
The Association between Acute Myocardial Infarction-Related Outcomes and the Ramadan Period: A Retrospective Population-Based Study

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Setting
2.2. Study Groups and Time Periods
2.3. Data Collection and Variables
2.4. Outcomes
2.5. Statistical Analysis
2.5.1. Incidence
2.5.2. Mortality
2.5.3. Subgroup Analysis
3. Results
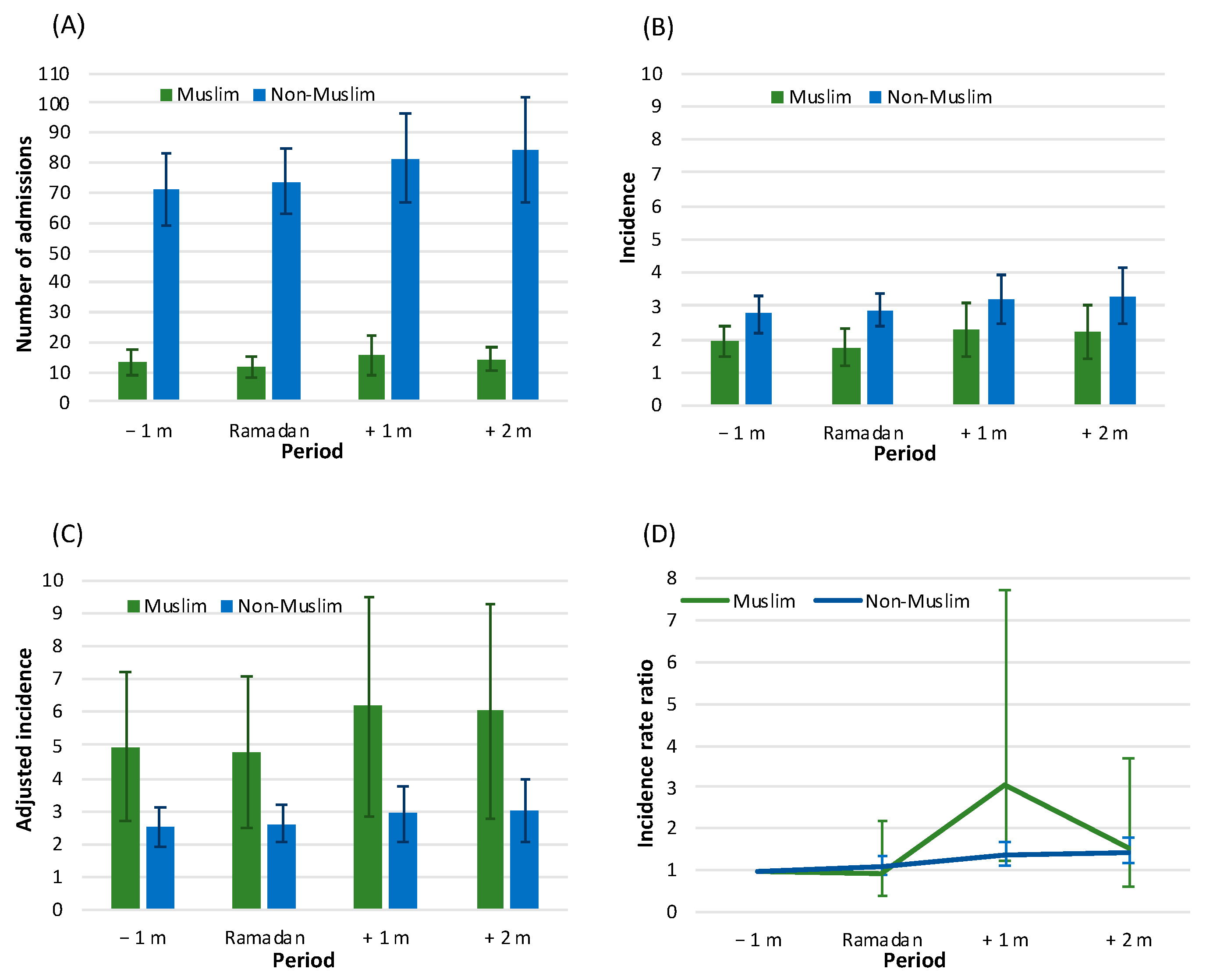
3.1. Incidence
3.2. Baseline Data by Time Period
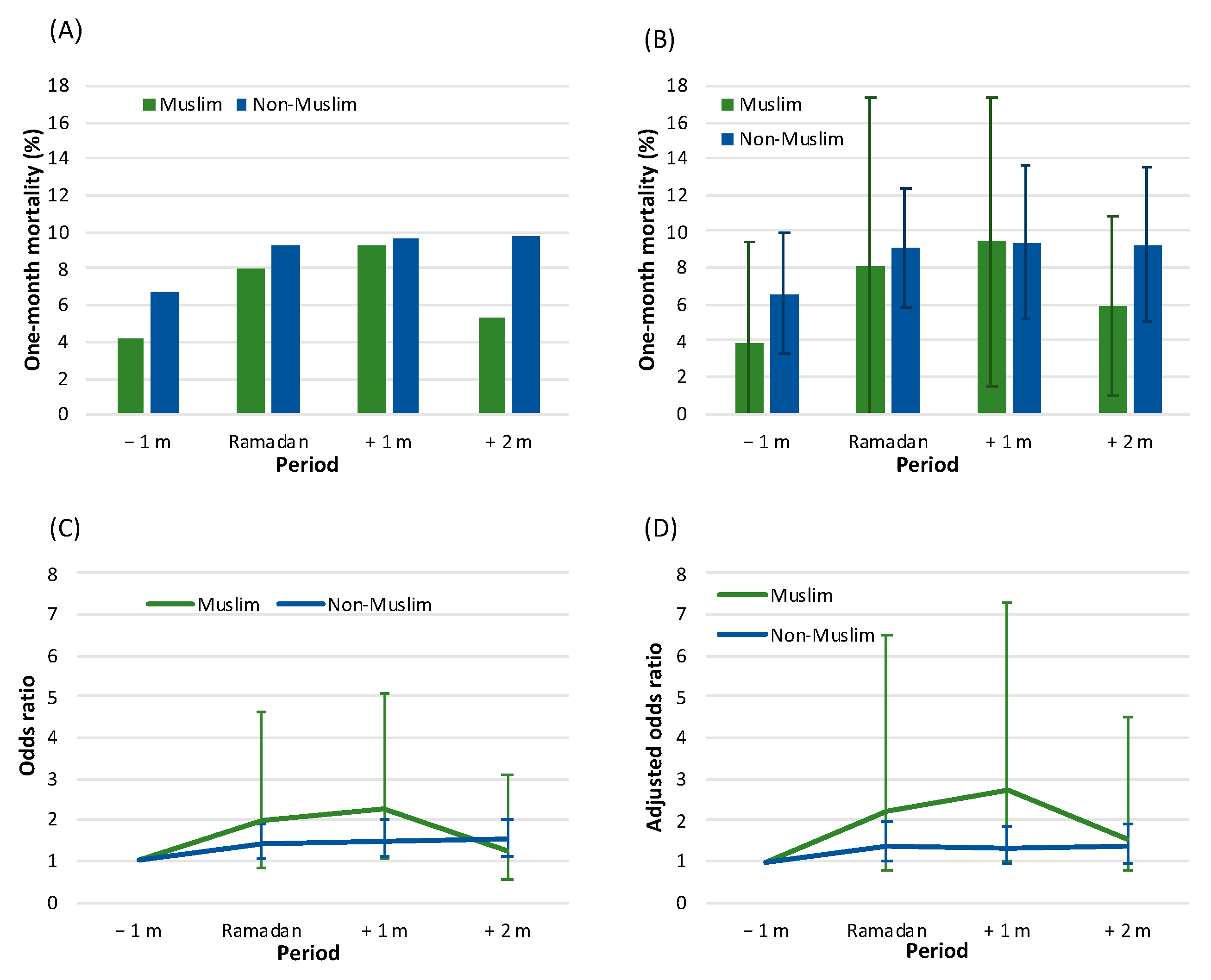
3.3. Mortality by Time Period
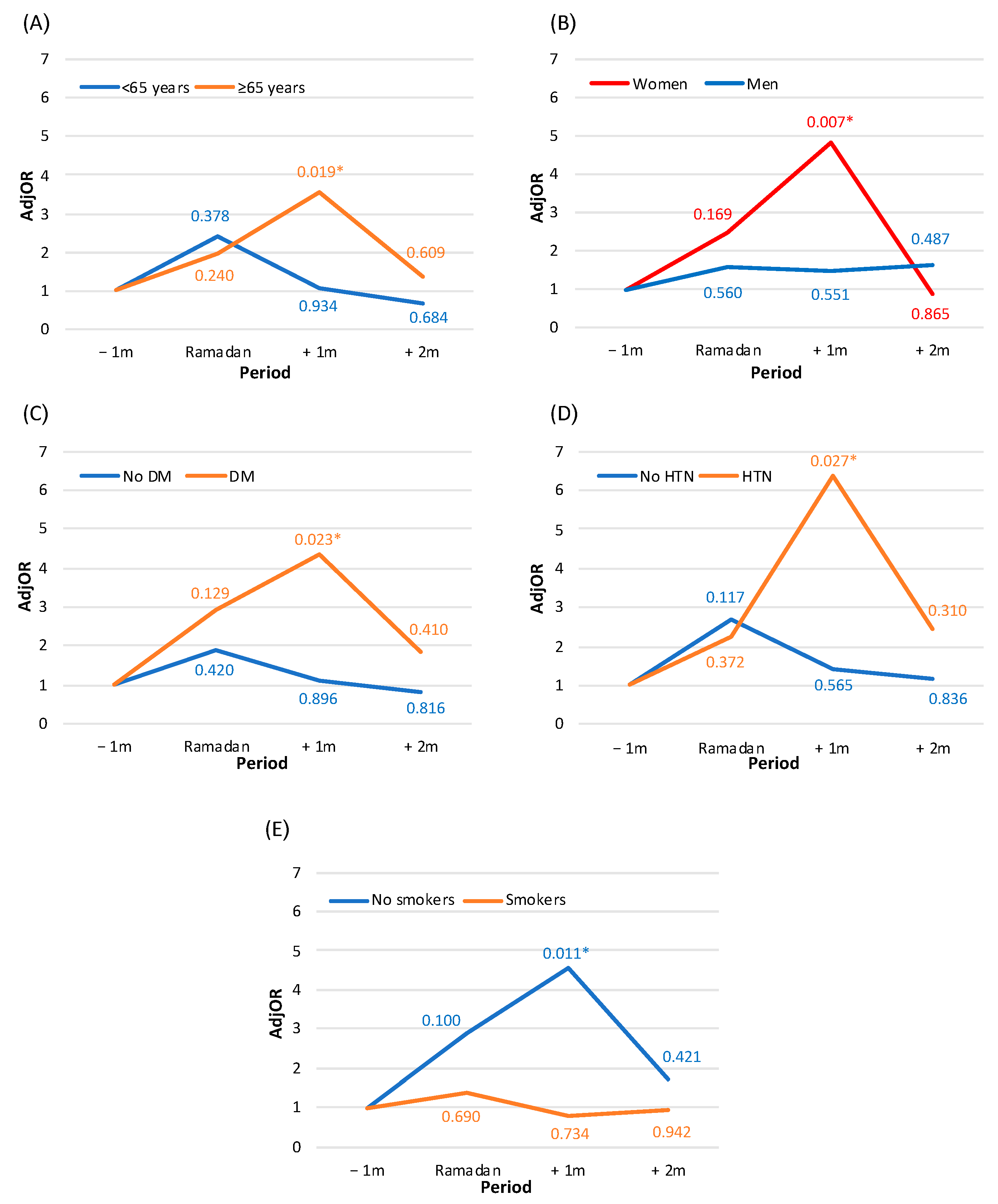
3.4. Subgroup Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reed, G.W.; Rossi, J.E.; Cannon, C.P. Acute myocardial infarction. Lancet 2016, 389, 197–210. [Google Scholar] [CrossRef]
- Yeh, R.W.; Go, A.S. Rethinking the Epidemiology of Acute Myocardial Infarction: Challenges and Opportunities. Arch. Intern. Med. 2010, 170, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Milanlouei, S.; Menichetti, G.; Li, Y.; Loscalzo, J.; Willett, W.C.; Barabási, A. A systematic comprehensive longitudinal evaluation of dietary factors associated with acute myocardial infarction and fatal coronary heart disease. Nat. Commun. 2020, 11, 6074. [Google Scholar] [CrossRef] [PubMed]
- Jamil, G.; Jamil, M.; Alkhazraji, H.; Haque, A.; Chedid, F.; Balasubramanian, M.; Khairallah, B.; Qureshi, A. Risk factor assessment of young patients with acute myocardial infarction. Am. J. Cardiovasc. Dis. 2013, 3, 170–174. Available online: https://www.ncbi.nlm.nih.gov/pubmed/23991352 (accessed on 20 June 2022). [PubMed]
- Lynch, J.; Krause, N.; Kaplan, G.A.; Tuomilehto, J.; Salonen, J.T. Workplace conditions, socioeconomic status, and the risk of mortality and acute myocardial infarction: The Kuopio Ischemic Heart Disease Risk Factor Study. Am. J. Public Health 1997, 87, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Lian, X.; Gu, J.; Wang, S.; Yan, J.; Chen, X.; Wang, M.; Zhang, Y.; Wang, L. Effects of sleep habits on acute myocardial infarction risk and severity of coronary artery disease in Chinese population. BMC Cardiovasc. Disord. 2021, 21, 481. [Google Scholar] [CrossRef] [PubMed]
