



Measuring the Quality of Life in Patients with Chronic Venous Disease before and Short Term after Surgical Treatment—A Comparison between Different Open Surgical Procedures



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Quality of Life Assessment
2.3. Inclusion and Exclusion Criteria
2.4. Data Analysis
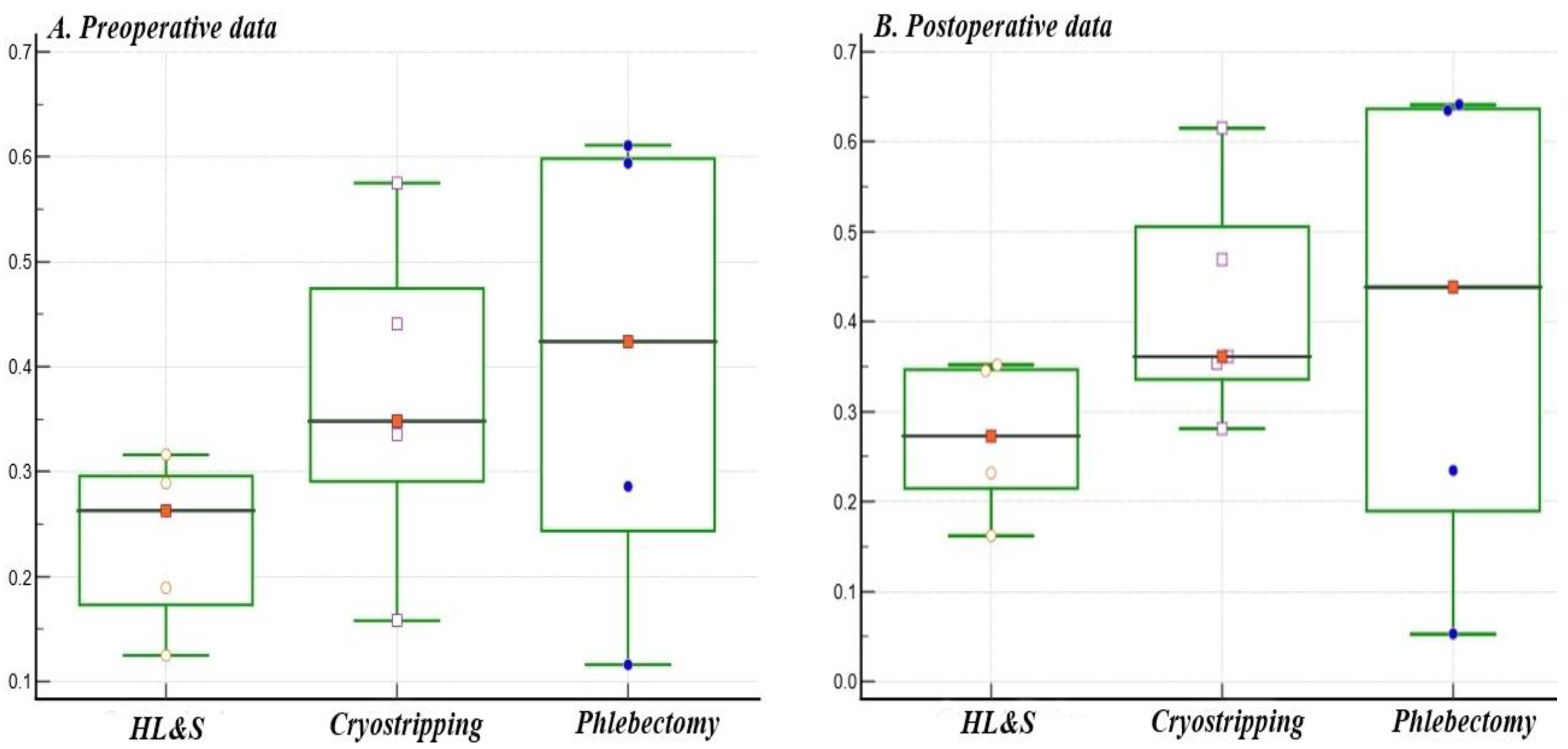
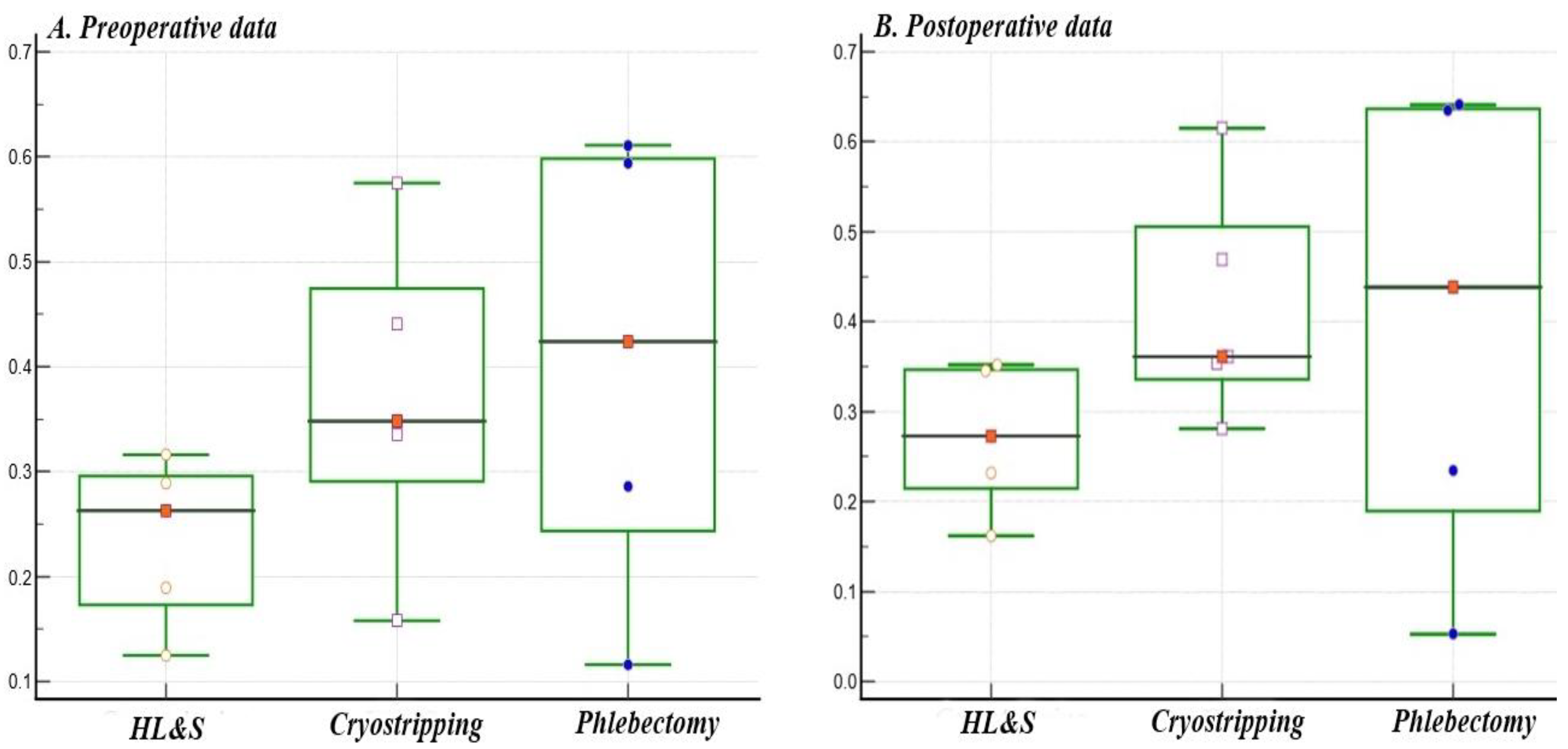
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taengsakul, T.N. Risk Factors for and Treatment of Chronic Venous Disease in Thai Patients. Vasc. Health Risk Manag. 2022, 18, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Gómez-Lahoz, A.M.; Sánchez-Trujillo, L.; Fraile-Martinez, O.; García-Montero, C.; Guijarro, L.G.; Bravo, C.; De Leon-Luis, J.A.; Saz, J.V.; Bujan, J.; et al. Chronic Venous Disease during Pregnancy Causes a Systematic Increase in Maternal and Fetal Proinflammatory Markers. Int. J. Mol. Sci. 2022, 23, 8976. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Fraile-Martínez, O.; García-Montero, C.; Álvarez-Mon, M.A.; Chaowen, C.; Ruiz-Grande, F.; Pekarek, L.; Monserrat, J.; Asúnsolo, A.; García-Honduvilla, N.; et al. Understanding Chronic Venous Disease: A Critical Overview of Its Pathophysiology and Medical Management. J. Clin. Med. 2021, 10, 3239. [Google Scholar] [CrossRef] [PubMed]
- Branisteanu, D.-E.; Feodor, T.; Baila, S.; Mitea, I.-A.; Vittos, O. Impact of chronic venous disease on quality of life: Results of vein alarm study. Exp. Ther. Med. 2018, 17, 1091–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, A.H. The Seriousness of Chronic Venous Disease: A Review of Real-World Evidence. Adv. Ther. 2019, 36 (Suppl. S1), 5–12. [Google Scholar] [CrossRef]
- Crawford, J.M.; Gasparis, A.; Amery, S.; Labropoulos, N. Treatment pattern of consecutive patients with chronic venous disease. J. Vasc. Surg. Venous Lymphat. Disord. 2018, 7, 344–348. [Google Scholar] [CrossRef]
- Almukhtar, R.M.; Goldman, M.P. Large Varicose Vein Closure: A Comprehensive Review. Dermatol. Surg. 2022, 48, 967–971. [Google Scholar] [CrossRef]
- Gao, R.-D.; Qian, S.-Y.; Wang, H.-H.; Liu, Y.-S.; Ren, S.-Y. Strategies and challenges in treatment of varicose veins and venous insufficiency. World J. Clin. Cases 2022, 10, 5946–5956. [Google Scholar] [CrossRef]
