

Effect of High-Intensity Strength and Endurance Training in the Form of Small Circuits on Changes in Lipid Levels in Men Aged 35–40 Years

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
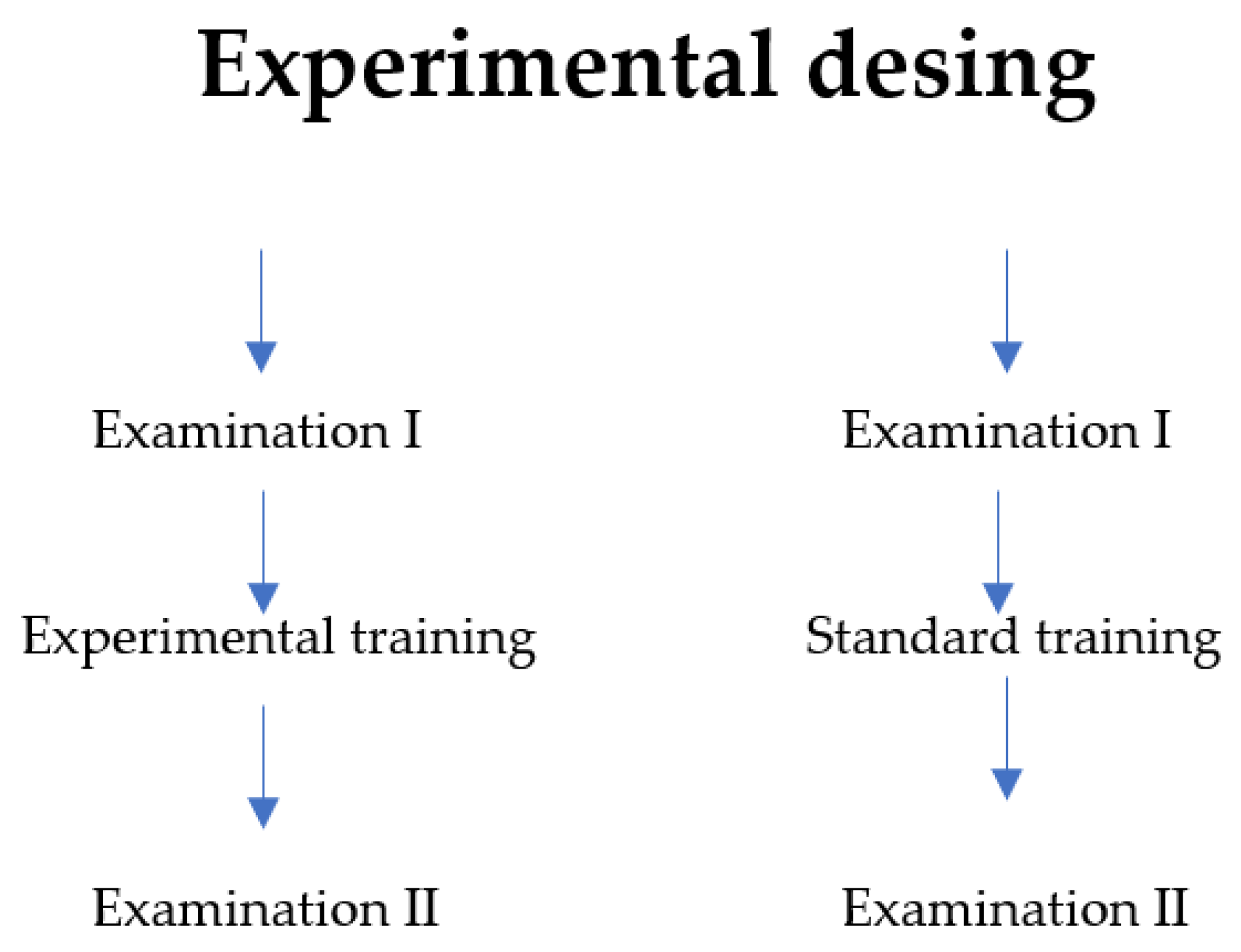
2.2. Research Program and Methodology
2.3. Description of the Exercises Included in the Experimental Program
- strength conditioning circuit (using barbells, dumbbells, and kettlebells);
- general fitness circuit (cardio exercises such as plyometrics and coordination exercises);
- functional fitness circuit (exercises involving muscle parts most commonly used in activities of daily living).
