
Fluid Overload Phenotypes in Critical Illness—A Machine Learning Approach

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
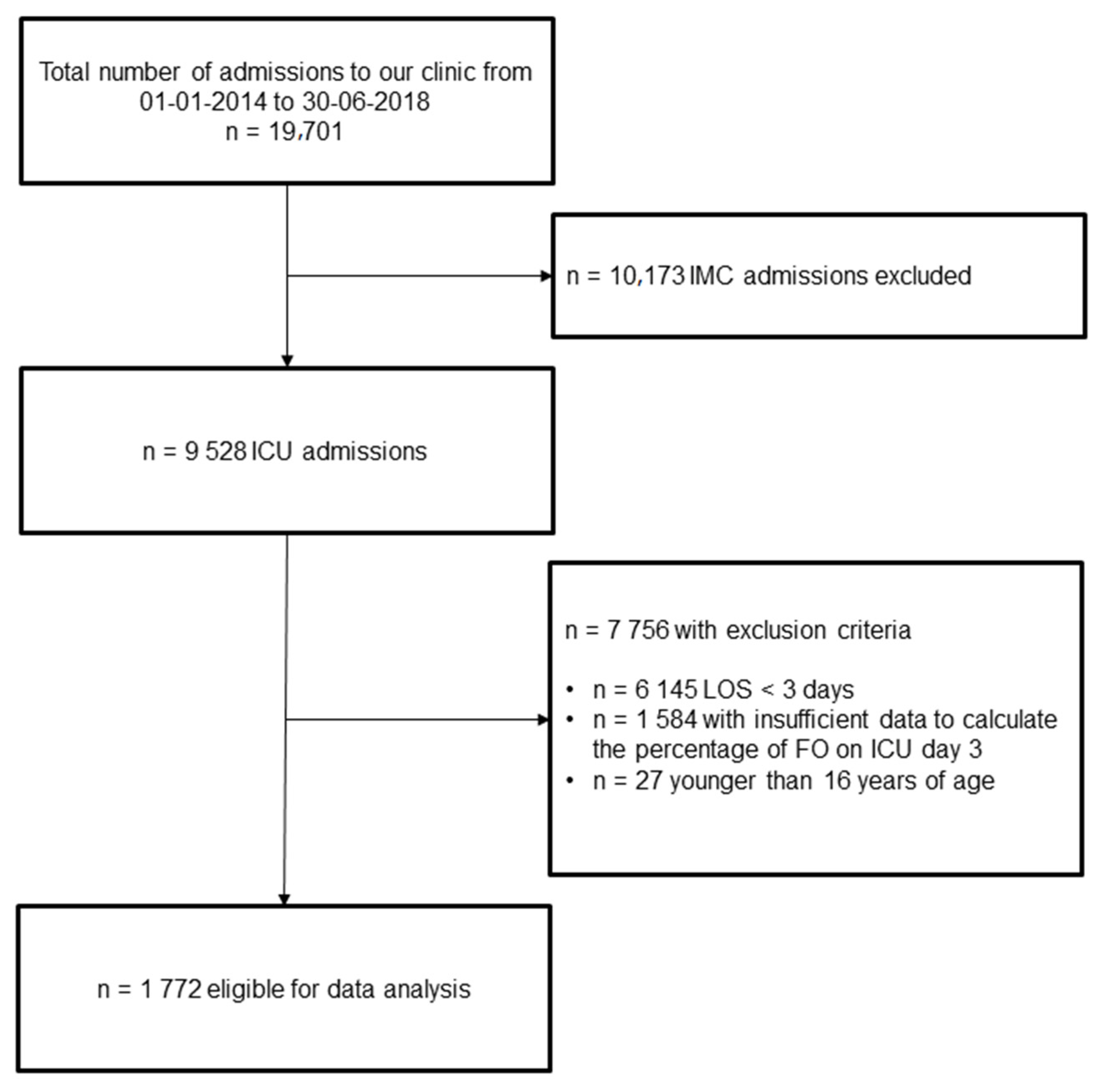
2.1. Setting & Study Design
2.2. Data Collection & Extraction
2.3. Statistical Analysis
2.4. Definitions
2.4.1. Fluid Overload
2.4.2. Cumulative Fluid Intake and Losses
3. Results
3.1. Univariable and Multivariable Analysis
3.2. Fast and Frugal Tree
3.3. Classification Decision Tree
3.4. Random Forest and Boruta Importance
3.5. Comparison of Statistical Models
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vincent, J.L. Fluid management in the critically ill. Kidney Int. 2019, 96, 52–57. [Google Scholar] [CrossRef]
- Finfer, S.; Myburgh, J.; Bellomo, R. Intravenous fluid therapy in critically ill adults. Nat. Rev. Nephrol. 2018, 14, 541–557. [Google Scholar] [CrossRef]
- Lankadeva, Y.R.; Kosaka, J.; Iguchi, N.; Evans, R.; Booth, L.C.; Bellomo, R.; May, C.N. Effects of Fluid Bolus Therapy on Renal Perfusion, Oxygenation, and Function in Early Experimental Septic Kidney Injury. Crit. Care Med. 2019, 47, e36–e43. [Google Scholar] [CrossRef] [PubMed]
- Nunes, T.S.O.; Ladeira, R.T.; Bafi, A.T.; de Azevedo, L.C.P.; Machado, F.R.; Freitas, F.G.R. Duration of hemodynamic effects of crystalloids in patients with circulatory shock after initial resuscitation. Ann. Intensive Care 2014, 4, 25. [Google Scholar] [CrossRef]
- Aya, H.D.; Ster, I.C.; Fletcher, N.; Grounds, R.M.; Rhodes, A.; Cecconi, M. Pharmacodynamic Analysis of a Fluid Challenge. Crit. Care Med. 2016, 44, 880–891. [Google Scholar] [CrossRef] [PubMed]
- Silversides, J.A.; Perner, A.; Malbrain, M.L.N.G. Liberal versus restrictive fluid therapy in critically ill patients. Intensive Care Med. 2019, 45, 1440–1442. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, M.E.; Prowle, J.R. Fluid Overload. Crit. Care Clin. 2015, 31, 803–821. [Google Scholar] [CrossRef]
- Acheampong, A.; Vincent, J.L. A positive fluid balance is an independent prognostic factor in patients with sepsis. Crit. Care 2015, 19, 251. [Google Scholar] [CrossRef] [PubMed]
- Cronhjort, M.; Hjortrup, P.B.; Holst, L.B.; Joelsson-Alm, E.; Martensson, J.; Svensen, C.; Perner, A. Association between fluid balance and mortality in patients with septic shock: A post hoc analysis of the TRISS trial. Acta Anaesthesiol. Scand. 2016, 60, 925–933. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, F.S.; Freitas, F.G.; Ferreira, E.M.; de Castro, I.; Bafi, A.T.; de Azevedo, L.C.; Machado, F.R. Positive fluid balance as a prognostic factor for mortality and acute kidney injury in severe sepsis and septic shock. J. Crit. Care 2015, 30, 97–101. [Google Scholar] [CrossRef]
