

Efficacy and Safety of Domperidone in Combination with Proton Pump Inhibitors in Gastroesophageal Reflux Disease: A Systematic Review and Meta-Analysis of Randomised Controlled Trials


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Outcome Measures
2.4. Data Extraction and Quality Assessment
2.5. Data Synthesis and Analysis
3. Results
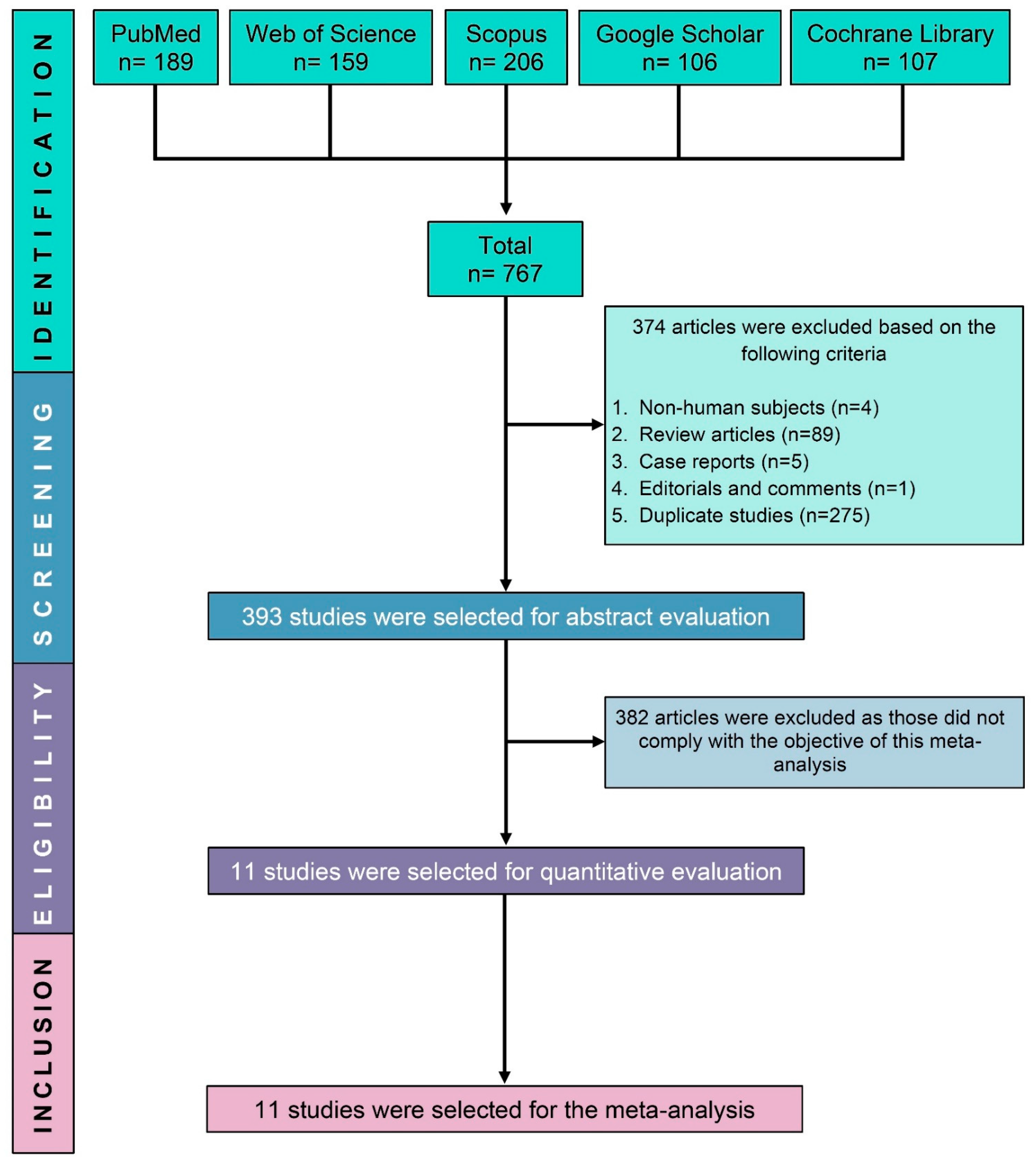
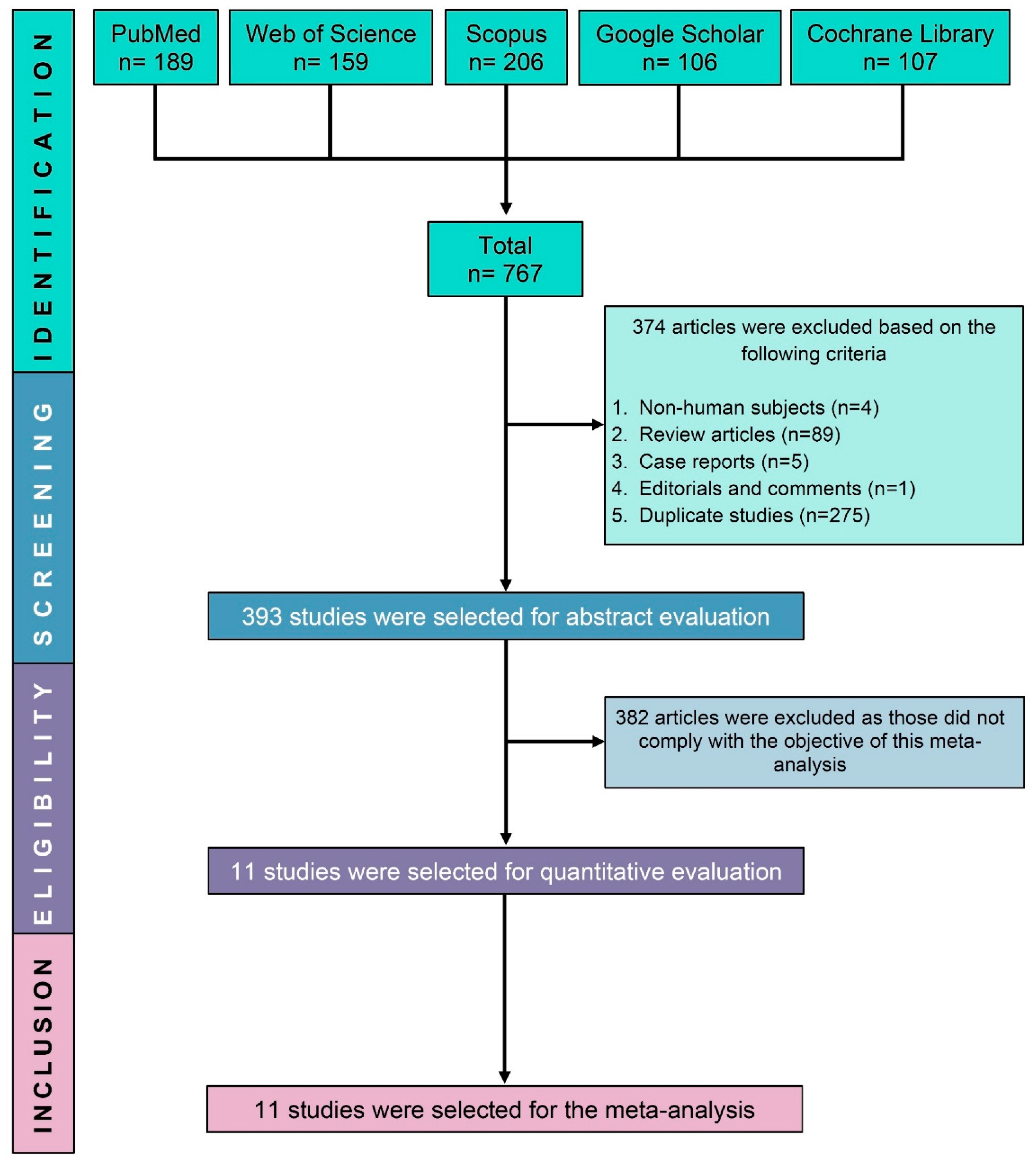
3.1. Search Outcomes
3.2. Study Characteristics
3.3. Study Quality
3.4. Primary Outcomes (Efficacy of Domperidone in Combination with PPI)
3.4.1. Modification of Symptom Scores
3.4.2. Heartburn Score, Reflux Times and Frequency
3.4.3. Improvement of Oesophageal pH
3.5. Secondary Outcomes (Safety of Domperidone in Combination with PPI)
Adverse Events
3.6. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nirwan, J.S.; Hasan, S.S.; Babar, Z.-U.-D.; Conway, B.R.; Ghori, M.U. Global prevalence and risk factors of gastro-oesophageal reflux disease (GORD): Systematic review with meta-analysis. Sci. Rep. 2020, 10, 5814. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.Y.; Kang, J.Y.; Seow, A. Prevalence of gastrointestinal symptoms in a multiracial asian population, with particular reference to reflux-type symptoms. Am. J. Gastroenterol. 1998, 93, 1816–1822. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.Y.; Chan, Y.H.; Kang, J.Y. Increasing trend of reflux esophagitis and decreasing trend of Helicobacter pylori infection in patients from a multiethnic Asian country. Am. J. Gastroenterol. 2005, 100, 1923–1928. [Google Scholar] [CrossRef]
- DeVault, K.R.; Castell, D.O. Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. Am. J. Gastroenterol. 2005, 100, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Talley, N.J.; Zand Irani, M. Optimal management of severe symptomatic gastroesophageal reflux disease. J. Intern. Med. 2021, 289, 162–178. [Google Scholar] [CrossRef] [PubMed]