- Paravastu, S.C.V.; Horne, M.; Dodd, P.D.F. Endovenous ablation therapy (laser or radiofrequency) or foam sclerotherapy versus conventional surgical repair for short saphenous varicose veins. Cochrane Database Syst. Rev. 2016, 11, CD010878. [Google Scholar] [CrossRef]
- Menyhei, G.; Gyevnár, Z.; Arató, E.; Kelemen, O.; Kollár, L. Conventional Stripping versus Cryostripping: A Prospective Randomised Trial to Compare Improvement in Quality of Life and Complications. Eur. J. Vasc. Endovasc. Surg. 2008, 35, 218–223. [Google Scholar] [CrossRef]
- Santler, B.; Goerge, T. Chronic venous insufficiency—A review of pathophysiology, diagnosis, and treatment. JDDG J. Dtsch. Dermatol. Ges. 2017, 15, 538–556. [Google Scholar] [CrossRef] [Green Version]
- Goel, R.R.; Hardy, S.C.; Brown, T. Surgery for deep venous insufficiency. Cochrane Database Syst. Rev. 2021, 9, CD001097. [Google Scholar] [CrossRef]
- Launois, R.; Mansilha, A.; Lozano, F. Linguistic validation of the 20 item-chronic venous disease quality-of-life questionnaire (CIVIQ-20). Phlebol. J. Venous Dis. 2013, 29, 484–487. [Google Scholar] [CrossRef]
- Kersten, P.; White, P.J.; Tennant, A. Is the Pain Visual Analogue Scale Linear and Responsive to Change? An Exploration Using Rasch Analysis. PLoS ONE 2014, 9, e99485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balestroni, G.; Bertolotti, G. L’EuroQol-5D (EQ-5D): Uno strumento per la misuradellaqualitàdella vita [EuroQol-5D (EQ-5D): An instrument for measuring quality of life]. Monaldi Arch. Chest Dis. 2012, 78, 155–159. (In Italian) [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Löwe, B. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef]
- Sritharan, K.; Lane, T.; Davies, A. The Burden of Depression in Patients with Symptomatic Varicose Veins. Eur. J. Vasc. Endovasc. Surg. 2012, 43, 480–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correa Posada, M.O.; Contreras Correa, L.M.; García Vélez, J.F. Factors associated with chronic venous disease: Study in 1136 patients treated for varicose veins of the lower limbs in a specialized clinic. J Vasc Bras. 2022, 21, e20220051. [Google Scholar] [CrossRef] [PubMed]
- Rabe, E.; Pannier, F. Was istgesichert in der Therapie der chronischenVeneninsuffizienz? [What is evidence-based in the treatment of chronic venous insufficiency?]. Internist 2020, 61, 1230–1237. [Google Scholar] [CrossRef]
