
Effects of Supervised Physical Exercise as Prehabilitation on Body Composition, Functional Capacity and Quality of Life in Bariatric Surgery Candidates: A Systematic Review and Meta-Analysis

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Plan and Literature Selection
2.2. Types of Participants/Population
2.3. Types of Intervention/Exposition
2.4. Types of Comparator/Control
2.5. Types of Outcome/Results Measurements
2.6. Studies Selection
2.7. Data Extraction
2.8. Risk of Bias Assessment
2.9. Evaluation of the Quality of Scientific Evidence
2.10. Statistical Analysis
3. Results
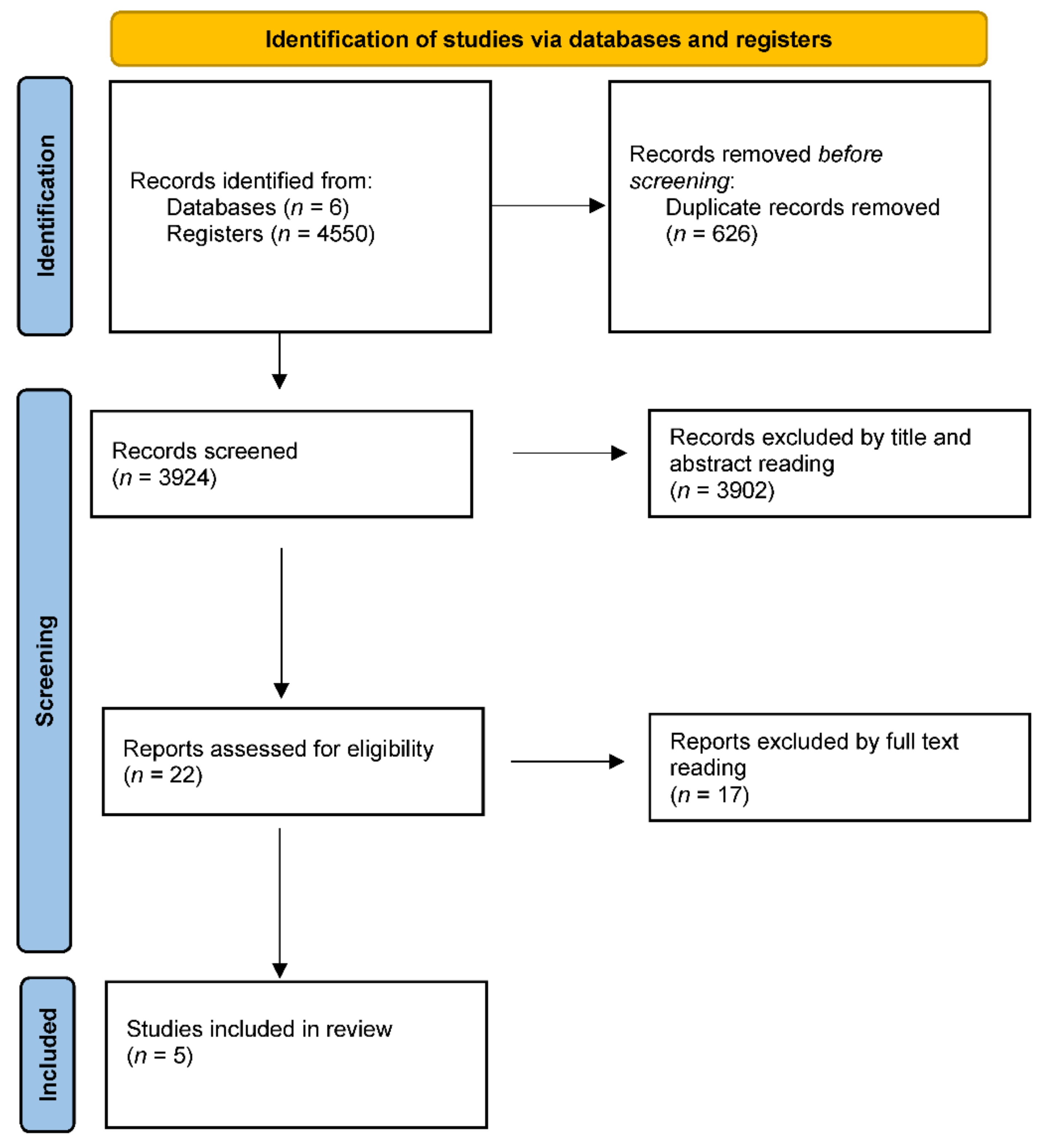
3.1. Article Selection
3.2. Articles’ Descriptions
3.3. Participants
3.4. Types of Intervention/Exposition
3.5. Types of Comparator/Control
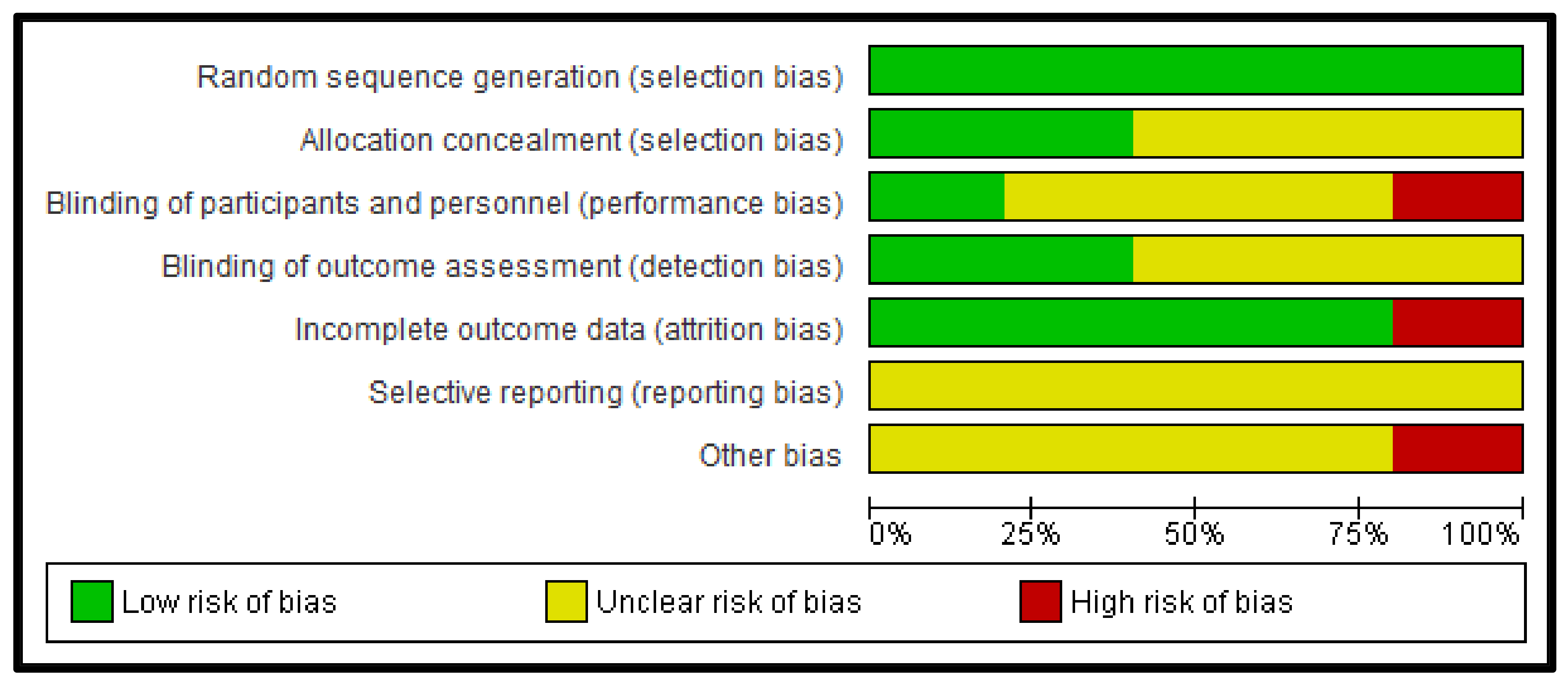
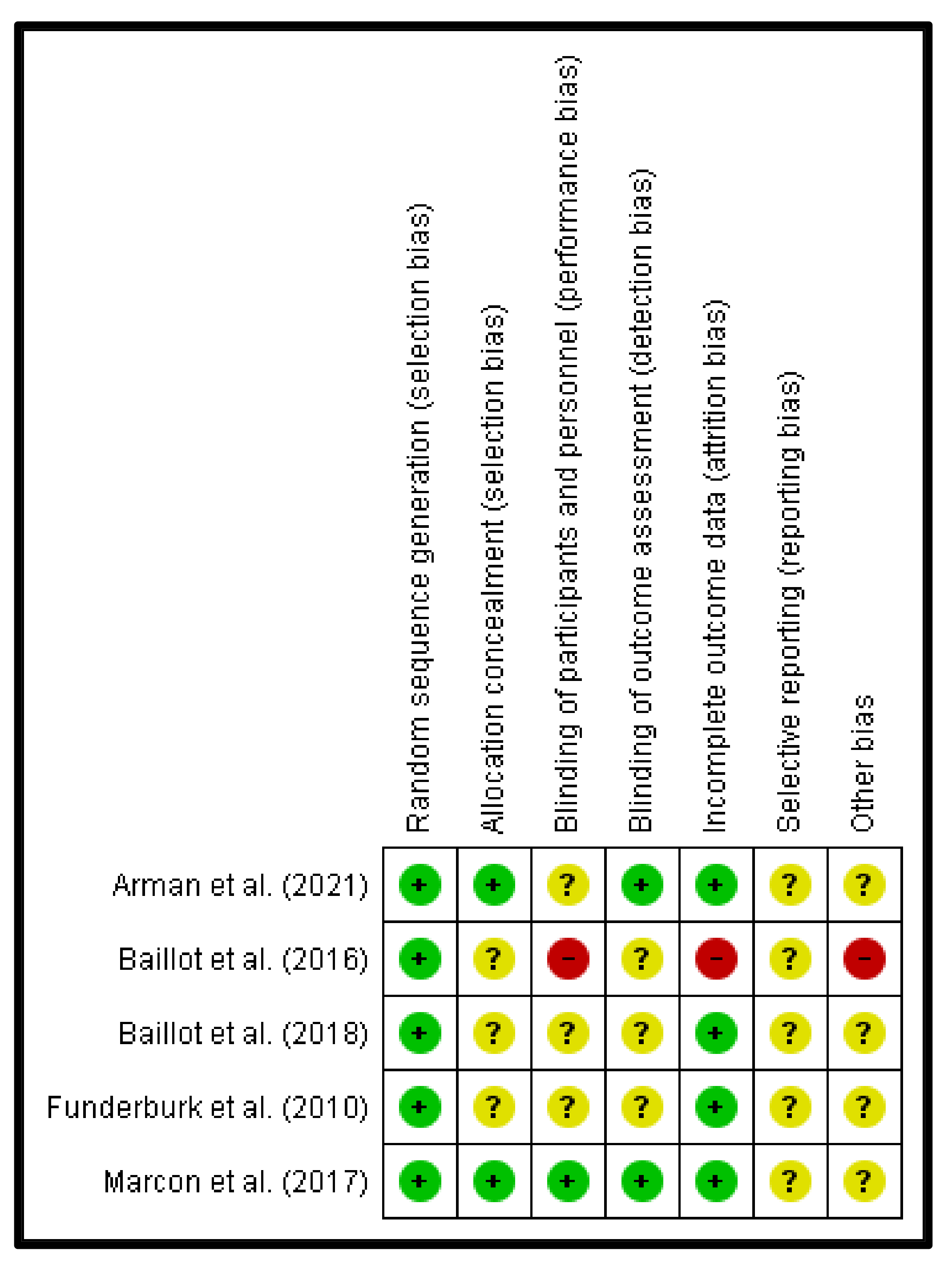
3.6. Risk of Bias Evaluation
3.7. Prehabilitation Effects on the Outcome Measurements
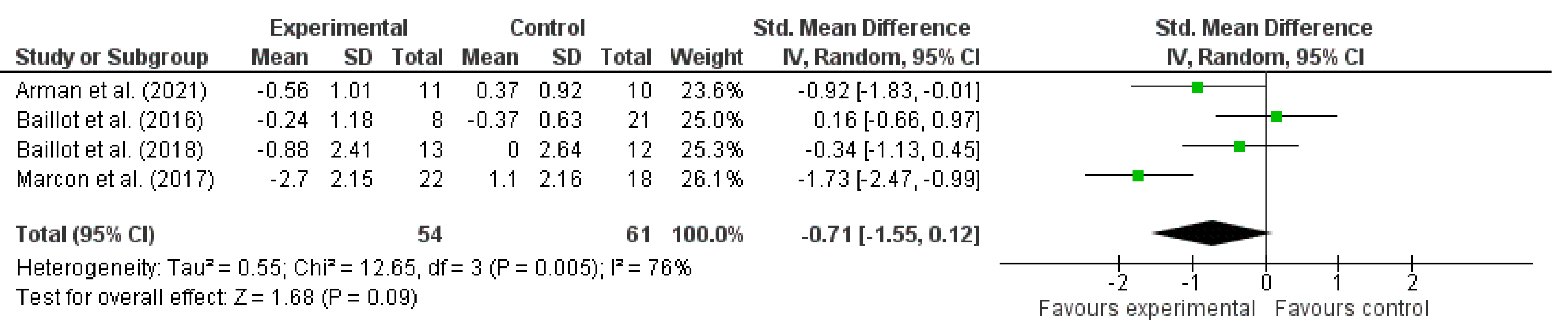
3.7.1. Body Composition
3.7.2. Functional Capacity
3.7.3. Quality of Life
3.7.4. Surgical Outcomes
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BS | Bariatric surgery. |
| ERAS | Enhanced recovery after surgery. |
| 6MWT | Six-minute walking test. |
| VO2 max | Maximal oxygen uptake. |
| GRADE | Grading of recommendations assessment, development, and evaluation. |
| SMD | Standard mean differences. |
| CORE | Core muscles of the body. |
| BMI | Body mass index. |
| OSQOL | Obesity Specific Quality of life. |
| HRR | Heart rate reserve. |
| WRQOL | Weight-Related Quality of Life. |
| SF 36 | Health-related quality of life questionnaire. |
| FM% | Fat mass in percent. |
| FFM Kg | Fat free mass in kilograms. |
| CI | Confidence interval. |
| RCTs | Randomized control trials |
References
- Schroeder, R.; Garrison, J.M., Jr.; Johnson, M.S. Treatment of adult obesity with bariatric surgery. Am. Fam. Physician 2011, 84, 805–814. [Google Scholar]
- Wharton, S.; Lau, D.C.; Vallis, M.; Sharma, A.M.; Biertho, L.; Campbell-Scherer, D.; Adamo, K.; Alberga, A.; Bell, R.; Boulé, N.; et al. Obesity in adults: A clinical practice guideline. CMAJ 2020, 192, E875–E891. [Google Scholar] [CrossRef]
- O’Brien, P.E.; Hindle, A.; Brennan, L.; Skinner, S.; Burton, P.; Smith, A.; Crosthwaite, G.; Brown, W. Long-Term Outcomes After Bariatric Surgery: A Systematic Review and Meta-analysis of Weight Loss at 10 or More Years for All Bariatric Procedures and a Single-Centre Review of 20-Year Outcomes After Adjustable Gastric Banding. Obes. Surg. 2019, 29, 3–14. [Google Scholar] [CrossRef]
