +9.0) |
| Femoral antetorsion (°) | 17.8 ± 11.4 (−6 to +52) |
| Tibial torsion (°) | 31.3 ± 7.4 (13 to 44) |
| Kinematic Outcome Variable | Regression Model Fit (R2; p-Value) | Factors Included in Regression Model β (95% CI) | p-Value (β) |
|---|---|---|---|
| Tibial internal/external rotation (°) | |||
| NA | NA | NA |
| 0.18; 0.03 | MC width: −0.30 (−0.58 to −0.03) | 0.03 |
| Lateral AP-translation (mm) | |||
| 0.24; 0.01 | Tibial slope asymmetry: 0.50 (0.13 to 0.87) | 0.01 |
| 0.38; 0.004 | LC flexion circle: −0.16 (−0.28 to −0.05) | 0.007 |
| MTP depth: 0.90 (0.23 to 1.56) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hodel, S.; Postolka, B.; Flury, A.; Schütz, P.; Taylor, W.R.; Vlachopoulos, L.; Fucentese, S.F. Influence of Bone Morphology on In Vivo Tibio-Femoral Kinematics in Healthy Knees during Gait Activities. J. Clin. Med. 2022, 11, 5082. https://doi.org/10.3390/jcm11175082
Hodel S, Postolka B, Flury A, Schütz P, Taylor WR, Vlachopoulos L, Fucentese SF. Influence of Bone Morphology on In Vivo Tibio-Femoral Kinematics in Healthy Knees during Gait Activities. Journal of Clinical Medicine. 2022; 11(17):5082. https://doi.org/10.3390/jcm11175082
Chicago/Turabian StyleHodel, Sandro, Barbara Postolka, Andreas Flury, Pascal Schütz, William R. Taylor, Lazaros Vlachopoulos, and Sandro F. Fucentese. 2022. "Influence of Bone Morphology on In Vivo Tibio-Femoral Kinematics in Healthy Knees during Gait Activities" Journal of Clinical Medicine 11, no. 17: 5082. https://doi.org/10.3390/jcm11175082
APA StyleHodel, S., Postolka, B., Flury, A., Schütz, P., Taylor, W. R., Vlachopoulos, L., & Fucentese, S. F. (2022). Influence of Bone Morphology on In Vivo Tibio-Femoral Kinematics in Healthy Knees during Gait Activities. Journal of Clinical Medicine, 11(17), 5082. https://doi.org/10.3390/jcm11175082