- Durazzo, M.; Lupi, G.; Cicerchia, F.; Ferro, A.; Barutta, F.; Beccuti, G.; Gruden, G.; Pellicano, R. Extra-esophageal presentation of gastroesophageal reflux disease: 2020 update. J. Clin. Med. 2020, 9, 2559. [Google Scholar] [CrossRef]
- Rajendra, S.; Alahuddin, S. Racial differences in the prevalence of heartburn. Aliment. Pharmacol. Ther. 2004, 19, 375–376. [Google Scholar] [CrossRef]
- Kumar, D.; Vinod, K.; Razavi, M. Gastroesophageal reflux disease: A Review of Superior Effects of Proton Pump Inhibitors and Prokinetic agents as a Combination Therapy versus Monotherapy. Management 2011, 705, 701–705. [Google Scholar]
- Nonaka, T.; Kessoku, T.; Ogawa, Y.; Yanagisawa, S.; Shiba, T.; Sakaguchi, T.; Atsukawa, K.; Takahashi, H.; Sekino, Y.; Iida, H. Comparative study of 2 different questionnaires in Japanese patients: The quality of life and utility evaluation survey technology questionnaire (QUEST) versus the frequency scale for the symptoms of gastroesophageal reflux disease questionnaire (FSSG). J. Neurogastroenterol. Motil. 2013, 19, 54. [Google Scholar] [CrossRef]
- Jonasson, C.; Wernersson, B.; Hoff, D.; Hatlebakk, J. Validation of the GerdQ questionnaire for the diagnosis of gastro-oesophageal reflux disease. Aliment. Pharmacol. Ther. 2013, 37, 564–572. [Google Scholar] [CrossRef]
- Bai, Y.; Du, Y.; Zou, D.; Jin, Z.; Zhan, X.; Li, Z.S.; Yang, Y.; Liu, Y.; Zhang, S.; Qian, J. Gastroesophageal Reflux Disease Questionnaire (GerdQ) in real-world practice: A national multicenter survey on 8065 patients. J. Gastroenterol. Hepatol. 2013, 28, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Cooper, G.S.; Mourand, W.A.; Koroukian, S.M. Diagnosis and treatment of gastroesophageal reflux disease in Ohio Medicaid patients: Practice patterns and temporal trends. Pharmacoepidemiol. Drug Saf. 2004, 13, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Langen, M.L.-v.; Zanten, S.V.V. Does the evidence show that prokinetic agents are effective in healing esophagitis and improving symptoms of GERD? Open Med. 2007, 1, 3–5. [Google Scholar]