- Segelman, J.; Nygren, J. Evidence or eminence in abdominal surgery: Recent improvements in perioperative care. World J. Gastroenterol. 2014, 20, 16615–16619. [Google Scholar] [CrossRef]
- Senturk, J.C.; Kristo, G.; Gold, J.; Bleday, R.; Whang, E. The Development of Enhanced Recovery After Surgery Across Surgical Specialties. J. Laparoendosc. Adv. Surg. Tech. 2017, 27, 863–870. [Google Scholar] [CrossRef]
- Dang, J.T.; Szeto, V.G.; Elnahas, A.; Ellsmere, J.; Okrainec, A.; Neville, A.; Malik, S.; Yorke, E.; Hong, D.; Biertho, L.; et al. Canadian consensus statement: Enhanced recovery after surgery in bariatric surgery. Surg. Endosc. 2020, 34, 1366–1375. [Google Scholar] [CrossRef]
- Stenberg, E.; Falcão, L.F.D.R.; O’Kane, M.; Liem, R.; Pournaras, D.J.; Salminen, P.; Urman, R.D.; Wadhwa, A.; Gustafsson, U.O.; Thorell, A. Guidelines for Perioperative Care in Bariatric Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations: A 2021 Update. World J. Surg. 2022, 46, 729–751. [Google Scholar] [CrossRef]
- Delgado Floody, P.; Jerez Mayorga, D.; Caamaño Navarrete, F.; Osorio Poblete, A.; Thuillier Lepeley, N.; Alarcón Hormazábal, M. Doce semanas de ejercicio físico intervalado con sobrecarga mejora las variables antropométricas de obesos mórbidos y obesos con comorbilidades postulantes a cirugía bariátrica. Nutr. Hosp. 2015, 32, 2007–2011. [Google Scholar]
- Carbone, S.; Del Buono, M.G.; Ozemek, C.; Lavie, C.J. Obesity, risk of diabetes and role of physical activity, exercise training and cardiorespiratory fitness. Prog. Cardiovasc. Dis. 2019, 62, 327–333. [Google Scholar] [CrossRef]
- Marc-Hernández, A.; Ruiz-Tovar, J.; Aracil, A.; Guillén, S.; Moya-Ramón, M. Impact of Exercise on Body Composition and Cardiometabolic Risk Factors in Patients Awaiting Bariatric Surgery. Obes. Surg. 2019, 29, 3891–3900. [Google Scholar] [CrossRef] [PubMed]
- Baillot, A.; Mampuya, W.M.; Dionne, I.J.; Comeau, E.; Méziat-Burdin, A.; Langlois, M.-F. Impacts of Supervised Exercise Training in Addition to Interdisciplinary Lifestyle Management in Subjects Awaiting Bariatric Surgery: A Randomized Controlled Study. Obes. Surg. 2016, 26, 2602–2610. [Google Scholar] [CrossRef]
