
Relationship between Pulmonary Regurgitation and Ventriculo–Arterial Interactions in Patients with Post-Early Repair of Tetralogy of Fallot: Insights from Wave-Intensity Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. CMR Imaging
2.3. Wave-Intensity Analysis
2.4. Data Analysis and Statistics
3. Results
3.1. Ventricular Function from CMR
3.2. Wave-Intensity Analysis
4. Discussion
4.1. Limitations
4.2. Clinical Significance
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parker, K.; Jones, C. Forward and Backward Running Waves in the Arteries: Analysis Using the Method of Characteristics. J. Biomech. Eng. 1990, 112, 322. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Khir, A. Determination of wave speed and wave separation in the arteries using diameter and velocity. J. Biomech. 2010, 43, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Biglino, G.; Ntsinjana, H.; Plymen, C.; Tann, O.; Giardini, A.; Derrick, G.; Parker, K.H.; Tsang, V.; Schievano, S.; Taylor, A.M. Ventriculovascular interactions late after atrial and arterial repair of transposition of the great arteries. J. Thorac. Cardiovasc. Surg. 2014, 148, 2627–2633. [Google Scholar] [CrossRef] [Green Version]
- Ohte, N.; Narita, H.; Sugawara, M.; Niki, K.; Okada, T.; Harada, A.; Hayano, J.; Kimura, G. Clinical usefulness of carotid arterial wave intensity in assessing left ventricular systolic and early diastolic performance. Heart Vessel. 2003, 18, 107–111. [Google Scholar] [CrossRef]
- Ammash, N.; Dearani, J.A.; Burkhart, H.M.; Connolly, H.M. Pulmonary Regurgitation after Tetralogy of Fallot Repair: Clinical Features, Sequelae, and Timing of Pulmonary Valve Replacement. Congenit. Heart Dis. 2007, 2, 386–403. [Google Scholar] [CrossRef] [PubMed]
- Kang, I. Differential Regurgitation in Branch Pulmonary Arteries After Repair of Tetralogy of Fallot: A Phase-Contrast Cine Magnetic Resonance Study. Circulation 2003, 107, 2938–2943. [Google Scholar] [CrossRef]
- Kempny, A.; Redington, A.; Benson, L. Right ventricular-left ventricular interaction in adults with Tetralogy of Fallot: A combined cardiac magnetic resonance and echocardiographic speckle tracking study. Int. J. Cardiol. 2012, 154, 259–264. [Google Scholar] [CrossRef]
- Bichell, D.P. Commentary: Ventriculo-ventricular interaction: A bad neighbor brings down the neighborhood. J. Thorac. Cardiovasc. Surg. 2020, 160, 1016–1017. [Google Scholar] [CrossRef] [PubMed]
- Brookes, C.; Ravn, H.; White, P.; Moeldrup, U.; Oldershaw, P.; Redington, A. Acute right ventricular dilatation in response to ischemia significantly impairs left ventricular systolic performance. Circulation 1999, 100, 761–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frigiola, A.; Redington, A.N.; Cullen, S.; Vogel, M. Pulmonary Regurgitation Is an Important Determinant of Right Ventricular Contractile Dysfunction in Patients with Surgically Repaired Tetralogy of Fallot. Circulation 2004, 110, 153–157. [Google Scholar] [CrossRef]
