
Factors Affecting Clinical over and Underestimation of Fetal Weight—A Retrospective Cohort

 , ,
, , 
Abstract
1. Introduction
2. Methods
2.1. Data Collection
- Maternal demographics and medical history (age, gravidity, parity, height, weight, body mass index (BMI, kg/m2), maternal stature (short: height <10th percentile or tall: >90th percentile), rates of obesity (BMI > 30 kg/m2), smoking, chronic hypertension, pregestational diabetes mellitus (DM), gestational diabetes mellitus (GDM) [18], prior preterm deliveries, prior first or second trimester abortions and background morbidities).
- Data at presentation, including clinical and sonographic EFW [19], premature uterine contractions, preterm or premature rupture of membranes, vaginal bleeding, placental implantation site, fetal presentation, preeclampsia or gestational hypertension diagnosed according to international guidelines [20] and rates of polyhydramnios or oligohydramnios [21].
- Delivery characteristics: GA at delivery, onset of delivery (spontaneous/induced), use of epidural anesthesia, intrapartum fever (a measurement of maternal fever ≥38 degree Celsius during delivery or up to 24 h from delivery), amniotic fluid color, fetal sex, mode of delivery (normal vaginal delivery, VE, CD), indication for VE or CD and intrapartum maternal blood loss.
- All neonates were evaluated by a pediatrician immediately after delivery, or by a neonatologist if the birthweight was <2500 g. Neonatal outcome data collected were Apgar scores, umbilical cord pH, fetal macrosomia, neonatal birthweight (small for gestational age (SGA), average for gestational age (AGA) or large for gestational age (LGA), diagnosed according to local birth weight charts [22]. Neonatal diagnoses were determined by the pediatrician at delivery and during neonatal hospitalization, according to international standards, relevant blood samples and imaging.
2.2. Ethics Approval
2.3. Statistical Analysis
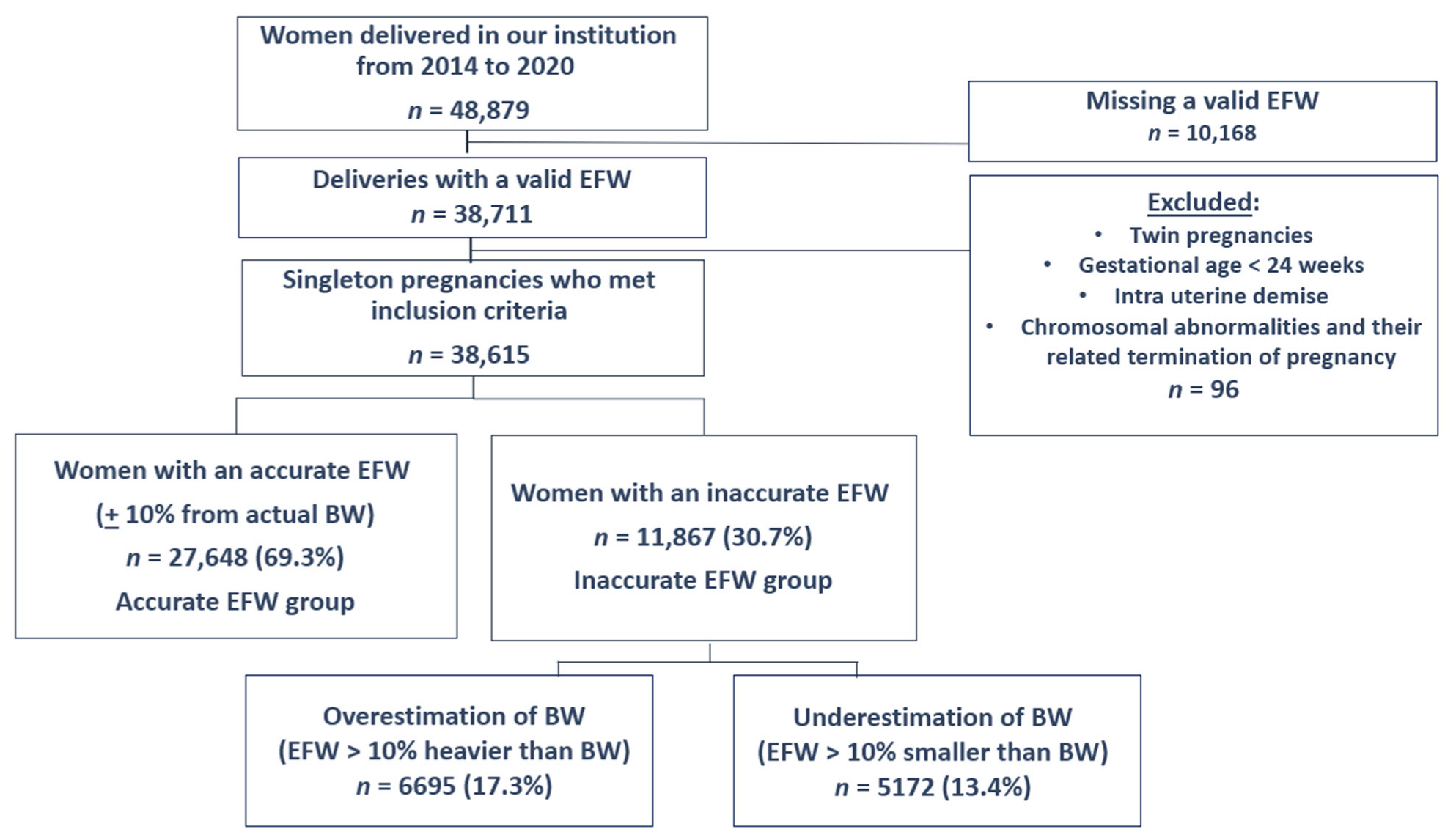
3. Results
3.1. Univariate Analysis
3.2. Multivariable Logistic Regression Analysis
3.3. Obstetric Implications of over or Underestimation
3.4. The Effect of BW Itself on EFW
3.5. Misclassification Due to over-and Underestimation of Neonatal BW
4. Discussion
4.1. Clinical Implications