- Lloréns, J.; Rovira, L.; Ballester, M.; Moreno, J.; Hernández-Laforet, J.; Santonja, F.-J.; Cassinello, N.; Ortega, J. Preoperative Inspiratory Muscular Training to Prevent Postoperative Hypoxemia in Morbidly Obese Patients Undergoing Laparoscopic Bariatric Surgery. A Randomized Clinical Trial. Obes. Surg. 2015, 25, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Whittle, J.; Wischmeyer, P.E.; Grocott, M.P.W.; Miller, T.E. Surgical Prehabilitation: Nutrition and Exercise. Anesthesiol. Clin. 2018, 36, 567–580. [Google Scholar] [CrossRef]
- Andrea Herrera, A.Z.; Nardo, N. Prehabilitation Effects on Body Composition, Functional Capacity, Quality of Life and Surgical Outcomes in Bariatric Surgery Candidates. PROSPERO, 2021, CRD42021261474. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021261474 (accessed on 25 October 2021).
- Baillot, A.; Vallée, C.-A.; Mampuya, W.M.; Dionne, I.J.; Comeau, E.; Méziat-Burdin, A.; Langlois, M.-F. Effects of a Pre-surgery Supervised Exercise Training 1 Year After Bariatric Surgery: A Randomized Controlled Study. Obes. Surg. 2018, 28, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Funderburk, J.; Callis, S. Aquatic intervention effect on quality of life prior to obesity surgery: A pilot study. Annu. Recreat. 2010, 18, 66–78. [Google Scholar]
- Marcon, E.R.; Baglioni, S.; Bittencourt, L.; Lopes, C.L.N.; Neumann, C.R.; Trindade, M.R.M. What Is the Best Treatment before Bariatric Surgery? Exercise, Exercise and Group Therapy, or Conventional Waiting: A Randomized Controlled Trial. Obes. Surg. 2017, 27, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Arman, N.; Tokgoz, G.; Seyit, H.; Karabulut, M. The effects of core stabilization exercise program in obese people awaiting bariatric surgery: A randomized controlled study. Complement. Ther. Clin. Pract. 2021, 43, 101342. [Google Scholar] [CrossRef]
- Bellicha, A.; van Baak, M.A.; Battista, F.; Beaulieu, K.; Blundell, J.E.; Busetto, L.; Carraça, E.V.; Dicker, D.; Encantado, J.; Ermolao, A.; et al. Effect of exercise training before and after bariatric surgery: A systematic review and meta-analysis. Obes. Rev. 2021, 22 (Suppl. 4), e13296. [Google Scholar] [CrossRef]
- Pouwels, S.; Wit, M.; Teijink, J.A.; Nienhuijs, S.W. Aspects of Exercise before or after Bariatric Surgery: A Systematic Review. Obes. Facts 2015, 8, 132–146. [Google Scholar] [CrossRef]
- O’Donoghue, G.; Blake, C.; Cunningham, C.; Lennon, O.; Perrotta, C. What exercise prescription is optimal to improve body composition and cardiorespiratory fitness in adults living with obesity? A network meta-analysis. Obes. Rev. 2021, 22, e13137. [Google Scholar] [CrossRef]
