
Psychometric Validation of the German Translation of the Quality of Life Questionnaire-Bronchiectasis (QOL-B)—Data from the German Bronchiectasis Registry PROGNOSIS



 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
2.2. Patient Population and Study Design
2.3. Quality of Life Assessment
2.4. Statistical Analysis
3. Results
3.1. Floor and Ceiling Effects, Internal Consistency and Test-Retest Reliability
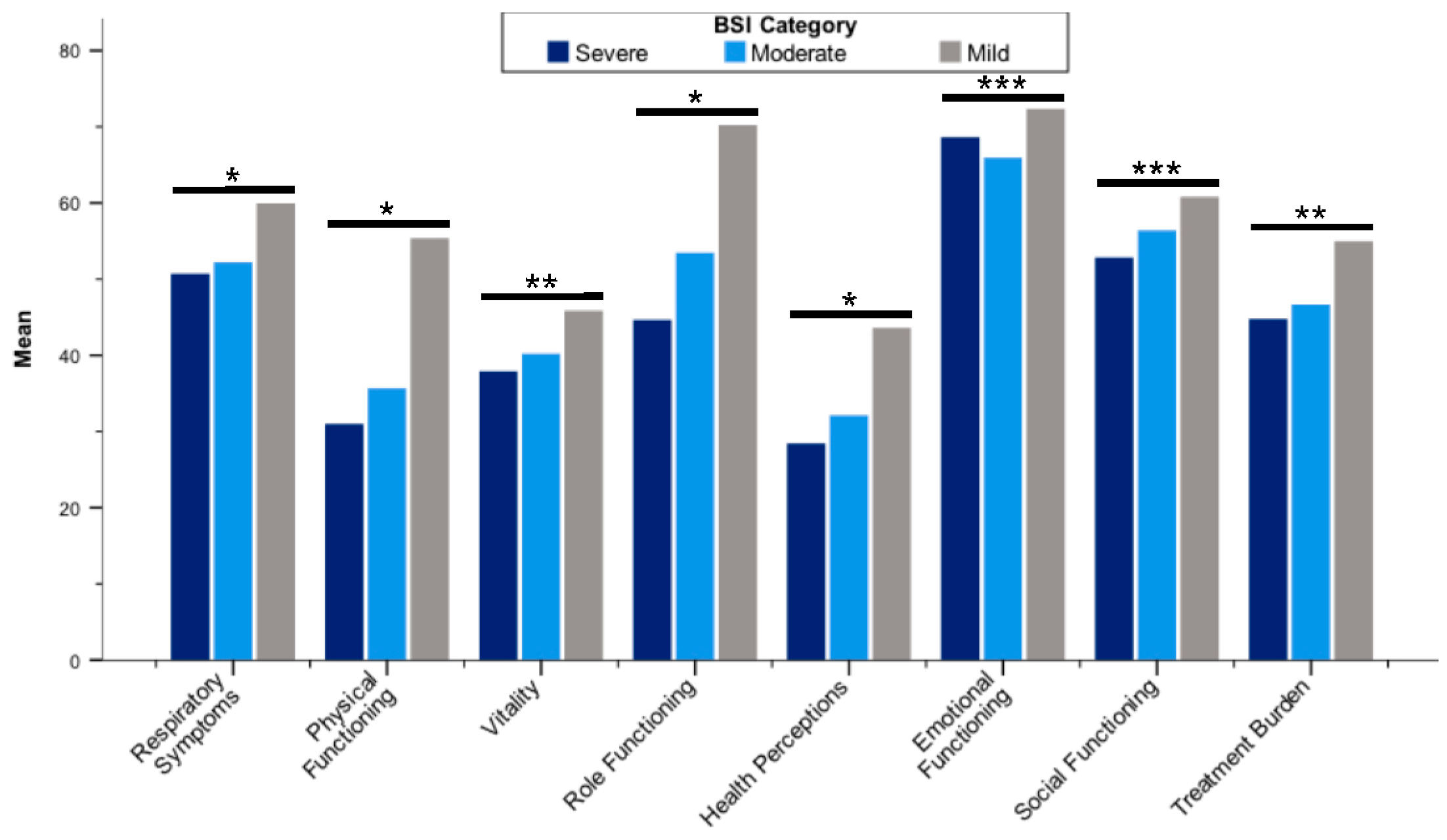
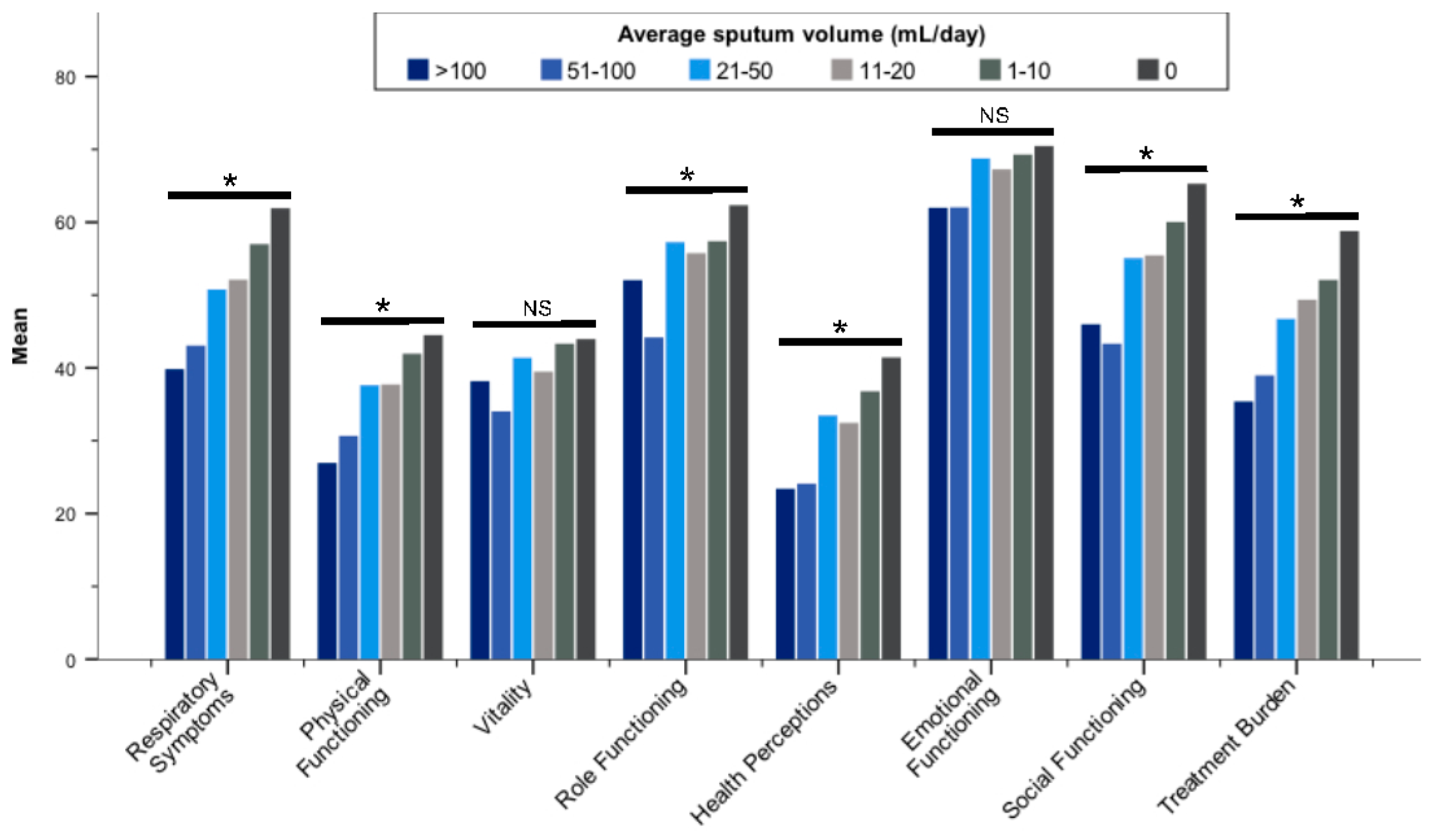
3.2. Discriminant and Convergent Validity of QOL-B Scores
3.3. Minimal Clinical Important Difference
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aliberti, S.; Goeminne, P.C.; O’Donnell, A.E.; Aksamit, T.R.; Al-Jahdali, H.; Barker, A.F.; Blasi, F.; Boersma, W.G.; Crichton, M.L.; De Soyza, A.; et al. Criteria and definitions for the radiological and clinical diagnosis of bronchiectasis in adults for use in clinical trials: International consensus recommendations. Lancet Respir. Med. 2021; Online ahead of print. [Google Scholar]
- Quint, J.K.; Millett, E.R.; Joshi, M.; Navaratnam, V.; Thomas, S.L.; Hurst, J.R.; Smeeth, L.; Brown, J.S. Changes in the incidence, prevalence and mortality of bronchiectasis in the UK from 2004 to 2013: A population-based cohort study. Eur. Respir. J. 2016, 47, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Ringshausen, F.C.; Rademacher, J.; Pink, I.; de Roux, A.; Hickstein, L.; Ploner, T.; Welte, T.; Diel, R. Increasing bronchiectasis prevalence in Germany, 2009–2017: A population-based cohort study. Eur. Respir. J. 2019, 54, 1900499. [Google Scholar] [CrossRef] [PubMed]
- Diel, R.; Chalmers, J.D.; Rabe, K.F.; Nienhaus, A.; Loddenkemper, R.; Ringshausen, F.C. Economic burden of bronchiectasis in germany. Eur. Respir. J. 2019, 53, 1802033. [Google Scholar] [CrossRef]
- Loebinger, M.R.; Polverino, E.; Chalmers, J.D.; Tiddens, H.; Goossens, H.; Tunney, M.; Ringshausen, F.C.; Hill, A.T.; Pathan, R.; Angyalosi, G.; et al. Efficacy and safety of TOBI podhaler in pseudomonas aeruginosa-infected bronchiectasis patients: iBEST study. Eur. Respir. J. 2021, 57, 2001451. [Google Scholar] [CrossRef]
- Haworth, C.S.; Bilton, D.; Chalmers, J.D.; Davis, A.M.; Froehlich, J.; Gonda, I.; Thompson, B.; Wanner, A.; O’Donnell, A.E. Inhaled liposomal ciprofloxacin in patients with non-cystic fibrosis bronchiectasis and chronic lung infection with pseudomonas aeruginosa (ORBIT-3 and ORBIT-4): Two phase 3, randomised controlled trials. Lancet Respir. Med. 2019, 7, 213–226. [Google Scholar] [CrossRef] [Green Version]
