
Arthritis in Systemic Lupus Erythematosus: From 2022 International GISEA/OEG Symposium

 , ,
, ,  , , ,
, , , 
 ,
,
Abstract
:1. Introduction
2. Pathogenesis of SLE: Focus on the Musculoskeletal Manifestations
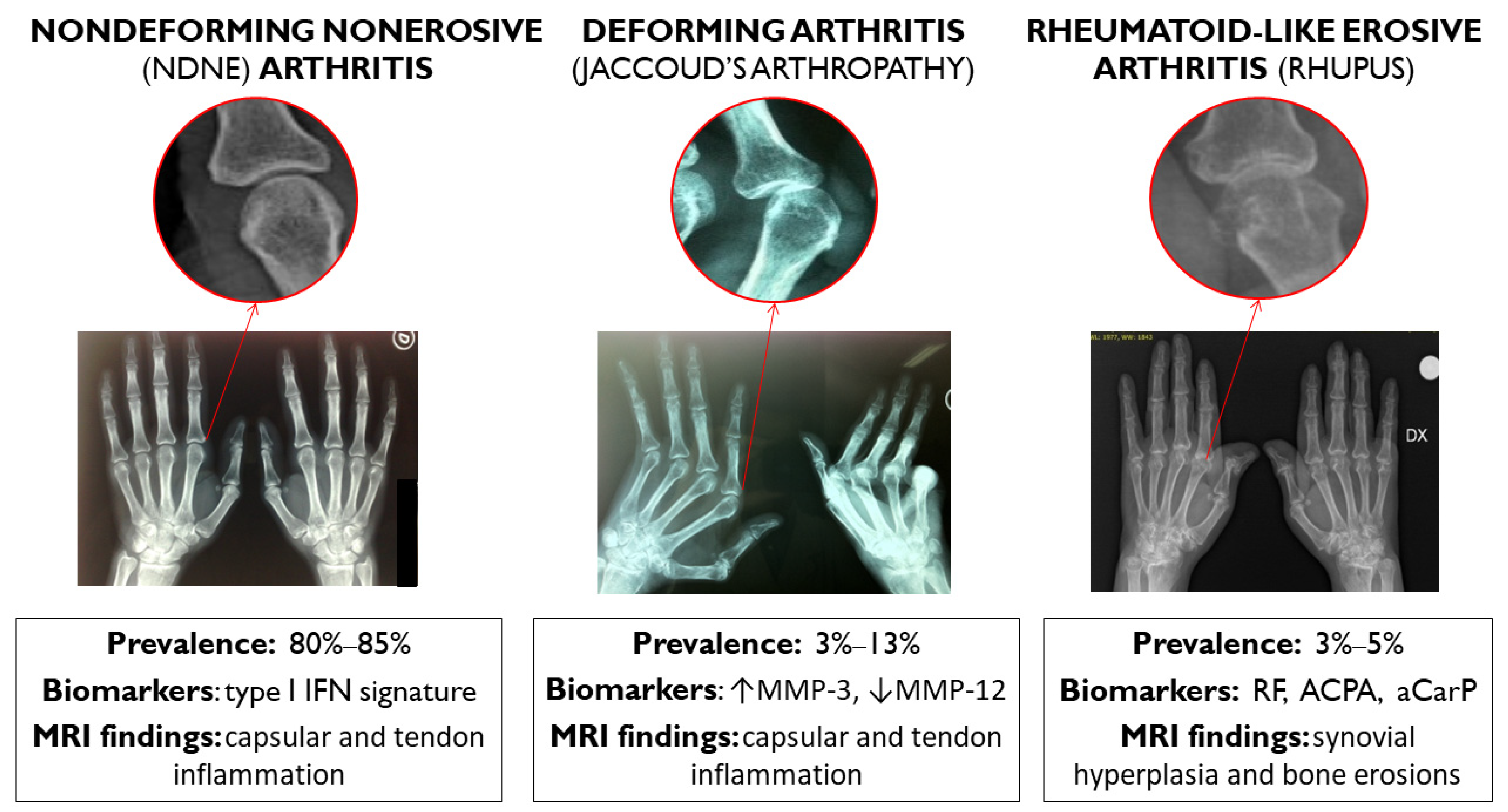
2.1. NDNE and JA
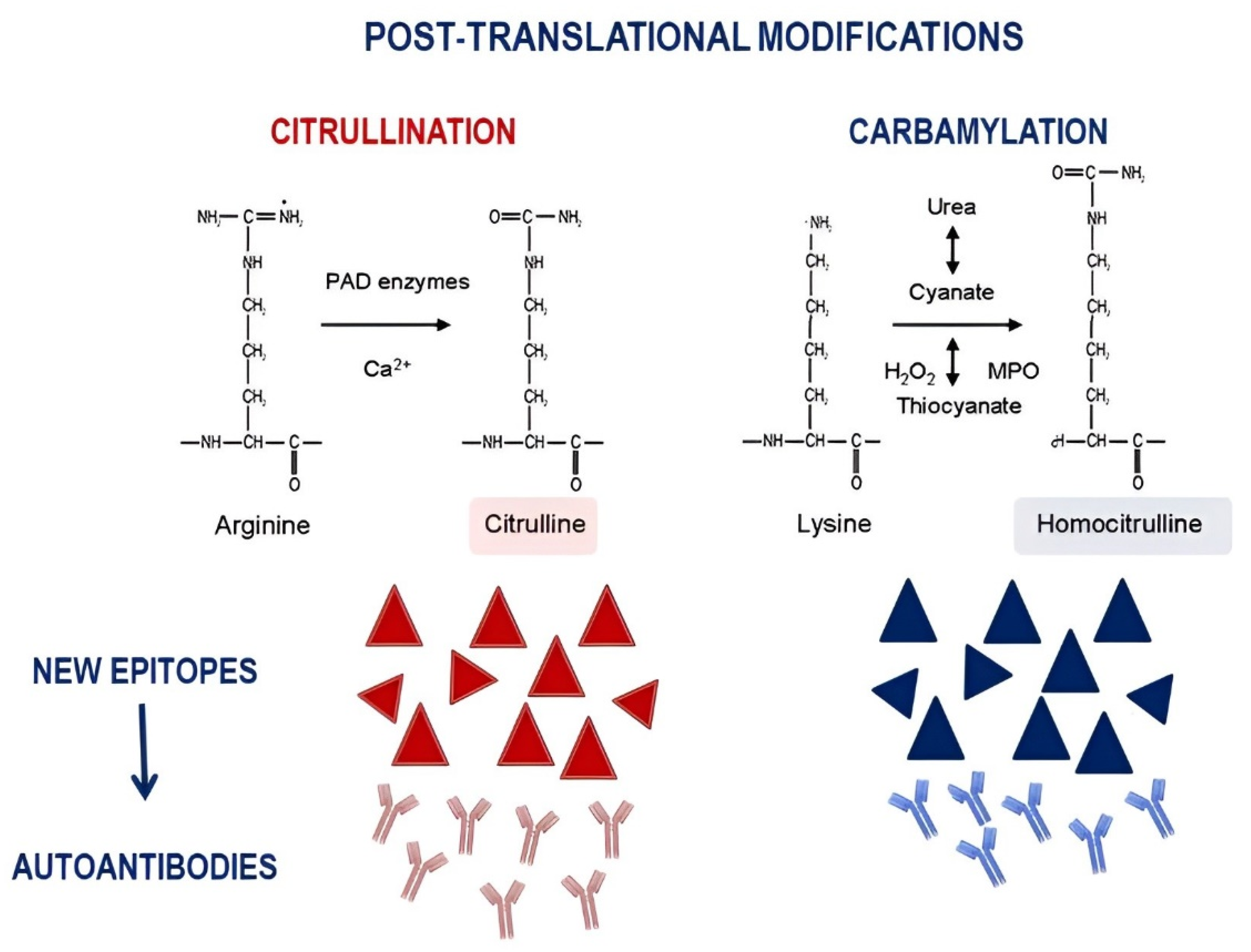
2.2. Erosive Arthritis in SLE
3. The Modern Treatment of SLE: What about the Musculoskeletal Manifestations
Funding
Acknowledgments
Conflicts of Interest
References
- Lapadula, G.; Ferraccioli, G.; Ferri, C.; Punzi, L.; Trotta, F. GISEA: An Italian Biological Agents Registry in Rheumatology. Reumatismo 2011, 63, 155–164. [Google Scholar] [CrossRef] [Green Version]
- Cervera, R.; Khamashta, M.A.; Font, J.; Sebastiani, G.D.; Gil, A.; Lavilla, P.; Mejía, J.C.; Aydintug, A.O.; Chwalinska-Sadowska, H.; De Ramón, E.; et al. Morbidity and Mortality in Systemic Lupus Erythematosus during a 10-Year Period: A Comparison of Early and Late Manifestations in a Cohort of 1000 Patients. Medicine 2003, 82, 299–308. [Google Scholar] [CrossRef]
- Mosca, M.; Costenbader, K.H.; Johnson, S.R.; Lorenzoni, V.; Sebastiani, G.D.; Hoyer, B.F.; Navarra, S.; Bonfa, E.; Ramsey-Goldman, R.; Medina-Rosas, J.; et al. Brief Report: How Do Patients with Newly Diagnosed Systemic Lupus Erythematosus Present? A Multicenter Cohort of Early Systemic Lupus Erythematosus to Inform the Development of New Classification Criteria. Arthritis Rheumatol. 2019, 71, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Floris, A.; Piga, M.; Cauli, A.; Mathieu, A. Predictors of Flares in Systemic Lupus Erythematosus: Preventive Therapeutic Intervention Based on Serial Anti-DsDNA Antibodies Assessment. Analysis of a Monocentric Cohort and Literature Review. Autoimmun. Rev. 2016, 15, 656–663. [Google Scholar] [CrossRef]
- Grossman, J.M. Lupus Arthritis. Best Pract. Res. Clin. Rheumatol. 2009, 23, 495–506. [Google Scholar] [CrossRef]
- Hochberg, M.C. Updating the American College of Rheumatology Revised Criteria for the Classification of Systemic Lupus Erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef]
- Petri, M.; Orbai, A.-M.; Alarcón, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O.; et al. Derivation and Validation of Systemic Lupus International Collaborating Clinics Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Ann. Rheum. Dis. 2019, 78, 1151–1159. [Google Scholar] [CrossRef] [Green Version]
- Ceccarelli, F.; Perricone, C.; Massaro, L.; Pacucci, V.A.; Cipriano, E.; Truglia, S.; Miranda, F.; Spinelli, F.R.; Alessandri, C.; Valesini, G.; et al. The Role of Disease Activity Score 28 in the Evaluation of Articular Involvement in Systemic Lupus Erythematosus. Sci. World J. 2014, 2014, 236842. [Google Scholar] [CrossRef] [Green Version]