- Neyra, J.A.; Li, X.; Canepa-Escaro, F.; Adams-Huet, B.; Toto, R.D.; Yee, J.; Hedayati, S.S.; Acute Kidney Injury in Critical Illness Study Group. Cumulative Fluid Balance and Mortality in Septic Patients With or Without Acute Kidney Injury and Chronic Kidney Disease. Crit. Care Med. 2016, 44, 1891–1900. [Google Scholar] [CrossRef]
- Messmer, A.S.; Zingg, C.; Müller, M.; Gerber, J.L.; Schefold, J.C.; Pfortmueller, C.A. Fluid Overload and Mortality in Adult Critical Care Patients-A Systematic Review and Meta-Analysis of Observational Studies. Crit. Care Med. 2020, 48, 1862–1870. [Google Scholar] [CrossRef] [PubMed]
- Han, M.J.; Park, K.H.; Shin, J.-H.; Kim, S.H. Influence of Daily Fluid Balance prior to Continuous Renal Replacement Therapy on Outcomes in Critically Ill Patients. J. Korean Med. Sci. 2016, 31, 1337–1344. [Google Scholar] [CrossRef] [PubMed]
- Chao, W.-C.; Tseng, C.-H.; Chien, Y.-C.; Sheu, C.-C.; Tsai, M.-J.; Fang, W.-F.; Chen, Y.-M.; Kao, K.-C.; Hu, H.-C.; Perng, W.-C.; et al. Association of day 4 cumulative fluid balance with mortality in critically ill patients with influenza: A multicenter retrospective cohort study in Taiwan. PLoS ONE 2018, 13, e0190952. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, R.; Cass, A.; Cole, L.; Finfer, S.; Gallagher, M.; Lee, J.; Lo, S.; McArthur, C.; McGuiness, S.; Norton, R.; et al. An observational study fluid balance and patient outcomes in the Randomized Evaluation of Normal vs. Augmented Level of Replacement Therapy trial. Crit. Care Med. 2012, 40, 1753–1760. [Google Scholar] [PubMed]
- Corl, K.A.; Prodromou, M.; Merchant, R.C.; Gareen, I.; Marks, S.; Banerjee, D.; Amass, T.; Abbasi, A.; Delcompare, C.; Palmisciano, A.; et al. The Restrictive IV Fluid Trial in Severe Sepsis and Septic Shock (RIFTS): A Randomized Pilot Study. Crit. Care Med. 2019, 47, 951–959. [Google Scholar] [CrossRef]
- Bjerregaard, M.R.; Hjortrup, P.B.; Perner, A. Indications for fluid resuscitation in patients with septic shock: Post-hoc analyses of the CLASSIC trial. Acta Anaesthesiol. Scand. 2019, 63, 337–343. [Google Scholar] [CrossRef]
- Hjortrup, P.B.; Haase, N.; Bundgaard, H.; Thomsen, S.L.; Winding, R.; Pettiläa, V.; Aaen, A.; Lodahl, D.; Berthelsen, R.E.; Christensen, H.; et al. Restricting volumes of resuscitation fluid in adults with septic shock after initial management: The CLASSIC randomised, parallel-group, multicentre feasibility trial. Intensive Care. Med. 2016, 42, 1695–1705. [Google Scholar] [CrossRef]