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| EFW | Clinically estimated fetal birth weight |
| BW | Birth weight |
| GA | Gestational age |
| VE | Vacuum extraction |
| IOL | Induction of labor |
| CD | Cesarean delivery |
| BMI | Body mass index |
| DM | Diabetes mellitus |
| GDM | Gestational diabetes mellitus |
| SGA | Small for gestational age |
| LGA | Large for gestational age |
| Aga | Average for gestational age |
| OR | Adjusted odds ratio |
| CI | 95% confidence interval |
References
- Boulvain, M.; Senat, M.-V.; Perrotin, F.; Winer, N.; Beucher, G.; Subtil, D.; Bretelle, F.; Azria, E.; Hejaiej, D.; Vendittelli, F.; et al. Induction of labour versus expectant management for large-for-date fetuses: A randomised controlled trial. Lancet 2015, 385, 2600–2605. [Google Scholar] [CrossRef]
- Ray, E.M.; Alhusen, J.L. The Suspected Macrosomic Fetus at Term: A Clinical Dilemma. J. Midwifery Womens Health 2016, 61, 263–269. [Google Scholar] [CrossRef]
- Frick, A.P.; Syngelaki, A.; Zheng, M.; Poon, L.C.; Nicolaides, K.H. Prediction of large-for-gestational-age neonates: Screening by maternal factors and biomarkers in the three trimesters of pregnancy. Ultrasound Obstet. Gynecol. 2016, 47, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Bjørstad, A.R.; Irgens-Hansen, K.; Daltveit, A.K.; Irgens, L.M. Macrosomia: Mode of delivery and pregnancy outcome. Acta Obstet. Gynecol. Scand. 2010, 89, 664–669. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Decker, A.; Platt, R.W.; Kramer, M.S. How big is too big? The perinatal consequences of fetal macrosomia. Am. J. Obstet. Gynecol. 2008, 198, 517.e1–517.e6. [Google Scholar] [CrossRef]
- Gupta, N.; Usha Kiran, T.; Mulik, V.; Bethel, J.; Bhal, K. The incidence, risk factors and obstetric outcome in primigravid women sustaining anal sphincter tears. Acta Obstet. Gynecol. Scand. 2003, 82, 736–743. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Practice Bulletin No. 134. Obstet. Gynecol. 2013, 121, 1122–1133. [Google Scholar] [CrossRef]
- Lanowski, J.-S.; Lanowski, G.; Schippert, C.; Drinkut, K.; Hillemanns, P.; Staboulidou, I. Ultrasound versus Clinical Examination to Estimate Fetal Weight at Term. Geburtshilfe Frauenheilkd. 2017, 77, 276–283. [Google Scholar] [CrossRef]