- Ceccarelli, F.; Perricone, C.; Cipriano, E.; Massaro, L.; Natalucci, F.; Spinelli, F.R.; Alessandri, C.; Valesini, G.; Conti, F. Usefulness of Composite Indices in the Assessment of Joint Involvement in Systemic Lupus Erythematosus Patients: Correlation with Ultrasonographic Score. Lupus 2019, 28, 383–388. [Google Scholar] [CrossRef]
- Ceccarelli, F.; Perricone, C.; Cipriano, E.; Massaro, L.; Natalucci, F.; Capalbo, G.; Leccese, I.; Bogdanos, D.; Spinelli, F.R.; Alessandri, C.; et al. Joint Involvement in Systemic Lupus Erythematosus: From Pathogenesis to Clinical Assessment. Semin. Arthritis Rheum. 2017, 47, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Ball, E.M.A.; Bell, A.L. Lupus Arthritis—Do We Have a Clinically Useful Classification? Rheumatology 2012, 51, 771–779. [Google Scholar] [CrossRef] [Green Version]
- Tani, C.; D’Aniello, D.; Sedie, A.D.; Carli, L.; Cagnoni, M.; Possemato, N.; Carbone, M.; Della Rossa, A.; Riente, L.; Baldini, C.; et al. Rhupus Syndrome: Assessment of Its Prevalence and Its Clinical and Instrumental Characteristics in a Prospective Cohort of 103 SLE Patients. Autoimmun. Rev. 2013, 12, 537–541. [Google Scholar] [CrossRef]
- Antonini, L.; Le Mauff, B.; Marcelli, C.; Aouba, A.; de Boysson, H. Rhupus: A Systematic Literature Review. Autoimmun. Rev. 2020, 19, 102612. [Google Scholar] [CrossRef]
- Ceccarelli, F.; Natalucci, F.; Olivieri, G.; Perricone, C.; Pirone, C.; Spinelli, F.R.; Alessandri, C.; Conti, F. Erosive Arthritis in Systemic Lupus Erythematosus: Not Only Rhupus. Lupus 2021, 30, 2029–2041. [Google Scholar] [CrossRef]
- Gabba, A.; Piga, M.; Vacca, A.; Porru, G.; Garau, P.; Cauli, A.; Mathieu, A. Joint and Tendon Involvement in Systemic Lupus Erythematosus: An Ultrasound Study of Hands and Wrists in 108 Patients. Rheumatology 2012, 51, 2278–2285. [Google Scholar] [CrossRef] [Green Version]
- Iagnocco, A.; Ceccarelli, F.; Rizzo, C.; Truglia, S.; Massaro, L.; Spinelli, F.R.; Vavala, C.; Valesini, G.; Conti, F. Ultrasound Evaluation of Hand, Wrist and Foot Joint Synovitis in Systemic Lupus Erythematosus. Rheumatology 2014, 53, 465–472. [Google Scholar] [CrossRef] [Green Version]
- Mosca, M.; Tani, C.; Carli, L.; Vagnani, S.; Possemato, N.; Delle Sedie, A.; Cagnoni, M.; D’Aniello, D.; Riente, L.; Caramella, D.; et al. The Role of Imaging in the Evaluation of Joint Involvement in 102 Consecutive Patients with Systemic Lupus Erythematosus. Autoimmun. Rev. 2015, 14, 10–15. [Google Scholar] [CrossRef]
