Oral Anticoagulant Use and Appropriateness in Elderly Patients with Atrial Fibrillation in Complex Clinical Conditions: ACONVENIENCE Study

 ,
,
Abstract
:1. Introduction
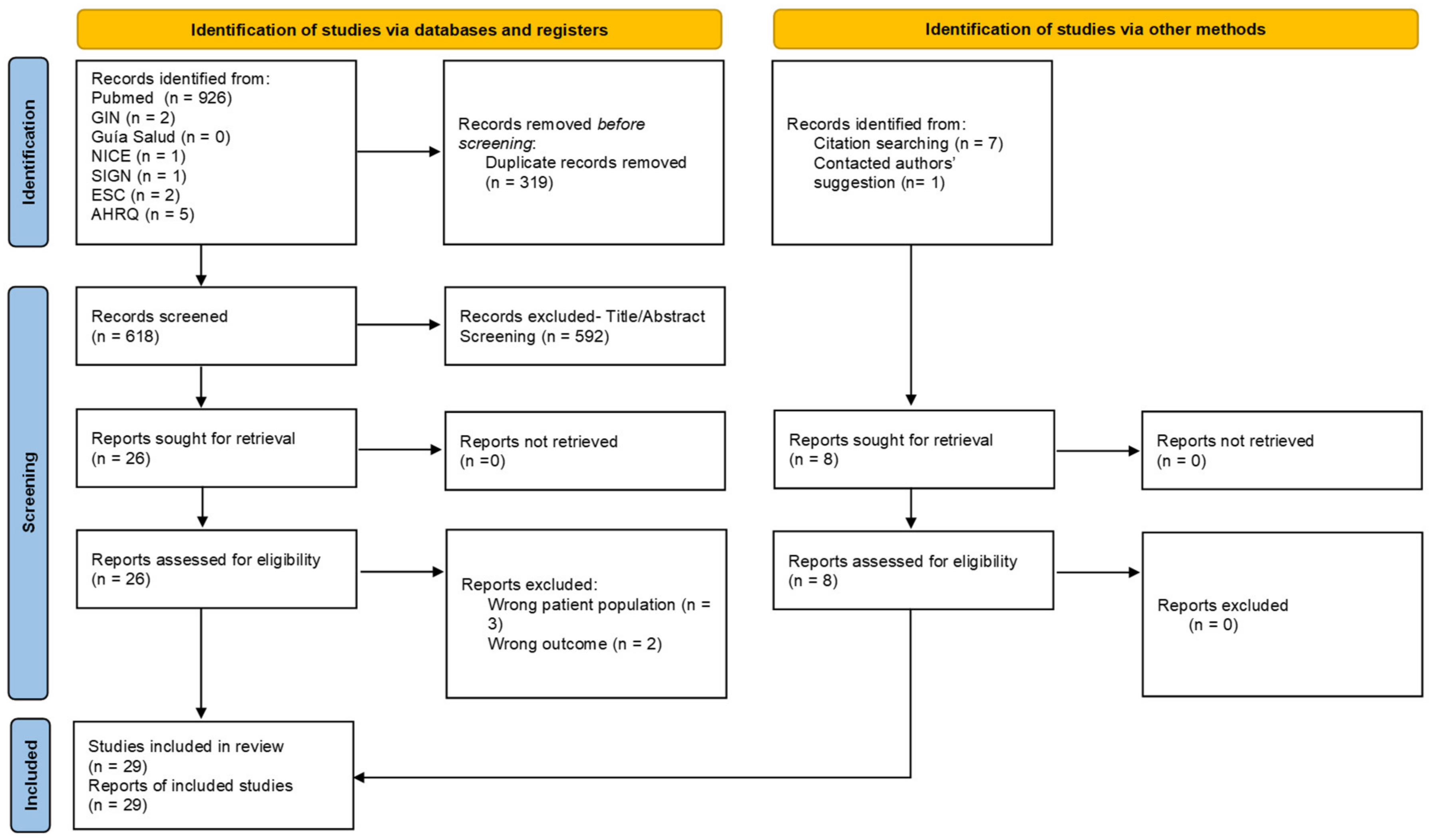