- Joshi, A.; Panta, O.B.; Sharma, B. Estimated Fetal Weight: Comparison of Clinical Versus Ultrasound Estimate. J. Nepal Health Res. Counc. 2017, 15, 51–55. [Google Scholar] [CrossRef]
- Preyer, O.; Husslein, H.; Concin, N.; Ridder, A.; Musielak, M.; Pfeifer, C.; Oberaigner, W.; Husslein, P. Fetal weight estimation at term—Ultrasound versus clinical examination with Leopold’s manoeuvres: A prospective blinded observational study. BMC Pregnancy Childbirth 2019, 19, 122. [Google Scholar] [CrossRef]
- Daykan, Y.; Shavit, M.; Yagur, Y.; Schreiber, H.; Weitzner, O.; Schonman, R.; Biron-Shental, T.; Markovitch, O. Fetal weight estimation in tall women: Is ultrasound more accurate than clinical assessment? A prospective trial. Arch. Gynecol. Obstet. 2021, 305, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Weiner, E.; Mizrachi, Y.; Fainstein, N.; Elyashiv, O.; Mevorach-Zussman, N.; Bar, J.; Kovo, M. Comparison between Three Methods of Fetal Weight Estimation during the Active Stage of Labor Performed by Residents: A Prospective Cohort Study. Fetal Diagn. Ther. 2017, 42, 117–123. [Google Scholar] [CrossRef]
- Weiner, Z.; Ben-Shlomo, I.; Beck-Fruchter, R.; Goldberg, Y.; Shalev, E. Clinical and ultrasonographic weight estimation in large for gestational age fetus. Eur. J. Obstet. Gynecol. Reprod. Biol. 2002, 105, 20–24. [Google Scholar] [CrossRef]
- Shittu, A.S.; Kuti, O.; Orji, E.O.; Makinde, N.O.; Ogunniy, S.O.; Ayoola, O.O.; Sule, S.S. Clinical versus sonographic estimation of foetal weight in southwest Nigeria. J. Health. Popul. Nutr. 2007, 25, 14–23. [Google Scholar] [PubMed]
- Malin, G.L.; Morris, R.K.; Riley, R.; Teune, M.J.; Khan, K.S. When is birthweight at term abnormally low? A systematic review and meta-analysis of the association and predictive ability of current birthweight standards for neonatal outcomes. BJOG 2014, 121, 515–526. [Google Scholar] [CrossRef]
- Beta, J.; Khan, N.; Khalil, A.; Fiolna, M.; Ramadan, G.; Akolekar, R. Maternal and neonatal complications of fetal macrosomia: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2019, 54, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Leopold, S. Die Leitung der regelm ssigen Geburten nur durch ussere Untersuchung. Arch. Gynakol. 1894, 45, 337–368. [Google Scholar] [CrossRef]
- ACOG Practice Bulletin No. 190: Gestational Diabetes Mellitus. Obstet. Gynecol. 2018, 131, e49–e64.