- Meyhoff, T.S.; Hjortrup, P.B.; Møller, M.H.; Wetterslev, J.; Lange, T.; Kjær, M.N.; Jonsson, A.B.; Hjortsø, C.J.S.; Cronhjort, M.; Laake, J.H.; et al. Conservative vs liberal fluid therapy in septic shock (CLASSIC) trial-Protocol and statistical analysis plan. Acta Anaesthesiol. Scand. 2019, 63, 1262–1271. [Google Scholar] [CrossRef]
- Famous, K.R.; Delucchi, K.; Ware, L.B.; Kangelaris, K.N.; Liu, K.; Thompson, B.T.; Calfee, C.S. Acute Respiratory Distress Syndrome Subphenotypes Respond Differently to Randomized Fluid Management Strategy. Am. J. Respir. Crit. Care Med. 2017, 195, 331–338. [Google Scholar] [CrossRef]
- Seymour, C.W.; Kennedy, J.N.; Wang, S.; Chang, C.-C.H.; Elliott, C.; Xu, Z.; Berry, S.; Clermont, G.; Cooper, G.; Gomez, H.; et al. Derivation, Validation, and Potential Treatment Implications of Novel Clinical Phenotypes for Sepsis. JAMA 2019, 321, 2003–2017. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, E.; Zafrani, L.; Mirouse, A.; Lengliné, E.; Darmon, M.; Chevret, S. Clinical phenotypes of critically ill COVID-19 patients. Intensive Care Med. 2020, 46, 1651–1652. [Google Scholar] [CrossRef] [PubMed]
- Daulasim, A.; Vieillard-Baron, A.; Geri, G. Hemodynamic clinical phenotyping in septic shock. Curr. Opin. Crit. Care 2021, 27, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Liaw, A.; Wiener, M. Classification and Regression by randomForest. R News 2002, 2, 18–22. [Google Scholar]
- Phillips, N.D.; Neth, H.; Woike, J.K.; Gaissmaier, W. FFTrees: A toolbox to create, visualize, and evaluate fast-and-frugal decision trees. Judgm. Decis. Mak. 2017, 12, 344–368. [Google Scholar]
- Breiman, L.; Friedman, J.; Stone, C.J.; Olshen, R.A. Classification and Regression Trees, 1st ed.; Routledge: Abingdon-on-Thames, UK, 1984. [Google Scholar]
- Delong, E.R.; Delong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Senaviratna, N.A.M.R.; Cooray, T.M.J.A. Diagnosing Multicollinearity of Logistic Regression Model. Asian J. Probab. Stat. 2019, 5, 1–9. [Google Scholar] [CrossRef]
- Kursa, M.; Rudnicki, W. Feature Selection with the Boruta Package. J. Stat. Softw. 2010, 36, 1–13. [Google Scholar] [CrossRef]
- Druml, W. Infusion Therapy: “To Do As Much Nothing As Possible”? Crit. Care Med. 2020, 48, 1915–1917. [Google Scholar] [CrossRef] [PubMed]
- Hecking, M.; Karaboyas, A.; Antlanger, M.; Saran, R.; Wizemann, V.; Chazot, C.; Rayner, H.; Hörl, W.H.; Pisoni, R.L.; Robinson, B.M.; et al. Significance of Interdialytic Weight Gain versus Chronic Volume Overload: Consensus Opinion. Am. J. Nephrol. 2013, 38, 78–90. [Google Scholar] [CrossRef]
- Ohashi, Y.; Sakai, K.; Hase, H.; Joki, N. Dry weight targeting: The art and science of conventional hemodialysis. Semin. Dial. 2018, 31, 551–556. [Google Scholar] [CrossRef]