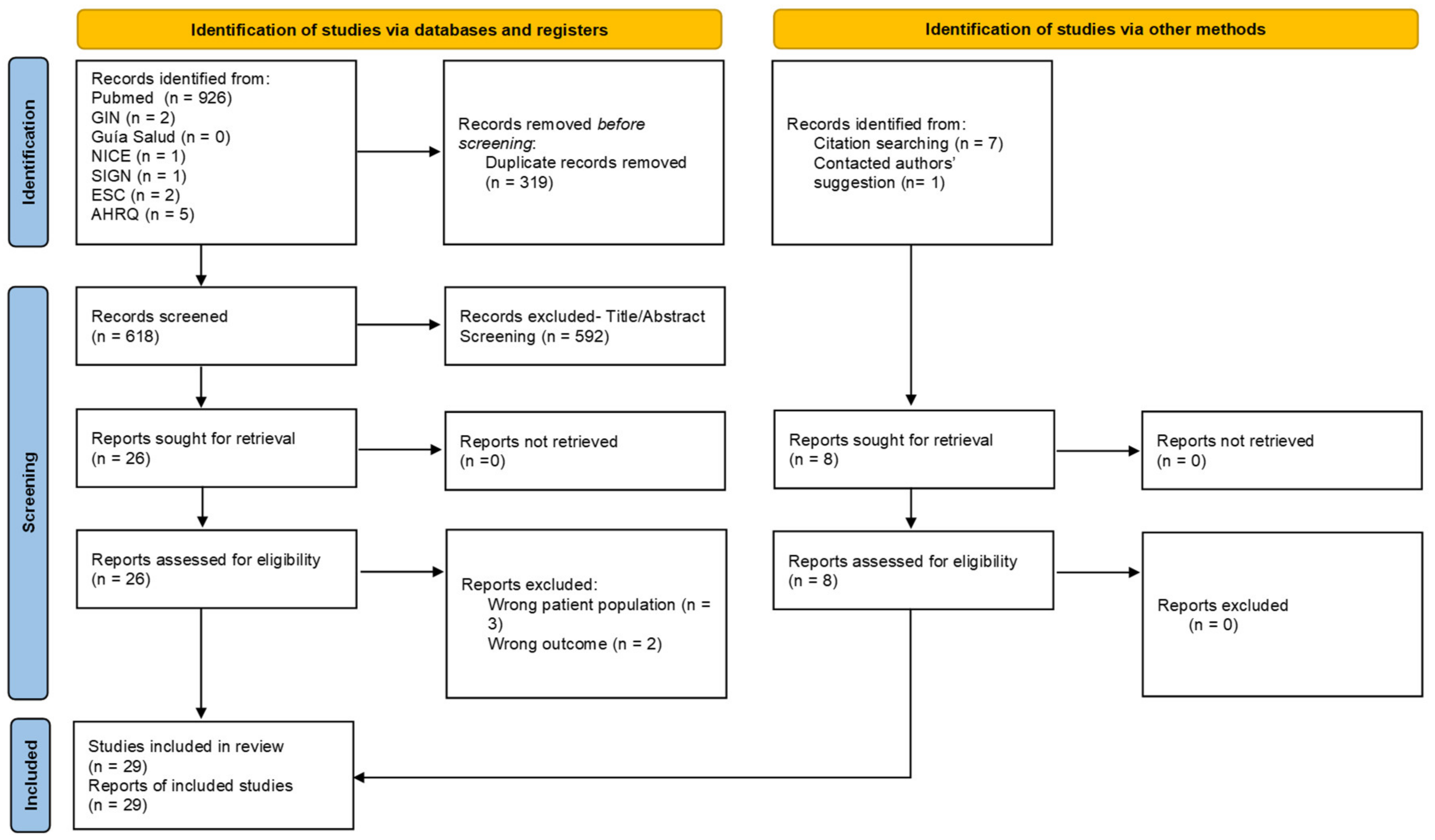
2. Materials and Methods
3. Results
3.1. Participants
3.2. Delphi Questionnaire Results
- -
- The use of DOACs, rather than VKAs, is recommended for stroke prevention in older patients with NVAF.