2.4. Statistical Analysis
3. Results
4. Discussion
Limitation of the Study
5. Conclusions
Practical Implication
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carrera-Bastos, P.; Fontes-Villalba, M.; O’Keefe, J.H.; Lindeberg, S.; Cordain, L. The western diet and lifestyle and diseases of civilization. Res. Rep. Clin. Cardiol. 2011, 2, 15–35. [Google Scholar] [CrossRef]
- Kopp, W. How Western Diet And Lifestyle Drive The Pandemic Of Obesity And Civilization Diseases. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2221–2236. [Google Scholar] [CrossRef]
- Esgin, T.; Hersh, D.; Rowley, K.G.; Macniven, R.; Glenister, K.; Crouch, A.; Newton, R.U. Physical Activity and Self-Reported Metabolic Syndrome Risk Factors in the Aboriginal Population in Perth, Australia, Measured Using an Adaptation of the Global Physical Activity Questionnaire (GPAQ). Int. J. Environ. Res. Pub Health. 2021, 18, 5969. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, P.L.; Carrera-Bastos, P.; Gálvez, B.G.; Ruiz-Hurtado, G.; Ordovas, J.M.; Ruilope, L.M.; Lucia, A. Lifestyle interventions for the prevention and treatment of hypertension. Nat. Rev. Cardiol. 2021, 18, 251–275. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during COVID-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- Yang, S.; Guo, B.; Ao, L.; Yang, C.; Zhang, L.; Zhou, J.; Jia, P. Obesity and activity patterns before and during COVID-19 lockdown among youths in China. Clin. Obes. 2020, 10, e12416. [Google Scholar] [CrossRef] [PubMed]
- Martinez-de-Quel, Ó.; Suárez-Iglesias, D.; López-Flores, M.; Pérez, C.A. Physical activity, dietary habits and sleep quality before and during COVID-19 lockdown; A longitudinal study. Appetite 2021, 158, 105019. [Google Scholar] [CrossRef]
- Howley, E.T.; Franks, B.D. Health/Fitness Instructor’s Handbook; Hum Kin Publishers: Champaign, IL, USA, 1986; ISBN 0-87322-064-1. [Google Scholar]
- Skinner, J.S.; Oja, P. Laboratory and field tests for assessing health-related fitness. In Physical Activity, Fitness and Health; Bouchard, C., Shephard, R.J., Eds.; Human Kinetics: Champaign, IL, USA, 1994. [Google Scholar]
- Suni, J.H.; Miilunpalo, A.I.; Asikainen, T.-M.; Laukkanen, R.T.; Oja, P.; Pasanen, M.E.; Bös, K.; Vuori, I.M. Safety and Feasibility of Health-Related Fitness Test Battery for Adults. Phys. Ther. 1998, 78, 134–148. [Google Scholar] [CrossRef]
- Brunzell, J.D.; Davidson, M.; Furberg, C.D.; Goldberg, R.B.; Howard, B.V.; Stein, J.H.; Witztum, J.L. Lipoprotein Management in Patients with Cardiometabolic Risk: Consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care 2008, 31, 811–822. [Google Scholar] [CrossRef]
- Zhong, V.W.; Van Horn, L.; Cornelis, M.C.; Wilkins, J.T.; Ning, H.; Carnethon, M.R.; Greenland, P.; Mentz, R.J.; Tucker, K.L.; Zhao, L.; et al. Associations of Dietary Cholesterol or Egg Consumption with Incident Cardiovascular Disease and Mortality. JAMA 2019, 321, 1081. [Google Scholar] [CrossRef]
- Finegold, J.A.; Asaria, P.; Francis, D.P. Mortality from ischaemic heart disease by country, region, and age: Statistics from World Health Organisation and United Nations. Int. J. Cardiol. 2013, 168, 934–945. [Google Scholar] [CrossRef] [PubMed]
- Frost, P.H.; Havel, R.J. Rationale for use of non-high-density lipoprotein cholesterol as a tool for lipoprotein cholesterol screening and assessment of risk and therapy. Am. J. Cardiol. 1998, 81, 26B–31B. [Google Scholar] [CrossRef]