- Budhram, A.; Chu, R.; Rusta-Sallehy, S.; Ioannidis, G.; Denburg, J.A.; Adachi, J.D.; Haaland, D.A. Anti-Cyclic Citrullinated Peptide Antibody as a Marker of Erosive Arthritis in Patients with Systemic Lupus Erythematosus: A Systematic Review and Meta-Analysis. Lupus 2014, 23, 1156–1163. [Google Scholar] [CrossRef]
- Ostendorf, B.; Scherer, A.; Specker, C.; Mödder, U.; Schneider, M. Jaccoud’s Arthropathy in Systemic Lupus Erythematosus: Differentiation of Deforming and Erosive Patterns by Magnetic Resonance Imaging. Arthritis Rheum. 2003, 48, 157–165. [Google Scholar] [CrossRef]
- Piga, M.; Saba, L.; Gabba, A.; Congia, M.; Balestrieri, A.; Mathieu, A.; Cauli, A. Ultrasonographic Assessment of Bone Erosions in the Different Subtypes of Systemic Lupus Erythematosus Arthritis: Comparison with Computed Tomography. Arthritis Res. Ther. 2016, 18, 222. [Google Scholar] [CrossRef] [Green Version]
- Piga, M.; Gabba, A.; Congia, M.; Figus, F.; Cauli, A.; Mathieu, A. Predictors of Musculoskeletal Flares and Jaccoud׳s Arthropathy in Patients with Systemic Lupus Erythematosus: A 5-Year Prospective Study. Semin. Arthritis Rheum. 2016, 46, 217–224. [Google Scholar] [CrossRef] [Green Version]
- Piga, M.; Congia, M.; Gabba, A.; Figus, F.; Floris, A.; Mathieu, A.; Cauli, A. Musculoskeletal Manifestations as Determinants of Quality of Life Impairment in Patients with Systemic Lupus Erythematosus. Lupus 2018, 27, 190–198. [Google Scholar] [CrossRef]
- Girgis, F.L.; Popple, A.W.; Bruckner, F.E. Jaccoud’s Arthropathy. A Case Report and Necropsy Study. Ann. Rheum. Dis. 1978, 37, 561–565. [Google Scholar] [CrossRef] [Green Version]
- Cruickshank, B. Lesions of Joint and Tendon Sheaths in Systemic Lupus Erythematosus. Ann. Rheum. Dis. 1959, 18, 111–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hubbard, E.L.; Catalina, M.D.; Heuer, S.; Bachali, P.; Robl, R.; Geraci, N.S.; Grammer, A.C.; Lipsky, P.E. Analysis of Gene Expression from Systemic Lupus Erythematosus Synovium Reveals Myeloid Cell-Driven Pathogenesis of Lupus Arthritis. Sci. Rep. 2020, 10, 17361. [Google Scholar] [CrossRef]
- Nzeusseu Toukap, A.; Galant, C.; Theate, I.; Maudoux, A.L.; Lories, R.J.U.; Houssiau, F.A.; Lauwerys, B.R. Identification of Distinct Gene Expression Profiles in the Synovium of Patients with Systemic Lupus Erythematosus. Arthritis Rheum. 2007, 56, 1579–1588. [Google Scholar] [CrossRef]