- Taylor, B.S.; Hammer, S.M. Shifts to and from daylight saving time and incidence of myocardial infarction. N. Engl. J. Med. 2008, 359, 1966–1968. [Google Scholar] [CrossRef]
- Sakr, A.H. Fasting in Islam. J. Am. Diet. Assoc. 1975, 67, 17–21. [Google Scholar]
- Iraki, L.; Bogdan, A.; Hakkou, F.; Amrani, N.; Abkari, A.; Touitou, Y. Ramadan Diet Restrictions Modify the Circadian Time Structure in Humans. A Study on Plasma Gastrin, Insulin, Glucose, and Calcium and on Gastric pH1. J. Clin. Endocrinol. Metab. 1997, 82, 1261–1273. [Google Scholar] [CrossRef]
- Sarraf-Zadegan, N.; Atashi, M.; Naderi, G.A.; Baghai, A.M.; Asgary, S.; Fatehifar, M.R.; Samarian, H.; Zarei, M. The effect of fasting in Ramadan on the values and interrelations between biochemical, coagulation and hematological factors. Ann. Saudi Med. 2000, 20, 377–381. [Google Scholar] [CrossRef]
- Raffee, L.A.; Alawneh, K.Z.; Al Suleiman, M.K.; Ibdah, R.K.; Rawashdeh, S.I.; Al-Mistarehi, A.W. An observational study of the occurrence of acute coronary syndrome (ACS) among jordanian patients: Identifying the influence of Ramadan Fasting. Ann. Med. Surg. 2020, 59, 171–175. [Google Scholar] [CrossRef]
- Chamsi-Pasha, M.; Chamsi-Pasha, H. The cardiac patient in Ramadan. Avicenna J. Med. 2016, 6, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Turin, T.; Ahmed, S.; Shommu, N.; Afzal, A.; Al Mamun, M.; Qasqas, M.; Rumana, N.; Vaska, M.; Berka, N. Ramadan fasting is not usually associated with the risk of cardiovascular events: A systematic review and meta-analysis. J. Fam. Community Med. 2016, 23, 73–81. [Google Scholar] [CrossRef] [PubMed]
