Abstract
Superinfections are a fundamental critical care problem, and their significance in severe COVID-19 cases needs to be determined. This study analyzed data from the Lean European Open Survey on SARS-CoV-2-Infected Patients (LEOSS) cohort focusing on intensive care patients. A retrospective analysis of patient data from 840 cases of COVID-19 with critical courses demonstrated that co-infections were frequently present and were primarily of nosocomial origin. Furthermore, our analysis showed that invasive therapy procedures accompanied an increased risk for healthcare-associated infections. Non-ventilated ICU patients were rarely affected by secondary infections. The risk of infection, however, increased even when non-invasive ventilation was used. A further, significant increase in infection rates was seen with the use of invasive ventilation and even more so with extracorporeal membrane oxygenation (ECMO) therapy. The marked differences among ICU techniques used for the treatment of COVID-19-induced respiratory failure in terms of secondary infection risk profile should be taken into account for the optimal management of critically ill COVID-19 patients, as well as for adequate antimicrobial therapy.
1. Introduction
COVID-19, a pulmonary disease from an infection with the single-stranded RNA virus SARS-CoV-2, has evolved into a global pandemic since March 2020. Clinical manifestation is highly variable. Asymptomatic courses, mild respiratory diseases, severe pneumonia, and severe organ dysfunction that can be accompanied by shock and death have been described [1,2,3,4,5,6]. A certain proportion of patients develop an increased respiratory rate (>30/min), a decrease in oxygen saturation with hypoxemia, and respiratory insufficiency, which requires intensive care, usually due to dyspnea [3,4,5,6,7].
During the course of the pandemic, specific therapies for COVID-19 have been developed. However, the corresponding drugs should be applied within the first days after infection [8]. Relative risk reduction with respect to hospitalization or adverse outcome by the administration of antivirals or neutralizing monoclonal antibodies was described with the initiation of therapy at 3 to a maximum of 6 days after symptom onset [8]. Therefore, in an intensive care unit (ICU), only supportive treatment options are available to alleviate symptoms. In severe respiratory failure, intubation and invasive ventilation is the standard therapy in clinical practice [9]. It is a life-saving measure and usually ensures a safe airway and sufficient oxygenation, along with carbon dioxide elimination [9]. Early intubation counteracts the progressive deterioration of lung function due to increased respiratory stress [4,6]. It has also been reported that the critical delay of intubation in the event of failure of non-invasive ventilation options is associated with a poorer prognosis [4,6]. However, invasive ventilation may be the cause of ventilator-associated lung injury [6,7,9]. In addition, the safe airway required for invasive ventilation can promote serious, even lethal, infections [10]. The scientific literature, therefore, also contains reports recommending the avoidance of intubation as long as it is not essential [11].
Patients with viral infections are known to be predisposed to secondary infections [12,13,14,15,16]. In particular, bacteria may benefit from viral infections, and even those that are normally harmless could turn into opportunistic pathogens. The viral facilitation of bacterial pathogenesis is based on complex and multifactorial processes that, ultimately, promote bacterial adherence, disrupt epithelial layers, lead to the displacement of commensal bacteria, and subvert the host immune response [16]. There are multiple reports associating SARS-CoV-2 with co-infections of, primarily, bacterial but also fungal origin. The most common bacterial microorganisms in respiratory cultures from COVID-19 patients are Pseudomonas aeruginosa, Klebsiella species, Staphylococcus aureus, Escherichia coli, and Stenotrophomonas maltophilia [13,14]. The main fungal pathogens identified are Aspergillus and Candida species, but there are also reports of secondary infections with Mucormycetes, Histoplasma spp, Cryptococcus spp, and Pneumocystis jirovecii [12]. Alarmingly, such secondary infections have been linked to a severe clinical course with possible poor outcome [15,16].
Infections are a common problem in ICUs. A critical condition, an impaired immune response, and invasive treatments (i.e., mechanical ventilation and catheterization) all pose risk factors for nosocomial infections [10,17,18,19,20,21]. It is of concern that secondary infections in viral diseases of the respiratory tract, such as influenza, have been described as causes of morbidity and mortality [22,23,24,25]. However, the prevalence and clinical impact of healthcare-associated infections of bacterial or fungal nature in COVID-19 patients treated in ICUs is not well-understood and constitutes a serious knowledge gap. There is also insufficient knowledge on whether bacterial colonialization present on admission impacts disease severity and outcome. More data on community-acquired colonializations, as well as nosocomial infections in ICUs, are needed to optimize the management and treatment of the most severe COVID-19 cases. This could not only help to save lives but also to improve antimicrobial stewardship [26,27,28,29].
The aim of the present study is to unravel the prevalence of community-acquired colonializations with multidrug-resistant bacteria, as well as healthcare-associated secondary bacterial and fungal infections, in critically ill COVID-19 patients treated at an ICU. The primary objective was to determine whether (i) there is an association between a patient’s infection status and the ventilation therapy used and whether (ii) co-infections are related to mortality. The secondary objectives are to examine the frequency of use and the clinical benefit of antimicrobial therapy in critically ill COVID-19 patients.
2. Materials and Methods
2.1. Patient Cohort
This study analyzed patient data from the Lean European Open Survey on SARS-CoV-2-Infected Patients (LEOSS) cohort [30]. The LEOSS project represents a non-interventional, multicenter network that aims at addressing the lack of in-depth knowledge on the epidemiology and clinical course of COVID-19. Established in March 2020, the LEOSS registry encloses data mainly on hospitalized COVID-19 patients. In the LEOSS protocol, patients can be included via PCR confirmed diagnosis or rapid antigen tests as an acceptable alternative. Detailed information on LEOSS can be found on the project’s website (https://leoss.net, accessed date: 5 August 2022). The study was registered at the German Clinical Trials Register (DRKS, No S00021145).
Clinical data are reported in an electronic case report form (eCRF) using the online platform ClinicalSurveys.net, which was developed by the University Hospital of Cologne (UHC), Germany, and is hosted by QuestBack, Oslo, Norway, on servers of the UHC [31]. Anonymized patient data are added to the LEOSS registry retrospectively at the end of the acute treatment setting, i.e., when either the treatment is completed or the patient has died. In order to ensure anonymity in all steps of the analysis process, an individual LEOSS Scientific Use File (SUF) was created, which is based on the LEOSS Public Use File (PUF) principles described in Jakob et al. [31]. Re-identification is prevented by vertical (categorical assessment of numerical variables) and horizontal data aggregation (data aggregation within the phases of disease). Categorization is based on four phases, which can be roughly characterized as asymptomatic or mild symptoms (uncomplicated phase), need for oxygen supplementation (complicated phase), need for critical care (critical phase), and the recovery phase. A detailed description of the clinical phases as defined in the LEOSS registry, as well as of the recorded data items, can be found on the project’s website (https://leoss.net; accessed on 4 August 2022) and in [32].
2.2. Study Design
This analysis included data of 840 patients who were documented by a LEOSS partner site between 23 March 2020 and 12 October 2020 due to COVID-19 disease diagnosed and treated between February 2020 and October 2020. Only patients who reached the critical phase according to the definitions of the LEOSS database [32] during the course of their COVID-19 disease were included in the analysis. The onset of the critical phase was declared if at least one of the following criteria was present: need for catecholamines, life-threatening cardiac arrhythmia, need for unplanned mechanical ventilation (invasive or non-invasive), prolongation (>24 h) of planned mechanical ventilation, liver failure with Quick <50% or INR >3.5, a qSOFA score of ≥2, or acute renal failure with need of dialysis. Dedicated intensive care data items were developed by a working group of specialized intensive care physicians (LEOSS Intensive Care Group) and implemented in the LEOSS registry. From this set, the following data items were analyzed: (i) the colonialization status of the patients with regard to multidrug-resistant pathogens at baseline, i.e., day of positive SARS-CoV-2 diagnosis (multidrug-resistant, Gram-negative bacteria (3MRGN/4MRGN), methicillin-resistant Staphylococcus aureus (MRSA), and vancomycin-resistant enterococci (VRE)), as well as bacterial and fungal superinfections in the critical phase; (ii) the ventilation treatments performed (non-invasive ventilation, invasive ventilation, or extracorporeal membrane oxygenation (ECMO)); (iii) the medications used; and (iv) the outcome (recovery or death). 3MRGN and 4MRGN are enterobacteriaceae, Pseudomonas aeruginosa, and Acinetobacter baumannii exhibiting resistance to three or four of these antibiotics or antibiotic groups: piperacillin, carbapenems, quinolones, and cephalosporins of the third generation. Two endpoints were defined: (i) the prevalence of community-acquired colonializations and healthcare-associated secondary infections in patients in need of or receiving a specific ventilation therapy (non-invasive ventilation, invasive ventilation, or ECMO) and (ii) the effect of community-acquired colonializations and healthcare-associated secondary infections on patient outcome.
