
Creating Three-Dimensional Templates of Smiling and Pouting Faces for Different Sex- and Age Groups

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Analyses
2.2.1. Analysis 1, Average Face
2.2.2. Analysis 2, PCA
2.2.3. Analysis 3, SD Analysis
2.2.4. Analysis 4, Ratio Analysis
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Closed Smile
3.2.1. Average Faces, First Principal Component (PC), and Group Variation
3.2.2. Analysis of Ratios
3.3. Pouting
3.3.1. Average Faces, First Principal Component (PC), and Group Variation
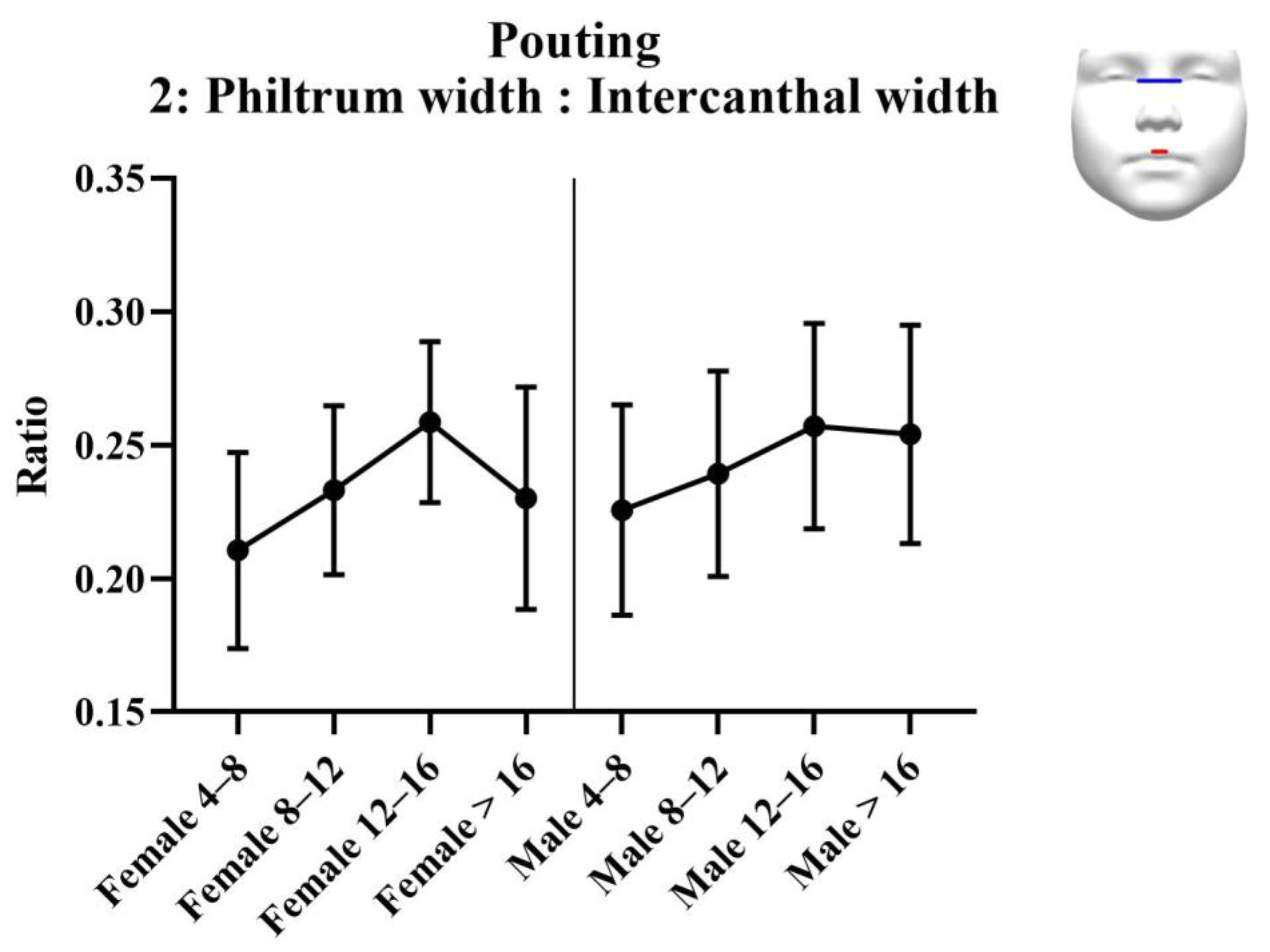
3.3.2. Analysis of Ratios
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johns, F.R.; Johnson, P.C.; Buckley, M.J.; Braun, T.W.; Close, J.M. Changes in facial movement after maxillary osteotomies. J. Oral Maxillofac. Surg. 1997, 55, 1044–1048. [Google Scholar] [CrossRef]
- Proffit, W.R.; Turvey, T.A.; Phillips, C. The hierarchy of stability and predictability in orthognathic surgery with rigid fixation: An update and extension. Head Face Med. 2007, 3, 21. [Google Scholar] [CrossRef] [Green Version]
- Busby, B.R.; Bailey, L.J.; Proffit, W.R.; Phillips, C.; White, R.P. Long-term stability of surgical class III treatment: A study of 5-year postsurgical results. Int. J. Adult Orthod. Orthognath. Surg. 2002, 17, 159–170. [Google Scholar]
- Rosenberg, A.; Muradin, M.S.M.; Van Der Bilt, A. Nasolabial esthetics after Le Fort I osteotomy and V-Y closure: A statistical evaluation. Int. J. Adult Orthod. Orthognath. Surg. 2002, 17, 29–39. [Google Scholar]
- Suckiel, J.; Kohn, M.W. Soft-tissue changes related to the surgical management of mandibular prognathism. Am. J. Orthod. 1978, 73, 676–680. [Google Scholar] [CrossRef]
- O’Ryan, F.; Schendel, S. Nasal anatomy and maxillary surgery. I. Esthetic and anatomic principles. Int. J. Adult Orthodon. Orthognath. Surg. 1989, 4, 27–37. [Google Scholar]
- O’Ryan, F.; Schendel, S. Nasal anatomy and maxillary surgery. II. Unfavorable nasolabial esthetics following the Le Fort I osteotomy. Int. J. Adult Orthodon. Orthognath. Surg. 1989, 4, 75–84. [Google Scholar]
- Betts, N.J.; Vig, K.W.; Vig, P.; Spalding, P.; Fonseca, R.J. Changes in the nasal and labial soft tissues after surgical repositioning of the maxilla. Int. J. Adult Orthod. Orthognath. Surg. 1993, 8, 7–23. [Google Scholar] [CrossRef]
- Muradin, M.S.; Seubring, K.; Stoelinga, P.J.; Bilt, A.V.; Koole, R.; Rosenberg, A.J. A Prospective Study on the Effect of Modified Alar Cinch Sutures and V-Y Closure Versus Simple Closing Sutures on Nasolabial Changes After Le Fort I Intrusion and Advancement Osteotomies. J. Oral Maxillofac. Surg. 2011, 69, 870–876. [Google Scholar] [CrossRef]