- Barker, A.F.; O’Donnell, A.E.; Flume, P.; Thompson, P.J.; Ruzi, J.D.; de Gracia, J.; Boersma, W.G.; De Soyza, A.; Shao, L.; Zhang, J.; et al. Aztreonam for inhalation solution in patients with non-cystic fibrosis bronchiectasis (AIR-BX1 and AIR-BX2): Two randomised double-blind, placebo-controlled phase 3 trials. Lancet Respir. Med. 2014, 2, 738–749. [Google Scholar] [CrossRef]
- Bilton, D.; Daviskas, E.; Anderson, S.D.; Kolbe, J.; King, G.; Stirling, R.G.; Thompson, B.R.; Milne, D.; Charlton, B. Phase 3 randomized study of the efficacy and safety of inhaled dry powder mannitol for the symptomatic treatment of non-cystic fibrosis bronchiectasis. Chest 2013, 144, 215–225. [Google Scholar] [CrossRef]
- Aliberti, S.; Masefield, S.; Polverino, E.; De Soyza, A.; Loebinger, M.R.; Menendez, R.; Ringshausen, F.C.; Vendrell, M.; Powell, P.; Chalmers, J.D.; et al. Research priorities in bronchiectasis: A consensus statement from the EMBARC clinical research collaboration. Eur. Respir. J. 2016, 48, 632–647. [Google Scholar] [CrossRef] [Green Version]
- U.S. Food & Drug Administration (FDA). Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims. 2009. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/patient-reported-outcome-measures-use-medical-product-development-support-labeling-claims (accessed on 20 November 2021).