- Golbidi, S.; Mesdaghinia, A.; Laher, I. Exercise in the metabolic syndrome. Oxid. Med. Cell. Longev. 2012, 2012, 349710. [Google Scholar] [CrossRef] [PubMed]
- Morrison, M.C.; Kleemann, R. Role of Macrophage Migration Inhibitory Factor in Obesity, Insulin Resistance, Type 2 Diabetes, and Associated Hepatic Co-Morbidities: A Comprehensive Review of Human and Rodent Studies. Front. Immunol. 2015, 6, 308. [Google Scholar] [CrossRef] [PubMed]
- Liñán, Á.C.; Sánchez-Oliver, A.J.; Reina, I.G.; Carmona, W.S.; González-Jurado, J.A. Erddef. Ejercicio físico, obesidad e inflamación. EmásF Rev. Digit. Educ. Física 2016, 41, 65–82. [Google Scholar]
- Lundby, C.; Jacobs, R.A. Adaptations of skeletal muscle mitochondria to exercise training. Exp. Physiol. 2016, 101, 17–22. [Google Scholar] [CrossRef]
- Carraça, E.V.; Encantado, J.; Battista, F.; Beaulieu, K.; Blundell, J.E.; Busetto, L.; van Baak, M.; Dicker, D.; Ermolao, A.; Farpour-Lambert, N.; et al. Effect of exercise training on psychological outcomes in adults with overweight or obesity: A systematic review and meta-analysis. Obes. Rev. 2021, 22 (Suppl. 4), e13261. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| [18] Arman et al. (2021) | |
|---|---|
| Randomization | Software Stratified by Sex and Age Was Used. |
| Participants | 21 participants: 1 man—20 women. Institution: Rehabilitation and Physical Therapy Department, Health Sciences Department, Istanbul University-Cerrahpasa. Country: Turkey. Inclusion criteria: candidates to a BS, 18 years or older, both sexes. Exclusion criteria: participants with comorbidities that prevent their participation in the prehabilitation program like the existence of acute pain, cardiac pain or a previous dolor heart attack, cardiac failure, diabetes, or uncompensated hypertension. |
| Intervention | Program of the institution: 1. Warm-up (10–15 min): walk was performed on a treadmill; heart rate was monitored with a pulse oximeter and as a goal it was set at 50 to 60 heartbeats. 2. Load (30–45 min): exercises for core stabilization were progressively performed in supine position, long sitting position, knee position, crawling position, foot over one leg position and sitting on a ball as exercise. Involved a combination of strengthening, resistance, and balance exercises, along with breathing. Exercises for each main muscle group were performed during 2 cycles of 7 and 10 repetitions at a moderate intensity of 50% of maximum repetition. As sessions progressed the number and intensity of exercises were gradually increased. 