- Liu, Z.; Davidson, A. Taming Lupus-a New Understanding of Pathogenesis Is Leading to Clinical Advances. Nat. Med. 2012, 18, 871–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López, P.; Rodríguez-Carrio, J.; Caminal-Montero, L.; Mozo, L.; Suárez, A. A Pathogenic IFNα, BLyS and IL-17 Axis in Systemic Lupus Erythematosus Patients. Sci. Rep. 2016, 6, 20651. [Google Scholar] [CrossRef] [Green Version]
- Eilertsen, G.; Nikolaisen, C.; Becker-Merok, A.; Nossent, J.C. Interleukin-6 Promotes Arthritis and Joint Deformation in Patients with Systemic Lupus Erythematosus. Lupus 2011, 20, 607–613. [Google Scholar] [CrossRef]
- Sippl, N.; Faustini, F.; Rönnelid, J.; Turcinov, S.; Chemin, K.; Gunnarsson, I.; Malmström, V. Arthritis in Systemic Lupus Erythematosus Is Characterized by Local IL-17A and IL-6 Expression in Synovial Fluid. Clin. Exp. Immunol. 2021, 205, 44–52. [Google Scholar] [CrossRef]
- Piga, M.; Congia, M.; Balestrieri, A.; Angioni, M.M.; Cangemi, I.; Cau, R.; Chessa, E.; Floris, A.; Figus, F.; Iagnocco, A.; et al. Imbalanced MMP-3 and MMP-12 Serum Levels in Systemic Lupus Erythematosus Patients with Jaccoud’s Arthropathy and a Distinctive MRI Pattern. Rheumatology 2021, 60, 4218–4228. [Google Scholar] [CrossRef]
- Mastrangelo, A.; Colasanti, T.; Barbati, C.; Pecani, A.; Sabatinelli, D.; Pendolino, M.; Truglia, S.; Massaro, L.; Mancini, R.; Miranda, F.; et al. The Role of Posttranslational Protein Modifications in Rheumatological Diseases: Focus on Rheumatoid Arthritis. J. Immunol. Res. 2015, 2015, 712490. [Google Scholar] [CrossRef] [Green Version]
- Qing, Y.F.; Zhang, Q.B.; Zhou, J.G.; Yuan, G.H.; Wei, J.; Xing, Y.; Liu, J.P.; Jiang, L.; Chen, J.P. The Detecting and Clinical Value of Anti-Cyclic Citrullinated Peptide Antibodies in Patients with Systemic Lupus Erythematosus. Lupus 2009, 18, 713–717. [Google Scholar] [CrossRef]
- Nielen, M.M.J.; Van Schaardenburg, D.; Reesink, H.W.; Van De Stadt, R.J.; Van Der Horst-Bruinsma, I.E.; De Koning, M.H.M.T.; Habibuw, M.R.; Vandenbroucke, J.P.; Dijkmans, B.A.C. Specific Autoantibodies Precede the Symptoms of Rheumatoid Arthritis: A Study of Serial Measurements in Blood Donors. Arthritis Rheum. 2004, 50, 380–386. [Google Scholar] [CrossRef]
- Shi, J.; Van De Stadt, L.A.; Levarht, E.W.N.; Huizinga, T.W.J.; Hamann, D.; Van Schaardenburg, D.; Toes, R.E.M.; Trouw, L.A. Anti-Carbamylated Protein (Anti-CarP) Antibodies Precede the Onset of Rheumatoid Arthritis. Ann. Rheum. Dis. 2014, 73, 780–783. [Google Scholar] [CrossRef] [PubMed]