- Flume, P.A.; Griffith, D.E.; Chalmers, J.D.; Daley, C.L.; Olivier, K.; O’Donnell, A.; Aksamit, T.; Kasperbauer, S.; Leitman, A.; Winthrop, K.L. Development of drugs for nontuberculous mycobacterial disease: Clinicians’ interpretation of a US Food and Drug Administration workshop. Chest 2021, 159, 537–543. [Google Scholar] [CrossRef]
- Quittner, A.L.; O’Donnell, A.E.; Salathe, M.A.; Lewis, S.A.; Li, X.; Montgomery, A.B.; O’Riordan, T.G.; Barker, A.F. Quality of life questionnaire-bronchiectasis: Final psychometric analyses and determination of minimal important difference scores. Thorax 2015, 70, 12–20. [Google Scholar] [CrossRef] [Green Version]
- Spinou, A.; Fragkos, K.C.; Lee, K.K.; Elston, C.; Siegert, R.J.; Loebinger, M.R.; Wilson, R.; Garrod, R.; Birring, S.S. The validity of health-related quality of life questionnaires in bronchiectasis: A systematic review and meta-analysis. Thorax 2016, 71, 683–694. [Google Scholar] [CrossRef] [Green Version]
- Spinou, A.; Siegert, R.J.; Guan, W.J.; Patel, A.S.; Gosker, H.R.; Lee, K.K.; Elston, C.; Loebinger, M.R.; Wilson, R.; Garrod, R.; et al. The development and validation of the Bronchiectasis Health Questionnaire. Eur. Respir. J. 2017, 49, 1601532. [Google Scholar] [CrossRef] [Green Version]
- Crichton, M.L.; Dudgeon, E.K.; Shoemark, A.; Chalmers, J.D. Validation of the Bronchiectasis Impact Measure (BIM): A novel patient-reported outcome measure. Eur. Respir. J. 2021, 57, 2003156. [Google Scholar] [CrossRef]
- McLeese, R.H.; Spinou, A.; Alfahl, Z.; Tsagris, M.; Elborn, J.S.; Chalmers, J.D.; De Soyza, A.; Loebinger, M.R.; Birring, S.S.; Fragkos, K.C.; et al. Psychometrics of health-related quality of life questionnaires in bronchiectasis: A systematic review and meta-analysis. Eur. Respir. J. 2021, 58, 2100025. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Goeminne, P.; Aliberti, S.; McDonnell, M.J.; Lonni, S.; Davidson, J.; Poppelwell, L.; Salih, W.; Pesci, A.; Dupont, L.J.; et al. The Bronchiectasis Severity Index. An international derivation and validation study. Am. J. Respir. Crit. Care Med. 2014, 189, 576–585. [Google Scholar] [CrossRef]
- Olveira, C.; Olveira, G.; Espildora, F.; Giron, R.M.; Munoz, G.; Quittner, A.L.; Martinez-Garcia, M.A. Validation of a quality of life questionnaire for bronchiectasis: Psychometric analyses of the Spanish QOL-B-V3.0. Qual. Life Res. 2014, 23, 1279–1292. [Google Scholar] [CrossRef] [PubMed]
- Rademacher, J.; de Roux, A.; Ringshausen, F.C. [PROGNOSIS—The prospective German non-cf bronchiectasis patient registry]. Pneumologie 2015, 69, 391–393. [Google Scholar] [PubMed] [Green Version]