- -
- DOACs have a more favourable risk–benefit profile than VKAs in frail patients.
- -
- Apixaban may have a more favourable risk–benefit profile than VKAs in patients at risk of falling.
- -
- Anticoagulation should be avoided or administered with extreme caution in patients with fewer than 50,000 platelets/mL.
- -
- High risk of bleeding should not automatically prompt the withdrawal of anticoagulation before monitoring modifiable bleeding risk factors and instigating closer patient follow-up.
- -
- Polypharmacy requires greater awareness of drug interactions in patients with high bleeding risk.
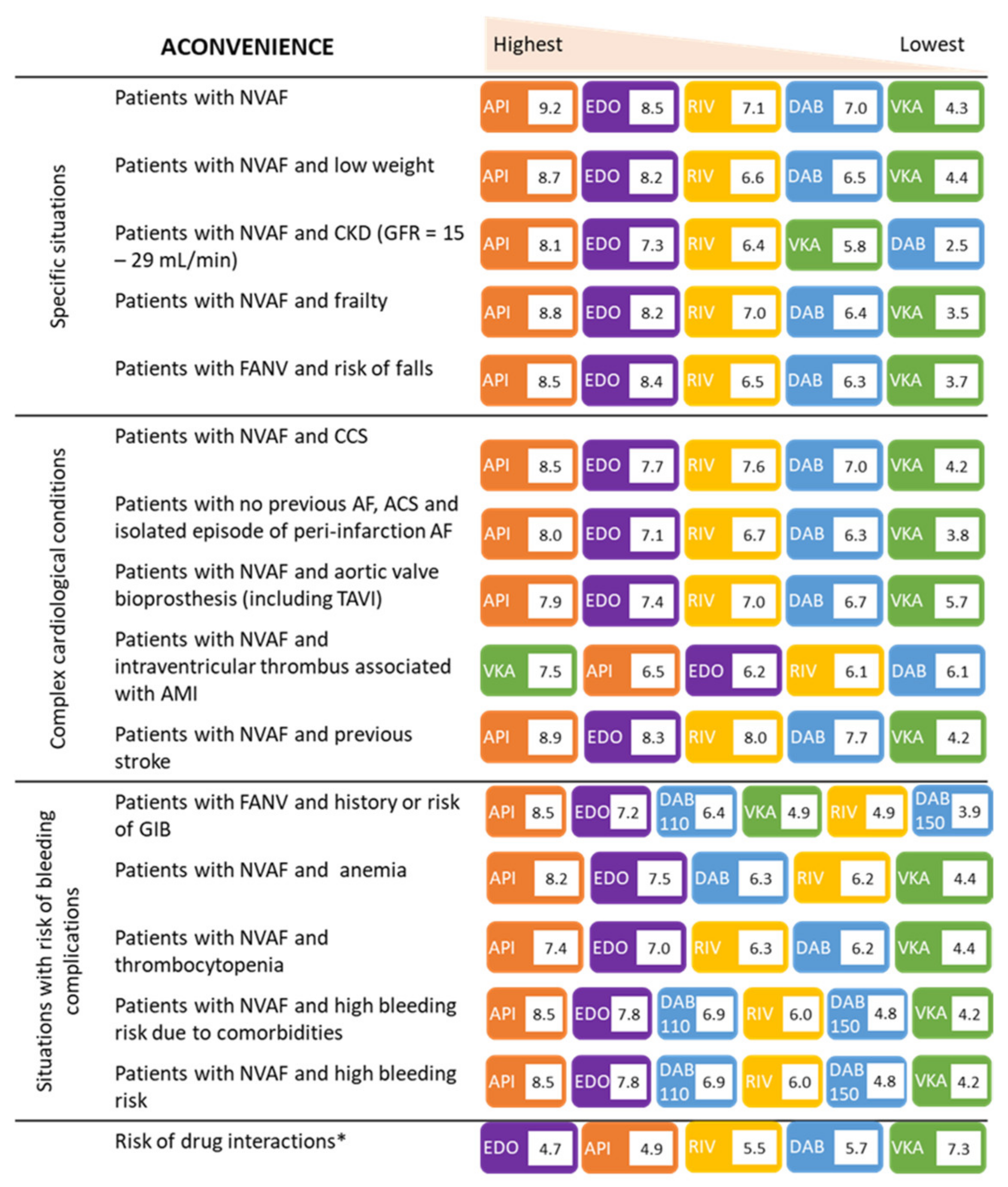
3.3. Results of the Evaluation of Therapeutic Options in the Clinical Scenarios under Consideration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Gómez-Doblas, J.J.; Muñiz, J.; Martin, J.J.A.; Rodríguez-Roca, G.; Lobos, J.M.; Awamleh, P.; Permanyer-Miralda, G.; Chorro, F.J.; Anguita, M.; Roig, E. Prevalence of Atrial Fibrillation in Spain. OFRECE Study Results. Rev. Esp. Cardiol. Engl. Ed. 2014, 67, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Villacastín, J.; Castellano, N.P.; Planas, J.M. Epidemiología de la fibrilación auricular en España en los últimos 20 años. Rev. Esp. Cardiol. 2013, 66, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Levy, D.; Vaziri, S.M.; D’Agostino, R.B.; Belanger, A.J.; Wolf, P.A. Independent Risk Factors for Atrial Fibrillation in a Population-Based Cohort: The Framingham Heart Study. JAMA 1994, 271, 840–844. [Google Scholar] [CrossRef] [PubMed]
- Marinigh, R.; Lip, G.Y.; Fiotti, N.; Giansante, C.; Lane, D.A. Age as a Risk Factor for Stroke in Atrial Fibrillation Patients: Implications for Thromboprophylaxis. J. Am. Coll. Cardiol. 2010, 56, 827–837. [Google Scholar] [CrossRef]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.; Lip, G.Y. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Caldeira, D.; Nunes-Ferreira, A.; Rodrigues, R.; Vicente, E.; Pinto, F.J.; Ferreira, J.J. Non-vitamin K antagonist oral anticoagulants in elderly patients with atrial fibrillation: A systematic review with meta-analysis and trial sequential analysis. Arch. Gerontol. Geriatr. 2019, 81, 209–214. [Google Scholar] [CrossRef]