- Cresi, F.; Marinaccio, C.; Russo, M.C.; Miniero, R.; Silvestro, L. Short-term effect of domperidone on gastroesophageal reflux in newborns assessed by combined intraluminal impedance and pH monitoring. J. Perinatol. 2008, 28, 766–770. [Google Scholar] [CrossRef]
- Johnson, A.G. Domperidone in the Treatment of Gastroesophageal Reflux Disease. In Advances in Drug Therapy of Gastroesophageal Reflux Disease; Karger Publishers: Basel, Switzerland, 2015; Volume 20, pp. 45–53. [Google Scholar]
- Bor, S.; Demir, M.; Ozdemir, O.; Yuksel, K. A meta-analysis on the cardiac safety profile of domperidone compared to metoclopramide. United Eur. Gastroenterol. J. 2018, 6, 1331–1346. [Google Scholar] [CrossRef]
- Jung, D.H.; Huh, C.W.; Lee, S.K.; Park, J.C.; Shin, S.K.; Lee, Y.C. A Systematic Review and Meta-analysis of Randomized Control Trials: Combination Treatment With Proton Pump Inhibitor Plus Prokinetic for Gastroesophageal Reflux Disease. J. Neurogastroenterol. Motil. 2021, 27, 165–175. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Hasim, N.; Bakar, M.A.A.; Islam, M.A. Efficacy and Safety of Isotonic and Hypotonic Intravenous Maintenance Fluids in Hospitalised Children: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Children 2021, 8, 785. [Google Scholar] [CrossRef]
- Seak, Y.S.; Nor, J.; Tuan Kamauzaman, T.H.; Arithra, A.; Islam, M.A. Efficacy and Safety of Intranasal Ketamine for Acute Pain Management in the Emergency Setting: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3978. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Shaoxiang, Z. Combined application of omeprazole and domperidone in the treatment of gastroesophageal reflux Observation of the curative effect of the disease. Chin. Sanit. Stand. Manag. 2017, 8, 84–85. [Google Scholar]
- Junsuan, S.; County, B.; Province, H. Combined treatment of omeprazole and domperidone in the treatment of gastroesophageal reflux in children Observation of the clinical efficacy of the disease. Chin. Community Physician 2018, 34, 68–70. [Google Scholar]