- Claure-Del Granado, R.; Mehta, R.L. Fluid overload in the ICU: Evaluation and management. BMC Nephrol. 2016, 17, 109. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; Brophy, P.D.; Cruz, D.; Ronco, C. Fluid balance as a biomarker: Impact of fluid overload on outcome in critically ill patients with acute kidney injury. Crit. Care 2008, 12, 169. [Google Scholar] [CrossRef]
- Bouchard, J.; Soroko, S.B.; Chertow, G.M.; Himmelfarb, J.; Ikizler, T.; Paganini, E.P.; Mehta, R.L. Fluid accumulation, survival and recovery of kidney function in critically ill patients with acute kidney injury. Kidney Int. 2009, 76, 422–427. [Google Scholar] [CrossRef]
- Woodward, C.W.; Lambert, J.; Ortiz-Soriano, V.; Li, Y.; Ruiz-Conejo, M.; Bissell, B.; Kelly, A.; Adams, P.; Yessayan, L.; Morris, P.E.; et al. Fluid Overload Associates With Major Adverse Kidney Events in Critically Ill Patients With Acute Kidney Injury Requiring Continuous Renal Replacement Therapy. Crit. Care Med. 2019, 47, e753–e760. [Google Scholar] [CrossRef]
- Oh, T.K.; Song, I.-A.; Do, S.-H.; Jheon, S.; Lim, C. Association of perioperative weight-based fluid balance with 30-day mortality and acute kidney injury among patients in the surgical intensive care unit. J. Anesth. 2019, 33, 354–363. [Google Scholar] [CrossRef]
- Bihari, S.; Holt, A.W.; Prakash, S.; Bersten, A.D. Addition of indapamide to frusemide increases natriuresis and creatinine clearance, but not diuresis, in fluid overloaded ICU patients. J. Crit. Care 2016, 33, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.Y.; Kim, J.H.; Lee, D.W.; Lee, S.B.; Rhee, H.; Seong, E.Y.; Kwak, I.S.; Song, S.H. Fluid overload and survival in critically ill patients with acute kidney injury receiving continuous renal replacement therapy. PLoS ONE 2017, 12, e0172137. [Google Scholar] [CrossRef] [PubMed]
- Schrier, R.W. AKI: Fluid overload and mortality. Nat. Rev. Nephrol. 2009, 5, 485. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sakr, Y.; Vincent, J.-L.; Reinhart, K.; Groeneveld, J.; Michalopoulos, A.; Sprung, C.L.; Artigas, A.; Ranieri, V.M. High Tidal Volume and Positive Fluid Balance Are Associated With Worse Outcome in Acute Lung Injury. Chest 2005, 128, 3098–3108. [Google Scholar] [CrossRef]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The Surviving Sepsis Campaign Bundle: 2018 Update. Crit. Care Med. 2018, 46, 997–1000. [Google Scholar] [CrossRef]
- Cecconi, M.; De Backer, D.; Antonelli, M.; Beale, R.; Bakker, J.; Hofer, C.K.; Jaeschke, R.; Mebazaa, A.; Pinsky, M.R.; Teboul, J.-L.; et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014, 40, 1795–1815. [Google Scholar] [CrossRef] [PubMed]