- Van Arsdell, G.S.; Maharaj, G.S.; Tom, J.; Rao, V.K.; Coles, J.G.; Freedom, R.M.; Williams, W.G.; McCrindle, B.W. What is the Optimal Age for Repair of Tetralogy of Fallot? Circulation 2000, 102, 123–129. [Google Scholar] [CrossRef]
- Benbrik, N.; Romefort, B.; Le Gloan, L.; Warin, K.; Hauet, Q.; Guerin, P.; Baron, O.; Gournay, V. Late repair of tetralogy of Fallot during childhood in patients from developing countries. Eur. J. Cardio-Thorac. Surg. 2015, 47, 113–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romeo, J.L.R.; Etnel, J.R.; Takkenberg, J.J.; Roos-Hesselink, J.W.; Helbing, W.A.; van de Woestijne, P.; Bogers, A.J.; Mokhles, M.M. Outcome after surgical repair of tetralogy of Fallot: A systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2020, 159, 220–236. [Google Scholar] [CrossRef] [Green Version]
- Mimic, B.; Brown, K.L.; Oswal, N.; Simmonds, J.; Hsia, T.-Y.; Tsang, V.T.; De Leval, M.R.; Kostolny, M. Neither age at repair nor previous palliation affects outcome in tetralogy of Fallot repair. Eur. J. Cardiothorac. Surg. 2014, 45, 92–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odille, F.; Steeden, J.; Muthurangu, V.; Atkinson, D. Automatic segmentation propagation of the aorta in real-time phase contrast MRI using nonrigid registration. J. Magn. Reson. Imaging 2011, 33, 232–238. [Google Scholar] [CrossRef]
- Parker, K. An introduction to wave intensity analysis. Med. Biol. Eng. Comput. 2009, 47, 175–188. [Google Scholar] [CrossRef]
- Biglino, G.; Steeden, J.A.; Baker, C.; Schievano, S.; Taylor, A.M.; Parker, K.H.; Muthurangu, V. A non-invasive clinical application of wave intensity analysis based on ultrahigh temporal resolution phase-contrast cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2012, 14, 57. [Google Scholar] [CrossRef] [Green Version]
- Gatzoulis, M.; Till, J.; Redington, A. Depolarization-Repolarization Inhomogeneity after Repair of Tetralogy of Fallot: The Substrate for Malignant Ventricular Tachycardia? Circulation 1997, 95, 401–404. [Google Scholar] [CrossRef]
- Gatzoulis, M.; Balaji, S.; Webber, S.A.; Siu, S.C.; Hokanson, J.S.; Poile, C.; Rosenthal, M.; Nakazawa, M.; Moller, J.H.; Gillette, P.C.; et al. Risk factors for arrhythmia and sudden cardiac death late after repair of tetralogy of Fallot: A multicentre study. Lancet 2000, 356, 975–981. [Google Scholar] [CrossRef]