- BaHammam, A.S.; Almeneessier, A.S. Recent Evidence on the Impact of Ramadan Diurnal Intermittent Fasting, Mealtime, and Circadian Rhythm on Cardiometabolic Risk: A Review. Front. Nutr. 2020, 7, 28. [Google Scholar] [CrossRef]
- NasrAllah, M.M.; Osman, N.A. Fasting during the month of Ramadan among patients with chronic kidney disease: Renal and cardiovascular outcomes. Clin. Kidney J. 2014, 7, 348–353. [Google Scholar] [CrossRef]
- Berbari, A.E.; Daouk, N.A.; Mallat, S.G.; Jurjus, A.R. Ramadan Fasting in Health and Disease; Special Issues in Hypertension; Springer Milan: Milano, Italy, 2012; pp. 331–346. [Google Scholar]
- Nachvak, S.M.; Pasdar, Y.; Pirsaheb, S.; Darbandi, M.; Niazi, P.; Mostafai, R.; Speakman, J.R. Effects of Ramadan on food intake, glucose homeostasis, lipid profiles and body composition composition. Eur. J. Clin. Nutr. 2019, 73, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Central Bureau of Statistics, Israel. Available online: https://www.cbs.gov.il/he/pages/default.asp (accessed on 14 December 2021).
- Population by Religion and Religiosity. Available online: https://www.cbs.gov.il/en/subjects/Pages/Population-by-Religion-and-Population-Group.aspx (accessed on 21 June 2022).
- Plakht, Y.; Shiyovich, A.; Weitzman, S.; Fraser, D.; Zahger, D.; Gilutz, H. Soroka acute myocardial infarction (SAMI) score predicting 10-year mortality following acute myocardial infarction. Int. J. Cardiol. 2012, 167, 3068–3070. [Google Scholar] [CrossRef]
- Plakht, Y.; Shiyovich, A.; Weitzman, S.; Freaser, D.; Zagher, D.; Gilutz, H. A new risk score predicting 1- and 5-year mortality following acute myocardial infarction Soroka Acute Myocardial Infarction (SAMI) Project. Int. J. Cardiol. 2012, 154, 173–179. [Google Scholar] [CrossRef]
- Pew Research Center. Available online: https://www.pewresearch.org/ (accessed on 16 August 2022).