- Jansen, T.C.; van Bommel, J.; Schoonderbeek, F.J.; Sleeswijk Visser, S.J.; van der Klooster, J.M.; Lima, A.P.; Willemsen, S.P.; Bakker, J.; LACTATE study group. Early lactate-guided therapy in intensive care unit patients: A multicenter, open-label, randomized controlled trial. Am. J. Respir. Crit. Care Med. 2010, 182, 752–761. [Google Scholar] [CrossRef] [PubMed]
- Ronco, J.J.; Fenwick, J.C.; Tweeddale, M.G.; Wiggs, B.R.; Phang, P.T.; Cooper, D.J.; Cunningham, K.F.; Russell, J.A.; Walley, K.R. Identification of the critical oxygen delivery for anaerobic metabolism in critically ill septic and nonseptic humans. JAMA 1993, 270, 1724–1730. [Google Scholar] [CrossRef] [PubMed]
- Friedman, G.; De Backer, D.; Shahla, M.; Vincent, J.-L. Oxygen supply dependency can characterize septic shock. Intensive Care Med. 1998, 24, 118–123. [Google Scholar] [CrossRef]
- Mikkelsen, M.E.; Miltiades, A.N.; Gaieski, D.F.; Goyal, M.; Fuchs, B.D.; Shah, C.V.; Bellamy, S.L.; Christie, J.D. Serum lactate is associated with mortality in severe sepsis independent of organ failure and shock. Crit. Care Med. 2009, 37, 1670–1677. [Google Scholar] [CrossRef]
- Howell, M.D.; Donnino, M.; Clardy, P.; Talmor, D.; Shapiro, N.I. Occult hypoperfusion and mortality in patients with suspected infection. Intensive Care Med. 2007, 33, 1892–1899. [Google Scholar] [CrossRef]
- Jansen, T.C.; Van Bommel, J.; Mulder, P.G.; Rommes, J.H.; Schieveld, S.J.; Bakker, J. The prognostic value of blood lactate levels relative to that of vital signs in the pre-hospital setting: A pilot study. Crit. Care 2008, 12, R160. [Google Scholar] [CrossRef]
- Jones, A.E. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: A randomized clinical trial. JAMA 2010, 303, 739–746. [Google Scholar] [CrossRef]
- Hernández, G.; Ospina-Tascón, G.A.; Damiani, L.P.; Estenssoro, E.; Dubin, A.; Hurtado, J.; Friedman, G.; Castro, R.; Alegría, L.; Teboul, J.; et al. Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients With Septic Shock: The ANDROMEDA-SHOCK Randomized Clinical Trial. JAMA 2019, 321, 654–664. [Google Scholar] [CrossRef]
- Zampieri, F.G.; Damiani, L.P.; Bakker, J.; Ospina-Tascón, G.A.; Castro, R.; Cavalcanti, A.B.; Hernandez, G. Effects of a Resuscitation Strategy Targeting Peripheral Perfusion Status versus Serum Lactate Levels among Patients with Septic Shock. A Bayesian Reanalysis of the ANDROMEDA-SHOCK Trial. Am. J. Respir. Crit. Care Med. 2020, 201, 423–429. [Google Scholar] [CrossRef]
- Messmer, A.S.; Pfortmueller, C.A. Protocolised Early De-Resuscitation in Septic Shock (REDUCE). Available online: https://clinicaltrials.gov/ct2/show/NCT04931485 (accessed on 6 July 2021).