- Hadlock, F.P.; Harrist, R.B.; Sharman, R.S.; Deter, R.L.; Park, S.K. Estimation of fetal weight with the use of head, body, and femur measurements—A prospective study. Am. J. Obstet. Gynecol. 1985, 151, 333–337. [Google Scholar] [CrossRef]
- Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet. Gynecol. 2013, 122, 1122–1131. [Google Scholar] [CrossRef]
- Kehl, S.; Schelkle, A.; Thomas, A.; Puhl, A.; Meqdad, K.; Tuschy, B.; Berlit, S.; Weiss, C.; Bayer, C.; Heimrich, J.; et al. Single deepest vertical pocket or amniotic fluid index as evaluation test for predicting adverse pregnancy outcome (SAFE trial): A multicenter, open-label, randomized controlled trial. Ultrasound Obstet. Gynecol. 2016, 47, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Dollberg, S.; Haklai, Z.; Mimouni, F.B.; Gorfein, I.; Gordon, E.-S. Birth weight standards in the live-born population in Israel. Isr. Med. Assoc. J. 2005, 7, 311–314. [Google Scholar] [PubMed]
- Farrell, T.; Holmes, R.; Stone, P. The effect of body mass index on three methods of fetal weight estimation. BJOG Int. J. Obstet. Gynaecol. 2002, 109, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Blitz, M.J.; Rochelson, B.; Stork, L.B.; Augustine, S.; Greenberg, M.; Sison, C.P.; Vohra, N. Effect of Maternal Body Mass Index and Amniotic Fluid Index on the Accuracy of Sonographic Estimation of Fetal Weight in Late Gestation. Am. J. Perinatol. 2018, 35, 1235–1240. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, S.P.; Lutton, P.M.; Bailey, K.J.; Guerrieri, J.P.; Morrison, J.C. Intrapartum clinical, sonographic, and parous patients’ estimates of newborn birth weight. Obstet. Gynecol. 1992, 79, 956–958. [Google Scholar] [PubMed]
- Baum, J.D.; Gussman, D.; Wirth, J.C. Clinical and patient estimation of fetal weight vs. ultrasound estimation. J. Reprod. Med. 2002, 47, 194–198. [Google Scholar] [CrossRef]
- Kesrouani, A.; Atallah, C.; AbouJaoude, R.; Assaf, N.; Khaled, H.; Attieh, E. Accuracy of clinical fetal weight estimation by Midwives. BMC Pregnancy Childbirth 2017, 17, 59. [Google Scholar] [CrossRef]
- Hill, M.G.; Cohen, W.R. Shoulder Dystocia: Prediction and Management. Women’s Health 2016, 12, 251–261. [Google Scholar] [CrossRef]
- Hill, D.A.; Lense, J.; Roepcke, F. Shoulder Dystocia: Managing an Obstetric Emergency. Am. Fam. Physician 2020, 102, 84–90. [Google Scholar]
- Wilson, A.N.; Homer, C.S.E. Third- and fourth-degree tears: A review of the current evidence for prevention and management. Aust. N. Z. J. Obstet. Gynaecol. 2020, 60, 175–182. [Google Scholar] [CrossRef]
- Tsai, L.-Y.; Chen, Y.-L.; Tsou, K.-I.; Mu, S.-C.; Taiwan Premature Infant Developmental Collaborative Study Group. The impact of small-for-gestational-age on neonatal outcome among very-low-birth-weight infants. Pediatr. Neonatol. 2015, 56, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Zafman, K.B.; Bergh, E.; Fox, N.S. Accuracy of sonographic estimated fetal weight in suspected macrosomia: The likelihood of overestimating and underestimating the true birthweight. J. Matern. Fetal. Neonatal Med. 2020, 33, 967–972. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics Practice Bulletin No. 173: Fetal Macrosomia. Obstet. Gynecol. 2016, 128, e195–e209. [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Estimated Birthweight | |||