- Reiff, D.B.; Wells, A.U.; Carr, D.H.; Cole, P.J.; Hansell, D.M. CT findings in bronchiectasis: Limited value in distinguishing between idiopathic and specific types. AJR Am. J. Roentgenol. 1995, 165, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Quittner, A.L.; Marciel, K.K.; Salathe, M.A.; O’Donnell, A.E.; Gotfried, M.H.; Ilowite, J.S.; Metersky, M.L.; Flume, P.A.; Lewis, S.A.; McKevitt, M.; et al. A preliminary quality of life questionnaire-bronchiectasis: A patient-reported outcome measure for bronchiectasis. Chest 2014, 146, 437–448. [Google Scholar] [CrossRef]
- Field, A. Correlation. In Discovering Statistics Using SPSS, 3rd ed.; SAGE Publications Ltd.: London, UK, 2009; pp. 166–196. [Google Scholar]
- Altenburg, J.; Wortel, K.; de Graaff, C.S.; van der Werf, T.S.; Boersma, W.G. Validation of a visual analogue score (LRTI-VAS) in non-CF bronchiectasis. Clin. Respir. J. 2016, 10, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Finch, S.; Laska, I.F.; Abo-Leyah, H.; Fardon, T.C.; Chalmers, J.D. Validation of the COPD Assessment Test (CAT) as an outcome measure in bronchiectasis. Chest 2020, 157, 815–823. [Google Scholar] [CrossRef]
- Murray, M.P.; Turnbull, K.; MacQuarrie, S.; Pentland, J.L.; Hill, A.T. Validation of the Leicester Cough Questionnaire in non-cystic fibrosis bronchiectasis. Eur. Respir. J. 2009, 34, 125–131. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Cipolla, D.; Thompson, B.; Davis, A.M.; O’Donnell, A.; Tino, G.; Gonda, I.; Haworth, C.; Froehlich, J. Changes in respiratory symptoms during 48-week treatment with ARD-3150 (inhaled liposomal ciprofloxacin) in bronchiectasis: Results from the ORBIT-3 and -4 studies. Eur. Respir. J. 2020, 56, 2000110. [Google Scholar] [CrossRef] [PubMed]
- Crichton, M.L.; Lonergan, M.; Barker, A.F.; Sibila, O.; Goeminne, P.; Shoemark, A.; Chalmers, J.D. Inhaled aztreonam improves symptoms of cough and sputum production in patients with bronchiectasis: A post hoc analysis of the AIR-BX studies. Eur. Respir. J. 2020, 56, 2000608. [Google Scholar] [CrossRef] [PubMed]
- Aksamit, T.; De Soyza, A.; Bandel, T.J.; Criollo, M.; Elborn, J.S.; Operschall, E.; Polverino, E.; Roth, K.; Winthrop, K.L.; Wilson, R. RESPIRE 2: A phase III placebo-controlled randomised trial of ciprofloxacin dry powder for inhalation in non-cystic fibrosis bronchiectasis. Eur. Respir. J. 2018, 51, 1702053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Soyza, A.; Aksamit, T.; Bandel, T.J.; Criollo, M.; Elborn, J.S.; Operschall, E.; Polverino, E.; Roth, K.; Winthrop, K.L.; Wilson, R. RESPIRE 1: A phase III placebo-controlled randomised trial of ciprofloxacin dry powder for inhalation in non-cystic fibrosis bronchiectasis. Eur. Respir. J. 2018, 51, 1702052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serisier, D.J.; Bilton, D.; De Soyza, A.; Thompson, P.J.; Kolbe, J.; Greville, H.W.; Cipolla, D.; Bruinenberg, P.; Gonda, I. Inhaled, dual release liposomal ciprofloxacin in non-cystic fibrosis bronchiectasis (ORBIT-2): A randomised, double-blind, placebo-controlled trial. Thorax 2013, 68, 