- Kraut, J.A.; Madias, N.E. Metabolic acidosis: Pathophysiology, diagnosis and management. Nat. Rev. Nephrol. 2010, 6, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Mochizuki, K.; Fujii, T.; Paul, E.; Anstey, M.; Pilcher, D.V.; Bellomo, R. Early metabolic acidosis in critically ill patients: A binational multicentre study. Coll. Intensive Care Med. 2021, 23, 67–75. [Google Scholar] [CrossRef]
- Yagi, K.; Fujii, T. Management of acute metabolic acidosis in the ICU: Sodium bicarbonate and renal replacement therapy. Crit. Care 2021, 25, 314. [Google Scholar] [CrossRef] [PubMed]
- Jung, B.; Martinez, M.; Claessens, Y.E.; Darmon, M.; Klouche, K.; Lautrette, A.; Levraut, J.; Maury, E.; Oberlin, M.; Terzi, N.; et al. Diagnosis and management of metabolic acidosis: Guidelines from a French expert panel. Ann. Intensive Care 2019, 9, 92. [Google Scholar] [CrossRef]
- Cotton, B.A.; Guy, J.S.; Morris, J.A.; Abumrad, N.N. The cellular, metabolic, and systemic consequences of aggressive fluid resuscitation strategies. Shock 2006, 26, 115–121. [Google Scholar] [CrossRef]
- Kellum, J. Metabolic acidosis in patients with sepsis: Epiphenomenon or part of the pathophysiology? Coll. Intensive Care Med. 2004, 6, 197–203. [Google Scholar]
- Stephens, R.; Mythen, M. Resuscitation fluids and hyperchloraemic metabolic acidosis. Trauma 2003, 5, 141–147. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The Surviving Sepsis Campaign Bundle: 2018 update. Intensive Care Med. 2018, 44, 925–928. [Google Scholar] [CrossRef]
- Marik, P.; Bellomo, R. A rational approach to fluid therapy in sepsis. Br. J. Anaesth. 2016, 116, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Cavallazzi, R. Does the central venous pressure predict fluid responsiveness? An updated meta-analysis and a plea for some common sense. Crit. Care Med. 2013, 41, 1774–1781. [Google Scholar] [CrossRef] [PubMed]
- Cannesson, M.; Le Manach, Y.; Hofer, C.K.; Goarin, J.P.; Lehot, J.J.; Vallet, B.; Tavernier, B. Assessing the diagnostic accuracy of pulse pressure variations for the prediction of fluid responsiveness: A “gray zone” approach. Anesthesiology 2011, 115, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Biais, M.; Ehrmann, S.; Mari, A.; Conte, B.; Mahjoub, Y.; Desebbe, O.; Pottecher, J.; Lakhal, K.; Benzekri-Lefevre, D.; Molinari, N.; et al. Clinical relevance of pulse pressure variations for predicting fluid responsiveness in mechanically ventilated intensive care unit patients: The grey zone approach. Crit. Care 2014, 18, 587. [Google Scholar] [CrossRef] [PubMed]
- Hippensteel, J.A.; Uchimido, R.; Tyler, P.D.; Burke, R.C.; Han, X.; Zhang, F.; McMurtry, S.A.; Colbert, J.F.; Lindsell, C.J.; Angus, D.C.; et al. Intravenous fluid resuscitation is associated with septic endothelial glycocalyx degradation. Crit. Care 2019, 23, 259. [Google Scholar] [CrossRef]
- Maitland, K.; Kiguli, S.; Opoka, R.O.; Engoru, C.; Olupot-Olupot, P.; Akech, S.O.; Nyeko, R.; Mtove, G.; Reyburn, H.; Lang, T.; et al. Mortality after fluid bolus in African children with severe infection. N. Engl. J. Med. 2011, 364, 2483–2495. [Google Scholar] [CrossRef]
- Andrews, B.; Semler, M.W.; Muchemwa, L.; Kelly, P.; Lakhi, S.; Heimburger, D.C.; Mabula, C.; Bwalya, M.; Bernard, G.R. Effect of an Early Resuscitation Protocol on In-hospital Mortality Among Adults With Sepsis and Hypotension: A Randomized Clinical Trial. JAMA 2017, 318, 1233–1240. [Google Scholar] [CrossRef]
