
Multimodal Treatment with Cognitive Behavioral Therapeutic Intervention Plus Bladder Treatment Is More Effective than Monotherapy for Patients with Interstitial Cystitis/Bladder Pain Syndrome—A Randomized Clinical Trial

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Ethical Considerations
2.2. Participants
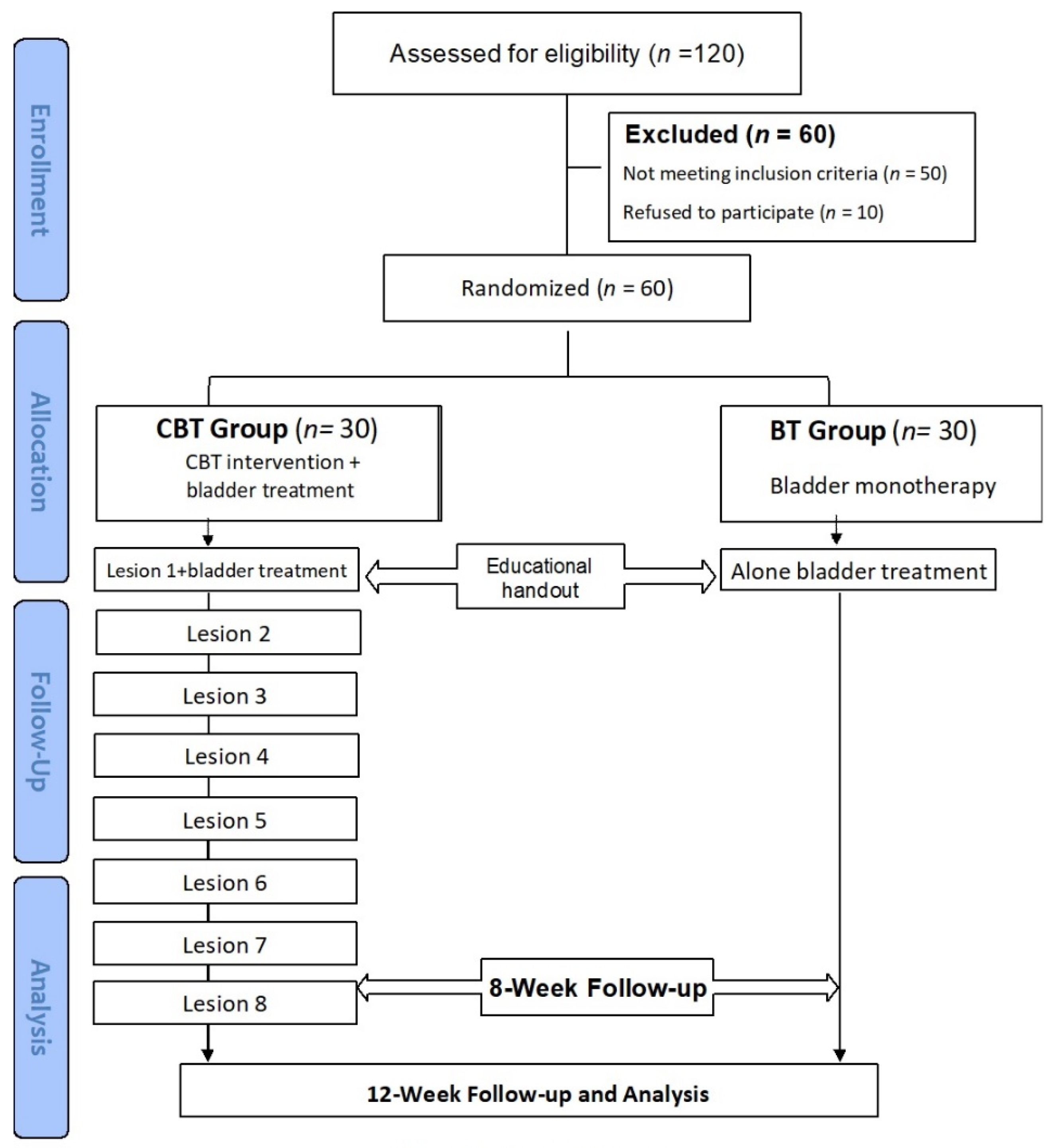
2.3. Randomization
2.4. Treatment Procedure
2.5. Treatment Outcomes
2.6. Sample Size and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Homma, Y.; Akiyama, Y.; Tomoe, H.; Furuta, A.; Ueda, T.; Maeda, D.; Lin, A.T.; Kuo, H.C.; Lee, M.H.; Oh, S.J. Clinical guidelines for interstitial cystitis/bladder pain syndrome. Int. J. Urol. 2020, 27, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Hanno, P.M.; Erickson, D.; Moldwin, R.; Faraday, M.M. Diagnosis and treatment of interstitial cystitis/bladder pain syndrome: AUA guideline amendment. J. Urol. 2015, 193, 1545–1553. [Google Scholar] [CrossRef] [PubMed]
- Van de Merwe, J.P.; Nordling, J.; Bouchelouche, P.; Bouchelouche, K.; Cervigni, M.; Daha, L.K.; Elneil, S.; Fall, M.; Hohlbrugger, G.; Irwin, P. Diagnostic criteria, classification, and nomenclature for painful bladder syndrome/interstitial cystitis: An ESSIC proposal. Eur. Urol. 2008, 53, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.C.; Meng, E.; Chancellor, M.; Kuo, H.C. Pain reduction realized with extracorporeal shock wave therapy for the treatment of symptoms associated with interstitial cystitis/bladder pain syndrome—A prospective, multicenter, randomized, double-blind, placebo-controlled study. Neurourol. Urodyn. 2020, 39, 1505–1514. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.R.; Peng, T.C.; Yeh, H.L.; Kuo, H.C. Anxiety severity does not influence treatment outcomes in patients with interstitial cystitis/bladder pain syndrome. Neurourol. Urodyn. 2019, 38, 1602–1610. [Google Scholar] [CrossRef]
- Malde, S.; Palmisani, S.; Al-Kaisy, A.; Sahai, A. Guideline of guidelines: Bladder pain syndrome. BJU Int. 2018, 122, 729–743. [Google Scholar] [CrossRef]
- Trama, F.; Illiano, E.; Marchesi, A.; Brancorsini, S.; Crocetto, F.; Pandolfo, S.D.; Zucchi, A.; Costantini, E. Use of intravesical injections of platelet-rich plasma for the treatment of bladder pain syndrome: A comprehensive literature review. Antibiotics 2021, 10, 1194. [Google Scholar] [CrossRef]