- Biteker, M.; Başaran, Ö.; Doğan, V.; Altun, I.; Karadeniz, F.; Tekkesin, A.I.; Çakıllı, Y.; Türkkan, C.; Hamidi, M.; Demir, V.; et al. Real-World Clinical Characteristics and Treatment Patterns of Individuals Aged 80 and Older with Nonvalvular Atrial Fibrillation: Results from the ReAl-life Multicenter Survey Evaluating Stroke Study. J. Am. Geriatr. Soc. 2017, 65, 1684–1690. [Google Scholar] [CrossRef]
- Frain, B.; Castelino, R.; Bereznicki, L.R. The Utilization of Antithrombotic Therapy in Older Patients in Aged Care Facilities with Atrial Fibrillation. Clin. Appl. Thromb. 2017, 24, 519–524. [Google Scholar] [CrossRef]
- Oqab, Z.; Pournazari, P.; Sheldon, R.S. What is the Impact of Frailty on Prescription of Anticoagulation in Elderly Patients with Atrial Fibrillation? A Systematic Review and Meta-Analysis. J. Atr. Fibrillation 2018, 10, 1870. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Arrevad, P.S.; Peterson, G.; Bereznicki, L.R. Evaluation of antithrombotic usage for atrial fibrillation in aged care facilities. J. Clin. Pharm. Ther. 2011, 36, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.-P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.M.E.E.G.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grymonprez, M.; Steurbaut, S.; De Backer, T.L.; Petrovic, M.; LaHousse, L. Effectiveness and Safety of Oral Anticoagulants in Older Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2020, 11, 583311. [Google Scholar] [CrossRef] [PubMed]
- Escobar, C.; Borrás, X.; Freire, R.B.; González-Juanatey, C.; Morillas, M.; Muñoz, A.V.; Gómez-Doblas, J.J. A Delphi consensus on the management of oral anticoagulation in patients with non-valvular atrial fibrillation in Spain: ACOPREFERENCE study. PLoS ONE 2020, 15, e0231565. [Google Scholar] [CrossRef]
- Torregrossa, R.P.; Soler, P.A.; García, A.N.; Lázaro, M.G.; Rodríguez, J.G.; Gil Gregorio, P.; Martín-Sánchez, F.J.; Ruíz-Artacho, P.; Noriega, Ó.D.; Fernández, F.V. Oral anticoagulation therapy in the elderly population with atrial fibrillation: A review article. Rev. Esp. Geriatr. Gerontol. 2018, 53, 344–355. [Google Scholar] [CrossRef]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club. 1995, 123, A12. [Google Scholar] [CrossRef]
- Dalkey, N.C. The Delphi Method: An Experimental Study of Group Opinion; RAND Corp: Santa Monica, CA, USA, 1969. [Google Scholar]