2.3. Statistical Analysis
All data were presented as categorical variables (numbers and percentages). To compare categorical variables, Pearson’s chi-squared or Fisher’s exact test was used where appropriate. The level of significance was set at p < 0.05. The data management, statistical analysis, and computation of figures were conducted using R (R Development Core Team, Vienna, Austria, Version 4.1.1, 2021).
3. Results
3.1. Characteristics of the Study Population
From February 2020 to October 2020, 840 SARS-CoV-2-positive diagnosed patients were admitted to an ICU at a LEOSS study site (Table 1). The majority of the patients were between 46 and 85 years old (85.1%; 715/840), and 6.7% (56/840) were older than 85 years. A total of 602 of the 840 patients (71.7%) were male; the only age group without a male predominance was the 85+ age group. The most common comorbidities were hypertension (61.0%, 512/840), diabetes mellitus (28.1%; 236/840), chronic kidney disease (17.3%; 145/840), coronary artery disease (16.7%; 140/840), and atrial fibrillation (16.0%; 134/840). Only 13.9% of the patients (117/840) had no documented comorbidities; one comorbidity was documented for 22.0% of the patients (185/840), and multiple comorbidities (up to 14) were reported in 64.1% of the patients (538/840). Mechanical ventilation therapy was used in the vast majority of patients. In 21.5% of the patients (181/840), an attempt at non-invasive ventilation failed, requiring intubation; in 37.0% of the patients (311/840), intubation was performed without prior non-invasive ventilation. Exclusive non-invasive ventilation was documented in 10.4% of the patients (87/840). Extracorporeal membrane oxygenation (ECMO) was required in 13.6% of the patients (114/840). Still, 17.5% of the patients (147/840) did not receive mechanical ventilation therapy. The majority of the patients (66.2%, 556/840) had a length of stay in the ICU of 0–3 weeks; 264 of 840 patients (31.4%) received intensive care for 4–9 weeks, and for 2.4% of the patients (20/840), a length of treatment in the ICU exceeding 9 weeks was documented. The overall mortality rate was 46% (386/840).

Table 1.
Epidemiological data of the total cohort, as well as subcohorts, subdivided according to the type of ventilation performed. ECMO: extracorporeal membrane oxygenation.
3.2. Community-Acquired Colonializations with Multidrug-Resistant Bacteria
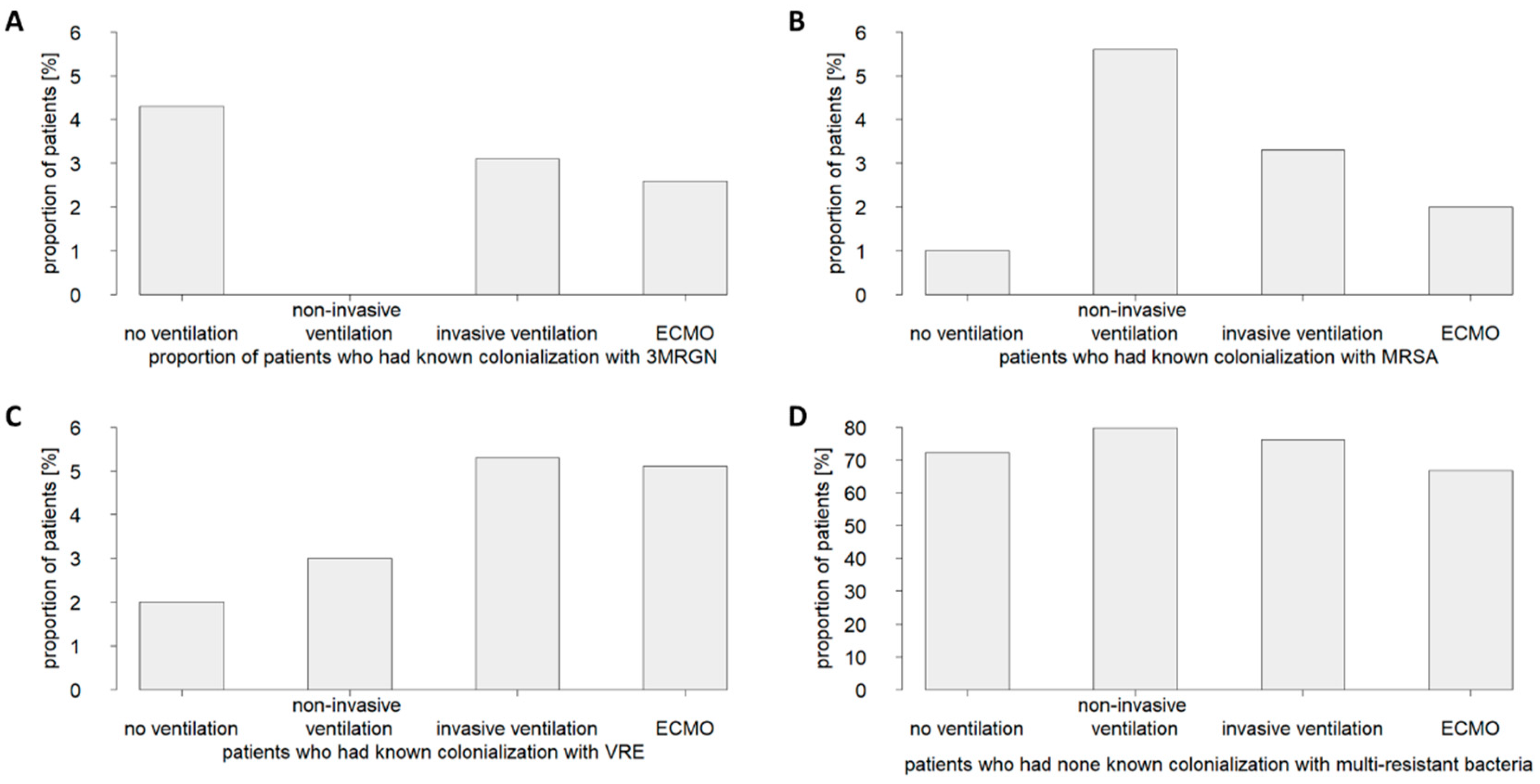
Complete or at least partial information on colonializations with multidrug-resistant pathogens at baseline (say of positive SARS-CoV-2 diagnosis) was available for 71.2% of the patients (598/840). Among these, colonialization with 3MRGN was documented in 2.8% of the cases, with MRSA in 2.6% of the cases and VRE in 4.1% of the cases. However, the majority of the patients (75.1% of the cases) were declared free of colonialization with these bacteria on presentation. Information on 4MRGN was captured in the dataset, but so few infections were reported that details were not made available in the LEOSS Scientific Use File to maintain patient anonymity.
Examining in detail the patient subcohorts grouped by ventilation therapy performed (i.e., no ventilation, non-invasive ventilation, invasive ventilation, or ECMO) indicated no fundamental differences in colonialization prevalence with multidrug-resistant pathogens (Figure 1). Thus, the data did not support the hypothesis that a community-acquired colonialization with a multidrug-resistant pathogen increased the risk of a critically ill COVID-19 patient to require invasive ventilation or ECMO therapy.