3. Cool down (10 min): stretching large muscle groups like hamstrings, hip flexors, shoulder muscles, etc. Total days of training: 16. Duration of intervention: 8 weeks. Frequency per week: 2 times. Load adjustment: not detailed in the text. |
| Outcome measurements | 1. Body composition: BMI, fat mass in kg, fat mass in %, free fat mass in kg. (Bioelectrical impedance analysis). 2. Functional capacity: 6MWT, chair stand test, postural stability test, abdominal strength, core flexor strength, modified push up test. 3. Quality of life: OSQOL. 4. Surgical objectives: not studied in the research. |
| Global risk bias | Uncertain. |
| [11] Baillot et al. (2016) | |
| Randomization | Used software stratified by sex and maximum aerobic capacity (> o ≤ 7 MET). |
| Participants | 29 participants: 7 men—22 women. Institution: Centre hospitalier universitaire de Sherbrooke (CHUS), Quebec. Country: Canada. Inclusion criteria: candidates to BS, 18 years old or older, both sexes. Exclusion criteria: participants with comorbidities that prevent their participation in the prehabilitation program like a medical contraindication to practice physical activity, functional limitations that do not allow them to perform the 6MWT, not understanding the French language, or decompensated neuro-psychiatric pathology. |
| Intervention | Gym program: 1. Warm-up (10 min). 2. Aerobic phase: 30 min of exercise (treadmill, walking circuit, arm ergometer, elliptical machine) 3. Resistance phase: 20 to 30 min. 4. Cool down: 10 min. Total days of training: 24. Intervention duration: 12 weeks. Frequency per week: 2 times. Load adjustment: Aerobic: according to HRR from 55 to 75/80%. 8 levels were determined: A: 55%, B: 55%, C: 55%, D: 55%/65%, E: 65%, F: 65%/75%, G: 75% and H: 75%/85%. The duration was of 24 min at an A level and 30 min during rest. Resistance: increased from 2 to 3 sets, from 12 to 15 repetitions and at a weight of 5 to 12 lbs. for men, and 2 to 10 lbs. for women. |
| Outcome measurements | 1. Body composition: BMI, fat mass in %. (Bioelectrical impedance analysis). 2. Functional capacity: 6MWT, chair stand test, half squat test, arm curl test. 3. Quality of life: WRQOL. 4. Surgical objectives: not studied in the research. |
| Global risk bias | High. |