- Nooreyazdan, M.; Trotman, C.-A.; Faraway, J.J. Modeling facial movement: II. A dynamic analysis of differences caused by orthognathic surgery. J. Oral Maxillofac. Surg. 2004, 62, 1380–1386. [Google Scholar] [CrossRef] [Green Version]
- Trotman, C.-A.; Faraway, J.J. Modeling facial movement: I. A dynamic analysis of differences based on skeletal characteristics. J. Oral Maxillofac. Surg. 2004, 62, 1372–1379. [Google Scholar] [CrossRef] [PubMed]
- Al-Hiyali, A.; Ayoub, A.; Ju, X.; Almuzian, M.; Al-Anezi, T. The Impact of Orthognathic Surgery on Facial Expressions. J. Oral Maxillofac. Surg. 2015, 73, 2380–2390. [Google Scholar] [CrossRef] [PubMed]
- Ekman, P.; Friesen, W.V. Felt, false, and miserable smiles. J. Nonverbal Behav. 1982, 6, 238–252. [Google Scholar] [CrossRef]
- Frank, M.G.; Ekman, P.; Friesen, W.V. Behavioral markers and recognizability of the smile of enjoyment. J. Pers. Soc. Psychol. 1993, 64, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Krumhuber, E.; Manstead, A.S.R.; Kappas, A. Temporal Aspects of Facial Displays in Person and Expression Perception: The Effects of Smile Dynamics, Head-tilt, and Gender. J. Nonverbal Behav. 2007, 31, 39–56. [Google Scholar] [CrossRef]
- Ozono, H.; Watabe, M.; Yoshikawa, S.; Nakashima, S.; Rule, N.O.; Ambady, N.; Adams, J.R.B. What’s in a Smile? Cultural Differences in the Effects of Smiling on Judgments of Trustworthiness. Lett. Evol. Behav. Sci. 2010, 1, 15–18. [Google Scholar] [CrossRef]
- Hess, U.; Blairy, S.; Kleck, R.E. The Influence of Facial Emotion Displays, Gender, and Ethnicity on Judgments of Dominance and Affiliation. J. Nonverbal Behav. 2000, 24, 265–283. [Google Scholar] [CrossRef]
- Otta, E.; Lira, B.B.P.; Delevati, N.M.; Cesar, O.P.; Pires, C.S.G. The Effect of Smiling and of Head Tilting on Person Perception. J. Psychol. 1994, 128, 323–331. [Google Scholar] [CrossRef]
- Dong, J.K.; Jin, T.H.; Cho, H.-W.; Oh, S.C. The esthetics of the smile: A review of some recent studies. Int. J. Prosthodont. 1999, 12, 9–19. [Google Scholar]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Fortini, A.; Deregibus, A.; Debernardi, C.L. Children’s perceptions of smile esthetics and their influence on social judgment. Angle Orthod. 2016, 86, 1050–1055. [Google Scholar] [CrossRef] [Green Version]
- Hancock, P.J.B. Evolving faces from principal components. Behav. Res. Methods Instrum. Comput. 2000, 32, 327–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farkas, L.G.; Hreczko, T.; Katic, M. Anthropometric growth patterns in the nasal root and intercanthal widths of a North American Caucasian population. Anthropologie 1992, 30, 227–231. [Google Scholar]