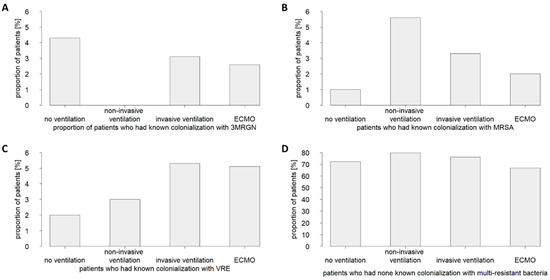
Figure 1.
Prevalence of community-acquired colonializations with multidrug-resistant bacteria in patients critically ill with COVID-19 who received no ventilation therapy or were treated with non-invasive ventilation, invasive ventilation, or ECMO (extracorporeal membrane oxygenation). Shown are the proportions of patients who were colonized with (A) 3MRGN (multidrug-resistant Gram-negative bacteria), (B) MRSA (methicillin-resistant Staphylococcus aureus), or (C) VRE (vancomycin-resistant enterococci), or those where (D) no colonization was found.
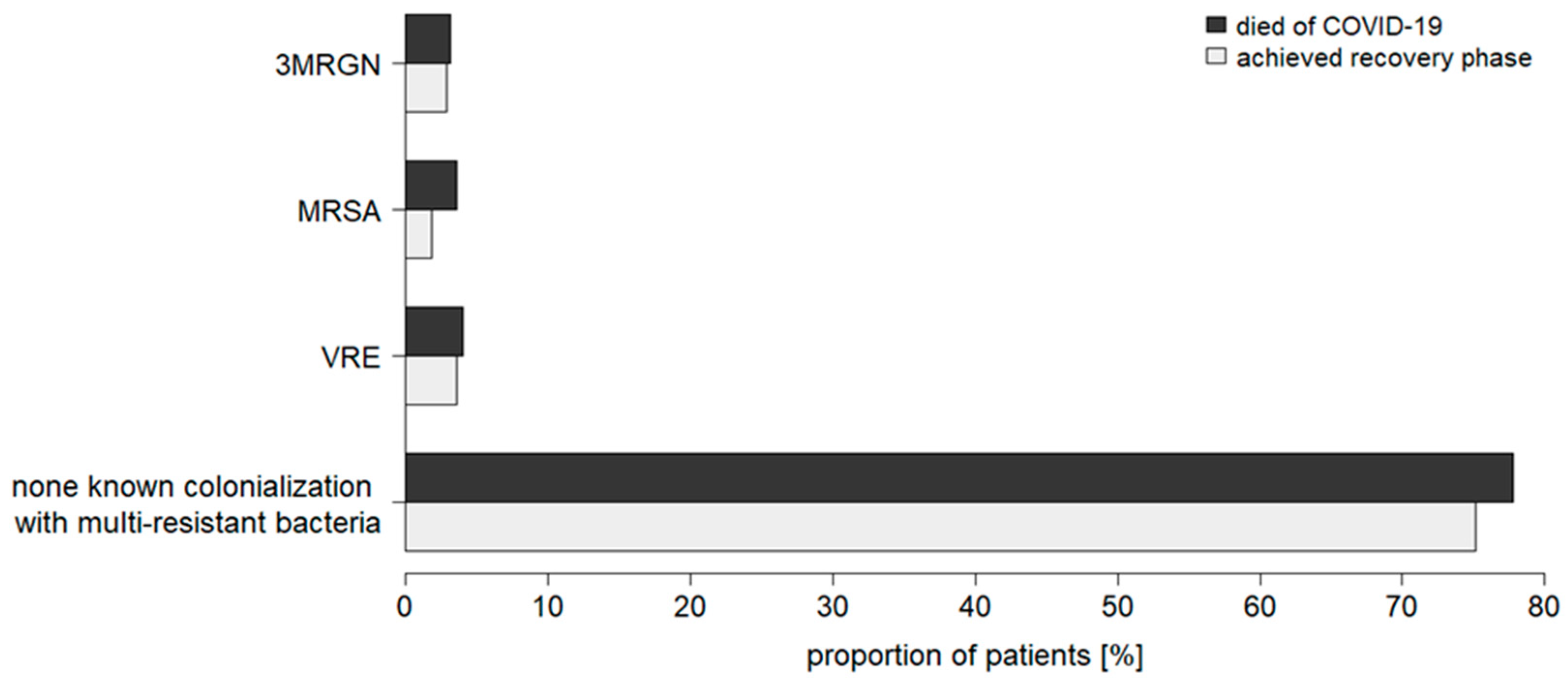
Furthermore, the data demonstrated no association between a pre-existing colonialization with a multidrug-resistant bacterium and mortality in critically ill COVID-19 patients (Figure 2). No significant difference in colonialization status was observed between recovered and deceased patients (Figure 2).
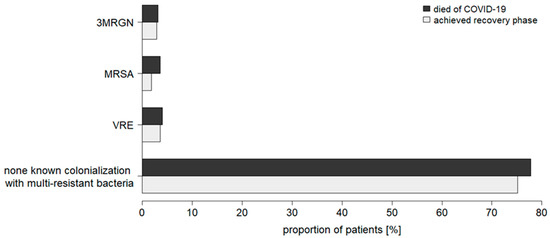
Figure 2.
Prevalence of community-acquired colonializations with multidrug-resistant bacteria in recovered and deceased patients critically ill with COVID-19 (total cohort). MRGN: multidrug-resistant Gram-negative bacteria; MRSA: methicillin-resistant Staphylococcus aureus; VRE: vancomycin-resistant enterococci.
3.3. Healthcare-Associated Bacterial and Fungal Infections
Information on hospital-acquired bacterial and fungal infections of critically ill patients in the ICU was available for 806 cases (96.0% of the total cohort). Overall, secondary bacterial infection was documented for 326 patients in the critical phase (40.4% of the cases), and secondary fungal infection was documented for 118 patients in the critical phase (14.6% of the cases).