| [15] Baillot et al. (2018) | |
| Randomization | Used software stratified by sex and maximum aerobic capacity (> o ≤ 7 MET). |
| Participants | 25 participants: 5 men—20 women. Institution: Centre hospitalier universitaire de Sherbrooke (CHUS), Quebec. Country: Canada. Inclusion criteria: candidates to a BS, 18-year-old or older, both sexes. Exclusion criteria: participants with comorbidities that prevent their participation in the prehabilitation program like a medical contraindication to practice physical activity, functional limitations that do not allow them to perform the 6MWT, not understanding the French language, or decompensated neuro-psychiatric pathology. |
| Intervention | Gym program: 1. Warm up: 10 min. 2. Aerobic phase: 30 min of exercise on the treadmill, walking circuit, arm ergometer, elliptical machine, aerobic dance. 3. Resistance phase: 20 to 30 min with small equipment, elastic bands, medicine balls, dumbbells, sticks. 4. Cool down: 10 min. Total days of training: 36. Intervention duration: 12 weeks. Frequency per week: 3 times. Load adjustment: Aerobic: according to a HRR from 55 to 75/80% (there are no more details in the article). |
| Outcome measurements | 1. Body composition: BMI, free fat mass in %. (Bioelectrical impedance analysis). 2. Functional capacity: 6MWT, half squat test. 3. Quality of life: WRQOL. 4. Surgical objectives: not studied in the research. |
| Global risk bias | Uncertain. |
| [16] Funderburk et al. (2010) | |
| Randomization | Unexplained. |
| Participants | 7 participants: 1 man, 6 women. Institution: Hospital Pitt County Memorial, Rehabilitation center, Greenville. Country: United States of America. Inclusion criteria: candidates to a BS, 18 years old or older, both sexes. Exclusion criteria: no reports in the article. |
| Intervention | Program of the institution: The program included a warmup with exercises (walking in the water), strength and resistance exercises, and Ai Chi exercises for balance, core strengthening, and relaxation. Ai Chi is an aquatic exercise that was designed to increase relaxation, range of motion, and mobility. It is performed standing with the water at shoulder level using a combination of deep breathing and complete slow movements of the lower and superior extremities, as well as the torso. (There are no more details in the article). Total days of training: 24. Intervention duration: 12 weeks. Frequency per week: 2 times. Load adjustment: not detailed in the article. |