- Blaha, M.J.; Blumenthal, R.S.; Brinton, E.A.; Jacobson, T.A. On behalf of the National Lipid Association Taskforce on Non-HDL Cholesterol. J. Clin. Lip. 2008, 2, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Arima, H.; Fujiyoshi, A.; Miura, K.; Takashima, N.; Ohkubo, T.; Kadota, A.; Hayakawa, T.; Kita, Y.; Miyagawa, N.; et al. Relationship between non-high-density lipoprotein cholesterol and the long-term mortality of cardiovascular diseases: NIPPON DATA 90. Int. J. Cardiol. 2016, 220, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, X.; Pan, B.; Jin, X.; Yao, H.; Chen, B.; Zou, Y.; Ge, J.; Chen, H. A modified formula for calculation low-density lipoprotein cholesterol values. Lipids Health Dis. 2010, 9, 52. [Google Scholar] [CrossRef]
- Tighle, D.A.; Ockene, I.S.; Reed, G.; Nicolosi, R. Calculated low density lipoprotein cholesterol levels frequently underestimate directly measured low density lipoprotein cholesterol determination in patients with serum triglyceride levels ≤4.52 mmol/L: An analysis comparing the LipiDirect magnetic LDL assay with the Friedewald calculation. Clin. Chem. Acta 2006, 365, 236–242. [Google Scholar] [CrossRef]
- Sampson, M.; Ling, C.; Sun, Q.; Harb, R.; Ashmaig, M.; Warnic, R.; Sethi, A.; Fleming, J.L.; Otvos, J.D.; Meehausen, J.W.; et al. A New Equation for Calculation of Low-Density Lipoprotein Cholesterol in Patients with Normolipidemia and/or Hypertrigliceridemia. JAMA Cardiol. 2020, 5, 540–554. [Google Scholar] [CrossRef]
- Duncan, M.S.; Vasan, R.S.; Xanthakis, V. Trajectories of blood lipid concentrations over the adult life course and risk of cardiovascular disease and all-cause mortality: Observations from the Framingham Study over 35 years. J. Am Heart Assoc. 2019, 8, e011433. [Google Scholar] [CrossRef]
- Majerczak, J.; Grandys, M.; Frołow, M.; Szkutnik, Z.; Zakrzewska, A.; Niżankowski, R.; Duda, K.; Chłopicki, S.; Żołądź, J.A. Age-dependent impairment in endothelial function and arterial stiffness in former high class male athletes is no different to that in men with no history of physical training. J. Am. Heart Assoc. 2019, 8, e012670. [Google Scholar] [CrossRef]
- Yi, S.-W.; Yi, J.-J.; Ohn, H. Total cholesterol and all-cause mortality by sex and age: A prospective cohort study among 12.8 million adults. Sci. Rep. 2019, 9, 1596. [Google Scholar] [CrossRef] [PubMed]
- Benn, M.; Tybjaerg-Hansen, A.; Nordestgaard, B.G. Low LDL cholesterol by PCSK variation reduces cardiovascular mortality. J. Am. Coll. Cardiol. 2019, 73, 24. [Google Scholar] [CrossRef] [PubMed]
- Maciejewska-Skrendo, A.; Buryta, M.; Czarny, W.; Król, P.; Spieszny, M.; Stastny, P.; Petr, M.; Safranow, K.; Sawczuk, M. The polymorphism of the peroxisome-proliferator activated receptors’ alfa gene modify the aerobic training induced changes of cholesterol and glucose. J. Clin. Med. 2019, 8, 1043. [Google Scholar] [CrossRef] [PubMed]
- de Roos, N.M.; Bots, M.L.; Katan, M.B. Replacement of dietary saturated fatty acids by trans fatty acids lowers serum HDL cholesterol and impairs endothelial function in healthy men and women. Arteri. Thromb. Vasc. Biol. 2001, 21, 1233–1237. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-L.; Ndi Nifor, O.; Ho, C.-C.; Lee, K.-J.; Lu, W.-Y.; Lung, C.-C.; Tantoh, D.M.; Hsu, S.-Y.; Chou, M.-C.; Liaw, Y.-P. Combination of Exercise and Vegetarian diet: Relationship with High Density-Lipoprotein Cholesterol in Taiwanese Adults Based on MTHFR rs1801133 Polymorphism. Nutrients 2020, 12, 1564. [Google Scholar] [CrossRef]