812–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serisier, D.J.; Martin, M.L.; McGuckin, M.A.; Lourie, R.; Chen, A.C.; Brain, B.; Biga, S.; Schlebusch, S.; Dash, P.; Bowler, S.D. Effect of long-term, low-dose erythromycin on pulmonary exacerbations among patients with non-cystic fibrosis bronchiectasis: The BLESS randomized controlled trial. JAMA 2013, 309, 1260–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revicki, D.; Hays, R.D.; Cella, D.; Sloan, J. Recommended methods for determining responsiveness and minimally important differences for patient-reported outcomes. J. Clin. Epidemiol. 2008, 61, 102–109. [Google Scholar] [CrossRef]
- Dhar, R.; Singh, S.; Talwar, D.; Mohan, M.; Tripathi, S.K.; Swarnakar, R.; Trivedi, S.; Rajagopala, S.; D’Souza, G.; Padmanabhan, A.; et al. Bronchiectasis in India: Results from the European Multicentre Bronchiectasis Audit and Research Collaboration (EMBARC) and Respiratory Research Network of India Registry. Lancet Glob. Health 2019, 7, e1269–e1279. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Age (years), mean (SD) | 59.5 (15.8) |
| Females, n (%) | 538 (59.5) |
| BMI (kg/m2), mean (SD) | 24.1 (4.5) |
| FEV1 %predicted, mean (SD) | 69.8 (26.8) |
| ≥80%predicted, n (%) | 344 (38.1) |
| 50–79%predicted, n (%) | 322 (35.6) |
| 30–49%predicted, n (%) | 180 (19.9) |
| <30%predicted, n (%) | 58 (6.4) |
| Radiological severity, n (%) | |
| <3 lobes affected | 325 (36.0) |
| ≥3 lobes affected and/or cystic bronchiectasis | 579 (64.0) |
| MRC dyspnea scale, n (%) | |
| 1–3 | 751 (83.1) |
| 4–5 | 153 (16.9) |
| Smoking, n (%) | |
| Active smoker | 57 (6.3) |
| Former smoker | 335 (37.1) |
| Never smoked | 512 (56.6) |
| Exacerbations in the past 12 months, median (IQR) | 1 (0–3) |
| 0, n (%) | 271 (30.0) |
| 1–2, n (%) | 361 (39.9) |
| ≥3, n (%) | 272 (30.1) |
| Prior hospital admission, n (%) 1 | 349 (38.6) |
| Hospitalizations in the past 12 months, median (IQR) 1 | 0 (0–1) |
| Regular pharmacological treatment of bronchiectasis, n (%) | 704 (77.9) |
| Regular sputum production, n (%) | 704 (77.9) |
| Average daily sputum volume, median (IQR) | 20 (10–50) |
| 0 mL/day, n (%) | 284 (31.4) |
| 1–10 mL/day, n (%) | 261 (28.9) |
| 11–20 mL/day, n (%) | 122 (13.5) |
| 21–50 mL/day, n (%) | 151 (16.7) |
| 51–100 mL/day, n (%) | 60 (6.6) |
| >100 mL/day, n (%) | 26 (2.9) |
| BSI category (n = 666), n (%) 2 | |
| Mild (0–4) | 150 (22.5) |
| Moderate (5–8) | 390 (58.6) |
| Severe (≥9) | 126 (18.9) |
| QOL-B Scale | n 1 | Mean (SD) QOL-B Scores | Floor Effects, n (%) | Ceiling Effects, n (%) | Cronbach’s α | ICC (95% CI) |
|---|---|---|---|---|---|---|
| Respiratory Symptoms | 892 | 56.2 (21.0) | 1 (0.1) | 9 (1.0) | 0.84 | 0.93 (0.82–0.97) |
| Physical Functioning | 889 | 41.8 (29.8) | 95 (10.7) | 42 (4. 7) | 0.92 | 0.96 (0.90–0.99) |
| Vitality | 892 | 42.0 (21.4) | 40 (4.5) | 10 (1.1) | 0.76 | 0.94 (0.84–0.97) |
| Role Functioning | 898 | 58.8 (27.4) | 23 (2.6) | 63 (7.0) | 0.86 | 0.88 (0.69–0.95) |