- van Delft, M.A.M.; Verheul, M.K.; Burgers, L.E.; Derksen, V.F.A.M.; van der Helm-van Mil, A.H.M.; van der Woude, D.; Huizinga, T.W.J.; Toes, R.E.M.; Trouw, L.A. The Isotype and IgG Subclass Distribution of Anti-Carbamylated Protein Antibodies in Rheumatoid Arthritis Patients. Arthritis Res. Ther. 2017, 19, 190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Truchetet, M.E.; Dublanc, S.; Barnetche, T.; Vittecoq, O.; Mariette, X.; Richez, C.; Blanco, P.; Mahler, M.; Contin-Bordes, C.; Schaeverbeke, T. Association of the Presence of Anti-Carbamylated Protein Antibodies in Early Arthritis with a Poorer Clinical and Radiologic Outcome: Data From the French ESPOIR Cohort. Arthritis Rheumatol. 2017, 69, 2292–2302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pecani, A.; Alessandri, C.; Spinelli, F.R.; Priori, R.; Riccieri, V.; Di Franco, M.; Ceccarelli, F.; Colasanti, T.; Pendolino, M.; Mancini, R.; et al. Prevalence, Sensitivity and Specificity of Antibodies against Carbamylated Proteins in a Monocentric Cohort of Patients with Rheumatoid Arthritis and Other Autoimmune Rheumatic Diseases. Arthritis Res. Ther. 2016, 18, 276. [Google Scholar] [CrossRef] [Green Version]
- Massaro, L.; Ceccarelli, F.; Colasanti, T.; Pendolino, M.; Perricone, C.; Cipriano, E.; Natalucci, F.; Capalbo, G.; Lucchetti, R.; Pecani, A.; et al. Anti-Carbamylated Protein Antibodies in Systemic Lupus Erythematosus Patients with Articular Involvement. Lupus 2018, 27, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Ziegelasch, M.; van Delft, M.A.M.; Wallin, P.; Skogh, T.; Magro-Checa, C.; Steup-Beekman, G.M.; Trouw, L.A.; Kastbom, A.; Sjöwall, C. Antibodies against Carbamylated Proteins and Cyclic Citrullinated Peptides in Systemic Lupus Erythematosus: Results from Two Well-Defined European Cohorts. Arthritis Res. Ther. 2016, 18, 289. [Google Scholar] [CrossRef] [Green Version]
- Ceccarelli, F.; Perricone, C.; Colasanti, T.; Massaro, L.; Cipriano, E.; Pendolino, M.; Natalucci, F.; Mancini, R.; Spinelli, F.R.; Valesini, G.; et al. Anti-Carbamylated Protein Antibodies as a New Biomarker of Erosive Joint Damage in Systemic Lupus Erythematosus. Arthritis Res. Ther. 2018, 20, 126. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Cheema, K.; Anders, H.J.; Aringer, M.; Bajema, I.; Boletis, J.; Frangou, E.; Houssiau, F.A.; Hollis, J.; et al. 2019 Update of the Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) Recommendations for the Management of Lupus Nephritis. Ann. Rheum. Dis. 2020, 79, S713–S723. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, Y. State-of-the-Art Treatment of Systemic Lupus Erythematosus. Int. J. Rheum. Dis. 2020, 23, 465–471. [Google Scholar] [CrossRef] [Green Version]