- Eyskens, B.; Reybrouck, T.; Bogaert, J.; Dymarkowsky, S.; Daenen, W.; Dumoulin, M.; Gewillig, M. Homograft insertion for pulmonary regurgitation after repair of tetralogy of Fallot improves cardiorespiratory exercise performance. Am. J. Cardiol. 2000, 85, 221–225. [Google Scholar] [CrossRef]
- Therrien, J.; Siu, S.; Harris, L.; Dore, A.; Niwa, K.; Janousek, J.; Williams, W.; Webb, G.; Gatzoulis, M. Impact of Pulmonary Valve Replacement on Arrhythmia Propensity Late After Repair of Tetralogy of Fallot. Circulation 2001, 103, 2489–2494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oechslin, E.; Harrison, D.; Harris, L.; Downar, E.; Webb, G.; Siu, S.; Williams, W. Reoperation in adults with repair of tetralogy of fallot: Indications and outcomes. J. Thorac. Cardiovasc. Surg. 1999, 118, 245–251. [Google Scholar] [CrossRef] [Green Version]
- Schievano, S.; Capelli, C.; Young, C.; Lurz, P.; Nordmeyer, J.; Owens, C.; Bonhoeffer, P.; Taylor, A.M. Four-dimensional computed tomography: A method of assessing right ventricular outflow tract and pulmonary artery deformations throughout the cardiac cycle. Eur. Radiol. 2010, 21, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Rutz, T.; Max, F.; Wahl, A.; Wustmann, K.; Khattab, K.; Pfammatter, J.-P.; Kadner, A.; Schwerzmann, M. Distensibility and Diameter of Ascending Aorta Assessed by Cardiac Magnetic Resonance Imaging in Adults with Tetralogy of Fallot or Complete Transposition. Am. J. Cardiol. 2012, 110, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Bouzas, B. Pulmonary regurgitation: Not a benign lesion. Eur. Heart J. 2004, 26, 433–439. [Google Scholar] [CrossRef] [Green Version]
- Champion, H.; Michelakis, E.; Hassoun, P. Comprehensive Invasive and Noninvasive Approach to the Right Ventricle-Pulmonary Circulation Unit: State of the Art and Clinical and Research Implications. Circulation 2009, 120, 992–1007. [Google Scholar] [CrossRef] [Green Version]
- Helbing, W.; Niezen, R.A.; Le Cessie, S.; Van Der Geest, R.J.; Ottenkamp, J.; De Roos, A. Right Ventricular Diastolic Function in Children with Pulmonary Regurgitation after Repair of Tetralogy of Fallot: Volumetric Evaluation by Magnetic Resonance Velocity Mapping. J. Am. Coll. Cardiol. 1996, 28, 1827–1835. [Google Scholar] [CrossRef]
- Davlouros, P.; Kilner, P.; Hornung, T. Right ventricular function in adults with repaired tetralogy of fallot assessed with cardiovascular magnetic resonance imaging: Detrimental role of right ventricular outflow aneurysms or akinesia and adverse right-to-left ventricular interaction. ACC Curr. J. Rev. 2003, 12, 101. [Google Scholar] [CrossRef]
- Sophocleous, F.; Biffi, B.; Milano, E.G.; Bruse, J.; Caputo, M.; Rajakaruna, C.; Schievano, S.; Emanueli, C.; Bucciarelli-Ducci, C.; Biglino, G. Aortic morphological variability in patients with bicuspid aortic valve and aortic coarctation. Eur. J. Cardio-Thorac. Surg. 2019, 55, 704–713. [Google Scholar] [CrossRef]