| Health Perceptions | 891 | 36.3 (22.6) | 42 (4.7) | 3 (0.3) | 0.79 | 0.84 (0.59–0.94) |
| Emotional Functioning | 889 | 69.2 (21.9) | 4 (0.4) | 97 (10.9) | 0.82 | 0.94 (0.85–0.98) |
| Social Functioning | 878 | 59.9 (26.9) | 31 (3.5) | 80 (9.1) | 0.73 | 0.87 (0.66–0.95) |
| Treatment Burden | 645 | 51.3 (25.1) | 18 (2.8) | 27 (4.2) | 0.73 | 0.90 (0.73–0.96) |
| Mean (SD) QOL-B Scores at Baseline According to Pulmonary Exacerbations | ||||
|---|---|---|---|---|
| QOL-B Scale | 0 | 1–2 | ≥3 | p-Value 1 |
| Respiratory Symptoms | 62.0 (20.7) | 56.8 (19.9) | 49.7 (20.7) | <0.001 |
| Physical Functioning | 47.6 (30.5) | 44.3 (30.1) | 33.3 (26.5) | <0.001 |
| Vitality | 46.3 (21.8) | 43.7 (20.9) | 36.3 (20.1) | <0.001 |
| Role Functioning | 67.7 (25.0) | 60.9 (26.1) | 47.7 (27.4) | <0.001 |
| Health Perceptions | 42.9 (24.0) | 37.9 (21.7) | 27.9 (19.5) | <0.001 |
| Emotional Functioning | 73.4 (20.3) | 71.1 (20.0) | 63.0 (23.7) | <0.001 |
| Social Functioning | 68.5 (23.4) | 60.2 (25.7) | 51.2 (28.8) | <0.001 |
| Treatment Burden | 59.2 (24.1) | 52.4 (24.7) | 42.7 (24.0) | <0.001 |
| Mean (SD) QOL-B Scores at Baseline According to Prior Hospitalization | |||
|---|---|---|---|
| QOL-B Scale | Yes | No | p-Value 1 |
| Respiratory Symptoms | 51.3 (21.3) | 59.2 (20.3) | <0.001 |
| Physical Functioning | 32.4 (27.3) | 47.7 (29.8) | <0.001 |
| Vitality | 39.0 (21.5) | 43.9 (21.1) | <0.001 |
| Role Functioning | 48.4 (27.0) | 65.4 (25.6) | <0.001 |
| Health Perceptions | 31.6 (21.1) | 39.4 (22.9) | <0.001 |
| Emotional Functioning | 66.5 (22.9) | 70.8 (21.1) | <0.001 |
| Social Functioning | 55.2 (27.8) | 62.8 (25.9) | <0.001 |
| Treatment Burden | 44.5 (24.2) | 55.9 (24.7) | <0.001 |
| Mean (SD) QOL-B Scores According to Pseudomonas aeruginosa Infection | |||
|---|---|---|---|
| QOL-B Scale | Yes | No | p-Value 1 |
| Respiratory Symptoms | 51.0 (20.1) | 59.0 (21.0) | <0.001 |
| Physical Functioning | 35.2 (28.2) | 45.5 (30.0) | <0.001 |
| Vitality | 40.5 (21.4) | 42.9 (21.3) | 0.080 |
| Role Functioning | 52.3 (27.4) | 62.4 (26.7) | <0.001 |
| Health Perceptions | 31.7 (20.3) | 38.8 (23.4) | <0.001 |
| Emotional Functioning | 67.2 (22.5) | 70.2 (21.5) | 0.063 |
| Social Functioning | 54.5 (26.1) | 62.8 (26.9) | <0.001 |
| Treatment Burden | 45.8 (23.6) | 55.0 (25.5) | <0.001 |
| Correlations of Baseline Scores on QOL-B Scales with Measures of Health Status | |||||
|---|---|---|---|---|---|
| QOL-B Scale | ppFEV1 | Pulmonary Exacerbation Rate | Hospitalization Rate | MRC Dyspnea Scale | Average Sputum Volume (mL/Day) |
| Respiratory Symptoms (n = 892) | r = 0.304 p < 0.001 | r = −0.241 p < 0.001 | r = −0.223 p < 0.001 | r = −0.414 p < 0.001 | r = −0.321 p < 0.001 |
| Physical Functioning (n = 889) | r = 0.470 p < 0.001 | r = −0.203 p < 0.001 | r = −0.282 p < 0.001 | r = −0.620 p < 0.001 | r = −0.139 p < 0.001 |