- Gohel, M.S.; Barwell, J.R.; Taylor, M.; Chant, T.; Foy, C.; Earnshaw, J.J.; Heather, B.P.; Mitchell, D.C.; Whyman, M.R.; Poskitt, K.R. Long term results of compression therapy alone versus compression plus surgery in chronic venous ulceration (ESCHAR): Randomised controlled trial. BMJ 2007, 335, 83. [Google Scholar] [CrossRef] [PubMed]
- Mościcka, P.; Cwajda-Białasik, J.; Szewczyk, M.T.; Jawień, A. Healing Process, Pain, and Health-Related Quality of Life in Patients with Venous Leg Ulcers Treated with Fish Collagen Gel: A 12-Week Randomized Single-Center Study. Int. J. Environ. Res. Public Health 2022, 19, 7108. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Team, V.; Qiu, Y.; Weller, C.D. Investigating quality of life instrument measurement properties for adults with active venous leg ulcers: A systematic review. Wound Repair Regen. 2022, 30, 468–486. [Google Scholar] [CrossRef]
- Murad, M.H.; Coto-Yglesias, F.; Zumaeta-Garcia, M.; Elamin, M.B.; Duggirala, M.K.; Erwin, P.J.; Montori, V.; Gloviczki, P. A systematic review and meta-analysis of the treatments of varicose veins. J. Vasc. Surg. 2011, 53 (Suppl. S5), 49S–65S. [Google Scholar] [CrossRef] [Green Version]
- Burckhardt, C.S.; Anderson, K.L. The Quality of Life Scale (QOLS): Reliability, Validity, and Utilization. Health Qual. Life Outcomes 2003, 1, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeldan, I.; Gürdal Karakelle, S.; Tosun Aydın, G.; Mustafaoğlu, R.; Ozalhas, T.; Alpagut, I. The relationship between clinical severity and outcome measures in patients with chronic venous insufficiency with or without leg ulcer. J. Tissue Viability 2021, 30, 310–316. [Google Scholar] [CrossRef]
- Dernek, B.; Adiyeke, L.; Duymus, T.M.; Aydogmus, S.; Kesiktas, F.N.; Paker, N. Efficacy of subcutaneous lidocaine injection in venous insufficiency: A prospective, randomized, controlled study, and new treatment protocol. J. Phys. Ther. Sci. 2018, 30, 748–754. [Google Scholar] [CrossRef] [Green Version]
- Quittner, A.L.; Romero, S.L.; Kimberg, C.I.; Blackwell, L.S.; Cruz, I. Chronic Illness. Encycl. Adolesc. 2011, 3, 91–99. [Google Scholar]