- Rahman, M.; Rashid, M.; Basher, S.; Sultana, S.; Nomani, M.Z.A. Improved serum HDL cholesterol profile among Bangladeshi male students during Ramadan fasting. East. Mediterr. Health J. 2004, 10, 131–137. [Google Scholar] [CrossRef]
- Kutluhan, S.; Galip, A.; Koyuncuoglu, H.R.; Gultekin, F.; Kumral, E. Diurnal variation of stroke in Ramadan. BioMed Res. 2000, 11, 303–307. [Google Scholar]
- Stokholm, K.H.; Breum, L.; Astrup, A. Cardiac contractility, central haemodynamics and blood pressure regulation during semistarvation. Clin. Physiol. 1991, 11, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Gallucci, G.; Tartarone, A.; Lerose, R.; Lalinga, A.V.; Capobianco, A.M. Cardiovascular risk of smoking and benefits of smoking cessation. J. Thorac. Dis. 2020, 12, 3866–3876. [Google Scholar] [CrossRef]
- Mazidi, M.; Rezaie, P.; Chaudhri, O.; Karimi, E.; Nematy, M. The effect of Ramadan fasting on cardiometabolic risk factors and anthropometrics parameters: A systematic review. Pak. J. Med Sci. 2015, 31, 1250–1255. [Google Scholar] [CrossRef]
- Anjum, S.; Yousuf, S.; Ahmedani, M.Y. Effect of Ramadan fasting on renal function of people with diabetes; a prospective longitudinal study. Diabetes Res. Clin. Pract. 2021, 181, 109090. [Google Scholar] [CrossRef] [PubMed]
- Chinwong, D.; Mookmanee, N.; Chongpornchai, J.; Chinwong, S. A comparison of gender differences in smoking behaviors, intention to quit, and nicotine dependence among Thai university students. J. Addict. 2018, 2018, 8081670. [Google Scholar] [CrossRef]
- Zainudin, S.B.; Abu Bakar, K.N.B.; Abdullah, S.B.; Hussain, A.B. Diabetes education and medication adjustment in Ramadan (DEAR) program prepares for self-management during fasting with tele-health support from pre-Ramadan to post-Ramadan. Ther. Adv. Endocrinol. Metab. 2018, 9, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Temizhan, A.; Dönderici, Ö.; Ouz, D.; Demirbas, B. Is there any effect of Ramadan fasting on acute coronary heart disease events? Int. J. Cardiol. 1999, 70, 149–153. [Google Scholar] [CrossRef]