| Outcome measurements | 1. Body composition: not studied in the article. 2. Functional capacity: 6MWT, chair stand test, postural stability test, abdominal strength, core flexor strength, modified push up test. 3. Quality of life: SF 36. 4. Surgical objectives: not studied in the research. |
| Global risk bias | Uncertain. |
| [17] Marcon et al. (2017) | |
| Randomization | In blocks of 12 participants. |
| Participants | 57 participants: 6 men—51 women. Institution: Hospital de Clinicas de Porto Alegre, Porto Alegre. Country: Brazil. Inclusion criteria: candidates to a BS, 18 years old or older, both sexes. Exclusion criteria: participants with comorbidities that prevent their participation in the prehabilitation program, participating in another supervised exercise program, patients with a class III or IV of heart functional capacity, orthopedic problems, severe retinopathy, severe neuropathy, drug addiction, severe mental illness, severe metabolic decompensation (250 mg/DI of blood glucose, systolic pressure over 200 mmHg, diastolic pressure over 100 mmHG). |
| Intervention | Gym program: Included aerobic exercise and stretching, intensity was measured by Borg’s scale, using a range between 2 to 4, considering it low to moderate intensity respectively. Arm and leg movements were alternated, moving to simulate walking. Stretching included: arms, legs, torso, and neck for 6 min after the aerobic phase in each session. (There are no more details in the article). Total days of training: 32. Intervention duration: 16 weeks. Frequency per week: 2 times. Load adjustment: not detailed in the article. |
| Outcome measurements | 1.- Body composition: BMI. (Bioelectrical impedance analysis) 2.- Functional capacity: 6MWT, VO2 max from equations after the test. 3.- Quality of life: not studied in the research. 4.- Surgical objectives: not studied in the research. |
| Global risk bias | Uncertain. |
| Certainty Assessment | No. of Patients | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Aerobic Physical Exercise, Resistance or Both | Standard Care (no Exercise) | Relative (95% CI) | Absolute (95% CI) | |
| 4 | randomised trials | Serious a | Serious b | not serious | Serious c | none | 54 | 61 | - | SMD 0.71 SD fewer (1.55 fewer to 0.12 more) | ⨁◯◯◯ Very low |
| 3 | randomised trials | Serious d | not serious | not serious | not serious | none | 39 | 36 | - | SMD 0.38 SD more (0.47 fewer to 1.85 more) | ⨁⨁⨁◯ Moderate |
