


Physical Agent-Based Treatments for Overactive Bladder: A Review


Abstract
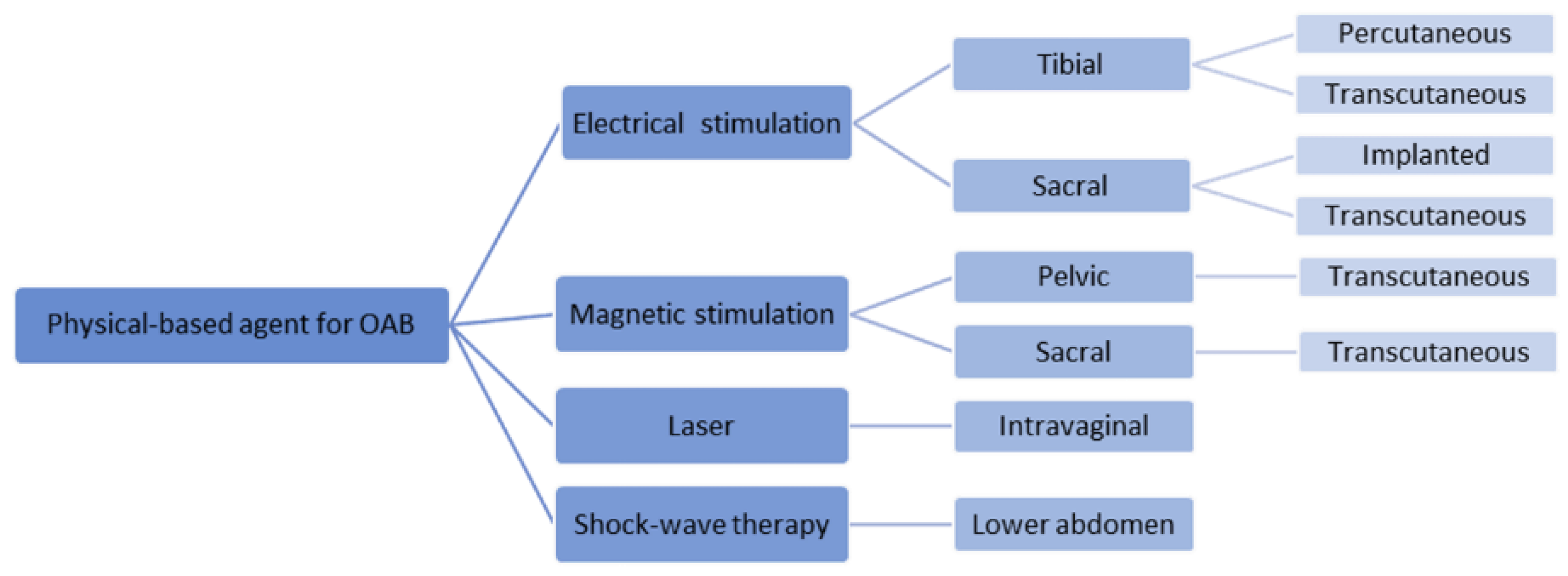
:1. Introduction
2. Electrical Stimulation Modalities
2.1. Percutaneous Sacral Nerve Stimulation (P-SNS)
2.2. Transcutaneous Sacral Nerve Stimulation (T-SNS)
2.3. Percutaneous Posterior Tibial Nerve Stimulation (P-TNS)
2.4. Transcutaneous Tibial Nerve Stimulation (T-TNS)
3. Magnetic Stimulation Modalities
3.1. Pelvic Magnetic Stimulation (P-MS)
3.2. Sacral Magnetic Stimulation (S-MS)
4. Potential New Therapeutic Technologies
4.1. Laser Therapy for OAB
4.2. Low-Intensity Extracorporeal Shock Wave (Li-ESW)
5. Challenges Ahead
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Wang, Y.; Xu, K.; Hu, H.; Zhang, X.; Wang, X.; Na, Y.; Kang, X. Prevalence, risk factors, and impact on health related quality of life of overactive bladder in China. Neurourol. Urodyn. 2011, 30, 1448–1455. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Shin, Y.S.; Lee, J.H.; Cho, W.J.; Kim, D.K. The Prevalence of Lower Urinary Tract Symptoms and Overactive Bladder in South Korea: A Cross-Sectional, Population-Based Study. Int. Neurourol. J. 2022, 26, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Drake, M.J. Do we need a new definition of the overactive bladder syndrome? ICI-RS 2013. Neurourol. Urodyn. 2014, 33, 622–624. [Google Scholar] [CrossRef] [PubMed]
- Irwin, D.E.; Milsom, I.; Hunskaar, S.; Reilly, K.; Kopp, Z.; Herschorn, S.; Coyne, K.; Kelleher, C.; Hampel, C.; Artibani, W.; et al. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: Results of the EPIC study. Eur. Urol. 2006, 50, 1306–1314. [Google Scholar] [CrossRef]
- Chuang, Y.-C.; Liu, S.-P.; Lee, K.-S.; Liao, L.; Wang, J.; Yoo, T.K.; Chu, R.; Sumarsono, B. Prevalence of overactive bladder in China, Taiwan and South Korea: Results from a cross-sectional, population-based study. Low Urin. Tract Symptoms 2019, 11, 48–55. [Google Scholar] [CrossRef]
- Ganz, M.L.; Smalarz, A.M.; Krupski, T.L.; Anger, J.T.; Hu, J.C.; Wittrup-Jensen, K.U.; Pashos, C.L. Economic costs of overactive bladder in the United States. Urology 2010, 75, 526–532.e18. [Google Scholar] [CrossRef]
- Coyne, K.S.; Sexton, C.C.; Kopp, Z.S.; Ebel-Bitoun, C.; Milsom, I.; Chapple, C. The impact of overactive bladder on mental health, work productivity and health-related quality of life in the UK and Sweden: Results from EpiLUTS. BJU Int. 2011, 108, 1459–1471. [Google Scholar] [CrossRef]
- Fontaine, C.; Papworth, E.; Pascoe, J.; Hashim, H. Update on the management of overactive bladder. Ther. Adv. Urol. 2021, 13, 17562872211039034. [Google Scholar] [CrossRef]
- Abdelbary, A.; Al-Dessoukey, A.A.; Moussa, A.S.; El-Nasr, M.S.; Elmarakbi, A.A.; Ragheb, A.M.; Elbatanouny, A.M.; Abdellateef, A.; Sayed, O.; Lotfy, A.; et al. Overactive bladder symptoms recurrence after sudden versus gradual weaning of Solifenacin. Afr. J. Urol. 2020, 26, 91. [Google Scholar] [CrossRef]