- Huang, Y.-W.; Jian, Z.-H.; Chang, H.-C.; Ndi Nfor, O.; Ko, P.-C.; Lung, C.-C.; Lin, L.-Y.; Ho, C.-C.; Chiang, Y.-C.; Liaw, Y.-P. Vegan diet and blood lipid profiles: A cross-sectional study of pre and postmenopausal women. BMC Women’s Health 2014, 14, 55. [Google Scholar] [CrossRef]
- Haskell, W.L.; Lee, I.-M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical Activity and Public Health. Med. Sci. Sport. Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults. Med. Sci. Sport. Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Gielen, S.; Laughlin, M.H.; O’Conner, C.; Duncker, D.J. Exercise Training in Patients with Heart Disease: Review of Beneficial Effects and Clinical Recommendations. Prog. Cardiovasc. Dis. 2015, 57, 347–355. [Google Scholar] [CrossRef]
- Kraus, W.E.; Houmard, J.A.; Duscha, B.D.; Knetzger, K.J.; Wharton, M.B.; McCartney, J.S.; Bales, C.W.; Henes, S.; Samsa, G.P.; Otvos, J.D.; et al. Effects of the Amount and Intensity of Exercise on Plasma Lipoproteins. N. Engl. J. Med. 2002, 347, 1483–1492. [Google Scholar] [CrossRef]
- Slentz, C.A.; Houmard, J.A.; Johnson, J.L.; Bateman, L.A.; Tanner, C.J.; McCartney, J.S.; Duscha, B.D.; Kraus, W.E. Inactivity, exercise training and detraining, and plasma lipoproteins. STRRIDE: A randomized, controlled study of exercise intensity and amount. J. Appl. Physiol. 2007, 103, 432–442. [Google Scholar] [CrossRef]
- Monda, K.L.; Ballantyne, C.M.; North, K.E. Longitudinal impact of physical activity on lipid profiles in middle-aged adults: The Atherosclerosis Risk in Communities Study. J. Lipid Res. 2009, 50, 1685–1691. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, N.; Sawada, S.S.; Shimada, K.; Lee, I.-M.; Gando, Y.; Momma, H.; Kawakami, R.; Miyachi, M.; Hagi, Y.; Kinugawa, C.; et al. Relationship between Cardiorespiratory Fitness and Non-High-Density Lipoprotein Cholesterol: A Cohort Study. J. Ather. Thr. 2018, 25, 1196–1205. [Google Scholar] [CrossRef] [PubMed]
- Haxhi, J.; Scotto di Palumbo, A.; Sacchetti, M. Exercising for Metabolic Control: Is Timing Important. Ann. Nutr. Metab. 2013, 62, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Sénéchal, M.; Bouchard, D.R.; Dionne, I.J.; Brochu, M. The effects of lifestyle interventions in dynapenic-obese postmenopausal women. Menopause 2012, 19, 1015–1021. [Google Scholar] [CrossRef]
- Dominguez-Amorós, M.; Aoaricio-Chueca, P. Lack of Association between the Reasons for and Time spent Doing Physical Activity. Int. J. Environ. Res. Public Health 2020, 17, 6777. [Google Scholar] [CrossRef]
- Nowak, M.; Ambroży, T. Współczesny Trening Obwodowy w Teorii i Praktyce; Fall: Kraków, Poland, 2015. [Google Scholar]
- Ambroży, T. W poszukiwaniu związków treningu obwodowego z prozdrowotną aktywnością fizyczną. Annales Medicina 2007, 62, 55–60. [Google Scholar]
- U.S. Department of Education Office of Educational Research and Iprovement. Research Digest Definitiona: Health, Fitness and Physical Activity. Available online: http://www.fitness.gov/activity/activity2/digest_mar2000/digest_mar2000.html (accessed on 10 July 2022).