- Sophocleous, F.; Bône, A.; Shearn, A.I.; Forte MN, V.; Bruse, J.L.; Caputo, M.; Biglino, G. Feasibility of a longitudinal statistical atlas model to study aortic growth in congenital heart disease. Comput. Biol. Med. 2022, 144, 105326. [Google Scholar] [CrossRef]
- Mongeon, F.-P.; Gurwitz, M.; Broberg, C.; Aboulhosn, J.; Opotowsky, A.; Kay, J.; Valente, A.; Earing, M.; Lui, G.; Gersony, D.; et al. Aortic root dilatation in adults with surgically repaired tetralogy of fallot: A multicenter cross-sectional study. Circulation 2013, 127, 172–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, W.; Hu, Y.-L.; Coast, D.; Vido, D.A.; Kramer, C.M.; Pyeritz, R.E.; Reichek, N. Age-associated changes in regional aortic pulse wave velocity. J. Am. Coll. Cardiol. 2001, 38, 1123–1129. [Google Scholar] [CrossRef] [Green Version]
- Kozerke, S.; Scheidegger, M.; Pedersen, E.; Boesiger, P. Heart motion adapted cine phase-contrast flow measurements through the aortic valve. Magn. Reson. Med. 1999, 42, 970–978. [Google Scholar] [CrossRef]
- Kilner, P.; Gatehouse, P.; Firmin, D. Flow Measurement by Magnetic Resonance: A Unique Asset Worth Optimising. J. Cardiovasc. Magn. Reson. 2007, 9, 723–728. [Google Scholar] [CrossRef]
- Quail, M.A.; Steeden, J.A.; Taylor, A.M.; Muthurangu, V. The Effect of Temporal Resolution on MR Assessment of Pulse Wave Velocity. Artery Res. 2013, 7, 157–158. [Google Scholar] [CrossRef]
- Khir, A.; Zambanini, A.; Parker, K. Local and regional wave speed in the aorta: Effects of arterial occlusion. Med. Eng. Phys. 2004, 26, 23–29. [Google Scholar] [CrossRef]
- van den Wijngaard, J.; Siebes, M.; Westerhof, B. Comparison of arterial waves derived by classical wave separation and wave intensity analysis in a model of aortic coarctation. Med. Biol. Eng. Comput. 2008, 47, 211–220. [Google Scholar] [CrossRef] [Green Version]
- Quail, M.; Frigiola, A.; Giardini, A.; Muthurangu, V.; Hughes, M.; Lurz, P.; Khambadkone, S.; Deanfield, J.E.; Tsang, V.; Taylor, A.M. Impact of Pulmonary Valve Replacement in Tetralogy of Fallot with Pulmonary Regurgitation: A Comparison of Intervention and Nonintervention. Ann. Thorac. Surg. 2012, 94, 1619–1626. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | No PR (n = 17) | Mild (n = 38) | Moderate (n = 90) | Severe (n = 56) | p (Overall) |
|---|---|---|---|---|---|
| Age at magnetic resonance imaging (MRI) follow-up scan (y) | 17 ± 5 | 16 ± 10 | 15 ± 9 | 14 ± 6 | 0.062 |
| Sex (M/F) | 7/10 | 24/14 | 55/35 | 43/13 | 0.043 |
| BSA (m2) | 1.7 ± 0.3 | 1.5 ± 0.5 | 1.5 ± 0.4 | 1.4 ± 0.4 | 0.007 |
| HR (bmp) | 75 ± 10 | 78 ± 5 | 80 ± 13 | 79 ± 3 | 0.583 |