- Bernardi, M.H.; Schmidlin, D.; Ristl, R.; Heitzinger, C.; Schiferer, A.; Neugebauer, T.; Wrba, T.; Hiesmayr, M.; Druml, W.; Lassnigg, A. Serum Creatinine Back-Estimation in Cardiac Surgery Patients: Misclassification of AKI Using Existing Formulae and a Data-Driven Model. Clin. J. Am. Soc. Nephrol. 2016, 11, 395–404. [Google Scholar] [CrossRef]
- Kork, F.; Balzer, F.; Krannich, A.; Bernardi, M.H.; Eltzschig, H.K.; Jankowski, J.; Spies, C. Back-calculating baseline creatinine overestimates prevalence of acute kidney injury with poor sensitivity. Acta Physiol. 2017, 219, 613–624. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Harrison, A.M. The comparison of the commonly used surrogates for baseline renal function in acute kidney injury diagnosis and staging. BMC Nephrol. 2016, 17, 6. [Google Scholar] [CrossRef] [PubMed]
- Handelman, G.S.; Kok, H.K.; Chandra, R.V.; Razavi, A.H.; Lee, M.J.; Asadi, H. eDoctor: Machine learning and the future of medicine. J. Intern. Med. 2018, 284, 603–619. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, M.; Reynolds, E.; Andersson, H.B.; Nallamothu, B.K. Tree-Based Analysis. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e004879. [Google Scholar] [CrossRef] [PubMed]
- Kotsiantis, S.B. Decision trees: A recent overview. Artif. Intell. Rev. 2013, 39, 261–283. [Google Scholar] [CrossRef]
- Martignon, L.; Vitouch, O.; Takezawa, M.; Forster, M.R. Naive and Yet Enlightened: From Natural Frequencies to Fast and Frugal Decision Trees. In Thinking: Psychological Perspectives on Reasoning, Judgment and Decision Making; Hardman, D., Macchi, L., Eds.; Wiley & Sons: New York, NY, USA, 2003; pp. 189–211. [Google Scholar]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Couronné, R.; Probst, P.; Boulesteix, A.L. Random forest versus logistic regression: A large-scale benchmark experiment. BMC Bioinform. 2018, 19, 270. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Univariable Model | Multivariable Model | |||||
|---|---|---|---|---|---|---|
| Variable | Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value |
| Demographics | ||||||
| Age | 1.01 | (1.00–1.01) | 0.081 | |||
| Sex (male) | 0.74 | (0.58–0.93) | 0.012 | 0.71 | (0.50–0.99) | 0.046 |
| APACHE IV | 1.03 | (1.02–1.04) | <0.001 | 1.00 | (0.99–1.02) | 0.637 |
| Admission type (planned) | 3.11 | (2.35–4.11) | <0.001 | 1.70 | (1.07–2.70) | 0.024 |
| Past Medical History | ||||||
| Immune deficiency | 1.48 | (1.09–2.02) | 0.012 | 1.02 | (0.59–1.76) | 0.938 |
| Chronic kidney disease | 1.72 | (1.36–2.18) | <0.001 | 1.05 | (0.74–1.49) | 0.795 |
| Chronic liver disease | 1.84 | (1.36–2.47) | <0.001 | 1.55 | (0.98–2.44) | 0.061 |
| Cancer | 1.00 | (0.69–1.46) | 0.981 | |||
| Organ transplantation | 2.93 | (1.81–4.75) | <0.001 | 1.23 | (0.52–2.89) | 0.634 |
| Arterial hypertension | 1.09 | (0.87–1.37) | 0.465 | |||
| Diabetes mellitus (any type) | 1.06 | (0.64–1.75) | 0.814 | |||
| Malnutrition | 1.72 | (1.33–2.23) | <0.001 | 1.08 | (0.74–1.58) | 0.697 |
| Diagnosis at ICU admission | ||||||
| Sepsis/septic shock | 1.91 | (1.51–2.42) | <0.001 | 2.05 | (1.44–2.91) | 0.007 |
| Respiratory failure | 0.92 | (0.72–1.17) | 0.483 | |||
| Heart failure and cardiogenic shock | 1.70 | (1.34–2.16) | <0.001 | 0.96 | (0.67–1.37) | 0.827 |