- Joy, A.; Muralidharan, A.; Alfaraj, M.; Shantharam, D.; Cherukuri, A.S.S.; Muthukumar, A. The Role of Belimumab in Systemic Lupus Erythematosis: A Systematic Review. Cureus 2022, 14, e25887. [Google Scholar] [CrossRef]
- Navarra, S.V.; Guzmán, R.M.; Gallacher, A.E.; Hall, S.; Levy, R.A.; Jimenez, R.E.; Li, E.K.M.; Thomas, M.; Kim, H.Y.; León, M.G.; et al. Efficacy and Safety of Belimumab in Patients with Active Systemic Lupus Erythematosus: A Randomised, Placebo-Controlled, Phase 3 Trial. Lancet 2011, 377, 721–731. [Google Scholar] [CrossRef]
- Iaccarino, L.; Andreoli, L.; Bocci, E.B.; Bortoluzzi, A.; Ceccarelli, F.; Conti, F.; De Angelis, R.; De Marchi, G.; De Vita, S.; Di Matteo, A.; et al. Clinical Predictors of Response and Discontinuation of Belimumab in Patients with Systemic Lupus Erythematosus in Real Life Setting. Results of a Large, Multicentric, Nationwide Study. J. Autoimmun. 2018, 86, 1–8. [Google Scholar] [CrossRef]
- Pimentel-Quiroz, V.R.; Ugarte-Gil, M.F.; Alarcón, G.S. Abatacept for the Treatment of Systemic Lupus Erythematosus. Expert Opin. Investig. Drugs 2016, 25, 493–499. [Google Scholar] [CrossRef]
- Benucci, M.; Damiani, A.; Li Gobbi, F.; Grossi, V.; Infantino, M.; Arena, A.; Manfredi, M. Jaccoud’s Arthropathy, an Unusual Manifestation of Idiopathic Retroperitoneal Fibrosis: Rapid Improvement of Symptoms after Tocilizumab Treatment. Reumatismo 2017, 69, 88–91. [Google Scholar] [CrossRef] [Green Version]
- Ocampo, V.; Haaland, D.; Legault, K.; Mittoo, S.; Aitken, E. Successful Treatment of Recurrent Pleural and Pericardial Effusions with Tocilizumab in a Patient with Systemic Lupus Erythematous. BMJ Case Rep. 2016, 2016, bcr2016215423. [Google Scholar] [CrossRef] [PubMed]
- Piantoni, S.; Korsten, P. Rituximab-a B Cell Targeted Therapy in Systemic Lupus Erythematosus: Where Do We Stand? Rheumatology 2022, 61, 1752–1755. [Google Scholar] [CrossRef]
- Teng, S.; Tian, Y.; Luo, N.; Zheng, Q.; Shao, M.; Li, L. Efficacy and Safety of an Anti-CD20 Monoclonal Antibody, Rituximab, for Lupus Nephritis: A Meta-Analysis. Int. J. Rheum. Dis. 2022, 25, 101–109. [Google Scholar] [CrossRef]
- Piga, M.; Gabba, A.; Cauli, A.; Garau, P.; Vacca, A.; Mathieu, A. Rituximab Treatment for “Rhupus Syndrome”: Clinical and Power-Doppler Ultrasonographic Monitoring of Response. A Longitudinal Pilot Study. Lupus 2013, 22, 624–628. [Google Scholar] [CrossRef]
- van Vollenhoven, R.F.; Hahn, B.H.; Tsokos, G.C.; Lipsky, P.; Gordon, R.M.; Fei, K.; Lo, K.H.; Chevrier, M.; Rose, S.; Berry, P.; et al. Efficacy and Safety of Ustekinumab in Patients with Active Systemic Lupus Erythematosus: Results of a Phase II Open-Label Extension Study. J. Rheumatol. 2022, 49, 380–387. [Google Scholar] [CrossRef]