- Leron, E.; Weintraub, A.Y.; Mastrolia, S.A.; Schwarzman, P. Overactive Bladder Syndrome: Evaluation and Management. Curr. Urol. 2018, 11, 117–125. [Google Scholar] [CrossRef]
- Gong, Q.Q.; Xu, Y.Q.; Xu, J.; Ding, X.Y.; Guo, C. Meta-Analysis of Randomized Controlled Trials Using Botulinum Toxin A at Different Dosages for Urinary Incontinence in Patients With Overactive Bladder. Front. Pharmacol. 2019, 10, 1618. [Google Scholar] [CrossRef]
- Ponce, F.A. Electrostimulation. In Encyclopedia of the Neurological Sciences, 2nd ed.; Aminoff, M.J., Daroff, R.B., Eds.; Eds.; Academic Press: Oxford, UK, 2014; pp. 1110–1111. [Google Scholar]
- Vasavada, S.; Rackley, R. Electrical stimulation and neuromodulation in storage and emptying failure. In Campbell-Walsh Urology; Elsevier: Amsterdam, The Netherlands, 2012; pp. 2026–2046.e4. [Google Scholar]
- Tanagho, E.A.; Schmidt, R.A. Bladder pacemaker: Scientific basis and clinical future. Urology 1982, 20, 614–619. [Google Scholar] [CrossRef]
- Malaguti, S.; Spinelli, M.; Giardiello, G.; Lazzeri, M.; van den Hombergh, U. Neurophysiological evidence may predict the outcome of sacral neuromodulation. J. Urol. 2003, 170, 2323–2326. [Google Scholar] [CrossRef]
- Liberman, D.; Ehlert, M.J.; Siegel, S.W. Sacral Neuromodulation in Urological Practice. Urology 2017, 99, 14–22. [Google Scholar] [CrossRef]
- Oelke, M.; Addali, M.; Reisenauer, C. What uro-gynecologists should know about sacral neuromodulation (SNM) for the treatment of refractory overactive bladder. Arch. Gynecol. Obstet. 2019, 299, 1243–1252. [Google Scholar] [CrossRef]
- Siegel, S.; Noblett, K.; Mangel, J.; Griebling, T.L.; Sutherland, S.E.; Bird, E.T.; Comiter, C.; Culkin, D.; Bennett, J.; Zylstra, S.; et al. Results of a prospective, randomized, multicenter study evaluating sacral neuromodulation with InterStim therapy compared to standard medical therapy at 6-months in subjects with mild symptoms of overactive bladder. Neurourol. Urodyn. 2015, 34, 224–230. [Google Scholar] [CrossRef]
- Wagner, L.; Alonso, S.; Le Normand, L.; Faix, A.; Kabani, S.; Castelli, C.; Gamé, X.; Cornu, J.; Bey, E. Unilateral versus bilateral sacral neuromodulation test in the treatment of refractory idiopathic overactive bladder: A randomized controlled pilot trial. Neurourol. Urodyn. 2020, 39, 2230–2237. [Google Scholar] [CrossRef]
- Siegel, S.; Noblett, K.; Mangel, J.; Bennett, J.; Griebling, T.L.; Sutherland, S.E.; Bird, E.T.; Comiter, C.; Culkin, D.; Zylstra, S.; et al. Five-Year Followup Results of a Prospective, Multicenter Study of Patients with Overactive Bladder Treated with Sacral Neuromodulation. J. Urol. 2018, 199, 229–236. [Google Scholar] [CrossRef]
- Kaaki, B.; Gupta, D. Medium-term outcomes of sacral neuromodulation in patients with refractory overactive bladder: A retrospective single-institution study. PLoS ONE 2020, 15, e0235961. [Google Scholar] [CrossRef]