| 2 | randomised trials | Serious e | not serious | not serious | not serious | none | 24 | 22 | - | SMD 0.41 SD fewer (1 fewer to 0.18 more) | ⨁⨁⨁◯ Moderate |
| Certainty Assessment | No. of Patients | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Aerobic Physical Exercise, Resistance or Both | Standard Care (no Exercise) | Relative (95% CI) | Absolute (95% CI) | |
| 2 | randomised trials | not serious | not serious | not serious | not serious | none | 33 | 28 | - | SMD 2.59 SD more (1.89 more to 3.3 more) | ⨁⨁⨁⨁ High |
| Certainty Assessment | No. of Patients | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Aerobic Physical Exercise, Resistance or Both | Standard Care (no Exercise | Relative (95% CI) | Absolute (95% CI) | |
| 3 | randomised trials | seriousa | not serious | not serious | not serious | none | 28 | 25 | - | SMD 0.88 SD more (0.23 fewer to 1.99 more) | ⨁⨁⨁◯ Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrera-Santelices, A.; Argüello-Florencio, G.; Westphal, G.; Nardo Junior, N.; Zamunér, A.R. Effects of Supervised Physical Exercise as Prehabilitation on Body Composition, Functional Capacity and Quality of Life in Bariatric Surgery Candidates: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 5091. https://doi.org/10.3390/jcm11175091
Herrera-Santelices A, Argüello-Florencio G, Westphal G, Nardo Junior N, Zamunér AR. Effects of Supervised Physical Exercise as Prehabilitation on Body Composition, Functional Capacity and Quality of Life in Bariatric Surgery Candidates: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(17):5091. https://doi.org/10.3390/jcm11175091
Chicago/Turabian StyleHerrera-Santelices, Andrea, Graciela Argüello-Florencio, Greice Westphal, Nelson Nardo Junior, and Antonio Roberto Zamunér. 2022. "Effects of Supervised Physical Exercise as Prehabilitation on Body Composition, Functional Capacity and Quality of Life in Bariatric Surgery Candidates: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 17: 5091. https://doi.org/10.3390/jcm11175091
APA StyleHerrera-Santelices, A., Argüello-Florencio, G., Westphal, G., Nardo Junior, N., & Zamunér, A. R. (2022). Effects of Supervised Physical Exercise as Prehabilitation on Body Composition, Functional Capacity and Quality of Life in Bariatric Surgery Candidates: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(17), 5091. https://doi.org/10.3390/jcm11175091