- Miller, M.; Ginsberg, H.N.; Schaefer, E.J. Relative Atherpgenicity and Predictive Value of Non-High_Density Lipoprotein Cholesterol for Corobary Heart Disease. Am. J. Cardiol. 2008, 101, 1003–1008. [Google Scholar] [CrossRef]
- Blüher, M.; Hentschel, B.; Rassoul, F.; Richter, V. Influence of dietary intake and physical activity on annual rhythm of human blood cholesterol concentration. Chronobiol. Int. 2001, 18, 541–557. [Google Scholar] [CrossRef]
- Wilson, P.W.; Abbot, R.D.; Castelli, W.P. High density lipoprotein cholesterol and mortality. The Framingham Heart Study. Arteriosclerosis 1988, 8, 737–741. [Google Scholar] [CrossRef]
- Musliner, T.A.; Krauss, R.M. Lipoprotein subspecies and risk of coronary disease. Clin. Chem. 1988, 34, B78–B83. [Google Scholar] [PubMed]
- Zimetbaum, P.; Frishman, W.H.; Ooi, W.L.; Derman, M.P.; Aronson, M.; Gidez, L.I.; Eder, H.A. Plasma Lipids and Lipoproteins and the Incidents of Cardiovascula Disease in the Very Elderly. Arterioscler. Thromb. 1992, 12, 416–423. [Google Scholar] [CrossRef]
- Lira, F.; Zanchi, N.E.; Lima-Silva, A.E.; Pires, F.O.; Bertuzzi, R.C.; Santos, R.V.; Caperuto, E.C.; Kiss, M.A.; Seeleander, M. Acute high-intensity exercise with low Energy expenditure reduced LDL-C and total cholesterol in men. Eur. J. Appl. Physiol. 2009, 107, 203–210. [Google Scholar] [CrossRef]
- Fabio, F.S.; Yamashita, A.S.; Uchida, M.C.; Zanchi, N.E.; Gualano, B.; Martins, E., Jr.; Caperuto, E.C.; Seeleander, M. Low and moderate, rather than high intensity strength exercise induces benefit regarding plasma lipid profile. Diabet. Metabo. Syn. 2010, 2, 1–6. [Google Scholar] [CrossRef]
- Wagganer, J.D.; Robinson, C.E.; Ackerman, T.A.; Davis, P.G. Effects of exercise accumulation on plasma lipids and lipoprotein. Appl. Physiol. Nutr. Metabol. 2015, 40, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Musa, D.I.; Adeniran, S.A.; Dikko, A.U.; Sayers, S.P. The Effect of a High-Intensity Interval Training Program on High-Density Lipoprotein Cholesterol in Young Men. J. Strength Cond. Res. 2009, 23, 587–592. [Google Scholar] [CrossRef]
- Sunami, Y.; Motoyama, M.; Kinoshita, F.; Mizooka, Y.; Sueta, K.; Matsunaga, A.; Sasaki, J.; Tanaka, H.; Shindo, M. Effects of Low-Intensity Aerobic Training on the High-Density Lipoprotein Cholesterol Concentration in Healthy Elderly Subjects. Metabolism 1999, 48, 984–988. [Google Scholar] [CrossRef]
- Kokkinos, P.F.; Fernhal, B. Physical Activity and High Density Lipoprotein Cholesterol Levels. What Is the Relationships? Sports Med. 1999, 28, 307–314. [Google Scholar] [CrossRef]
- Seidi, A.A.; Mahdirejei, H.A.; Abadei, S.F.R.; Gorji, N.E.; Madrilene, H.A.; Shahrestani, Z. Effect of 8 Weeks Endurance Training on Lipid Profile and Testosterone Levels in Young Judokas. J. Appl. Pharm. Sci. 2015, 5, 075–077. [Google Scholar] [CrossRef]
- Help Us Build a Vibrant, Collaborative Global Commons. Available online: http://creativecommons.org/licenses/by-nc-sa/3.0/ (accessed on 12 July 2022).