- Jhang, J.-F.; Jiang, Y.-H.; Kuo, H.-C. Current Understanding of the Pathophysiology and Novel Treatments of Interstitial Cystitis/Bladder Pain Syndrome. Biomedicines 2022, 10, 2380. [Google Scholar] [CrossRef]
- Kim, B.S.; Omizo, M.M. Asian cultural values, attitudes toward seeking professional psychological help, and willingness to see a counselor. Couns. Psychol. 2003, 31, 343–361. [Google Scholar] [CrossRef]
- Bernard, P.; Romain, A.J.; Caudroit, J.; Chevance, G.; Carayol, M.; Gourlan, M.; Dancause, K.; Moullec, G. Cognitive Behavioral Therapy combined with physical exercise for depression, anxiety, fatigue and pain in adults with chronic diseases: Systematic review and meta-analysis. Health Psychol. 2018, 37, 433–450. [Google Scholar] [CrossRef]
- Williams, D.A. Cognitive-behavioral therapy in central sensitivity syndromes. Curr. Rheumatol. Rev. 2016, 12, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T. Cognitive therapy: A 30-year retrospective. Am. Psychol. 1991, 46, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Kanter, G.; Komesu, Y.M.; Qaedan, F.; Jeppson, P.C.; Dunivan, G.C.; Cichowski, S.B.; Rogers, R.G. Mindfulness-based stress reduction as a novel treatment for interstitial cystitis/bladder pain syndrome: A randomized controlled trial. Int. Urogynecology J. 2016, 27, 1705–1711. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomized trials. Obstet. Gynecol. 2010, 115, 1063–1070. [Google Scholar] [CrossRef]
- Propert, K.; Mayer, R.; Wang, Y.; Sant, G.; Hanno, P.; Peters, K.; Kusek, J.; Interstitial Cystitis Clinical Trials Group. Responsiveness of symptom scales for interstitial cystitis. Urology 2006, 67, 55–59. [Google Scholar] [CrossRef]
- Julian, L.J. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Care Res. 2011, 63, S467–S472. [Google Scholar] [CrossRef]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck Depression Inventory (BDI-II); Pearson: London, UK, 1996; Volume 10. [Google Scholar] [CrossRef]