- Amundsen, C.L.; Komesu, Y.M.; Chermansky, C.; Gregory, W.T.; Myers, D.L.; Honeycutt, E.F.; Vasavada, S.P.; Nguyen, J.N.; Wilson, T.S.; Harvie, H.S.; et al. Two-Year Outcomes of Sacral Neuromodulation Versus OnabotulinumtoxinA for Refractory Urgency Urinary Incontinence: A Randomized Trial. Eur. Urol. 2018, 74, 66–73. [Google Scholar] [CrossRef]
- De Wachter, S.; Vaganee, D.; Kessler, T.M. Sacral Neuromodulation: Mechanism of Action. Eur Urol Focus. 2020, 6, 823–825. [Google Scholar] [CrossRef]
- Kessler, T.M.; Fowler, C.J. Sacral neuromodulation for urinary retention. Nat. Clin. Pract. Urol. 2008, 5, 657–666. [Google Scholar] [CrossRef]
- Gill, B.C.; Pizarro-Berdichevsky, J.; Bhattacharyya, P.K.; Brink, T.S.; Marks, B.K.; Quirouet, A.; Vasavada, S.P.; Jones, S.E.; Goldman, H.B. Real-Time Changes in Brain Activity during Sacral Neuromodulation for Overactive Bladder. J. Urol. 2017, 198, 1379–1385. [Google Scholar] [CrossRef]
- Groen, J.; Bosch, J.L.H.R.; van Mastrigt, R. Sacral Neuromodulation in Women With Idiopathic Detrusor Overactivity Incontinence: Decreased Overactivity but Unchanged Bladder Contraction Strength and Urethral Resistance During Voiding. J. Urol. 2006, 175, 1005–1009. [Google Scholar] [CrossRef]
- De Wachter, S.; Knowles, C.H.; Elterman, D.S.; Kennelly, M.J.; Lehur, P.A.; Matzel, K.E.; Engelberg, S.; Van Kerrebroeck, P.E. New Technologies and Applications in Sacral Neuromodulation: An Update. Adv. Ther. 2020, 37, 637–643. [Google Scholar] [CrossRef]
- De Wachter, S.; Knowles, C.H.; Elterman, D.S.; Kennelly, M.J.; Lehur, P.A.; Matzel, K.E.; Engelberg, S.; Van Kerrebroeck, P.E.V. Remotely programmed sacral neuromodulation for the treatment of patients with refractory overactive bladder: A prospective randomized controlled trial evaluating the safety and efficacy of a novel sacral neuromodulation device. World J. Urol. 2019, 37, 2481–2492. [Google Scholar]
- Bower, W.F.; Moore, K.H.; Adams, R.D.; Shepherd, R. A urodynamic study of surface neuromodulation versus sham in detrusor instability and sensory urgency. J. Urol. 1998, 160, 2133–2136. [Google Scholar] [CrossRef]
- Padilha, J.F.; Avila, M.A.; Seidel, E.J.; Driusso, P. Different electrode positioning for transcutaneous electrical nerve stimulation in the treatment of urgency in women: A study protocol for a randomized controlled clinical trial. Trials 2020, 21, 166. [Google Scholar] [CrossRef]
- Lordelo, P.; Soares, P.V.; Maciel, I.; Macedo, A., Jr.; Barroso, U., Jr. Prospective study of transcutaneous parasacral electrical stimulation for overactive bladder in children: Long-term results. J. Urol. 2009, 182, 2900–2904. [Google Scholar] [CrossRef]
- Hagstroem, S.; Mahler, B.; Madsen, B.; Djurhuus, J.C.; Rittig, S. Transcutaneous electrical nerve stimulation for refractory daytime urinary urge incontinence. J. Urol. 2009, 182, 2072–2078. [Google Scholar] [CrossRef]