| Vitality (n = 892) | r = 0.152 p < 0.001 | r = −0.198 p < 0.001 | r = −0.139 p < 0.001 | r = −0.315 p < 0.001 | r = −0.088 p = 0.009 |
| Role Functioning (n = 898) | r = 0.334 p < 0.001 | r = −0.305 p < 0.001 | r = −0.339 p < 0.001 | r = −0.513 p < 0.001 | r = −0.163 p < 0.001 |
| Health Perceptions (n = 891) | r = 0.256 p < 0.001 | r = −0.263 p < 0.001 | r = −0.198 p < 0.001 | r = −0.417 p < 0.001 | r = −0.215 p < 0.001 |
| Emotional Functioning (n = 889) | r = 0.107 p = 0.003 | r = −0.176 p < 0.001 | r = −0.108 p = 0.001 | r = −0.239 p < 0.001 | r = −0.090 p = 0.008 |
| Social Functioning (n = 878) | r = 0.087 p = 0.011 | r = −0.240 p < 0.001 | r = −0.162 p < 0.001 | r = −0.225 p < 0.001 | r = −0.236 p < 0.001 |
| Treatment Burden (n = 645) | r = 0.229 p < 0.001 | r = −0.260 p < 0.001 | r = −0.236 p < 0.001 | r = −0.370 p < 0.001 | r = −0.239 p < 0.001 |
| r < 0.3 weak correlation | r = 0.3–0.49 moderate correlation | r > 0.5 strong correlation | |||
| QOL-B Scale | MCID |
|---|---|
| Respiratory Symptoms | 8.5 |
| Physical Functioning | 8.7 |
| Vitality | 10.5 |
| Role Functioning | 10.4 |
| Health Perceptions | 10.3 |
| Emotional Functioning | 9.3 |
| Social Functioning | 14.1 |
| Treatment Burden | 13.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quellhorst, L.; Barten-Neiner, G.; de Roux, A.; Diel, R.; Mertsch, P.; Pink, I.; Rademacher, J.; Sutharsan, S.; Welte, T.; Zurawski, A.; et al. Psychometric Validation of the German Translation of the Quality of Life Questionnaire-Bronchiectasis (QOL-B)—Data from the German Bronchiectasis Registry PROGNOSIS. J. Clin. Med. 2022, 11, 441. https://doi.org/10.3390/jcm11020441
Quellhorst L, Barten-Neiner G, de Roux A, Diel R, Mertsch P, Pink I, Rademacher J, Sutharsan S, Welte T, Zurawski A, et al. Psychometric Validation of the German Translation of the Quality of Life Questionnaire-Bronchiectasis (QOL-B)—Data from the German Bronchiectasis Registry PROGNOSIS. Journal of Clinical Medicine. 2022; 11(2):441. https://doi.org/10.3390/jcm11020441
Chicago/Turabian StyleQuellhorst, Laura, Grit Barten-Neiner, Andrés de Roux, Roland Diel, Pontus Mertsch, Isabell Pink, Jessica Rademacher, Sivagurunathan Sutharsan, Tobias Welte, Annegret Zurawski, and et al. 2022. "Psychometric Validation of the German Translation of the Quality of Life Questionnaire-Bronchiectasis (QOL-B)—Data from the German Bronchiectasis Registry PROGNOSIS" Journal of Clinical Medicine 11, no. 2: 441. https://doi.org/10.3390/jcm11020441
APA StyleQuellhorst, L., Barten-Neiner, G., de Roux, A., Diel, R., Mertsch, P., Pink, I., Rademacher, J., Sutharsan, S., Welte, T., Zurawski, A., Ringshausen, F. C., & on behalf of the PROGNOSIS study group. (2022). Psychometric Validation of the German Translation of the Quality of Life Questionnaire-Bronchiectasis (QOL-B)—Data from the German Bronchiectasis Registry PROGNOSIS. Journal of Clinical Medicine, 11(2), 441. https://doi.org/10.3390/jcm11020441