- Katzmarzyk, P.T.; Leon, A.S.; Rankinen, T.; Gagnon, J.; Skinner, J.S.; Wilmore, J.H.; Rao, D.C.; Bouchard, C. Changes in Blood Lipids Consequent to Aerobic Exercise Training Related to Changes in Body Fatness and Aerobic Fitness. Metabilism 2001, 50, 841–848. [Google Scholar] [CrossRef]
- Nicklas, B.J.; Katzel, L.I.; Busby-Whiteheaf, J.; Goldberg, A.P. Increases in High-Density Lipoprotein Cholesterol with Endurance Exercise Training are Blunted in Obese Compared with Lean Men. Metabolism 1997, 46, 556–561. [Google Scholar] [CrossRef]
- Suraki, R.D.; Mohsenzade, M.; Tibana, R.A.; Ahmadizad, S. Effects of CrossFit on lipid profiles, body composition and physical fitness in overweight men. Sport Sci. Health 2021, 17, 855–862. [Google Scholar] [CrossRef]
- Karami, H.; Dehnou, V.V.; Nazari, A.; Gahreman, D. Regular training has a greater effect on aerobic capacity, fasting blood glucose and blood lipids in obese adolescent males compared to irregular training. J. Exerc. Sci. Fitness. 2021, 19, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Razi, O.; Mohammadi, M.; Zamani, N.; Hackney, A.C.; Tourny, C.; Zouita, S.; Laher, I.; Zouhal, H. Walking exercise and lower-body blood restriction: Effects on systemic inflammation, lipid profiles and hematological indices in overweight middle-aged males. Res. Sports Med. 2021, 30, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Spate-Douglas, T.; Keyser, R.E. Exercise Intensity: Its Effect on the High-Density Lipoprotein Profile. Arch. Phys. Med. Rehab. 1999, 80, 691–695. [Google Scholar] [CrossRef]
- Mann, S.; Beedie, C.; Jimenez, A. Differential effects of aerobic exercise, resistance training and combined exercise modalities on cholesterol and lipid profile: Review, Sythesis and Recomendation. Sports Med. 2014, 44, 211–221. [Google Scholar] [CrossRef]
- Gordon, B.; Chen, S.; Durstine, J.L. The effect of Exercise Training on the Traditional Lipid Profile and Beyond. Curr. Sports Med. Rep. 2014, 13, 253–259. [Google Scholar] [CrossRef]
- Ahtiainen, J.P.; Salinen, J.; Häkkinen, K.; Sillanpää, E. Inter-individual variation in response to resistance training in cardiometabolic health indicators. Scand. J. Med. Sci. Sports 2020, 30, 1040–1053. [Google Scholar] [CrossRef]
- Hsu, C.S.; Chang, S.T.; Ndi Nfor, O.; Lee, K.J.; Lee, S.S.; Liaw, Y.P. Effects of regular aerobic Exercise and resistance training on high-density lipoprotein cholesterol levels in Taiwanese Adults. Int. J. Environ. Res. Public Health 2019, 16, 2003. [Google Scholar] [CrossRef]
- Ouerghi, N.; Ben Fradji, M.C.; Bezrati, I.; Khammassi, M.; Feki, M.; Kaabachi, N.; Bouassida, A. Effects of high-intensity interval training on body composition, aerobic and anaerobic performance and plasma lipids in overweight/obese and normal-weight young men. Biol. Sport. 2017, 34, 385–392. [Google Scholar] [CrossRef]
- Heisz, J.J.; Tejada, M.G.M.; Paloucci, E.M.; Muir, C. Enjoyment for high-intensity interval exercise increases during the first six weeks of training; implication for promoting exercise adherence in sedentary adults. PLoS ONE 2016, 14, e0168534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mleczko, E.; Gradek, J.; Januszewski, J.; Cieśla, E.; Nieroda, R.; Szymańska, E. Health Related Fitness (H-Rf) of Obese and Overweight Children from Malopolska Region—Part. J. Kinesiol. Exerc. Sci. 2017, 27, 23–36. [Google Scholar] [CrossRef]