|---|---|---|---|---|
| Overestimation (n = 6695) | Accurate (n = 27,648) | p-Value | ||
| Maternal age (years), mean + SD | 31.0 ± 5.5 | 31.0 ± 5.3 | 0.908 | |
| Gestational age at delivery (weeks), mean + SD | 38.8 ± 1.4 | 39.3 ± 1.3 | <0.001 | |
| Gestational week at delivery, per week (n, %) | <34 w | 17 (0.3%) | 44 (0.2%) | 0.125 |
| 34–36 + 6 w | 327 (4.9%) | 704 (2.6%) | <0.001 | |
| ≥37 w | 6351 (94.9%) | 26,000 (97.2%) | <0.001 | |
| ≥41 w | 657 (9.8%) | 3899 (14.6%) | <0.001 | |
| Maternal BMI, kg/m2 (mean + SD) | 24.3 ± 4.0 | 23.9 ± 3.7 | <0.001 | |
| Obesity (BMI > 30) (n, %) | 567 (16.3%) | 1670 (11.5%) | <0.001 | |
| Maternal weight gain during pregnancy, kg, (mean + SD) | 11.87 ± 5.9 | 12.26 ± 6.0 | <0.001 | |
| Maternal height, m (mean + SD) | 1.63 ± 0.05 | 1.63 ± 0.05 | <0.001 | |
| Maternal height under 10th percentile (n, %) | 624 (9.3%) | 2171 (8.1%) | 0.001 | |
| Maternal height above 90th percentile (n, %) | 554 (8.1%) | 2257 (8.4%) | 0.213 | |
| Smoker (n, %) | 540 (8.1%) | 1392 (5.2%) | <0.001 | |
| Nulliparity (n, %) | 3183 (47.5%) | 9353 (35.0%) | <0.001 | |
| Previous cesarean delivery (among multiparas (n, %)) | 634 (18.4%) | 2340 (13.5%) | <0.001 | |
| Gestational DM/DM (n, %) | 806 (12.0%) | 2926 (10.9%) | 0.011 | |
| Preeclampsia/Hypertension (n, %) | 325 (4.9%) | 741 (2.8%) | <0.001 | |
| Placental location (n, %) | Anterior | 2167 (54.6%) | 8520 (51.8%) | 0.001 |
| Posterior | 1266 (31.9%) | 5743 (34.9%) | <0.001 | |
| Previa/low lying | 11 (0.3%) | 45 (0.3%) | 0.967 | |
| Other | 522 (13.2%) | 2141 (13.0%) | 0.807 | |
| Fetal sex (n, %) | Male | 2902 (43.3%) | 13,608 (50.9%) | <0.001 |
| Female | 3793 (56.7%) | 13,140 (49.1%) | ||
| Fetal presentation (n, %) | Vertex | 6084 (97.5%) | 24,480 (98.6%) | <0.001 |
| Breech | 147 (2.4%) | 309 (1.2%) | <0.001 | |
| Transverse | 6 (0.1%) | 27 (0.1%) | 0.785 | |
| Polyhydramnios (n, %) | 34 (0.5%) | 103 (0.4%) | 0.158 | |
| Oligohydramnios (n, %) | 239 (3.6%) | 560 (2.1%) | <0.001 | |
| Neonatal birth weight, mean + SD | 2838.5 ± 330.7 | 3307.9 ± 374.4 | <0.001 | |
| Small for gestational age (n, %) | 1862 (27.8%) | 934 (3.5%) | <0.001 | |
| Large for gestational age (n, %) | 26 (0.4%) | 2084 (7.8%) | <0.001 | |
| Macrosomia (n, %) | 3 (0.0%) | 914 (3.4%) | <0.001 | |
| Umbilical cord pH < 7 (n, %) | 26 (1.2%) | 80 (1.2%) | 0.866 | |
| Umbilical cord pH < 7.1 (n, %) | 122 (5.4%) | 318 (4.8%) | 0.218 | |
| 5 min Apgar score <7 (n, %) | 22 (0.3%) | 91 (0.3%) | 0.884 | |
| Neonatal composite outcome (Including hypoglycemia, hypothermia, meconium aspiration, non-invasive ventilation, phototherapy), (n, %) | 499 (9.2%) | 1543 (6.9%) | <0.001 | |
| Estimated Neonatal Birthweight | ||||
|---|---|---|---|---|