- Sforza, C.; Grandi, G.; Catti, F.; Tommasi, D.G.; Ugolini, A.; Ferrario, V.F. Age- and sex-related changes in the soft tissues of the orbital region. Forensic Sci. Int. 2009, 185, 115.e1–115.e8. [Google Scholar] [CrossRef] [PubMed]
- Coleman, S.R.; Grover, B.R. The anatomy of the aging face: Volume loss and changes in 3-dimensional topography. Aesthetic Surg. J. 2006, 26, S4–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harkel, T.C.T.; Vinayahalingam, S.; Ingels, K.J.A.O.; Berge, S.J.; Maal, T.J.J.; Speksnijder, C.M. Reliability and Agreement of 3D Anthropometric Measurements in Facial Palsy Patients Using a Low-Cost 4D Imaging System. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1817–1824. [Google Scholar] [CrossRef]
- Fagertun, J.; Harder, S.; Rosengren, A.; Moeller, C.; Werge, T.; Paulsen, R.R.; Hansen, T.F. 3D facial landmarks: Inter-operator variability of manual annotation. BMC Med. Imaging 2014, 14, 35. [Google Scholar] [CrossRef] [PubMed]
- Baysal, A.; Sahan, A.O.; Ozturk, M.A.; Uysal, T. Reproducibility and reliability of three-dimensional soft tissue landmark identification using three-dimensional stereophotogrammetry. Angle Orthod. 2016, 86, 1004–1009. [Google Scholar] [CrossRef] [Green Version]
- Myronenko, A.; Song, X. Point Set Registration: Coherent Point Drift. IEEE Trans. Pattern Anal. Mach. Intell. 2010, 32, 2262–2275. [Google Scholar] [CrossRef] [Green Version]
- House, J.W.; Brackmann, D.E. Facial Nerve Grading System. Otolaryngol. Neck Surg. 1985, 93, 146–147. [Google Scholar] [CrossRef]
- Burres, S.; Fisch, U. The Comparison of Facial Grading Systems. Arch. Otolaryngol. Head Neck Surg. 1986, 112, 755–758. [Google Scholar] [CrossRef]
- Tomat, L.R.; Manktelow, R.T. Evaluation of a New Measurement Tool for Facial Paralysis Reconstruction. Plast. Reconstr. Surg. 2005, 115, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Trotman, C.-A.; Faraway, J.J.; Essick, G.K. Three-Dimensional Nasolabial Displacement during Movement in Repaired Cleft Lip and Palate Patients. Plast. Reconstr. Surg. 2000, 105, 1273–1283. [Google Scholar] [CrossRef] [Green Version]
- Johnston, D.J.; Millett, D.T.; Ayoub, A.F.; Bock, M. Are Facial Expressions Reproducible? Cleft Palate-Craniofac. J. 2003, 40, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Miyakawa, T.; Morinushi, T.; Yamasaki, Y. Reproducibility of a method for analysis of morphological changes in perioral soft tissue in children using video cameras. J. Oral Rehabil. 2006, 33, 202–208. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Al | Alare |
|---|---|
| ch | Cheilion |
| cph | Crista philtri |
| en | Endocanthion |
| ex | Exocanthion |
| li | Labiale inferius |
| ls | Labiale superius |
| n | Nasion |
| pg | Pogonion |
| pn | Pronasale |
| sbal | Subalare |
| sn | Subnasale |