- Veiga, M.L.; Oliveira, K.; Batista, V.; Nacif, A.; Braga, A.A.M.; Barroso, U., Jr. Parasacral transcutaneous electrical nerve stimulation in children with overactive bladder: Comparison between sessions administered two and three times weekly. Int. Braz. J. Urol. 2021, 47, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Sluka, K.A.; Walsh, D. Transcutaneous electrical nerve stimulation: Basic science mechanisms and clinical effectiveness. J. Pain 2003, 4, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Dray, A.; Nunan, L.; Wire, W. Central 6-opioid receptor interactions and the inhibition of reflex urinary bladder contractions in the rat. Br. J. Pharmacol. 1985, 85, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Casal-Beloy, I.; Garcia-Novoa, M.A.; Gonzalez, M.G.; Nebril, B.A.; Argibay, I.S. Transcutaneous sacral electrical stimulation versus oxibutynin for the treatment of overactive bladder in children. J. Pediatr. Urol. 2021, 17, 644.e1–644.e10. [Google Scholar] [CrossRef] [PubMed]
- Borch, L.; Hagstroem, S.; Kamperis, K.; Siggaard, C.V.; Rittig, S. Transcutaneous Electrical Nerve Stimulation Combined with Oxybutynin is Superior to Monotherapy in Children with Urge Incontinence: A Randomized, Placebo Controlled Study. J. Urol. 2017, 198, 430–435. [Google Scholar] [CrossRef]
- Jacomo, R.H.; Alves, A.T.; Lucio, A.; Garcia, P.A.; Lorena, D.C.R.; de Sousa, J.B. Transcutaneous tibial nerve stimulation versus parasacral stimulation in the treatment of overactive bladder in elderly people: A triple-blinded randomized controlled trial. Clinics 2020, 75, e1477. [Google Scholar] [CrossRef]
- Van Balken, M.R.; Vandoninck, V.; Gisolf, K.W.; Vergunst, H.; Kiemeney, L.A.; Debruyne, F.M.; Bemelmans, B.L. Posterior tibial nerve stimulation as neuromodulative treatment of lower urinary tract dysfunction. J. Urol. 2001, 166, 914–918. [Google Scholar] [CrossRef]
- De Wall, L.L.; Heesakkers, J.P. Effectiveness of percutaneous tibial nerve stimulation in the treatment of overactive bladder syndrome. Res. Rep. Urol. 2017, 9, 145–157. [Google Scholar] [CrossRef]
- Gupta, P.; Ehlert, M.J.; Sirls, L.T.; Peters, K.M. Percutaneous tibial nerve stimulation and sacral neuromodulation: An update. Curr. Urol. Rep. 2015, 16, 4. [Google Scholar] [CrossRef]
- Bhide, A.A.; Tailor, V.; Fernando, R.; Khullar, V.; Digesu, G.A. Posterior tibial nerve stimulation for overactive bladder-techniques and efficacy. Int. Urogynecol. J. 2020, 31, 865–870. [Google Scholar] [CrossRef]
- Sonmez, R.; Yildiz, N.; Alkan, H. Efficacy of percutaneous and transcutaneous tibial nerve stimulation in women with idiopathic overactive bladder: A prospective randomised controlled trial. Ann. Phys. Rehabil. Med. 2022, 65, 101486. [Google Scholar] [CrossRef] [PubMed]
- Vandoninck, V.; van Balken, M.R.; Agro, E.F.; Petta, F.; Micali, F.; Heesakkers, J.; Debruyne, F.M.; Kiemeney, L.; Bemelmans, B.L. Percutaneous tibial nerve stimulation in the treatment of overactive bladder: Urodynamic data. Neurourol. Urodyn. 2003, 22, 227–232. [Google Scholar] [CrossRef]