| Variable | Underestimated (n = 5172) | Accurate (n = 27,648) | p-Value | |
| Maternal Age (years) mean + SD | 30.5 ± 5.2 | 31.0 ± 5.3 | <0.001 | |
| Gestational age at delivery (weeks) mean + SD | 39.5 ± 1.3 | 39.3 ± 1.3 | <0.001 | |
| Gestational week at delivery, per week (n, %) | <34 w | 12 (0.2%) | 44, (0.2%) | 0.288 |
| 34–36 + 6 w | 136 (2.6%) | 704 (2.6%) | 0.992 | |
| ≥37 w | 5024 (97.1%) | 26,000 (97.2%) | 0.795 | |
| ≥41 w | 968 (18.7%) | 3899 (14.6%) | <0.001 | |
| Maternal BMI, kg/m2 (mean + SD) | 23.3 ± 3.3 | 23.9 ± 3.7 | <0.001 | |
| Obesity (BMI > 30) (n, %) | 204 (7.4%) | 1670 (11.5%) | <0.001 | |
| Maternal weight gain during pregnancy, kg (mean + SD) | 12.47 ± 6.2 | 12.26 ± 6.0 | 0.021 | |
| Maternal height, m (mean + SD) | 1.63 ± 0.06 | 1.63 ± 0.05 | 0.036 | |
| Maternal height under 10th percentile (n, %) | 404 (7.8%) | 2171 (8.1%) | 0.461 | |
| Maternal height above 90th percentile (n, %) | 464 (9.0%) | 2257 (8.4%) | 0.209 | |
| Smoking (n, %) | 200 (3.9%) | 1392 (5.2%) | <0.001 | |
| Nulliparity (n, %) | 1410 (27.3%) | 9353 (35.0%) | <0.001 | |
| Previous cesarean delivery (among multiparas (n, %) | 356 (9.5%) | 2340 (13.5%) | <0.001 | |
| Gestational DM/DM (n, %) | 372 (7.2%) | 2926 (10.9%) | <0.001 | |
| PET/HTN (n, %) | 124 (2.4%) | 741 (2.8%) | 0.134 | |
| Placental location (n, %) | Anterior | 1602 (51.1%) | 8520 (51.8%) | 0.492 |
| Posterior | 1136 (36.3%) | 5743 (34.9%) | 0.148 | |
| Previa/low lying | 4 (0.1%) | 45 (0.3%) | 0.134 | |
| Other | 391 (12.5%) | 2141 (13.0%) | 0.413 | |
| Fetal sex (n, %) | Male | 3127 (60.5%) | 13,608 (50.9%) | <0.001 |
| Female | 2045 (39.5%) | 13,140 (49.1%) | ||
| Presentation (n, %) | Vertex | 4309 (98.4%) | 24,480 (98.6%) | 0.132 |
| Breech | 65 (1.4%) | 309 (1.2%) | 0.236 | |
| Transverse | 7 (0.1%) | 27 (0.1%) | 0.362 | |
| Polyhydramnios (n, %) | 14 (0.3%) | 103 (0.4%) | 0.214 | |
| Oligohydramnios (n, %) | 82 (1.6%) | 560 (2.1%) | 0.018 | |
| Neonatal birth weight, mean + SD | 3656.0 ± 400.3 | 3307.9 ± 374.4 | <0.001 | |
| SGA (n, %) | 26 (0.5%) | 934 (3.5%) | <0.001 | |
| LGA (n, %) | 1524 (29.5%) | 2084 (7.8%) | <0.001 | |
| Macrosomia (n, %) | 964 (18.6%) | 914 (3.4%) | <0.001 | |
| 3-4th degree perineal laceration (n, %) | 59 (1.1%) | 192 (0.7%) | 0.002 | |
| Failed vacuum extraction (n, %) | 22 (0.4%) | 68 (0.3%) | 0.034 | |
| Shoulder dystocia (n, %) | 70 (1.4%) | 163 (0.6%) | <0.001 | |
| Factors Associated with Overestimation of Neonatal Birthweight * | |||
|---|---|---|---|
| Adjusted Odds Ratio | 95% CI | p Value | |
| Nulliparity | 1.95 | 1.76–2.16 | <0.001 |
| Obesity (BMI > 30 kg/m2) | 1.52 | 1.33–1.74 | <0.001 |
| Short stature (Maternal height below 10th percentile) | 1.35 | 1.17–1.56 | <0.001 |
| Smoking | 1.60 | 1.33–1.93 | <0.001 |
| Hypertensive disorders | 1.30 | 1.03–1.63 | 0.027 |
| Oligohydramnios | 1.92 | 1.47–2.50 | <0.001 |
| Male fetus | 1.44 | 1.30–1.58 | <0.001 |
| Factors Associated with Underestimation of Neonatal Birthweight * | |||
| Adjusted Odds Ratio | 95% CI | p Value | |