- Jianzhong, L. Omeprazole combined with domperidone in the treatment of children with gastroesophageal reflux disease Observation of clinical efficacy. Chin. Med. Rec. 2019, 20, 73–75. [Google Scholar]
- Yajie, Y. Clinical observation of domperidone combined with omeprazole in the treatment of children with gastroesophageal reflux disease. Chin. Pract. Med. 2019, 14, 86–88. [Google Scholar]
- Huiying, L. Omeprazole combined with domperidone in the treatment of asthma with gastroesophageal reflux. Med. Info. 2020, 33, 144–145. [Google Scholar]
- Wang, F.; Zhang, X.; Wang, J. Effects of domperidone in combination with omeprazole in the treatment of chronic superficial gastritis. Pak. J. Med. Sci. 2017, 33, 306–309. [Google Scholar] [CrossRef]
- Ndraha, S. Combination of PPI with a prokinetic drug in gastroesophageal reflux disease. Acta Med. Indones 2011, 43, 233–236. [Google Scholar]
- Marakhouski, K.Y.; Karaseva, G.A.; Ulasivich, D.N.; Marakhouski, Y.K. Omeprazole-domperidone fixed dose combination vs omeprazole monotherapy: A phase 4, open-label, comparative, parallel randomized controlled study in mild to moderate gastroesophageal reflux disease. Clin. Med. Insights Gastroenterol. 2017, 10, 1–8. [Google Scholar] [CrossRef]
- Puranik, R.U.; Karandikar, Y.S.; Bhat, S.M.; Patil, V.A. Pharmacoeconomic evaluation of pantoprazole and pantoprazole plus domperidone in treatment of patients with gerd. J. Clin. Diagn. Res. 2018, 12, 1–5. [Google Scholar] [CrossRef]
- Bediwy, A.S.; Al-Biltagi, M.; Amer, H.G.; Saeed, N.K. Combination therapy versus monotherapy for gastroesophageal reflux in children with difficult-to-treat bronchial asthma. Egypt. J. Chest Dis. Tuberc. 2014, 63, 33–38. [Google Scholar] [CrossRef]