| sto | Stomion |
| Age Group | Female (n) | Mean Age * (SD) | Male (n) | Mean Age * (SD) |
|---|---|---|---|---|
| 4–8 years | 13 | 6.4 (1.0) | 17 | 6.2 (0.7) |
| 8–12 years | 60 | 9.5 (1.1) | 58 | 9.5 (1.1) |
| 12–16 years | 17 | 12.8 (0.9) | 22 | 12.9 (1.0) |
| >16 years | 78 | 40.9 (14.0) | 63 | 45.3 (10.4) |
| Female | Female 4–8 Years (n = 13) | Female 8–12 Years (n = 60) | Female 12–16 Years (n = 17) | Female >16 Years (n = 78) |
|---|---|---|---|---|
| Ratio 1: Nose width: Intercanthal width (SD) | 0.92 (0.10) | 0.10 (0.08) | 1.01 (0.08) | 1.03 (0.12) |
| Ratio 2: Philtrum width: Intercanthal width (SD) | 0.34 (0.04) | 0.38 (0.03) | 0.39 (0.04) | 0.41 (0.05) |
| Ratio 3: Mouth width: Intercanthal width (SD) | 1.59 (0.20) | 1.70 (0.15) | 1.76 (0.19) | 1.80 (0.20) |
| Intercanthal width in mm (SD) | 33.3 (3.45) | 32.5 (2.51) | 32.6 (2.30) | 34.1 (3.41) |
| Male | Male 4–8 years (n = 17) | Male 8–12 years (n = 58) | Male 12–16 years (n = 22) | Male >16 years (n = 63) |
| Ratio 1: Nose width: Intercanthal width (SD) | 0.99 (0.08) | 1.00 (0.07) | 1.01 (0.12) | 1.12 (0.11) |
| Ratio 2: Philtrum width: Intercanthal width (SD) | 0.38 (0.04) | 0.38 (0.03) | 0.40 (0.05) | 0.44 (0.05) |
| Ratio 3: Mouth width: Intercanthal width (SD) | 1.65 (0.13) | 1.73 (0.15) | 1.74 (0.20) | 1.85 (0.20) |
| Intercanthal width in mm (SD) | 31.6 (1.84) | 33.2 (2.73) | 34.0 (3.44) | 35.0 (3.20) |
| Female | Ratio 1 Nose: ICW | Ratio 2 Phi: ICW | Ratio 3 Mouth: ICW | ICW |
|---|---|---|---|---|
| ANOVA | 0.0035 * | <0.0001 * | 0.0003 * | 0.0147 * |
| Tukey’s | ||||
| Female 4–8 vs. 8–12 | 0.0739 | 0.0367 * | 0.2034 | 0.8109 |
| Female 4–8 vs. 12–16 | 0.0630 | 0.0240 * | 0.0640 | 0.9245 |
| Female 4–8 vs. >16 | 0.0024 * | <0.0001 * | 0.0012 * | 0.8123 |
| Female 8–12 vs. 12–16 | 0.9181 | 0.8428 | 0.6558 | 0.9987 |
| Female 8–12 vs. >16 | 0.2208 | 0.0004 * | 0.0118 * | 0.0111 * |
| Female 12–16 vs. >16 | 0.9388 | 0.2940 | 0.8507 | 0.2543 |
| Male | ||||
| ANOVA | <0.0001 * | <0.0001 * | <0.0001 * | 0.0001 * |
| Tukey’s | ||||
| Male 4–8 vs. 8–12 | 0.9949 | 0.9957 | 0.3726 | 0.1813 |
| Male 4–8 vs. 12–16 | 0.9668 | 0.3701 | 0.3675 | 0.0592 |
| Male 4–8 vs. >16 | <0.0001 * | <0.0001 * | 0.0003 * | 0.0002 * |
| Male 8–12 vs. 12–16 | 0.9876 | 0.2599 | 0.9890 | 0.7343 |
| Male 8–12 vs. >16 | <0.0001 * | <0.0001 * | 0.0012 * | 0.0071 * |
| Male 12–16 vs. >16 | 0.0001 * | 0.0008 * | 0.0692 | 0.5206 |
| Female | Female 4–8 Years (n = 13) | Female 8–12 Years (n = 60) | Female 12–16 Years (n = 17) | Female >16 Years (n = 78) |
|---|---|---|---|---|
| Ratio 1: Nose width: Intercanthal width (SD) | 0.90 (0.07) | 0.91 (0.08) | 0.94 (0.10) | 0.92 (0.11) |