| Pancreatitis | 1.06 | (0.48–2.36) | 0.883 | |||
| Major trauma | 0.62 | (0.44–0.88) | 0.008 | 1.02 | (0.61–1.71) | 0.927 |
| Non-traumatic neurological disease | 0.16 | (0.09–0.28) | <0.001 | 0.33 | (0.16–0.71) | 0.005 |
| Surgery prior admission | 4.20 | (3.30–5.35) | <0.001 | 2.35 | (1.52–3.62) | <0.001 |
| Infection (any type) at admission | 0.85 | (0.67–1.08) | 0.176 | |||
| Treatment at ICU admission | ||||||
| Mechanical ventilation | 2.31 | (1.84–2.91) | <0.001 | 1.56 | (1.10–2.20) | 0.012 |
| Vasoactives | 1.60 | (0.98–2.62) | 0.062 | |||
| Lab values at admission | ||||||
| Sodium (mmol/L) | 0.97 | (0.95–0.99) | 0.012 | 0.97 | (0.94–1.01) | 0.103 |
| Bicarbonate (mmol/L) | 0.85 | (0.83–0.88) | <0.001 | 0.89 | (0.85–0.93) | <0.001 |
| Lactate (mmol/L) | 1.50 | (1.42–1.60) | <0.001 | 1.28 | (1.18–1.39) | <0.001 |
| Creatinine (μmol/L) | 1.00 | (1.00–1.00) | <0.001 | 1.00 | (1.00–1.00) | 0.633 |
| Variable | Mean Imp | Median Imp | Min Imp | Max Imp | Norm Hits | Decision |
|---|---|---|---|---|---|---|
| Lactate (mmol/L) | 32.77 | 32.68 | 29.04 | 35.91 | 1 | Confirmed |
| Bicarbonate (mmol/L) | 19.92 | 20.04 | 16.59 | 23.41 | 1 | Confirmed |
| Surgery prior to admission | 12.3 | 12.21 | 9.24 | 15.16 | 1 | Confirmed |
| Sepsis/septic shock | 6.79 | 6.64 | 4.79 | 10.19 | 1 | Confirmed |
| Creatinine (μmol/L) | 6.28 | 6.24 | 3.51 | 8.32 | 1 | Confirmed |
| Non-traumatic neurological disease | 5.77 | 5.79 | 2.76 | 7.79 | 1 | Confirmed |
| Chronic liver disease | 5.05 | 5.19 | 2.27 | 8.23 | 0.93 | Confirmed |
| Admission type (planned) | 4.78 | 4.79 | 1.37 | 7.37 | 0.95 | Confirmed |
| Sodium (mmol/L) | 4.18 | 4.19 | 2.17 | 7.02 | 0.86 | Confirmed |
| APACHE IV | 3.97 | 3.95 | 1.16 | 7 | 0.87 | Confirmed |
| Chronic kidney failure | 3.46 | 3.35 | 0 | 6.2 | 0.76 | Confirmed |
| Hx of organ transplantation | 3.22 | 3.22 | 0.37 | 5.58 | 0.71 | Confirmed |
| Mechanical ventilation (at admission) | 3.14 | 3.23 | −0.68 | 5.15 | 0.7 | Confirmed |
| Hx of malnutrition | 2.9 | 2.96 | −0.2 | 5.41 | 0.68 | Confirmed |
| Heart failure/cardiogenic shock | 2.54 | 2.69 | −0.3 | 4.36 | 0.54 | Tentative |
| Sex (male) | 1.41 | 1.21 | −0.93 | 3.38 | 0.04 | Rejected |
| Hx of immune deficiency | −0.03 | −0.13 | −3.17 | 2.26 | 0.01 | Rejected |
| Major trauma | −0.13 | −0.49 | −1.46 | 1.54 | 0 | Rejected |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Messmer, A.S.; Moser, M.; Zuercher, P.; Schefold, J.C.; Müller, M.; Pfortmueller, C.A. Fluid Overload Phenotypes in Critical Illness—A Machine Learning Approach. J. Clin. Med. 2022, 11, 336. https://doi.org/10.3390/jcm11020336
Messmer AS, Moser M, Zuercher P, Schefold JC, Müller M, Pfortmueller CA. Fluid Overload Phenotypes in Critical Illness—A Machine Learning Approach. Journal of Clinical Medicine. 2022; 11(2):336. https://doi.org/10.3390/jcm11020336
Chicago/Turabian StyleMessmer, Anna S., Michel Moser, Patrick Zuercher, Joerg C. Schefold, Martin Müller, and Carmen A. Pfortmueller. 2022. "Fluid Overload Phenotypes in Critical Illness—A Machine Learning Approach" Journal of Clinical Medicine 11, no. 2: 336. https://doi.org/10.3390/jcm11020336
APA StyleMessmer, A. S., Moser, M., Zuercher, P., Schefold, J. C., Müller, M., & Pfortmueller, C. A. (2022). Fluid Overload Phenotypes in Critical Illness—A Machine Learning Approach. Journal of Clinical Medicine, 11(2), 336. https://doi.org/10.3390/jcm11020336