- Taghvaei, T.; Kazemi, A.; Hosseini, V.; Hamidian, M.; Fakheri, H.T.; Hashemi, S.A.; Maleki, I. Evaluation of the additive effect of domperidone on patients with refractory gastroesophageal reflux disease; a randomized double blind clinical trial. Middle East J. Dig. Dis. 2019, 11, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Katzka, D.A.; Pandolfino, J.E.; Kahrilas, P.J. Phenotypes of gastroesophageal reflux disease: Where Rome, Lyon, and Montreal meet. Clin. Gastroenterol. Hepatol. 2020, 18, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Rossor, T.; Andradi, G.; Bhat, R.; Greenough, A. Investigation and management of gastro-oesophageal reflux in United Kingdom neonatal intensive care units. Acta Paediatr. 2018, 107, 48–51. [Google Scholar] [CrossRef]
- Xi, L.; Zhu, J.; Zhang, H.; Muktiali, M.; Li, Y.; Wu, A. The treatment efficacy of adding prokinetics to PPIs for gastroesophageal reflux disease: A meta-analysis. Esophagus 2021, 18, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.H.; Chen, W.X.; Qian, L.J.; Li, S.; Gu, M.; Shi, R.H. Addition of prokinetics to PPI therapy in gastroesophageal reflux disease: A meta-analysis. World J. Gastroenterol. 2014, 20, 2412–2419. [Google Scholar] [CrossRef]
- Hemmink, G.J.; Bredenoord, A.J.; Weusten, B.L.; Monkelbaan, J.F.; Timmer, R.; Smout, A.J. Esophageal pH-impedance monitoring in patients with therapy-resistant reflux symptoms:‘on’or ‘off’proton pump inhibitor? Am. J. Gastroenterol. 2008, 103, 2446–2453. [Google Scholar] [CrossRef]
- Turk, H.; Hauser, B.; Brecelj, J.; Vandenplas, Y.; Orel, R. Effect of proton pump inhibition on acid, weakly acid and weakly alkaline gastro-esophageal reflux in children. World J. Pediatr. 2013, 9, 36–41. [Google Scholar] [CrossRef]
- Armstrong, D.; Marshall, J.K.; Chiba, N.; Enns, R.; Fallone, C.A.; Fass, R.; Hollingworth, R.; Hunt, R.H.; Kahrilas, P.J.; Mayrand, S. Canadian Consensus Conference on the management of gastroesophageal reflux disease in adults–update 2004. Can. J. Gastroenterol. 2005, 19, 15–35. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization Collaborating Centre for Drug Statistics Methodology. Available online: http://www.whocc.no/atc_ddd_index/?code1/4A02BC&showdescription1/4yes (accessed on 21 June 2022).