- Weng, C.Y.; Denollet, J.; Lin, C.L.; Lin, T.K.; Wang, W.C.; Lin, J.J.; Wong, S.S.; Mols, F. The validity of the Type D construct and its assessment in Taiwan. BMC Psychiatry 2013, 13, 1–9. [Google Scholar] [CrossRef]
- Chu, L.C.; Kao, H.S.R. The Moderation of Meditation Experience and Emotional Intelligence on the Relationship between Perceived Stress and Negative Mental Health. Chin. J. Psychol. 2005, 47, 157–179. [Google Scholar] [CrossRef]
- Chen, C.H.; Tseng, Y.F.; Wang, S.Y.; Lee, J.N. The prevalence and predictors of postpartum depression. Nurs. Res. 1994, 2, 263–274. [Google Scholar] [CrossRef]
- Emons, W.H.; Meijer, R.R.; Denollet, J. Negative affectivity and social inhibition in cardiovascular disease: Evaluating type-D personality and its assessment using item response theory. J. Psychosom. Res. 2007, 63, 27–39. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cohen, S.; Williamson, G. Perceived stress in a probability sample of the United States. In The Social Psychology of Health; Spacapan, S., Oskamp, S., Eds.; Sage Publications: Thousand Oaks, CA, USA, 1988; pp. 31–66. [Google Scholar]
- Grensman, A.; Acharya, B.D.; Wändell, P.; Nilsson, G.H.; Falkenberg, T.; Sundin, Ö.; Werner, S. Effect of traditional yoga, mindfulness–based cognitive therapy, and cognitive behavioral therapy, on health related quality of life: A randomized controlled trial on patients on sick leave because of burnout. BMC Complement. Altern. Med. 2018, 18, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Kyoda, Y.; Okada, M.; Kato, R.; Matsuki, M.; Ito, N.; Takahashi, A.; Tanuma, Y.; Tachiki, H.; Fukuta, F.; Hashimoto, K. Does cognitive behavioral therapy using a self-check sheet improve night-time frequency in patients with nocturia? Results of a multicenter randomized controlled trial. Int. J. Urol. 2021, 28, 444–449. [Google Scholar] [CrossRef]
- Shatkin-Margolis, A.; White, J.; Jedlicka, A.E.; Tam, T.; Hill, A.; Yeung, J.; Crisp, C.C.; Pauls, R.N. The effect of mindfulness-based stress reduction on the urinary microbiome in interstitial cystitis. Int. Urogynecology J. 2022, 33, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. Perceived Stress Scale. Available online: https://www.northottawawellnessfoundation.org/wp-content/uploads/2018/04/PerceivedStressScale.pdf (accessed on 31 August 2022).