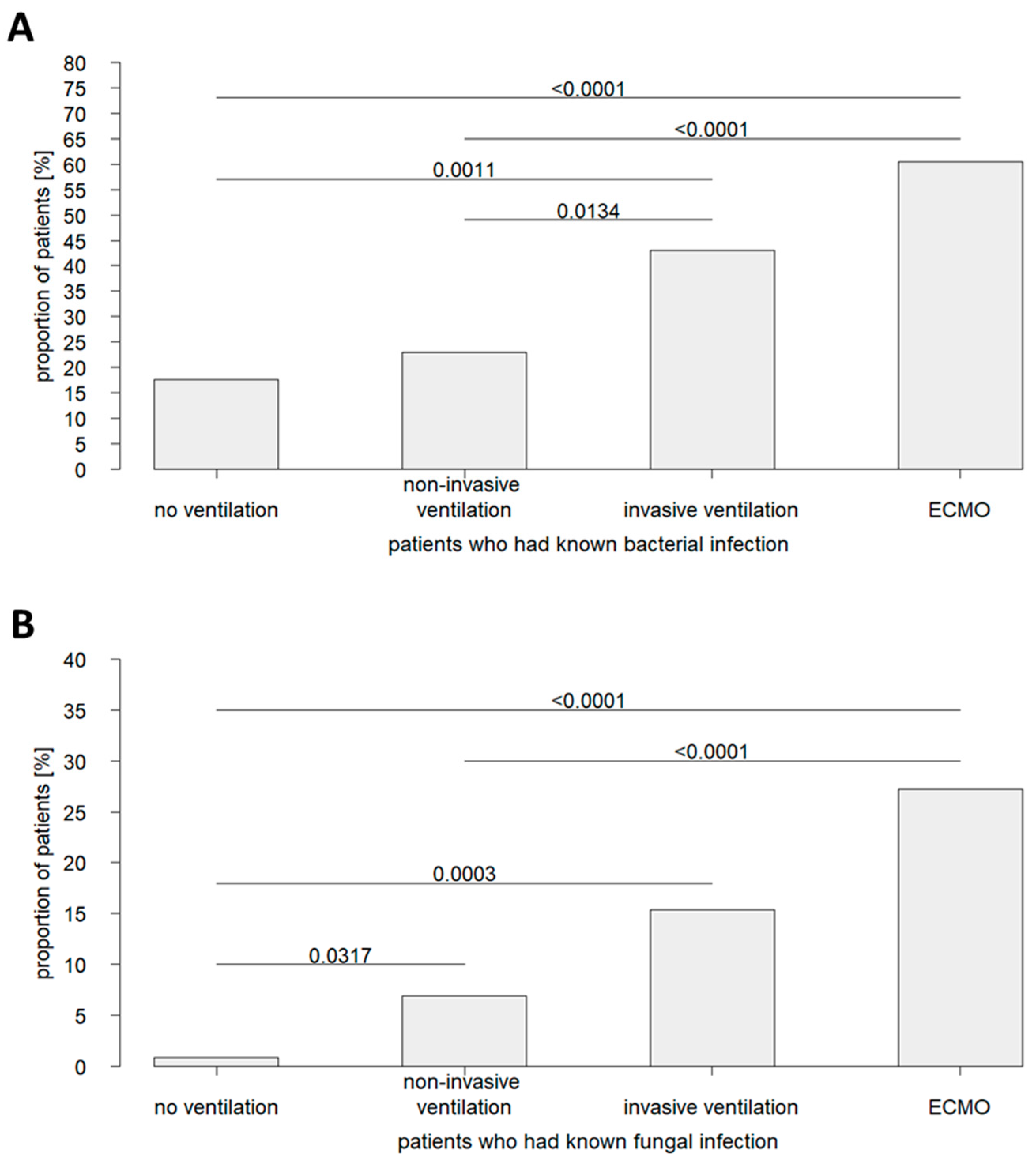
Remarkably, a comparative analysis of patient cohorts subdivided by ventilation therapy revealed significant differences in infection status (Figure 3). Healthcare-associated secondary infections with bacteria or fungi had an above-average prevalence in ECMO patients (bacterial co-infections in 60.5% of cases and fungal co-infections in 27.5% of cases). As such, ECMO patients were affected by nosocomial infections more frequently than invasively ventilated patients, in whom secondary co-infections with bacteria were documented in 43.1% of cases and with fungi in 15.4% of cases. However, a further lower, below-average prevalence of nosocomial infections was reported for the cohort of non-invasively ventilated patients (secondary bacterial co-infections in 23.0% of cases and secondary fungal co-infections in 6.9% of cases). In patients who did not receive ventilation, hospital-acquired bacterial co-infections were seen in 17.7% of cases and fungal co-infections in 0.9% of cases. These data support the hypothesis that invasive therapy procedures accompany an increased risk for healthcare-associated infections.
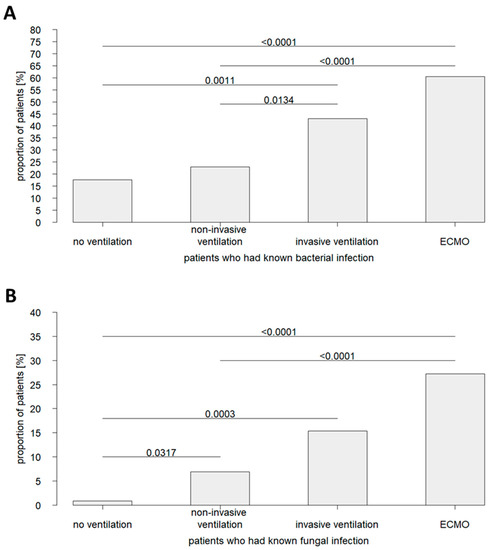
Figure 3.
Prevalence of secondary infections in patients critically ill with COVID-19 who received no ventilation therapy or were treated with non-invasive ventilation, invasive ventilation, or ECMO. Shown are the proportions of patients with (A) bacterial and (B) fungal infections of nosocomial origin.
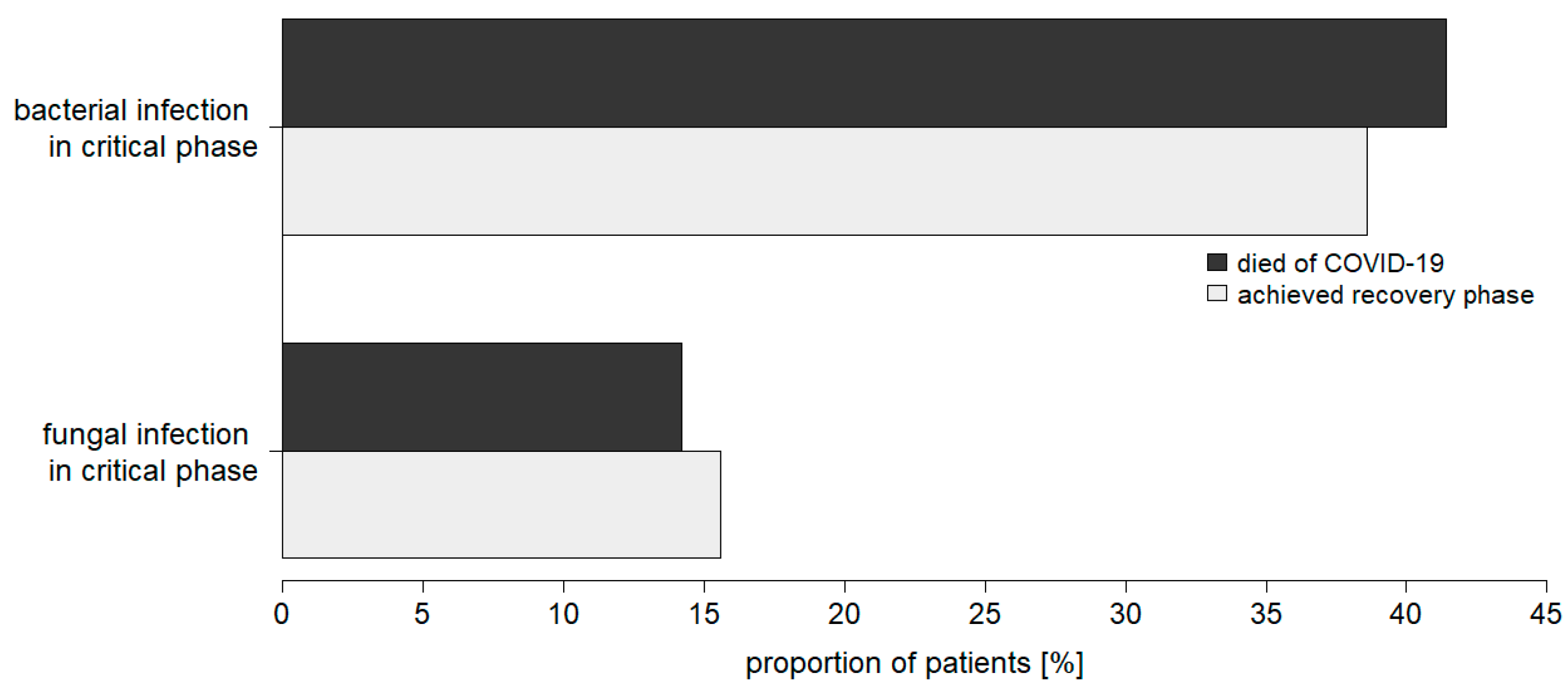
There were no significant differences in the frequencies of secondary bacterial or fungal infections when comparing critically ill COVID-19 patients who died or reached the recovery phase (Figure 4). Thus, no effect of hospital-acquired infections on outcome became apparent.
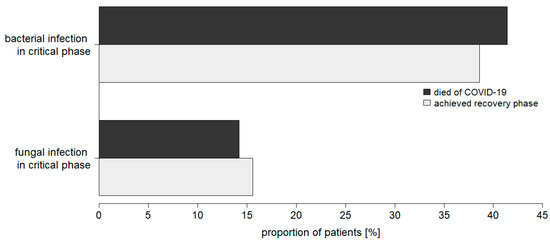
Figure 4.