- Al Suwaidi, J.; Bener, A.; Suliman, A.; Hajar, R.; Salam, A.M.; Numan, M.T.; Al Binali, H.A. A population based study of Ramadan fasting and acute coronary syndromes. Heart 2004, 90, 695–696. [Google Scholar] [CrossRef]
- Plakht, Y.; Gilutz, H.; Shiyovich, A.; Zahger, D.; Weitzman, S. Gender and ethnic disparities in outcome following acute myocardial infarction among Bedouins and Jews in southern Israel. Eur. J. Public Health 2011, 21, 74–80. [Google Scholar] [CrossRef]
- Ibrahim, M.; Davies, M.J.; Ahmad, E.; Annabi, A.F.; Eckel, R.H.; Ba-Essa, E.M.; El Sayed, N.A.; Fischl, A.H.; Houeiss, P.; Iraqi, H.; et al. Recommendations for management of diabetes during Ramadan: Update 2020, applying the principles of the ADA/EASD consensus. BMJ Open Diabetes Res. Care 2020, 8, e001248. [Google Scholar] [CrossRef]
- Beshyah, A.S.; Beshyah, S.A. The incidence of diabetic ketoacidosis during Ramadan fasting: A 10-year single-centre retrospective study. Diabetes Res. Clin. Pract. 2019, 150, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Raveendran, A.V.; Zargar, A.H. Diabetes control during Ramadan fasting. Clevel. Clin. J. Med. 2017, 84, 352–356. [Google Scholar] [CrossRef]
- Chen, L.; Yang, G. Recent advances in circadian rhythms in cardiovascular system. Front. Pharmacol. 2015, 6, 71. [Google Scholar] [CrossRef] [PubMed]
- Adawi, M.; Watad, A.; Brown, S.; Aazza, K.; Aazza, H.; Zouhir, M.; Sharif, K.; Ghanayem, K.; Farah, R.; Mahagna, H.; et al. Ramadan fasting exerts immunomodulatory effects: Insights from a systematic review. Front. Immunol. 2017, 8, 1144. [Google Scholar] [CrossRef]