| Ratio 2: Philtrum width: Intercanthal width (SD) | 0.21 (0.04) | 0.23 (0.03) | 0.26 (0.03) | 0.23 (0.04) |
| Ratio 3: Mouth width: Intercanthal width (SD) | 0.92 (0.15) | 1.06 (0.14) | 1.19 (0.13) | 1.08 (0.18) |
| Intercanthal width in mm (SD) | 31.2 (2.56) | 32.5 (2.39) | 32.8 (2.55) | 34.3 (3.98) |
| Male | Male 4–8 years (n = 17) | Male 8–12 years (n = 58) | Male 12–16 years (n = 22) | Male >16 years (n = 63) |
| Ratio 1: Nose width: Intercanthal width (SD) | 0.94 (0.06) | 0.93 (0.07) | 0.94 (0.08) | 0.99 (0.11) |
| Ratio 2: Philtrum width: Intercanthal width (SD) | 0.23 (0.04) | 0.24 (0.04) | 0.26 (0.04) | 0.25 (0.04) |
| Ratio 3: Mouth width: Intercanthal width (SD) | 0.99 (0.13) | 1.09 (0.16) | 1.16 (0.14) | 1.12 (0.14) |
| Intercanthal width in mm (SD) | 30.7 (1.84) | 32.2 (2.34) | 33.2 (1.91) | 35.0 (2.78) |
| Women | Ratio 1 Nose: ICW | Ratio 2 Phi: ICW | Ratio 3 Mouth: ICW | ICW |
|---|---|---|---|---|
| ANOVA | 0.5836 | 0.0048 * | 0.0002 * | 0.0012 * |
| Tukey’s | ||||
| Female 4–8 vs. 8–12 | 0.9881 | 0.1948 | 0.0357 * | 0.5789 |
| Female 4–8 vs. 12–16 | 0.6448 | 0.0030 * | <0.0001 * | 0.5462 |
| Female 4–8 vs. > 16 | 0.8982 | 0.2935 | 0.0056 * | 0.0102 * |
| Female 8–12 vs. 12–16 | 0.6211 | 0.0617 | 0.0189 * | 0.9840 |
| Female 8–12 vs. > 16 | 0.9204 | 0.9655 | 0.7592 | 0.0081 * |
| Female 12–16 vs. > 16 | 0.8378 | 0.0231 * | 0.0815 | 0.3262 |
| Men | ||||
| ANOVA | 0.0007 * | 0.017 * | 0.0012 * | <0.0001 * |
| Tukey’s | ||||
| Male 4–8 vs. 8–12 | 0.9946 | 0.5966 | 0.0610 | 0.1198 |
| Male 4–8 vs. 12–16 | 0.9944 | 0.0699 | 0.0014 * | 0.0104 * |
| Male 4–8 vs. > 16 | 0.0799 | 0.0465 * | 0.0035 * | <0.0001 * |
| Male 8–12 vs. 12–16 | 0.9325 | 0.2770 | 0.1678 | 0.3766 |
| Male 8–12 vs. > 16 | 0.0006 * | 0.1748 | 0.4868 | <0.0001 * |
| Male 12–16 vs. > 16 | 0.0960 | 0.9891 | 0.7224 | 0.0113 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schutte, H.; Muradin, M.S.M.; Bielevelt, F.; ten Harkel, T.C.; Speksnijder, C.M.; Rosenberg, A.J.W.P. Creating Three-Dimensional Templates of Smiling and Pouting Faces for Different Sex- and Age Groups. J. Clin. Med. 2022, 11, 7257. https://doi.org/10.3390/jcm11247257
Schutte H, Muradin MSM, Bielevelt F, ten Harkel TC, Speksnijder CM, Rosenberg AJWP. Creating Three-Dimensional Templates of Smiling and Pouting Faces for Different Sex- and Age Groups. Journal of Clinical Medicine. 2022; 11(24):7257. https://doi.org/10.3390/jcm11247257
Chicago/Turabian StyleSchutte, Hilde, Marvick S. M. Muradin, Freek Bielevelt, Timen C. ten Harkel, Caroline M. Speksnijder, and Antoine J. W. P. Rosenberg. 2022. "Creating Three-Dimensional Templates of Smiling and Pouting Faces for Different Sex- and Age Groups" Journal of Clinical Medicine 11, no. 24: 7257. https://doi.org/10.3390/jcm11247257