- Werth, V.P.; Merrill, J.T. A Double-Blind, Randomized, Placebo-Controlled, Phase II Trial of Baricitinib for Systemic Lupus Erythematosus: How to Optimize Lupus Trials to Examine Effects on Cutaneous Lupus Erythematosus. Br. J. Dermatol. 2019, 180, 964–965. [Google Scholar] [CrossRef] [Green Version]
- Mok, C.C. The Jakinibs in Systemic Lupus Erythematosus: Progress and Prospects. Expert Opin. Investig. Drugs 2019, 28, 85–92. [Google Scholar] [CrossRef]
- Hasni, S.A.; Gupta, S.; Davis, M.; Poncio, E.; Temesgen-Oyelakin, Y.; Carlucci, P.M.; Wang, X.; Naqi, M.; Playford, M.P.; Goel, R.R.; et al. Phase 1 Double-Blind Randomized Safety Trial of the Janus Kinase Inhibitor Tofacitinib in Systemic Lupus Erythematosus. Nat. Commun. 2021, 12, 3391. [Google Scholar] [CrossRef] [PubMed]
- Morand, E.F.; Furie, R.; Tanaka, Y.; Bruce, I.N.; Askanase, A.D.; Richez, C.; Bae, S.-C.; Brohawn, P.Z.; Pineda, L.; Berglind, A.; et al. Trial of Anifrolumab in Active Systemic Lupus Erythematosus. N. Engl. J. Med. 2020, 382, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Furie, R.; Morand, E.F.; Askanase, A.D.; Vital, E.M.; Merrill, J.T.; Kalyani, R.N.; Abreu, G.; Pineda, L.; Tummala, R. Anifrolumab Reduces Flare Rates in Patients with Moderate to Severe Systemic Lupus Erythematosus. Lupus 2021, 30, 1254–1263. [Google Scholar] [CrossRef]
- Jayne, D.; Rovin, B.; Mysler, E.F.; Furie, R.A.; Houssiau, F.A.; Trasieva, T.; Knagenhjelm, J.; Schwetje, E.; Chia, Y.L.; Tummala, R.; et al. Phase II Randomised Trial of Type I Interferon Inhibitor Anifrolumab in Patients with Active Lupus Nephritis. Ann. Rheum. Dis. 2022, 81, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Vital, E.M.; Merrill, J.T.; Morand, E.F.; Furie, R.A.; Bruce, I.N.; Tanaka, Y.; Manzi, S.; Kalunian, K.C.; Kalyani, R.N.; Streicher, K.; et al. Anifrolumab Efficacy and Safety by Type I Interferon Gene Signature and Clinical Subgroups in Patients with SLE: Post Hoc Analysis of Pooled Data from Two Phase III Trials. Ann. Rheum. Dis. 2022, 81, 951–961. [Google Scholar] [CrossRef]
- Chatham, W.W.; Furie, R.; Saxena, A.; Brohawn, P.; Schwetje, E.; Abreu, G.; Tummala, R. Long-Term Safety and Efficacy of Anifrolumab in Adults with Systemic Lupus Erythematosus: Results of a Phase II Open-Label Extension Study. Arthritis Rheumatol. 2021, 73, 816–825. [Google Scholar] [CrossRef]
- Parra Sánchez, A.R.; Voskuyl, A.E.; van Vollenhoven, R.F. Treat-to-Target in Systemic Lupus Erythematosus: Advancing towards Its Implementation. Nat. Rev. Rheumatol. 2022, 18, 146–157. [Google Scholar] [CrossRef]