- Medina-Ramón, M.; Zanobetti, A.; Cavanagh, D.P.; Schwartz, J. Extreme temperatures and mortality: Assessing effect modification by personal characteristics and specific cause of death in a multi-city case-only analysis. Environ. Health Perspect. 2006, 114, 1331–1336. [Google Scholar] [CrossRef] [PubMed]
- Morabito, M.; Modesti, P.A.; Cecchi, L.; Crisci, A.; Orlandini, S.; Maracchi, G.; Gensini, G.F. Relationships between weather and myocardial infarction: A biometeorological approach. Int. J. Cardiol. 2005, 105, 288–293. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| −1 m | Ramadan | +1 m | +2 m | Total | p | |
|---|---|---|---|---|---|---|
| N | 213 | 187 | 250 | 227 | 877 | |
| Demographics | ||||||
| Age (years), Mean (SD) | 58.48 (14.64) | 62.10 (14.91) | 60.79 (13.82) | 61.96 (13.79) | 60.81 (14.30) | 0.034 |
| 65–75 | 35 (16.4) | 42 (22.5) | 57 (22.8) | 62 (27.3) | 196 (22.3) | 0.064 |
| ≥75 | 31 (14.6) | 35 (18.7) | 35 (14.0) | 40 (17.6) | 141 (16.1) | |
| Sex, Males | 158 (74.2) | 135 (72.2) | 187 (74.8) | 157 (69.2) | 637 (72.6) | 0.524 |
| Cardiac diseases | ||||||
| Cardiomegaly | 21 (9.9) | 25 (13.4) | 30 (12.0) | 37 (16.3) | 113 (12.9) | 0.230 |
| Supraventricular arrhythmias | 23 (10.8) | 29 (15.5) | 33 (13.2) | 31 (13.7) | 116 (13.2) | 0.577 |
| CHF | 36 (16.9) | 38 (20.3) | 53 (21.2) | 49 (21.6) | 176 (20.1) | 0.601 |
| Pulmonary heart disease | 14 (6.6) | 24 (12.8) | 20 (8.0) | 30 (13.2) | 88 (10.0) | 0.043 |
| CIHD | 184 (86.4) | 159 (85.0) | 217 (86.8) | 195 (85.9) | 755 (86.1) | 0.959 |
| Cardiovascular risk factors | ||||||
| Renal diseases | 18 (8.5) | 22 (11.8) | 26 (10.4) | 25 (11.0) | 91 (10.4) | 0.721 |
| Diabetes mellitus | 98 (46.0) | 100 (53.5) | 124 (49.6) | 122 (53.7) | 444 (50.6) | 0.332 |
| Dyslipidemia | 154 (72.3) | 133 (71.1) | 175 (70.0) | 166 (73.1) | 628 (71.6) | 0.885 |
| Hypertension | 99 (46.5) | 100 (53.5) | 120 (48.0) | 118 (52.0) | 437 (49.8) | 0.439 |
| Obesity | 45 (21.1) | 44 (23.5) | 39 (15.6) | 51 (22.5) | 179 (20.4) | 0.149 |