- Czinn, S.J.; Blanchard, S. Gastroesophageal reflux disease in neonates and infants. Paediatr. Drugs 2013, 15, 19–27. [Google Scholar] [CrossRef]
- Knebel, W.; Tammara, B.; Udata, C.; Comer, G.; Gastonguay, M.; Meng, X. Population pharmacokinetic modeling of pantoprazole in pediatric patients from birth to 16 years. J. Clin. Pharmacol. 2011, 51, 333–345. [Google Scholar] [CrossRef]
- Isshi, K.; Furuhashi, H.; Nakada, K. Therapeutic strategy for the patients with coexisting gastroesophageal reflux disease and postprandial distress syndrome of functional dyspepsia. JGH Open 2020, 4, 582–588. [Google Scholar] [CrossRef]
- Manzotti, M.E.; Catalano, H.N.; Serrano, F.A.; Di Stilio, G.; Koch, M.F.; Guyatt, G. Prokinetic drug utility in the treatment of gastroesophageal reflux esophagitis: A systematic review of randomized controlled trials. Open Med. 2007, 1, e171–e180. [Google Scholar] [PubMed]
- Usai-Satta, P.; Bellini, M.; Morelli, O.; Geri, F.; Lai, M.; Bassotti, G. Gastroparesis: New insights into an old disease. World J. Gastroenterol. 2020, 26, 2333. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.; Chorath, K.; Balar, E.; Xu, K.; Naik, A.; Moreira, A.; Rajasekaran, K. Clinical Practice Guidelines on Pediatric Gastroesophageal Reflux Disease: A Systematic Quality Appraisal of International Guidelines. Pediatr. Gastroenterol. Hepatol. Nutr. 2022, 25, 109. [Google Scholar] [CrossRef] [PubMed]
- Tighe, M.P.; Afzal, N.A.; Bevan, A.; Beattie, R.M. Current pharmacological management of gastro-esophageal reflux in children. Paediatr. Drugs 2009, 11, 185–202. [Google Scholar] [CrossRef]
- Katz, P.O.; Dunbar, K.B.; Schnoll-Sussman, F.H.; Greer, K.B.; Yadlapati, R.; Spechler, S.J. ACG clinical guideline for the diagnosis and management of gastroesophageal reflux disease. Am. J. Gastroenterol. 2022, 117, 27–56. [Google Scholar] [CrossRef]
- Jung, H.K. Epidemiology of gastroesophageal reflux disease in asia: A systematic review. J. Neurogastroenterol. Motil. 2011, 17, 14–27. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| No | Study ID [References] | Country | Type of Participants | Disease Condition | Follow-Up Duration | Treatment Strategies | Domperidone + PPI | PPI Alone | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of Participants (% Female) | Age of the Participants (Mean ± SD/Range) Years | Number of Participants (% Female) | Age of the Participants (Mean ± SD/Range) Years | |||||||
| 1 | Bediwy 2014 [31] | Bahrain | Children | Asthma with GERD | 12 weeks | Domperidone 0.5 mg/kg + Esomeprazole 2 mg/kg for 12 weeks | 40 (20) (50%) | 8.1 ± 1.3 | 40 (45%) | 7.7 ± 1.2 |
| 2 | Huiying 2020 [26] | China | Adult | Asthma with GERD | 1 month | Domperidone 10 mg + Omeprazole 2 × 20 mg for 1 month | 75 (37) (49%) | 55.4 ± 4.5 | 75 (47%) | 55.1 ± 4.2 |
| 3 | Jianzhong 2019 [24] | China | Children | GERD | 2 months | Domperidone 10 mg + Omeprazole 20 mg for 1 month | 40 (16) (40%) | 2.5 ± 0.2 | 40 (35%) | 2.4 ± 0.1 |