Prevalence of secondary bacterial and fungal infections in recovered and deceased patients critically ill with COVID-19 (total cohort).
3.4. Antimicrobial Therapy: Frequency of Use and Clinical Benefit
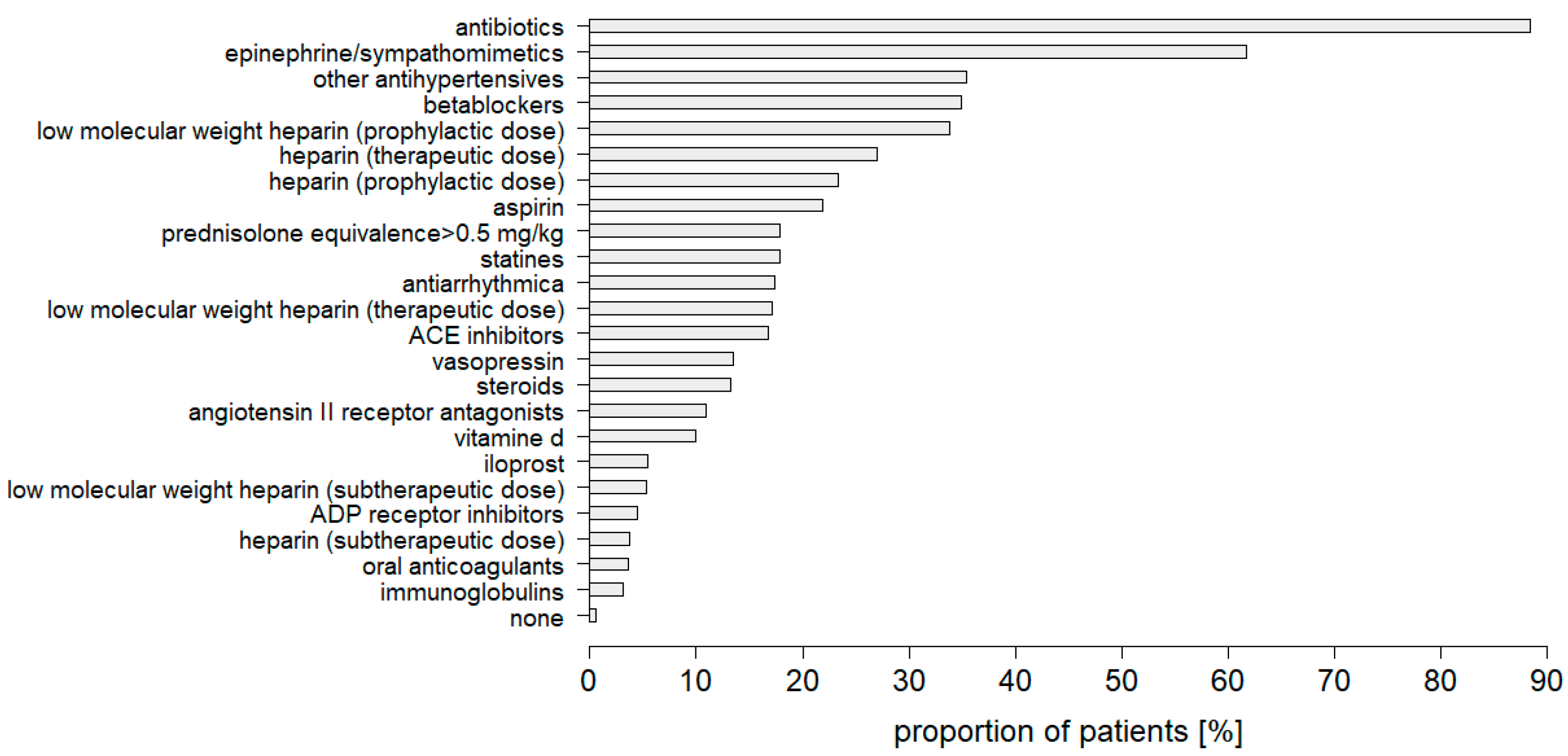
Antibiotic use data were available for only 285 critically ill patients with COVID-19 treated in the ICU (33.9% of the total cohort), an alarmingly low figure in terms of antimicrobial stewardship. An in-depth review of the pharmacologic treatment of these patients found that antibiotic treatment was the most frequently administered medication, even preceding epinephrine and sympathomimetics (Figure 5). Therefore, antibiotic therapy was administered in the vast majority of cases (88.4%), although bacterial infection was documented in just 40.4% of the overall patients and 47.6% of this particular patient subset.
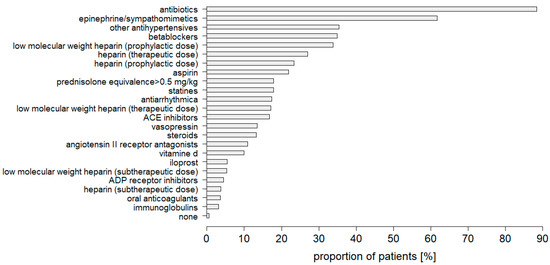
Figure 5.
Medication used in intensive care for patients critically ill with COVID-19.
A detailed examination of the patient cohorts subdivided by ventilation therapy revealed that almost all the ECMO patients (95.7% of cases) received antibiotic treatment. In the case of invasive ventilation, antibiotics were administered in 91.8% of the patients. Substantially less frequently, but still at a high level, antibiotics were used in non-invasively ventilated patients (71.9% of cases) and patients who did not receive ventilation therapy (75.0% of cases).
There was no difference in antibiotic use frequency between patients who died as a result of COVID-19 infection and those who reached the recovery phase. However, considering the high rate of antibiotic use, especially in intubated patients and patients on ECMO therapy, no valid conclusion can be drawn from this as to the clinical benefit of antibiotic treatment. While empiric antibiotic treatment might prevent the development of nosocomial infections, it also impedes microbial pathogen detection and, therefore, hinders specific anti-infective therapy when needed.
4. Discussion
In the present study, the relations between the colonization with nosocomial bacteria, the rate of nosocomial infections, the necessity to undergo ventilation, and the mode of ventilation were examined for COVID-19 patients treated in an ICU. The results of the study showed that colonializations with 3MRGN, MRSA, and VRE were similar in non-ventilated patients and patients undergoing non-invasive, invasive, and oxygenation ventilation, indicating that colonization was not associated with ventilation or its invasiveness. Moreover, a colonization with multi-resistant bacteria was not associated with a fatal outcome. On the other hand, the number of nosocomial infections significantly correlated with the invasiveness of the ventilation modus, indicated by the finding that the lowest infection rates were observed in non-ventilated COVID-19 patients, while the highest numbers occurred in patients oxygenated with ECMO. However, these infections were not related with a fatal outcome.
Since the outbreak of the pandemic, the field of COVID-19 has evolved. Vaccines have been developed that are proven to reduce the need for ICU treatment in the case of a breakthrough infection [33]. Furthermore, there are now drug treatment strategies that, when initiated in a timely manner, can have a mitigating effect on disease severity and, thus, counteract the need for critical care [8]. However, a significant number of patients still develop respiratory insufficiency requiring admission to an ICU and targeted ventilation. The present study clearly demonstrated that such treatment was associated with an increased risk of secondary infections, with the invasiveness of the ventilation technique used being an influential variable. This is even more important as no correlation between patient characteristics, such as age or comorbidities, and the occurrence of secondary infections was found.
Infections pose a significant problem in ICUs [10,19,34,35,36], especially in patients with viral respiratory infections. In severe influenza, for example, bacterial co-infections have been described in up to 20% to 30% of cases, and superinfections have been associated with pronounced disease severity and a higher risk of death [17,26,28,29,34,35,36]. Consequently, in critically ill COVID-19 patients, the prevalence of bacterial and fungal co-infections, their impact on the clinical course, and appropriate antimicrobial therapy in a primarily viral disease are of particular importance.