- Windgassen, S.; McKernan, L. Cognition, Emotion, and the Bladder: Psychosocial Factors in bladder pain syndrome and interstitial cystitis (BPS/IC). Curr. Bladder Dysfunct. Rep. 2020, 15, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Beck, J. Cognitive Behavior Therapy Basics and Beyond, 2nd ed.; The Guilford Press: New York, NY, USA, 2011; p. 391. [Google Scholar]
- Cao, R.; Yang, X.; Luo, J.; Wang, P.; Meng, F.; Xia, M.; He, Y.; Zhao, T.; Li, Z. The effects of cognitive behavioral therapy on the whole brain structural connectome in unmedicated patients with obsessive-compulsive disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 104, 110037. [Google Scholar] [CrossRef] [PubMed]
- Kairys, A.E.; Schmidt-Wilcke, T.; Puiu, T.; Ichesco, E.; Labus, J.S.; Martucci, K.; Farmer, M.A.; Ness, T.J.; Deutsch, G.; Mayer, E.A. Increased brain gray matter in the primary somatosensory cortex is associated with increased pain and mood disturbance in patients with interstitial cystitis/painful bladder syndrome. J. Urol. 2015, 193, 131–137. [Google Scholar] [CrossRef]


{kind=link}
| Patient Characteristics | Variables and Descriptions | n (%) |
|---|---|---|
| Age (years) | 53.5 ± 12.6 | |
| IC duration (years) | 9.1 ± 7.4 | |
| ICSI | 13.9 ± 4.3 | |
| ICPI | 13.1 ± 3.2 | |
| Numerical rating pain scale | 6.2 ± 2.7 | |
| Anxiety severity of BAI | 27.1 ± 8.9 | |
| Depression severity of BDI | 27.9 ± 12.7 | |
| PSS | 21.6 ± 7.1 | |
| DS14 | 31.3 ± 12.5 | |
| VUDS parameters | First sensation of filling (mL) | 117 ± 43 |
| Full sensation (mL) | 199 ± 76 | |
| Cystometric bladder capacity (mL) | 236 ± 88 | |
| Detrusor pressure (cm H2O) | 22.4 ± 19.6 | |
| Uroflowmetry | Maximum flow rate (mL/s) | 10.9 ± 4.9 |
| Voided volume (mL) | 226 ± 112 | |
| Post-void residual (mL) | 36.1 ± 72.6 | |
| Maximal bladder capacity | 766 ± 192 | |
| Glomerulation grade | 1.6 ± 0.9 | |
| Voiding dysfunction | Bladder neck dysfunction | 3 (5%) |
| Dysfunction voiding | 5 (8.3%) | |
| PRES | 7 (11.6%) | |
| Detrusor overactivity | 12 (20%) | |
| KCl test | No pain | 5 (8.3%) |
| Only pain | 47 (78.3%) | |
| Only urge | 5 (8.3%) | |
| Pain with urge | 3 (5%) | |
| CBT Group (n = 30) | BT Group (n = 30) | F | p-Value | |||
|---|---|---|---|---|---|---|
| Objective parameters | Age (years) | 53.9 ± 11.9 | 53.0 ± 13.6 | 0.776 | ||
| IC duration (years) | 9.5 ± 7.4 | 8.7 ± 7.5 | 0.699 | |||
| Current Treatment | HA instillation | 0 (0%) | 1 (3.3%) | 0.387 | ||
| BoNT-A injection | 3 (10%) | 1 (3.3%) | ||||
| PRP injection | 27 (90%) | 28 (93%) | ||||
| VUDS parameters | FSF (mL) | 113 ± 45.5 | 122 ± 40.2 | 0.414 | ||
| FS (mL) | 187 ± 83.9 | 214 ± 64.4 | 0.186 | |||
| CBC (mL) | 225 ± 98.4 | 250 ± 75.9 | 0.292 | |||
| Pdet (cm H2O) | 24.9 ± 23.3 | 19.5 ± 14.2 | 0.309 | |||
| Qmax (mL/s) | Baseline | 16.7 ± 8.8 | 15.3 ± 8.6 | 0.272 | 0.612 | |
| 8 weeks | 17.4 ± 9.5 | 17.5 ± 8 | ||||
| 12 weeks | 18.7 ± 10.5 | 16.9 ± 11.3 | ||||
| Voided volume (mL) | Baseline | 214 ± 115 | 222 ± 133 | 0.547 | 0.416 | |