| Smoking | 139 (65.3) | 113 (60.4) | 165 (66.0) | 124 (54.6) | 541 (61.7) | 0.045 |
| PVD | 16 (7.5) | 18 (9.6) | 20 (8.0) | 12 (5.3) | 66 (7.5) | 0.407 |
| Family history of IHD | 19 (8.9) | 12 (6.4) | 23 (9.2) | 18 (7.9) | 72 (8.2) | 0.732 |
| Other disorders | ||||||
| COPD | 35 (16.4) | 38 (20.3) | 48 (19.2) | 53 (23.3) | 174 (19.8) | 0.333 |
| Neurological disorders | 23 (10.8) | 24 (12.8) | 29 (11.6) | 27 (11.9) | 103 (11.7) | 0.939 |
| Malignancy | 5 (2.3) | 3 (1.6) | 5 (2.0) | 5 (2.2) | 18 (2.1) | 0.959 |
| Anemia | 70 (32.9) | 67 (35.8) | 87 (34.8) | 93 (41.0) | 317 (36.1) | 0.323 |
| GI bleeding | 4 (1.9) | 4 (2.1) | 3 (1.2) | 4 (1.8) | 15 (1.7) | 0.889 |
| Schizophrenia/psychosis | 4 (1.9) | 3 (1.6) | 3 (1.2) | 3 (1.3) | 13 (1.5) | 0.935 |
| Alcohol/drug addiction | 2 (0.9) | 0 (0) | 2 (0.8) | 4 (1.8) | 8 (0.9) | 0.312 |
| History of malignancy | 0 (0) | 5 (2.7) | 1 (0.4) | 4 (1.8) | 10 (1.1) | 0.039 |
| Administrative characteristics of the hospitalization | ||||||
| LOS, >7 days | 85 (39.9) | 83 (44.4) | 102 (40.8) | 75 (33.0) | 345 (39.3) | 0.111 |
| STEMI | 106 (49.8) | 76 (40.6) | 123 (49.2) | 100 (44.1) | 405 (46.2) | 0.192 |
| Results of echocardiography | ||||||
| Echocardiography performance | 160 (75.1) | 133 (71.1) | 166 (66.4) | 167 (73.6) | 626 (71.4) | 0.170 |
| Severe LV dysfunction | 19 (11.9) | 15 (11.3) | 28 (16.9) | 26 (15.6) | 88 (14.1) | 0.410 |
| LV hypertrophy | 9 (5.6) | 7 (5.3) | 9 (5.4) | 6 (3.6) | 31 (5.0) | 0.822 |
| Mitral regurgitation | 9 (5.6) | 9 (6.8) | 8 (4.8) | 18 (10.8) | 44 (7.0) | 0.149 |
| Tricuspid regurgitation | 3 (1.9) | 5 (3.8) | 5 (3.0) | 8 (4.8) | 21 (3.4) | 0.518 |
| Pulmonary hypertension | 5 (3.1) | 12 (9) | 7 (4.2) | 11 (6.6) | 35 (5.6) | 0.126 |
| Results of angiography | ||||||
| Angiography performance | 154 (72.3) | 119 (63.6) | 164 (65.6) | 153 (67.4) | 590 (67.3) | 0.274 |