- Peters, K.M.; Carrico, D.J.; Perez-Marrero, R.A.; Khan, A.U.; Wooldridge, L.; Davis, G.L.; MacDiarmid, S.A. Randomized trial of percutaneous tibial nerve stimulation versus Sham efficacy in the treatment of overactive bladder syndrome: Results from the SUmiT trial. J. Urol. 2010, 183, 1438–1443. [Google Scholar] [CrossRef] [PubMed]
- Vecchioli-Scaldazza, C.; Morosetti, C. Effectiveness and durability of solifenacin versus percutaneous tibial nerve stimulation versus their combination for the treatment of women with overactive bladder syndrome: A randomized controlled study with a follow-up of ten months. Int. Braz. J. Urol. 2018, 44, 102–108. [Google Scholar] [CrossRef]
- Wibisono, E.; Rahardjo, H.E. Effectiveness of Short Term Percutaneous Tibial Nerve Stimulation for Non-neurogenic Overactive Bladder Syndrome in Adults: A Meta-analysis. Acta Med. Indones. 2015, 47, 188–200. [Google Scholar] [PubMed]
- Peters, K.M.; Carrico, D.J.; Wooldridge, L.S.; Miller, C.J.; MacDiarmid, S.A. Percutaneous tibial nerve stimulation for the long-term treatment of overactive bladder: 3-year results of the STEP study. J. Urol. 2013, 189, 2194–2201. [Google Scholar] [CrossRef] [PubMed]
- Du, C.; Berg, W.; Siegal, A.R.; Huang, Z.; Jeong, R.; Hwang, K.; Kim, J. Real-world Compliance With Percutaneous Tibial Nerve Stimulation Maintenance Therapy in an American Population. Urology 2021, 153, 119–123. [Google Scholar] [CrossRef] [PubMed]
- McGuire, E.J.; Shi-chun, Z.; Horwinski, E.R.; Lytton, B. Treatment of Motor and Sensory Detrusor Instability by Electrical Stimulation. J. Urol. 1983, 129, 78–79. [Google Scholar] [CrossRef]
- Schreiner, L.; Nygaard, C.C.; dos Santos, T.G.; Knorst, M.R.; da Silva Filho, I.G. Transcutaneous tibial nerve stimulation to treat urgency urinary incontinence in older women: 12-month follow-up of a randomized controlled trial. Int. Urogynecol. J. 2021, 32, 687–693. [Google Scholar] [CrossRef]
- Stewart, F.; Gameiro, L.F.; el Dib, R.; Gameiro, M.O.; Kapoor, A.; Amaro, J.L. Electrical stimulation with non-implanted electrodes for overactive bladder in adults. Cochrane Database Syst. Rev. 2016, 12, CD010098. [Google Scholar]
- Alkis, O.; Sevim, M.; Kartal, I.G.; Baser, A.; Ivelik, H.I.; Aras, B. Comparison of transcutaneous tibial nerve stimulation (TTNS) protocols for women with refractory overactive bladder (OAB): A prospective randomised trial. Int. J. Clin. Pract. 2021, 75, e14342. [Google Scholar] [CrossRef]
- Booth, J.; Aucott, L.; Cotton, S.; Davis, B.; Fenocchi, L.; Goodman, C.; Hagen, S.; Harari, D.; Lawrence, M.; Lowndes, A.; et al. Tibial nerve stimulation compared with sham to reduce incontinence in care home residents: ELECTRIC RCT. Health Technol. Assess. 2021, 25, 1–110. [Google Scholar] [CrossRef]
- Finazzi Agrò, E.; Campagna, A.; Sciobica, F.; Petta, F.; Germani, S.; Zuccalà, A.; Miano, R. Posterior tibial nerve stimulation: Is the once-a-week protocol the best option? Minerva Urol. Nefrol. 2005, 57, 119–123. [Google Scholar]