| Gestational age (every added week) | 1.16 | 1.12–1.20 | <0.001 |
| Increased Risk for 3rd-or 4th-Degree Perineal Lacerations (Adjusted for Diabetes Mellitus, Obesity (BMI > 30 kg/m2), Fetal Macrosomia) | Adjusted Odds Ratio | 95% CI | p Value |
|---|---|---|---|
| Underestimation of fetal birthweight | 1.59 | 1.05–2.43 | 0.030 |
| Nulliparity | 3.37 | 2.37–4.80 | <0.001 |
| Increased Risk for Shoulder Dystocia (adjusted for obesity (BMI > 30 kg/m2)) | Adjusted Odds Ratio | 95% CI | p Value |
| Underestimation of fetal birthweight | 1.61 | 1.05–2.46 | 0.030 |
| Diabetes mellitus | 2.06 | 1.32–3.22 | 0.002 |
| Nulliparity | 3.37 | 2.37–4.80 | <0.001 |
| Fetal macrosomia | 5.35 | 3.45–8.32 | <0.001 |
| Increased Risk for Neonatal Composite Adverse Outcome * (adjusted for gestational age and neonatal birthweight) | Adjusted Odds Ratio | 95% CI | p Value |
| Overestimation of fetal birthweight | 1.15 | 1.02–1.30 | 0.023 |
| Nulliparity | 1.61 | 1.46–1.76 | <0.001 |
| Increased Risk for Induction of Labor | Adjusted Odds Ratio | 95% CI | p Value |
| Overestimation of fetal birthweight | 1.30 | 1.21–1.40 | <0.001 |
| Gestational age at delivery (every added week) | 1.25 | 1.22–1.28 | <0.001 |
| Nulliparity | 1.93 | 1.83–2.04 | <0.001 |
| Diabetes mellitus | 2.10 | 1.94–2.27 | <0.001 |
| Hypertensive disorders | 4.57 | 3.98–5.25 | <0.001 |
| Neonatal birthweight (every added kg) | 1.34 | 1.24–1.46 | <0.001 |
| Increased Risk for Cesarean Delivery (adjusted for hypertensive disorders and gestational age) | Adjusted Odds Ratio | 95% CI | p Value |
| Overestimation of fetal birthweight | 1.59 | 1.41–1.79 | <0.001 |
| Nulliparity | 1.78 | 1.63–1.95 | <0.001 |
| Diabetes mellitus | 1.41 | 1.24–1.60 | <0.001 |
| Maternal obesity (BMI >30 kg/m2) | 1.44 | 1.27–1.63 | <0.001 |
| Neonatal birthweight (every added kg) | 1.48 | 1.29–1.70 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cohen, G.; Shalev-Ram, H.; Schreiber, H.; Weitzner, O.; Daykan, Y.; Kovo, M.; Biron-Shental, T. Factors Affecting Clinical over and Underestimation of Fetal Weight—A Retrospective Cohort. J. Clin. Med. 2022, 11, 6760. https://doi.org/10.3390/jcm11226760
Cohen G, Shalev-Ram H, Schreiber H, Weitzner O, Daykan Y, Kovo M, Biron-Shental T. Factors Affecting Clinical over and Underestimation of Fetal Weight—A Retrospective Cohort. Journal of Clinical Medicine. 2022; 11(22):6760. https://doi.org/10.3390/jcm11226760
Chicago/Turabian StyleCohen, Gal, Hila Shalev-Ram, Hanoch Schreiber, Omer Weitzner, Yair Daykan, Michal Kovo, and Tal Biron-Shental. 2022. "Factors Affecting Clinical over and Underestimation of Fetal Weight—A Retrospective Cohort" Journal of Clinical Medicine 11, no. 22: 6760. https://doi.org/10.3390/jcm11226760
APA StyleCohen, G., Shalev-Ram, H., Schreiber, H., Weitzner, O., Daykan, Y., Kovo, M., & Biron-Shental, T. (2022). Factors Affecting Clinical over and Underestimation of Fetal Weight—A Retrospective Cohort. Journal of Clinical Medicine, 11(22), 6760. https://doi.org/10.3390/jcm11226760