| PR (%) | 0 | 9 ± 6 | 30 ± 5 | 49 ± 6 | 0.000 |
| LV EDVi (mL/m2) | 73 ± 12 | 75 ± 11 | 72 ± 12 | 73 ± 17 | 0.331 |
| LV ESVi (mL/m2) | 25 ± 8 | 28 ± 10 | 26 ± 7 | 30 ± 9 | 0.064 |
| LV SV (mL) | 82 ± 13 | 74 ± 28 | 67 ± 21 | 64 ± 26 | 0.007 |
| LV EF (%) | 67 ± 7 | 64 ± 8 | 64 ± 5 | 61 ± 6 | 0.001 |
| LV CI (L/min/m2) | 3.6 ± 0.6 | 3.7 ± 0.7 | 3.6 ± 0.7 | 3.6 ± 1.0 | 0.733 |
| RV EDVi (mL/m2) | 88 ± 17 | 98 ± 26 | 112 ± 35 | 154 ± 35 | 0.000 |
| RV ESVi (mL/m2) | 38 ± 14 | 43 ± 15 | 49 ± 24 | 73 ± 27 | 0.000 |
| RV SV (mL) | 83 ± 15 | 83 ± 39 | 94 ± 33 | 114 ± 42 | 0.001 |
| RV EF (%) | 58 ± 10 | 59 ± 10 | 58 ± 9 | 54 ± 8 | 0.103 |
| RV CI (L/min/m2) | 3.7 ± 0.7 | 4.4 ± 1.0 | 5.1 ± 1.0 | 6.4 ± 1.4 | 0.000 |
| Variable | No PR (n = 17) | Mild (n = 38) | Moderate (n = 90) | Severe (n = 56) | p (Overall) |
|---|---|---|---|---|---|
| Wave speed (m/s) | 3.9 ± 0.7 | 4.7 ± 1.1 | 4.9 ± 1.6 | 5.8 ± 1.5 | 0.000 |
| Distensibility (×10−3 1/mmHg) | 8.8 ± 2.8 | 6.5 ± 3.0 | 6.8 ± 3.6 | 4.8 ± 3.0 | 0.000 |
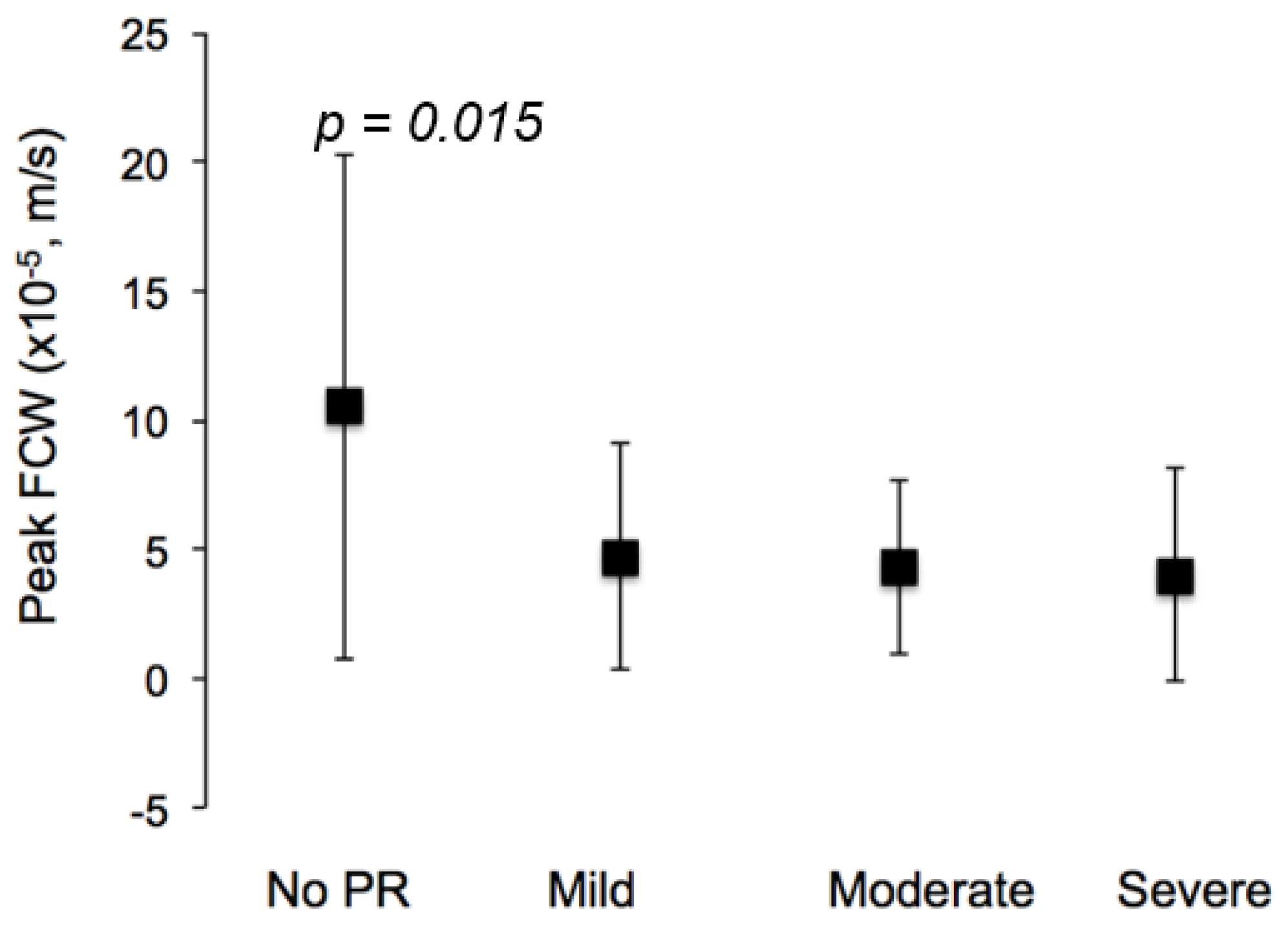
| FCW peak (×10−5, m/s) | 10.5 ± 9.7 | 4.7 ± 4.4 | 4.3 ± 3.4 | 4.0 ± 4.1 | 0.015 |
| FCW area (×10−3, m) | 2.7 ± 2.1 | 1.4 ± 1.3 | 1.3 ± 1.0 | 1.3 ± 1.3 | 0.021 |
| FEW peak (×10−5, m/s) | 0.6 ± 0.4 | 0.6 ± 0.5 | 0.7 ± 0.6 | 0.6 ± 0.4 | 0.578 |
| FEW area (×10−3, m) | 0.3 ± 0.2 | 0.3 ± 0.2 | 0.3 ± 0.2 | 0.3 ± 0.2 | 0.415 |
| FCW Predictor | Univariate | Multivariate | |
|---|---|---|---|
| Extent of PR (%) | p = 0.001, R2 = 0.053 | p = 0.971 | |
| Age at time of MRI (y) | p = 0.006, R2 = 0.037 | p = 0.065 | R2 = 0.097 |
| Sex (M/F) | p = 0.878, R2 = 0.000 | p = 0.948 | |
| Distensibility | p = 0.001, R2 = 0.073 | p = 0.003 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arya, N.; Schievano, S.; Caputo, M.; Taylor, A.M.; Biglino, G. Relationship between Pulmonary Regurgitation and Ventriculo–Arterial Interactions in Patients with Post-Early Repair of Tetralogy of Fallot: Insights from Wave-Intensity Analysis. J. Clin. Med. 2022, 11, 6186. https://doi.org/10.3390/jcm11206186
Arya N, Schievano S, Caputo M, Taylor AM, Biglino G. Relationship between Pulmonary Regurgitation and Ventriculo–Arterial Interactions in Patients with Post-Early Repair of Tetralogy of Fallot: Insights from Wave-Intensity Analysis. Journal of Clinical Medicine. 2022; 11(20):6186. https://doi.org/10.3390/jcm11206186
Chicago/Turabian StyleArya, Nikesh, Silvia Schievano, Massimo Caputo, Andrew M. Taylor, and Giovanni Biglino. 2022. "Relationship between Pulmonary Regurgitation and Ventriculo–Arterial Interactions in Patients with Post-Early Repair of Tetralogy of Fallot: Insights from Wave-Intensity Analysis" Journal of Clinical Medicine 11, no. 20: 6186. https://doi.org/10.3390/jcm11206186