| 8 weeks | 193 ± 106 | 236 ± 141 | ||||
| 12 weeks | 218 ± 126 | 234 ± 130 | ||||
| PVR (mL) | Baseline | 22.9.2 ± 23.9 | 14.5 ± 21.1 | 0.023 | 0.111 | |
| 8 weeks | 25.2 ± 36.1 | 16.8 ± 18.9 | ||||
| 12 weeks | 23.1 ± 35 | 13.2 ± 14.2 | ||||
| MBC (mL) | 772 ± 182 | 758 ± 206 | 0.786 | |||
| Glomerulation grade | 1.7 ± 1 | 1.4 ± 0.7 | 0.206 | |||
| Subjective parameters | ICSI | Baseline | 13.9 ± 3.5 | 14 ± 5.2 | 0.193 | |
| 8 weeks | 11.5 ± 4.2 | 10.5 ± 3.8 | ||||
| 12 weeks | 11 ± 3.8 | 10 ± 3.9 | ||||
| ICPI | Baseline | 13.3 ± 2.4 | 12.9 ± 4 | 0.524 | ||
| 8 weeks | 11.9 ± 3.1 | 10.5 ± 3.8 | ||||
| 12 weeks | 11 ± 3.8 | 9.9 ± 3.4 | ||||
| OSS | Baseline | 27.2 ± 5.4 | 26.9 ± 9 | 0.871 | 0.411 | |
| 8 weeks | 23.5 ± 6.8 | 22.8 ± 7.8 | ||||
| 12 weeks | 22.7 ± 7.6 | 19.9 ± 6.7 | ||||
| NRS | Baseline | 6 ± 2.2 | 6.4 ± 3.3 | 0.085 | 0.597 | |
| 8 weeks | 4.6 ± 2.4 | 5 ± 2.8 | ||||
| 12 weeks | 4.3 ± 2.2 | 4.4 ± 2.8 | ||||
| BAI | Baseline | 26.1 ± 8.2 | 28.3 ± 9.7 | 3.519 | 0.033 * | |
| 8 weeks | 18.6 ± 8.4 a | 24.4 ± 12.7 a | ||||
| 12 weeks | 14.8 ± 7.8 b.c | 22.7 ± 10.6 b.c | ||||
| BDI | Baseline | 27.6 ± 13 | 28.2 ± 12.6 | 0.097 | 0.679 | |
| 8 weeks | 21.8 ± 12.3 | 23.4 ± 11.8 | ||||
| 12 weeks | 21.2 ± 10.3 | 22.7 ± 11.6 | ||||
| GRA | 8 weeks | 1.3 ± 1.2 | 0.5 ± 1.6 | 7.161 | 0.001 * | |
| 12 weeks | 1.8 ± 0.7 | 0.5 ± 1.6 | ||||
| PPS | 22.5 ± 7 | 20.6 ± 7.2 | 0.314 | |||
| DS14 | 33.5 ± 11.7 | 28.6 ± 13.1 | 0.144 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, W.-R.; Jhang, J.-F.; Chen, B.-Y.; Ou, S.-R.; Li, H.-M.; Kuo, H.-C. Multimodal Treatment with Cognitive Behavioral Therapeutic Intervention Plus Bladder Treatment Is More Effective than Monotherapy for Patients with Interstitial Cystitis/Bladder Pain Syndrome—A Randomized Clinical Trial. J. Clin. Med. 2022, 11, 6221. https://doi.org/10.3390/jcm11206221
Yu W-R, Jhang J-F, Chen B-Y, Ou S-R, Li H-M, Kuo H-C. Multimodal Treatment with Cognitive Behavioral Therapeutic Intervention Plus Bladder Treatment Is More Effective than Monotherapy for Patients with Interstitial Cystitis/Bladder Pain Syndrome—A Randomized Clinical Trial. Journal of Clinical Medicine. 2022; 11(20):6221. https://doi.org/10.3390/jcm11206221
Chicago/Turabian StyleYu, Wan-Ru, Jia-Fong Jhang, Bai-Yueh Chen, Syuan-Ru Ou, Hao-Ming Li, and Hann-Chorng Kuo. 2022. "Multimodal Treatment with Cognitive Behavioral Therapeutic Intervention Plus Bladder Treatment Is More Effective than Monotherapy for Patients with Interstitial Cystitis/Bladder Pain Syndrome—A Randomized Clinical Trial" Journal of Clinical Medicine 11, no. 20: 6221. https://doi.org/10.3390/jcm11206221
APA StyleYu, W.-R., Jhang, J.-F., Chen, B.-Y., Ou, S.-R., Li, H.-M., & Kuo, H.-C. (2022). Multimodal Treatment with Cognitive Behavioral Therapeutic Intervention Plus Bladder Treatment Is More Effective than Monotherapy for Patients with Interstitial Cystitis/Bladder Pain Syndrome—A Randomized Clinical Trial. Journal of Clinical Medicine, 11(20), 6221. https://doi.org/10.3390/jcm11206221