Since the very beginning of the pandemic, co-infections of COVID-19 patients have been reported [18,19,35,36,37,38,39]. It needs to be noted that the several studies reporting superinfections have not distinctly distinguished between community-acquired and healthcare-associated infections, thus limiting the validity of these studies. Our study, however, clearly showed that the vast majority of patients had no evidence of colonialization with bacterial multidrug-resistant microorganisms at baseline, and only a single-digit percentage of patients was affected by colonialization with 3MRGN, MRSA, or VRE at hospital presentation. Thus, for the group of COVID-19 patients with a critical course, it resulted that colonization at the time of diagnosis of SARS-CoV-2 infection was rare, especially with regard to the most clinically relevant multidrug-resistant pathogens. Indeed, other studies have also reported low rates of early infection and, rather, direct the focus to nosocomial infection [17,34]. Reported rates of secondary bacterial infections in critically ill ICU patients with COVID-19 have ranged from 8.1% to 42.8% [13,17,18,34,35,36,37,38,39]. There is also a wide range of reported infection rates with respect to secondary fungal infections. As such, a meta-analysis of eight studies related to COVID-19 patients treated in an ICU setting reported an infection rate of 9.6% (95% CI 6.8–12.4) [37]. Specifically, in mechanically ventilated COVID-19 patients, a multicenter prospective cohort study found a rate of invasive fungal infections of 26.7% [40]. One can only speculate as to the causes of the wide range of case numbers reported. Workload, unfavorable physician- or nurse-to-patient ratios, and a lack of laboratory capacity, especially in the early months of the pandemic, might have partially limited the capability for widespread infection control. For additional consideration, especially for critically ill ICU patients, the true prevalence of secondary infections may be underestimated due to the untimely deaths of these patients. In any case, our study provided clear evidence that nosocomial infections of bacterial and fungal origin were common in COVID-19 patients receiving intensive care and warrant awareness and adequate management. There is a need for the proper diagnosis and effective treatment of not only bacterial but also fungal infections in COVID-19 patients receiving intensive care.
Critically ill COVID-19 patients undergo a variety of invasive interventions in the ICU, such as mechanical ventilation and catheterization, which promote bacterial and fungal infections [10,13,17,19,21,26,38,39,41] and are described to be more frequently subject to additive bacterial and fungal infections compared to patients treated in regular wards [13,35,36,37,38,39]. We were, therefore, interested in the impact of the level of therapeutic invasiveness on the prevalence of healthcare-associated infections. Indeed, our data clearly proved that non-ventilated ICU patients were at low risk for secondary infections. The risk of infection increased markedly, even when non-invasive ventilation was used. A dramatic rise in the proportion of patients with nosocomial infections was seen with the use of invasive ventilation, and even more so with ECMO therapy. Actually, in ECMO-treated patients, healthcare-associated bacterial infections were present in about two-thirds of cases and healthcare-associated fungal infections in nearly one-third of cases. Our data provided evidence that the techniques used in intensive care for the treatment of COVID-19-induced respiratory insufficiency differed significantly with respect to risk profiles for secondary infections. Based on these data, close infection control is recommended, especially when invasive methods are required.
There is ongoing discussion as to whether secondary infections impact mortality in COVID-19 patients. Some studies have reported an association of nosocomial infections with adverse outcome, whereas other studies have found no such correlation [19,20,37,39,41,42]. In our study, the rates of secondary infections of surviving and deceased COVID-19 patients were not significantly different. The same was true for community-acquired colonialization with 3MRGN, MRSA, and VRE. Patient-associated factors, such as pre-existing conditions, may be critical in determining whether co-infections ultimately impact survival. In a risk analysis, Silva et al. already showed that co-infections increased the risk of death, specifically in patients with obesity, cardiovascular disease, or diabetes mellitus [41]. Obesity, cardiovascular disease, and diabetes mellitus are known risk factors for a critical course of SARS-CoV-2 infection and are common in ICU patients (as in the present study cohort). This raises the possibility of a vicious circle. Large cohort studies are needed to investigate this in detail, with particular priority on ICU patients, given their high risk of developing secondary infections.
Several guidelines, such as those from the World Health Organization (WHO) and the Surviving Sepsis Campaign, advocate the use of empiric antibiotics in patients with severe COVID-19 [7,43]. This explains why, in our study, the absolute majority of patients (88.4%) were treated with antibiotics, despite the fact that only half of these patients had a positive finding of bacterial infection. Other studies have consistently reported hospitalized COVID-19 patients receiving antimicrobial therapy in 50% to 100% of cases [13,15,18,20,26,27,34,36,38]. The undifferentiated use of antimicrobial agents is known to increase selection pressure and may promote the spread of resistant bacterial strains. Indeed, there are concerns that the increased usage of antibiotics in the context of the COVID-19 pandemic may worsen the issue of multidrug-resistant pathogens worldwide [27,28,29,34]. Strict adherence to antibiotic stewardship programs, effective implementation of infection control procedures, and maintenance of established hygiene standards need to be upheld even in pandemic settings. This is particularly true for ICUs, as invasive treatments are key to the development of secondary infections, as illustrated by the present study.
Our study has certain limitations. Due to its retrospective nature, data availability was limited to the medical records added to the LEOSS registry. We did not have information of interest, such as the presence of antibiotic resistance or the type, dosage, and timing of antibiotic, antifungal, or immunosuppressant drugs. Accordingly, we could not make statements on these potential influencing factors. This study included ICU patients suffering from COVID-19 from Europe, predominantly Germany, which may limit the generalizability of our findings.
5. Conclusions
Healthcare-associated infections are common in critically ill COVID-19 patients treated in ICUs. Our study highlighted the importance of the type of intensive care treatment when it came to nosocomial infections. Patients receiving invasive ventilation had markedly increased rates of secondary bacterial and fungal infections compared with those receiving non-invasive treatment. Another distinct increase in infection rates was documented in ECMO-treated patients. This knowledge should inform future treatment decisions in the ICU.
Author Contributions
Conceptualization, S.B., D.E. and J.S.; methodology, S.B. and J.S.; validation, M.L.d.H., D.E. and J.S.; formal analysis, M.L.d.H. and J.S.; investigation, M.L.d.H., D.E. and J.S.; data curation, S.B., S.R., J.J.V., C.D.S., C.E.M.K., M.H., M.S. and F.H.; writing—original draft preparation, J.S.; writing—review and editing, M.L.d.H., S.B. and D.E.; visualization, M.L.d.H.; supervision, J.S.; project administration, J.S. All authors have read and agreed to the published version of the manuscript.
Funding
The LEOSS registry is supported by the German Center for Infection Research (DZIF) and the Willy Robert Pitzer Foundation.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Approval for LEOSS was obtained from the applicable local ethics committees of all participating centers and registered at the German Clinical Trails Register (DRKS, No. S00021145).
Informed Consent Statement
Patient consent was waived, as the study was based on a Scientific Use File (SUF) generated from the Lean European Open Survey on SARS-CoV-2-Infected Patients (LEOSS) registry. For the LEOSS database, data collection was performed fully anonymized, only once per case, and retrospectively after treatment was finished or the patient had died.
Data Availability Statement
Patient data from the LEOSS registry are subject to the LEOSS governance, data use, and access policy (policy text available on https://leoss.net; accessed on 4 August 2022).