- Launois, R. Health-related quality-of-life scales specific for chronic venous disorders of the lower limbs. J. Vasc. Surg.Venous Lymphat. Disord. 2015, 3, 219–227.e3. [Google Scholar] [CrossRef]
- Kuet, M.-L.; Lane, T.R.; A Anwar, M.A.; Davies, A.H. Comparison of disease-specific quality of life tools in patients with chronic venous disease. Phlebology 2013, 29, 648–653. [Google Scholar] [CrossRef]
- Carpentier, P.H.; Satger, B.; Sandrin, B. Patient Education in Spa Resorts: Experience from a French National Program for Patients with Chronic Venous Insufficiency. Int. J. Environ. Res. Public Health 2022, 19, 1176. [Google Scholar] [CrossRef] [PubMed]
- Gloviczki, P.; Lawrence, P.F.; Wasan, S.M.; Meissner, M.H.; Almeida, J.; Brown, K.; Bush, R.L.; Di Iorio, M.; Fish, J.; Fukaya, E.; et al. The 2022 Society for Vascular Surgery, American Venous Forum, and American Vein and Lymphatic Society Clinical Practice Guidelines for the Management of Varicose Veins of the Lower Extremities. J. Vasc. Surg. Venous Lymphat. Disord. 2022, 7, S2213-333X(22)00417-6. [Google Scholar] [CrossRef]
- Kobata, T.; Kasamaki, Y.; Kanda, T. Personal factors and postoperative changes in the revised Venous Clinical Severity Score of varicose veins. J. Vasc. Surg. Venous Lymphat. Disord. 2022, 5, S2213-333X(22)00319-5. [Google Scholar] [CrossRef] [PubMed]
- Hannon, B.; Prizeman, G.; Madhavan, P.; O’Neill, S.; Martin, Z.; O’Callaghan, A.; Colgan, M.-P.; Canning, C.; O’Donnell, S. Ambulatory outpatient venous surgery service: An examination of patient satisfaction and experiences. Phlebology 2022, 37, 588–595. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Surgical Technique | Age | CEAP Score | Total | ||||
|---|---|---|---|---|---|---|---|
| 2 | 3 | 4 | 5 | 6 | |||
| HL&S | <40 | 10 | 21 | 1 | 0 | 0 | 32 |
| 41–55 | 2 | 12 | 2 | 0 | 3 | 19 | |
| >56 | 0 | 20 | 16 | 5 | 4 | 45 | |
| Total | 12 | 53 | 19 | 5 | 7 | 96 | |
| Cryostripping | <40 | 7 | 24 | 4 | 0 | 0 | 35 |
| 41–55 | 0 | 26 | 3 | 0 | 2 | 31 | |
| >56 | 4 | 23 | 10 | 8 | 2 | 47 | |
| Total | 11 | 73 | 17 | 8 | 4 | 113 | |
| Phlebectomy | <40 | 4 | 12 | 1 | 0 | 0 | 17 |
| 41–55 | 0 | 26 | 1 | 0 | 13 | 40 | |
| >56 | 5 | 15 | 16 | 7 | 8 | 51 | |
| Total | 9 | 53 | 18 | 7 | 21 | 108 | |
| HL&S (n = 96) | Cryostripping (n = 113) | Phlebectomy (n = 108) | |
|---|---|---|---|
| CEAP Score 2/3/4/5/6 | |||