| 4 | Junsuan 2018 [23] | China | Children | GERD | 8 weeks | Domperidone 3 × (0.3 mg/kg) + IV Omeprazole (0.5–1 mg/kg) for 8 weeks | 30 (12) (40%) | 7.2 ± 1.4 | 30 (50%) | 7.6 ± 1.5 |
| 5 | Marakhouski 2017 [29] | Belarus | Adult | GERD | 12 weeks | Domperidone 30 mg + Omeprazole 20 mg for 8 weeks | 30 (19) (63%) | 47.1 ± 10.8 | 30 (46%) | 45.7 ± 13.0 |
| 6 | Ndraha 2011 [28] | Indonesia | Adult | GERD | 2 weeks | Domperidone 3 × 10 mg + omeprazole 2 × 20 mg for 2 weeks | 30 (16) (53%) | 44.3 ± 12.2 | 30 (80%) | 40.4 ± 13.9 |
| 7 | Puranik 2018 [30] | India | Adult | GERD | 2 weeks | Domperidone 30 mg + Pantoprazole 40 mg for 2 weeks | 40 (12) (30%) | 19.0–78.0 | 40 (30%) | 19.0–78.0 |
| 8 | Shaoxing 2017 [22] | China | Adult | GERD | 4 weeks | Domperidone 3 × 10 mg + Omeprazole 20 mg for 4 weeks | 34 (14) (41%) | 22.4 ± 1.4 | 34 (35%) | 22.1 ± 1.2 |
| 9 | Taghvei 2019 [32] | Iran | Adult | GERD | 1 month | Domperidone 3 × 10 mg + Pantoprazole 2 × 40 mg for 1 month | 13 (6) (46.2%) | 35.9 ± 9.9 | 16 (68%) | 37.3 ± 9.2 |
| 10 | Wang 2017 [27] | China | Adult | Superficial gastritis | 3 weeks | Domperidone 3 × 10 mg + Omeprazole 2 × 20 mg for 3 weeks | 48(27) (56.25%) | 42.7 ± 2.6 | 48 (37%) | 42.8 ± 2.7 |
| 11 | Yajie 2018 [25] | China | Children | GERD | 2 months | Domperidone 3 × 10 mg + Omeprazole for 2 months | 39 (18) (46%) | 7.1 ± 2.2 | 39 (41%) | 6.9 ± 2.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zamani, N.F.; Sjahid, A.S.; Tuan Kamauzaman, T.H.; Lee, Y.Y.; Islam, M.A. Efficacy and Safety of Domperidone in Combination with Proton Pump Inhibitors in Gastroesophageal Reflux Disease: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. J. Clin. Med. 2022, 11, 5268. https://doi.org/10.3390/jcm11185268
Zamani NF, Sjahid AS, Tuan Kamauzaman TH, Lee YY, Islam MA. Efficacy and Safety of Domperidone in Combination with Proton Pump Inhibitors in Gastroesophageal Reflux Disease: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Journal of Clinical Medicine. 2022; 11(18):5268. https://doi.org/10.3390/jcm11185268
Chicago/Turabian StyleZamani, Nur Fathurah, Afifah Sjamun Sjahid, Tuan Hairulnizam Tuan Kamauzaman, Yeong Yeh Lee, and Md Asiful Islam. 2022. "Efficacy and Safety of Domperidone in Combination with Proton Pump Inhibitors in Gastroesophageal Reflux Disease: A Systematic Review and Meta-Analysis of Randomised Controlled Trials" Journal of Clinical Medicine 11, no. 18: 5268. https://doi.org/10.3390/jcm11185268
APA StyleZamani, N. F., Sjahid, A. S., Tuan Kamauzaman, T. H., Lee, Y. Y., & Islam, M. A. (2022). Efficacy and Safety of Domperidone in Combination with Proton Pump Inhibitors in Gastroesophageal Reflux Disease: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Journal of Clinical Medicine, 11(18), 5268. https://doi.org/10.3390/jcm11185268