Acknowledgments
We express our deep gratitude to all the study teams supporting the LEOSS study. The LEOSS study group contributed at least 5 per million to the analyses of this study from: University Hospital Regensburg (Frank Hanses), University Hospital Freiburg (Siegbert Rieg), Technical University of Munich (Christoph Spinner), Hospital Ingolstadt (Stefan Borgmann), Klinikum Dortmund gGmbH, Hospital of University Witten/Herdecke (Martin Hower), University Hospital Frankfurt (Maria Vehreschild), University Hospital Wuerzburg (Nora Isberner), University Hospital Tuebingen (Siri Göpel), Hospital Maria Hilf GmbH Moenchengladbach (Juergen vom Dahl), University Hospital Augsburg (Christoph Roemmele), University Hospital Jena (Maria Madeleine Ruethrich), University Hospital Cologne (Norma Jung), University Hospital Erlangen (Richard Strauss), University Hospital Ulm (Beate Gruener), Hospital Bremen-Center (Christian Hohmann), Hospital Ernst von Bergmann (Lukas Tometten), Hospital Passau (Julia Lanznaster), University Hospital Saarland (Robert Bals), Municipal Hospital Karlsruhe (Christian Degenhardt), University Hospital Duesseldorf (Bjoern-Erik Jensen), University Hospital Heidelberg (Uta Merle), Johannes Wesling Hospital Minden Ruhr University Bochum (Kai Wille), University Hospital Dresden (Katja de With), Bundeswehr Hospital Koblenz (Dominic Rauschning), University Hospital of Giessen and Marburg (Janina Trauth), University Hospital Essen (Sebastian Dolff), University Hospital Schleswig-Holstein Kiel (Anette Friedrichs), Elbland Hospital Riesa (Joerg Schubert), Malteser Hospital St. Franziskus Flensburg (Milena Milovanovic), Marien Hospital Herne Ruhr University Bochum (Timm Westhoff), Clinic Munich (Wolfgang Guggemos), Catholic Hospital Bochum (St. Josef Hospital) Ruhr University Bochum (Kerstin Hellwig), Practice for general medicine Drs. Elisabeth Schroedter & Gabriele Mueller-Joerger Kuenzelsau (Gabriele Mueller-Joerger), Hospital Universitari Arnau de Vilanova (Juan Antonio Schoenenberger-Arnaiz), Hospital Braunschweig (Jan Kielstein), Hospital Leverkusen (Lukas Eberwein), University Hospital Munich/ LMU (Michael von Bergwelt-Baildon), Agaplesion Diakonie Hospital Rotenburg (David Heigener), Thorax University Hospital Heidelberg (Felix Herth), and Evangelisches Hospital Saarbruecken (Mark Neufang). The LEOSS study infrastructure group includes: Jörg Janne Vehreschild (Goethe University Frankfurt), Susana M. Nunes de Miranda (University Hospital of Cologne), Carolin E. M. Koll (University Hospital of Cologne), Melanie Stecher (University Hospital of Cologne), Lisa Pilgram (Goethe University Frankfurt), Nick Schulze (University Hospital of Cologne), Sandra Fuhrmann (University Hospital of Cologne), Annika Claßen (University Hospital of Cologne), Bernd Franke (University Hospital of Cologne), and Fabian Praßer (Charité, Universitätsmedizin Berlin).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sorbello, M.; El-Boghdadly, K.; Di Giacinto, I.; Cataldo, R.; Esposito, C.; Falcetta, S.; Merli, G.; Cortese, G.; Corso, R.M.; Bressan, F.; et al. The Italian coronavirus disease 2019 outbreak: Recommendations from clinical practice. Anaesthesia 2020, 75, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Der Nigoghossian, C.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow. J. Am. Coll. Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef]
- Pfeifer, M.; Ewig, S.; Voshaar, T.; Randerath, W.J.; Bauer, T.; Geiseler, J.; Dellweg, D.; Westhoff, M.; Windisch, W.; Schoenhofer, B.; et al. Position Paper for the State-of-the-Art Application of Respiratory Support in Patients with COVID-19. Respiration 2020, 99, 521–541. [Google Scholar] [CrossRef]
- Kluge, S.; Janssens, U.; Welte, T.; Weber-Carstens, S.; Marx, G.; Karagiannidis, C. German recommendations for critically ill patients with COVID-19. Med. Klin. Intensivmed. 2020, 115, 111–114. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Mostert, C.; Hentschker, C.; Voshaar, T.; Malzahn, J.; Schillinger, G.; Klauber, J.; Janssens, U.; Marx, G.; Weber-Carstens, S.; et al. Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: An observational study. Lancet Resp. Med. 2020, 8, 853–862. [Google Scholar] [CrossRef]
- Thomas-Rueddel, D.; Winning, J.; Dickmann, P.; Ouart, D.; Kortgen, A.; Janssens, U.; Bauer, M. Coronavirus disease 2019 (COVID-19): Update for anesthesiologists and intensivists March 2020. Anaesthesist 2021, 70, 1–10. [Google Scholar] [CrossRef]
- Alhazzani, W.; Moller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Int. Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef]
- Fachgruppe COVRIIN beim Robert-Koch-Institut. Antivirale Therapie in der Frühphase einer SARS-CoV-2-Infektion: Bei Patienten mit Risikofaktoren für einen Schweren Verlauf von COVID-19 (bei Asymptomatischen Patienten oder Patienten mit milder COVID-19); Bewertung durch die Fachgruppe COVRIIN beim Robert Koch-Institut. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/COVRIIN_Dok/Antivirale_Therapie_Fruehphase.pdf?__blob=publicationFile (accessed on 29 June 2022).
- Fichtner, F.; Moerer, O.; Weber-Carstens, S.; Nothacker, M.; Kaisers, U.; Laudi, S.; Grp, G. Clinical Guideline for Treating Acute Respiratory Insufficiency with Invasive Ventilation and Extracorporeal Membrane Oxygenation: Evidence-Based Recommendations for Choosing Modes and Setting Parameters of Mechanical Ventilation. Respiration 2019, 98, 357–372. [Google Scholar] [CrossRef]
- Vincent, J.L.; Bihari, D.J.; Suter, P.M.; Bruining, H.A.; White, J.; Nicolaschanoin, M.H.; Wolff, M.; Spencer, R.C.; Hemmer, M. The Prevalence of Nosocomial Infection in Intensive-Care Units in Europe—Results of the European Prevalence of Infection in Intensive-Care (EPIC) Study. JAMA-J. Am. Med. Assoc. 1995, 274, 639–644. [Google Scholar] [CrossRef]
- Tobin, M.J. Basing Respiratory Management of COVID-19 on Physiological Principles. Am. J. Respir. Crit. Care Med. 2020, 201, 1319–1320. [Google Scholar] [CrossRef] [Green Version]
- Chiurlo, M.; Mastrangelo, A.; Ripa, M.; Scarpellini, P. Invasive fungal infections in patients with COVID-19: A review on pathogenesis, epidemiology, clinical features, treatment, and outcomes. New Microbiol. 2021, 44, 71–83. [Google Scholar] [PubMed]
- Chong, W.H.; Saha, B.K.; Ramani, A.; Chopra, A. State-of-the-art review of secondary pulmonary infections in patients with COVID-19 pneumonia. Infection 2021, 49, 591–605. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.D.; Fairfield, C.J.; Drake, T.M.; Turtle, L.; Seaton, R.A.; Wootton, D.G.; Sigfrid, L.; Harrison, E.M.; Docherty, A.B.; de Silva, T.I.; et al. Co-infections, secondary infections, and antimicrobial use in patients hospitalised with COVID-19 during the first pandemic wave from the ISARIC WHO CCP-UK study: A multicentre, prospective cohort study. Lancet Microbe 2021, 2, E354–E365. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and Fungal Coinfection in Individuals With Coronavirus: A Rapid Review To Support COVID-19 Antimicrobial Prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef] [PubMed]