| p-value/r | |||
| Age | p = 0.08; r = 0.270 | p = 0.0001; r = 0.464 | p = 0.0019; r = 0.296 |
| Gender | p = 0.08 | p = 0.016 | p = 0.0002 |
| QoL—preoperative data | |||
| CIVIQ-20 | p = 0.019; r = 0.289 | p = 0.001; r = 0.575 | p = 0.001; r = 0.611 |
| VAS | p = 0.049; r = 0.263 | p = 0.005; r = 0.348 | p = 0.049; r = 0.286 |
| Eq-5D | p = 0.007; r = 0.316 | p = 0.001; r = 0.441 | p = 0.001; r = 0.594 |
| PHQ-9 | p = 0.0451; r = 0.189 | p = 0.009; r = 0.335 | p = 0.001; r = 0.424 |
| GAD-7 | p = 0.011; r = 0.125 | p = 0.124; r = 0.158 | p = 0.233; r = 0.116 |
| QoL—postoperative data | |||
| CIVIQ-20 | p = 0.001; r = 0.352 | p = 0.001; r = 0.615 | p = 0.001; r = 0.635 |
| VAS | p = 0.034; r = 0.273 | p = 0.003; r = 0.361 | p = 0.038; r = 0.526 |
| Eq-5D | p = 0.002; r = 0.345 | p = 0.001; r = 0.469 | p = 0.001; r = 0.641 |
| PHQ-9 | p = 0.013; r = 0.232 | p = 0.004; r = 0.354 | p = 0.001; r = 0.438 |
| GAD-7 | p = 0.001; r = 0.162 | p = 0.045; r = 0.281 | p = 0.014; r = 0.235 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matei, S.-C.; Dumitru, C.Ș.; Radu, D. Measuring the Quality of Life in Patients with Chronic Venous Disease before and Short Term after Surgical Treatment—A Comparison between Different Open Surgical Procedures. J. Clin. Med. 2022, 11, 7171. https://doi.org/10.3390/jcm11237171
Matei S-C, Dumitru CȘ, Radu D. Measuring the Quality of Life in Patients with Chronic Venous Disease before and Short Term after Surgical Treatment—A Comparison between Different Open Surgical Procedures. Journal of Clinical Medicine. 2022; 11(23):7171. https://doi.org/10.3390/jcm11237171
Chicago/Turabian StyleMatei, Sergiu-Ciprian, Cristina Ștefania Dumitru, and Daniela Radu. 2022. "Measuring the Quality of Life in Patients with Chronic Venous Disease before and Short Term after Surgical Treatment—A Comparison between Different Open Surgical Procedures" Journal of Clinical Medicine 11, no. 23: 7171. https://doi.org/10.3390/jcm11237171
APA StyleMatei, S.-C., Dumitru, C. Ș., & Radu, D. (2022). Measuring the Quality of Life in Patients with Chronic Venous Disease before and Short Term after Surgical Treatment—A Comparison between Different Open Surgical Procedures. Journal of Clinical Medicine, 11(23), 7171. https://doi.org/10.3390/jcm11237171