- Pierre, M.L.; Friso, B.; Casarotto, R.A.; Haddad, J.M.; Baracat, E.C.; Ferreira, E.A.G. Comparison of transcutaneous electrical tibial nerve stimulation for the treatment of overactive bladder: A multi-arm randomized controlled trial with blinded assessment. Clinics 2021, 76, e3039. [Google Scholar] [CrossRef]
- Patidar, N.; Mittal, V.; Kumar, M.; Sureka, S.K.; Arora, S.; Ansari, M.S. Transcutaneous posterior tibial nerve stimulation in pediatric overactive bladder: A preliminary report. J. Pediatr. Urol. 2015, 11, 351.e1–351.e6. [Google Scholar] [CrossRef]
- Barker, A.T. An introduction to Basic Principle of Magnetic Stimulation. J. Clin. Neurophysiol. 1991, 8, 26–37. [Google Scholar] [CrossRef]
- Kanjanapanang, N.; Chang, K.-V. Peripheral Magnetic Stimulation. Available online: https://www.ncbi.nlm.nih.gov/books/NBK526087/ (accessed on 2 June 2022).
- Kanjanapanang, N.; Chang, K. Peripheral magnetic stimulation. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Yamanishi, T.; Yasuda, K.; Suda, S.; Ishikawa, N.; Sakakibara, R.; Hattori, T. Effect of Functional Continuous Magnetic Stimulation for Urinary Incontinence. J. Urol. 2000, 163, 456–459. [Google Scholar] [CrossRef]
- Kim, J.W.; Kim, M.J.; Noh, J.Y.; Lee, H.Y.; Han, S.W. Extracorporeal pelvic floor magnetic stimulation in children with voiding dysfunction. BJU Int. 2005, 95, 1310–1313. [Google Scholar] [CrossRef]
- Goldberg, R.P.; Sand, P.K. Electromagnetic Pelvic Floor Stimulation: Applications for the Gynecologist. Obstet. Gynecol. Surv. 2000, 55, 715–720. [Google Scholar] [CrossRef]
- Morris, A.R.; O’Sullivan, R.; Dunkley, P.; Moore, K.H. Extracorporeal Magnetic Stimulation is of Limited Clinical Benefit to Women with Idiopathic Detrusor Overactivity: A Randomized Sham Controlled Trial. Eur. Urol. 2007, 52, 876–883. [Google Scholar] [CrossRef]
- Lo, T.-S.; Tseng, L.-H.; Lin, Y.-H.; Liang, C.-C.; Lu, C.-Y.; Pue, L.B. Effect of extracorporeal magnetic energy stimulation on bothersome lower urinary tract symptoms and quality of life in female patients with stress urinary incontinence and overactive bladder. J. Obstet. Gynaecol. Res. 2013, 39, 1526–1532. [Google Scholar] [CrossRef]
- Choe, J.H.; Choo, M.S.; Lee, K.S. Symptom change in women with overactive bladder after extracorporeal magnetic stimulation: A prospective trial. Int. Urogynecol. J. Pelvic Floor Dysfunct. 2007, 18, 875–880. [Google Scholar] [CrossRef]
- Suzuki, T.; Yasuda, K.; Yamanishi, T.; Kitahara, S.; Nakai, H.; Suda, S.; Ohkawa, H. Randomized, double-blind, sham-controlled evaluation of the effect of functional continuous magnetic stimulation in patients with urgency incontinence. Neurourol. Urodyn. 2007, 26, 767–772. [Google Scholar] [CrossRef]
- Vadalà, M.; Palmieri, B.; Malagoli, A.; Laurino, C. High-power Magnetotherapy: A New Weapon in Urinary Incontinence? LUTS Low. Urin. Tract Symptoms 2018, 10, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; China, T.; Takazawa, N.; Shimizu, F.; Fink, J.; Horie, S.; Imai, T. Therapeutic Effect of Magnetic Stimulation Therapy on Pelvic Floor Muscle Dysfunction; IntechOpen: London, UK, 2021. [Google Scholar]