- Manna, S.; Baindara, P.; Mandal, S.M. Molecular pathogenesis of secondary bacterial infection associated to viral infections including SARS-CoV-2. J. Infect. Public Health 2020, 13, 1397–1404. [Google Scholar] [CrossRef]
- Pasero, D.; Cossu, A.P.; Terragni, P. Multi-Drug Resistance Bacterial Infections in Critically Ill Patients Admitted with COVID-19. Microorganisms 2021, 9, 1773. [Google Scholar] [CrossRef]
- Fehér, Á.; Szarvas, Z.; Lehoczki, A.; Fekete, M.; Fazekas-Pongor, V. Co-infections in COVID-19 patients and correlation with mortality rate. Minireview. Physiol. Int. 2022, 109, 1–8. [Google Scholar] [CrossRef]
- Roudbary, M.; Kumar, S.; Kumar, A.; Cernakova, L.; Nikoomanesh, F.; Rodrigues, C.F. Overview on the Prevalence of Fungal Infections, Immune Response, and Microbiome Role in COVID-19 Patients. J. Fungi 2021, 7, 720. [Google Scholar] [CrossRef]
- Grasselli, G.; Scaravilli, V.; Mangioni, D.; Scudeller, L.; Alagna, L.; Bartoletti, M.; Bellani, G.; Biagioni, E.; Bonfanti, P.; Bottino, N.; et al. Hospital-Acquired Infections in Critically Ill Patients With COVID-19. Chest 2021, 160, 454–465. [Google Scholar] [CrossRef]
- Falcone, M.; Tiseo, G.; Giordano, C.; Leonildi, A.; Menichini, M.; Vecchione, A.; Pistello, M.; Guarracino, F.; Ghiadoni, L.; Forfori, F.; et al. Predictors of hospital-acquired bacterial and fungal superinfections in COVID-19: A prospective observational study. J. Antimicrob. Chemother. 2021, 76, 1078–1084. [Google Scholar] [CrossRef]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.-H.; Dugas, A. The frequency of influenza and bacterial coinfection: A systematic review and meta-analysis. Influenza Other Respir. Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef] [PubMed]
- MacIntyre, C.R.; Chughtai, A.A.; Barnes, M.; Ridda, I.; Seale, H.; Toms, R.; Heywood, A. The role of pneumonia and secondary bacterial infection in fatal and serious outcomes of pandemic influenza a(H1N1)pdm09. BMC Infect. Dis. 2018, 18, 637. [Google Scholar] [CrossRef]
- Rice, T.W.; Rubinson, L.; Uyeki, T.M.; Vaughn, F.L.; John, B.B.; Miller, R.R., II; Higgs, E.; Randolph, A.G.; Smoot, B.E.; Thompson, B.T.; et al. Critical illness from 2009 pandemic influenza A virus and bacterial coinfection in the United States. Crit. Care Med. 2012, 40, 1487–1498. [Google Scholar] [CrossRef] [PubMed]
- Esper, F.P.; Spahlinger, T.; Zhou, L. Rate and influence of respiratory virus co-infection on pandemic (H1N1) influenza disease. J. Infect. 2011, 63, 260–266. [Google Scholar] [CrossRef]
- Cox, M.J.; Loman, N.; Bogaert, D.; O’Grady, J. Co-infections: Potentially lethal and unexplored in COVID-19. Lancet Microbe 2020, 1, E11. [Google Scholar] [CrossRef]
- Getahun, H.; Smith, I.; Trivedi, K.; Paulin, S.; Balkhy, H.H. Tackling antimicrobial resistance in the COVID-19 pandemic. Bull World Health Organ. 2020, 98, 442. [Google Scholar] [CrossRef]
- Ginsburg, A.S.; Klugman, K.P. COVID-19 pneumonia and the appropriate use of antibiotics. Lancet Glob. Health 2020, 8, E1453–E1454. [Google Scholar] [CrossRef]
- Huttner, B.D.; Catho, G.; Pano-Pardo, J.R.; Pulcini, C.; Schouten, J. COVID-19: Don’t neglect antimicrobial stewardship principles! Clin. Microbiol. Infect. 2020, 26, 808–810. [Google Scholar] [CrossRef]
- Meintrup, D.; Borgmann, S.; Seidl, K.; Stecher, M.; Jakob, C.E.M.; Pilgram, L.; Spinner, C.D.; Rieg, S.; Isberner, N.; Hower, M.; et al. Specific Risk Factors for Fatal Outcome in Critically Ill COVID-19 Patients: Results from a European Multicenter Study. J. Clin. Med. 2021, 10, 3855. [Google Scholar] [CrossRef]
- Jakob, C.E.M.; Kohlmayer, F.; Meurers, T.; Vehreschild, J.J.; Prasser, F. Design and evaluation of a data anonymization pipeline to promote Open Science on COVID-19. Sci. Data 2020, 7, 435. [Google Scholar] [CrossRef]
- Jakob, C.E.M.; Borgmann, S.; Duygu, F.; Behrends, U.; Hower, M.; Merle, U.; Friedrichs, A.; Tometten, L.; Hanses, F.; Jung, N.; et al. First results of the Lean European Open Survey on SARS-CoV-2-Infected Patients (LEOSS). Infection 2021, 49, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Bahl, A.; Johnson, S.; Maine, G.; Garcia, M.H.; Nimmagadda, S.; Qu, L.; Chen, N.-W. Vaccination reduces need for emergency care in breakthrough COVID-19 infections: A multicenter cohort study. Lancet Reg Health Am. 2021, 4, 100065. [Google Scholar] [CrossRef] [PubMed]
- Peghin, M.; Vena, A.; Graziano, E.; Giacobbe, D.R.; Tascini, C.; Bassetti, M. Improving management and antimicrobial stewardship for bacterial and fungal infections in hospitalized patients with COVID-19. Ther. Adv. Infect. Dis. 2022, 9, 28. [Google Scholar] [CrossRef]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Alhumaid, S.; Al Mutair, A.; Al Alawi, Z.; Alshawi, A.M.; Alomran, S.A.; Almuhanna, M.S.; Almuslim, A.A.; Bu Shafia, A.H.; Alotaibi, A.M.; Ahmed, G.Y.; et al. Coinfections with Bacteria, Fungi, and Respiratory Viruses in Patients with SARS-CoV-2: A Systematic Review and Meta-Analysis. Pathogens 2021, 10, 809. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Leung, V.; Raybardhan, S.; Lo, J.; Kan, T.; Leung, F.; Westwood, D.; Daneman, N.; MacFadden, D.R.; et al. Predictors and microbiology of respiratory and bloodstream bacterial infection in patients with COVID-19: Living rapid review update and meta-regression. Clin. Microbiol. Infect. 2022, 28, 491–501. [Google Scholar] [CrossRef]
- Musuuza, J.S.; Watson, L.; Parmasad, V.; Putman-Buehler, N.; Christensen, L.; Safdar, N. Prevalence and outcomes of co-infection and superinfection with SARS-CoV-2 and other pathogens: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0251170. [Google Scholar] [CrossRef]
- White, P.L.; Dhillon, R.; Cordey, A.; Hughes, H.; Faggian, F.; Soni, S.; Pandey, M.; Whitaker, H.; May, A.; Morgan, M.; et al. A national strategy to diagnose COVID-19 associated invasive fungal disease in the ICU. Clin. Infect. Dis. 2020, 73, e1634–e1644. [Google Scholar] [CrossRef]
- Silva, D.L.; Lima, C.M.; Magalhaes, V.C.R.; Baltazar, L.M.; Peres, N.T.A.; Caligiorne, R.B.; Moura, A.S.; Fereguetti, T.; Martins, J.C.; Rabelo, L.F.; et al. Fungal and bacterial coinfections increase mortality of severely ill COVID-19 patients. J. Hosp. Infect. 2021, 113, 145–154. [Google Scholar] [CrossRef]
- Bardi, T.; Pintado, V.; Gomez-Rojo, M.; Escudero-Sanchez, R.; Azzam Lopez, A.; Diez-Remesal, Y.; Martinez Castro, N.; Ruiz-Garbajosa, P.; Pestana, D. Nosocomial infections associated to COVID-19 in the intensive care unit: Clinical characteristics and outcome. Europ. J. Clin. Microbiol. Infect. Dis. 2021, 40, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Wolrd Health Organization. Living Guidance for Clinical Management of COVID-19: Living Guidance, 23 November 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/349321/WHO-2019-nCoV-clinical-2021.2-eng.pdf (accessed on 4 August 2022).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).