- Idborg, H.; Oke, V. Cytokines as Biomarkers in Systemic Lupus Erythematosus: Value for Diagnosis and Drug Therapy. Int. J. Mol. Sci. 2021, 22, 11327. [Google Scholar] [CrossRef]
- Catalina, M.D.; Owen, K.A.; Labonte, A.C.; Grammer, A.C.; Lipsky, P.E. The Pathogenesis of Systemic Lupus Erythematosus: Harnessing Big Data to Understand the Molecular Basis of Lupus. J. Autoimmun. 2020, 110, 102359. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Phenotypes | Prevalence According to Traditional X-ray | Prevalence According to Ultrasound | Biomarkers Available | Treatment |
|---|---|---|---|---|
| Nondeforming nonerosive arthritis | 80–85% | 40–60% | Type I interferon signature | First-line treatment: GCs, HCQ, MTX Second-line treatment: belimumab |
| Deforming arthritis (Jaccoud’s arthropathy) | 3–13% | 2–47% | MMP3, MMP12 | First-line treatment: GCs, HCQ, MTX Second-line treatment: belimumab |
| Rheumatoid-like erosive arthritis (rhupus) | 3–5% | about 5% | RF, ACPA Anti-CarP | First-line treatment: GCs, HCQ, MTX Second-line treatment: belimumab Third-line treatment: rituximab |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceccarelli, F.; Govoni, M.; Piga, M.; Cassone, G.; Cantatore, F.P.; Olivieri, G.; Cauli, A.; Favalli, E.G.; Atzeni, F.; Gremese, E.; et al. Arthritis in Systemic Lupus Erythematosus: From 2022 International GISEA/OEG Symposium. J. Clin. Med. 2022, 11, 6016. https://doi.org/10.3390/jcm11206016
Ceccarelli F, Govoni M, Piga M, Cassone G, Cantatore FP, Olivieri G, Cauli A, Favalli EG, Atzeni F, Gremese E, et al. Arthritis in Systemic Lupus Erythematosus: From 2022 International GISEA/OEG Symposium. Journal of Clinical Medicine. 2022; 11(20):6016. https://doi.org/10.3390/jcm11206016
Chicago/Turabian StyleCeccarelli, Fulvia, Marcello Govoni, Matteo Piga, Giulia Cassone, Francesco Paolo Cantatore, Giulio Olivieri, Alberto Cauli, Ennio Giulio Favalli, Fabiola Atzeni, Elisa Gremese, and et al. 2022. "Arthritis in Systemic Lupus Erythematosus: From 2022 International GISEA/OEG Symposium" Journal of Clinical Medicine 11, no. 20: 6016. https://doi.org/10.3390/jcm11206016
APA StyleCeccarelli, F., Govoni, M., Piga, M., Cassone, G., Cantatore, F. P., Olivieri, G., Cauli, A., Favalli, E. G., Atzeni, F., Gremese, E., Iannone, F., Caporali, R., Sebastiani, M., Ferraccioli, G. F., Lapadula, G., & Conti, F. (2022). Arthritis in Systemic Lupus Erythematosus: From 2022 International GISEA/OEG Symposium. Journal of Clinical Medicine, 11(20), 6016. https://doi.org/10.3390/jcm11206016