- Tsai, P.Y.; Wang, C.P.; Hsieh, C.Y.; Tsai, Y.A.; Yeh, S.C.; Chuang, T.Y. Long-term sacral magnetic stimulation for refractory stress urinary incontinence. Arch. Phys. Med. Rehabil. 2014, 95, 2231–2238. [Google Scholar] [CrossRef]
- Fujishiro, T.; Takahashi, S.; Enomoto, H.; Ugawa, Y.; Ueno, S.; Kitamura, T. Magnetic stimulation of the sacral roots for the treatment of urinary frequency and urge incontinence: An investigational study and placebo controlled trial. J. Urol. 2002, 168, 1036–1039. [Google Scholar] [CrossRef]
- Fergany, L.A.; Shaker, H.; Arafa, M.; Elbadry, M.S. Does sacral pulsed electromagnetic field therapy have a better effect than transcutaneous electrical nerve stimulation in patients with neurogenic overactive bladder? Arab. J. Urol. 2017, 15, 148–152. [Google Scholar] [CrossRef]
- Avci, P.; Gupta, A.; Sadasivam, M.; Vecchio, D.; Pam, Z.; Pam, N.; Hamblin, M.R. Low-level laser (light) therapy (LLLT) in skin: Stimulating, healing, restoring. Semin. Cutan. Med. Surg. 2013, 32, 41–52. [Google Scholar]
- Perino, A.; Cucinella, G.; Gugliotta, G.; Saitta, S.; Polito, S.; Adile, B.; Marci, R.; Calagna, G. Is vaginal fractional CO2 laser treatment effective in improving overactive bladder symptoms in post-menopausal patients? Preliminary results. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 2491–2497. [Google Scholar] [PubMed]
- Aguiar, L.B.; Politano, C.A.; Costa-Paiva, L.; Juliato, C.R.T. Efficacy of Fractional CO2 Laser, Promestriene, and Vaginal Lubricant in the Treatment of Urinary Symptoms in Postmenopausal Women: A Randomized Clinical Trial. Lasers Surg. Med. 2020, 52, 713–720. [Google Scholar] [CrossRef]
- Lin, Y.H.; Hsieh, W.C.; Huang, L.; Liang, C.C. Effect of non-ablative laser treatment on overactive bladder symptoms, urinary incontinence and sexual function in women with urodynamic stress incontinence. Taiwan J. Obstet. Gynecol. 2017, 56, 815–820. [Google Scholar] [CrossRef]
- Okui, N. Efficacy and safety of non-ablative vaginal erbium:YAG laser treatment as a novel surgical treatment for overactive bladder syndrome: Comparison with anticholinergics and beta3-adrenoceptor agonists. World J. Urol. 2019, 37, 2459–2466. [Google Scholar] [CrossRef] [PubMed]
- Okui, N. Comparison between erbium-doped yttrium aluminum garnet laser therapy and sling procedures in the treatment of stress and mixed urinary incontinence. World J. Urol. 2019, 37, 885–889. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Shindel, A.W.; Lin, G.; Lue, T.F. Cellular signaling pathways modulated by low-intensity extracorporeal shock wave therapy. Int. J. Impot. Res. 2019, 31, 170–176. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Chuang, S.-M.; Lin, K.-L.; Chen, W.-C.; Lu, J.-H.; Chueh, K.-S.; Shen, M.-C.; Liu, L.-W.; Long, C.-Y.; Juan, Y.-S. Low-Intensity Extracorporeal Shock Wave Therapy Ameliorates the Overactive Bladder: A Prospective Pilot Study. BioMed Res. Int. 2020, 2020, 9175676. [Google Scholar] [CrossRef]