- Szymańska, E.; Mleczko, E.; Płatek, A. Proposal for The Evaluation of Physical Fitness According to the Health Related Fitness (H-Rf) Concept. J. Kinesiol. Exerc. Sci. 2017, 27, 43–63. [Google Scholar] [CrossRef]


{kind=link}
| Group | Variable | Mean | SD | Min–Max |
|---|---|---|---|---|
| Experimental N = 15 | Age (years) | 36.7 | 1.7 | 35–40 |
| Body height (cm) | 178.3 | 4.9 | 170–189 | |
| BM (kg) | 91.24 | 13.1 | 62.3–112.6 | |
| BMI (kg/m2) | 28.2 | 4.1 | 23.2–36.4 | |
| Control N = 15 | Age (years) | 38.4 | 1.8 | 35–40 |
| Body height (cm) | 177.8 | 7.4 | 163–192 | |
| BM (kg) | 87.8 | 14.4 | 65.4–121.2 | |
| BMI (kg/m2) | 26.9 | 2.9 | 21.2–31.6 |
| Experimental Program Based on the Circuit Training | |
|---|---|
| Number of circuits | 3 circuits × 3 type of training units |
| Number of exercises in a circuit | 5 |
| Number of repetitions or duration of the set | 1 circuit–15 repetitions in 45 s 2–3 circuits–exercises for 30 s |
| Percentage of maximum weight | 50% (individual levels) |
| Exercise intensity | Fast |
| Rests between circuits | 1 min between exercises–3 min between circuits |
| Strength Conditioning Circuit | General Fitness Circuit | Functional Fitness Circuit |
|---|---|---|
| Overhead squat | Footwork using speed ladders | Chest press with rubbers attached to the ladder |
| Narrow grip chest pull-ups | Transition from standing position to the push-up position followed by a tuck jump (burpees) | Lunges with moving the medicine ball from over the head |
| Lying alternate dumbbell press on the exercise ball | A-skips with dumbbells held in hands | Push-ups on Bosu ball and return to the standing position while alternate lifting the Bosu ball over the head and chest press |
| Kettlebell swing in from the sumo position | Jumping over the hurdle combined with moving under the hurdle | Pull-ups on the hanging rope with trunk rotations |
| Russian twists with the disc weight held with both hands | Squats followed by single leg jumps on a plyo-box | Side stepping between the discs |
| TC | Experimental Group | Control Group | Between Groups Differences | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Med | Min | Max | SD | Mean | Med | Min | Max | SD | t1 | p | d | |
| Pre | 213.3 | 209 | 146 | 301 | 41.3 | 209.3 | 216 | 145 | 265 | 35.3 | 0.28 | 0.781 | 0.10 |
| Post | 171.9 | 173 | 122 | 250 | 31.5 | 199.5 | 200 | 132 | 247 | 34.9 | −2.27 | 0.031 | 0.83 |
| Pre-post differences | 41.3 | 36 | 24 | 51 | 9.74 | 16 | 13 | 18 | - | - | 0.001 | ||
| Cohen’s d | t2 = 5.7 p < 0.001 1.47 | t2 = 2.39 p = 0.031 0.57 | |||||||||||
| HDL | Experimental Group | Control Group | Between Groups Differences | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Med | Min | Max | SD | Mean | Med | Min | Max | SD | t1 | p | d | |
| Pre | 51.9 | 49 | 37 | 71 | 10.0 | 53.7 | 51 | 32 | 82 | 12.5 | −0.45 | 0.667 | 0.19 |