| Measure of CAD, no or non-significant | 9 (5.8) | 6 (5.0) | 5 (3.0) | 6 (3.9) | 26 (4.4) | 0.618 |
| One vessel | 43 (27.9) | 36 (30.3) | 55 (33.5) | 52 (34.0) | 186 (31.5) | |
| Two vessels | 51 (33.1) | 38 (31.9) | 43 (26.2) | 53 (34.6) | 185 (31.4) | |
| Three vessels/LM | 51 (33.1) | 39 (32.8) | 61 (37.2) | 42 (27.5) | 193 (32.7) | |
| Type of treatment | ||||||
| Noninvasive | 45 (21.1) | 57 (30.5) | 61 (24.4) | 53 (23.3) | 216 (24.6) | 0.164 |
| PCI | 147 (69.0) | 116 (62.0) | 159 (63.6) | 158 (69.6) | 580 (66.1) | |
| CABG | 21 (9.9) | 14 (7.5) | 30 (12.0) | 16 (7.0) | 81 (9.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Betesh-Abay, B.; Shiyovich, A.; Davidian, S.; Gilutz, H.; Shalata, W.; Plakht, Y. The Association between Acute Myocardial Infarction-Related Outcomes and the Ramadan Period: A Retrospective Population-Based Study. J. Clin. Med. 2022, 11, 5145. https://doi.org/10.3390/jcm11175145
Betesh-Abay B, Shiyovich A, Davidian S, Gilutz H, Shalata W, Plakht Y. The Association between Acute Myocardial Infarction-Related Outcomes and the Ramadan Period: A Retrospective Population-Based Study. Journal of Clinical Medicine. 2022; 11(17):5145. https://doi.org/10.3390/jcm11175145
Chicago/Turabian StyleBetesh-Abay, Batya, Arthur Shiyovich, Shani Davidian, Harel Gilutz, Walid Shalata, and Ygal Plakht. 2022. "The Association between Acute Myocardial Infarction-Related Outcomes and the Ramadan Period: A Retrospective Population-Based Study" Journal of Clinical Medicine 11, no. 17: 5145. https://doi.org/10.3390/jcm11175145
APA StyleBetesh-Abay, B., Shiyovich, A., Davidian, S., Gilutz, H., Shalata, W., & Plakht, Y. (2022). The Association between Acute Myocardial Infarction-Related Outcomes and the Ramadan Period: A Retrospective Population-Based Study. Journal of Clinical Medicine, 11(17), 5145. https://doi.org/10.3390/jcm11175145