- Lu, J.-H.; Chueh, K.-S.; Chuang, S.-M.; Wu, Y.-H.; Lin, K.-L.; Long, C.-Y.; Lee, Y.-C.; Shen, M.-C.; Sun, T.-W.; Juan, Y.-S. Low Intensity Extracorporeal Shock Wave Therapy as a Potential Treatment for Overactive Bladder Syndrome. Biology 2021, 10, 540. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.-L.; Lu, J.-H.; Chueh, K.-S.; Juan, T.-J.; Wu, B.-N.; Chuang, S.-M.; Lee, Y.-C.; Shen, M.-C.; Long, C.-Y.; Juan, Y.-S. Low-Intensity Extracorporeal Shock Wave Therapy Promotes Bladder Regeneration and Improves Overactive Bladder Induced by Ovarian Hormone Deficiency from Rat Animal Model to Human Clinical Trial. Int. J. Mol. Sci. 2021, 22, 9296. [Google Scholar] [CrossRef]
- Arlandis, S.; Castro, D.; Errando, C.; Fernández, E.; Jiménez, M.; González, P.; Crespo, C.; Staeuble, F.; Rodríguez, J.M.; Brosa, M. Cost-effectiveness of sacral neuromodulation compared to botulinum neurotoxin a or continued medical management in refractory overactive bladder. Value Health 2011, 14, 219–228. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| No. | Device | Advantages | Consideration | Long-Term Efficacy | Symptom Reduction |
|---|---|---|---|---|---|
| 1 | P-SNS |
| 3–5 years [20,21] | Urgency, frequency, incontinence episodes [19] | |
| 2 | T-SNS |
| Needs at least 20 sessions [31] or daily up to 6 months at home [36] | 2 years [31] | Nocturia, urgency, incontinence episodes [38] |
| 3 | P-TNS | Superior to solifenacin alone; however, the combination of both is more beneficial [46] |
| 3 years [48] | Day and night time frequency, urgency and urge incontinence [46] |
| 4 | T-TNS |
|
| 1 years [51] | Nocturia, frequency, incontinence episodes [43] |
| 5 | P-MS |
| 6 months [67] | Urgency, frequency, urgency incontinence [67] | |
| 6 | S-MS |
| Needs 20 sessions [72] | No data | Urgency, frequency, bladder capacity [71] |
| 7 | Laser | Intravaginal procedure [77,78] | <12 months [76] | Frequency, nocturia, urgency, urge incontinence episodes [77,78] | |
| 8 | Li-ESW |
| Needs 8 sessions [80,81] | No data | Daytime frequency, urgency, decreased post-voided residual urine, increased bladder capacity [80,81] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khasanah, N.; Chin, H.-Y.; Peng, C.-W. Physical Agent-Based Treatments for Overactive Bladder: A Review. J. Clin. Med. 2022, 11, 5150. https://doi.org/10.3390/jcm11175150
Khasanah N, Chin H-Y, Peng C-W. Physical Agent-Based Treatments for Overactive Bladder: A Review. Journal of Clinical Medicine. 2022; 11(17):5150. https://doi.org/10.3390/jcm11175150
Chicago/Turabian StyleKhasanah, Nurida, Hung-Yen Chin, and Chih-Wei Peng. 2022. "Physical Agent-Based Treatments for Overactive Bladder: A Review" Journal of Clinical Medicine 11, no. 17: 5150. https://doi.org/10.3390/jcm11175150