| Post | 49.9 | 45 | 35 | 70 | 11.1 | 50.5 | 49 | 25 | 73 | 14.0 | −0.12 | 0.909 | 0.08 |
| Pre-post differences | 2 | 4 | 2 | 1 | 3.2 | 2 | 7 | 9 | 0.735 | ||||
| Cohen’s d | t2 = 0.98 p = 0.344 0.253 | t2 = 1.06 p = 0.308 0.268 | |||||||||||
| TG | Experimental Group | Control Group | Between Groups Differences | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Med | Min | Max | SD | Mean | Med | Min | Max | SD | t1 | p | d | |
| Pre | 142.2 | 132 | 69 | 238 | 65.4 | 119.7 | 117 | 57 | 185 | 40.0 | 1.14 | 0.264 | 0.41 |
| Post | 108.6 | 90 | 44 | 254 | 42.5 | 125.1 | 119 | 62 | 241 | 50.7 | −0.85 | 0.404 | 0.31 |
| Pre-post differences | 33.6 | 42 | 25 | 16 | −5.47 | −2 | −5 | −56 | - | - | <0.001 | ||
| Cohen’s d | t2 = 3.07 p = 0.008 0.788 | t2 = −0.49 p = 0.631 0.115 | |||||||||||
| LDL | Experimental Group | Control Group | Between Groups Differences | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Med | Min | Max | SD | Mean | Med | Min | Max | SD | t1 | p | d | |
| Pre | 132.9 | 125 | 78 | 228 | 42.5 | 131.6 | 130 | 45 | 190 | 38.6 | 0.09 | 0.931 | 0.03 |
| Post | 99.1 | 101 | 49 | 156 | 29.4 | 124.0 | 137 | 45 | 176 | 37.6 | −1.92 | 0.064 | 0.74 |
| Pre-post differences | 33.8 | 24 | 29 | 72 | - | 7.6 | - | 0 | 35 | - | - | <0.001 | |
| Cohen’s d | t2 = 4.25 p = 0.001 1.18 | t2 = 1.69 p = 0.113 0.469 | |||||||||||
| non-HDL | Experimental Group | Control Group | Between Groups Differences | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Med | Min | Max | SD | Mean | Med | Min | Max | SD | t1 | p | d | |
| Pre | 161.4 | 157 | 115 | 261 | 46.9 | 155.5 | 157 | 63 | 219 | 43.9 | 0.37 | 0.714 | 0.12 |
| Post | 122.2 | 119 | 79 | 207 | 32.7 | 149.1 | 154 | 68 | 200 | 40.5 | 1.96 | 0.061 | 0.72 |
| Pre-post differences | 42.2 | 38 | 36 | 54 | - | 6.4 | 12 | 23 | 42 | - | - | <0.001 | |
| Cohen’s d | t2 = 5.3 p < 0.001 1.344 | t2 = −1.35 p = 0.197 0.376 | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ambroży, T.; Rydzik, Ł.; Obmiński, Z.; Spieszny, M.; Szczepanik, A.; Ambroży, D.; Basiaga-Pasternak, J.; Spieszny, J.; Niewczas, M.; Jaszczur-Nowicki, J. Effect of High-Intensity Strength and Endurance Training in the Form of Small Circuits on Changes in Lipid Levels in Men Aged 35–40 Years. J. Clin. Med. 2022, 11, 5146. https://doi.org/10.3390/jcm11175146
Ambroży T, Rydzik Ł, Obmiński Z, Spieszny M, Szczepanik A, Ambroży D, Basiaga-Pasternak J, Spieszny J, Niewczas M, Jaszczur-Nowicki J. Effect of High-Intensity Strength and Endurance Training in the Form of Small Circuits on Changes in Lipid Levels in Men Aged 35–40 Years. Journal of Clinical Medicine. 2022; 11(17):5146. https://doi.org/10.3390/jcm11175146
Chicago/Turabian StyleAmbroży, Tadeusz, Łukasz Rydzik, Zbigniew Obmiński, Michał Spieszny, Antoni Szczepanik, Dorota Ambroży, Joanna Basiaga-Pasternak, Jakub Spieszny, Marta Niewczas, and Jarosław Jaszczur-Nowicki. 2022. "Effect of High-Intensity Strength and Endurance Training in the Form of Small Circuits on Changes in Lipid Levels in Men Aged 35–40 Years" Journal of Clinical Medicine 11, no. 17: 5146. https://doi.org/10.3390/jcm11175146