- Zathar, Z.; Karunatilleke, A.; Fawzy, A.M.; Lip, G.Y.H. Atrial Fibrillation in Older People: Concepts and Controversies. Front. Med. 2019, 6, 175. [Google Scholar] [CrossRef]
- Mostaza, J.M.; Jiménez, M.J.R.; Laiglesia, F.J.R.; Peromingo, J.A.D.; Robles, M.B.; Sierra, E.G.; Bilbao, A.S.; Suárez, C. Clinical characteristics and type of antithrombotic treatment in a Spanish cohort of elderly patients with atrial fibrillation according to dependency, frailty and cognitive impairment. J. Geriatr. Cardiol. 2018, 15, 268–274. [Google Scholar] [CrossRef]
- Pugh, D.; Pugh, J.; Mead, G.E. Attitudes of physicians regarding anticoagulation for atrial fibrillation: A systematic review. Age Ageing 2011, 40, 675–683. [Google Scholar] [CrossRef]
- Steffel, J.; Verhamme, P.; Potpara, T.S.; Albaladejo, P.; Antz, M.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur. Heart J. 2018, 39, 1330–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raposeiras-Roubín, S.; Rodríguez, D.A.; Freire, S.J.C.; Abu-Assi, E.; Cobas-Paz, R.; Pascual, C.R.; Comesaña, J.G.; López, A.G.-C.; Fernández, N.C.; Ríos, Á.L.-M.; et al. Vitamin K Antagonists and Direct Oral Anticoagulants in Nonagenarian Patients with Atrial Fibrillation. J. Am. Med. Dir. Assoc. 2020, 21, 367–373.e1. [Google Scholar] [CrossRef] [PubMed]
- Patti, G.; Pecen, L.; Lucerna, M.; Huber, K.; Rohla, M.; Renda, G.; Siller-Matula, J.; Ricci, F.; Kirchhof, P.; De Caterina, R. Net Clinical Benefit of Non-Vitamin K Antagonist vs Vitamin K Antagonist Anticoagulants in Elderly Patients with Atrial Fibrillation. Am. J. Med. 2019, 132, 749–757.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fumagalli, S.; Said, S.A.; Laroche, C.; Gabbai, D.; Marchionni, N.; Boriani, G.; Maggioni, A.P.; Popescu, M.I.; Rasmussen, L.H.; Crijns, H.J.; et al. Age-Related Differences in Presentation, Treatment, and Outcome of Patients with Atrial Fibrillation in Europe: The EORP-AF General Pilot Registry (EURObservational Research Programme-Atrial Fibrilla-tion). JACC Clin. Electrophysiol. 2015, 1, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Potpara, T.S.; Simovic, S.; Pavlovic, N.; Nedeljkovic, M.; Paparisto, V.; Music, L.; Goshev, E.; Loncar, D.; Popescu, R.; Manola, S.; et al. Stroke prevention in elderly patients with non-valvular atrial fibrillation in the BALKAN-AF survey. Eur. J. Clin. Investig. 2020, 50, e13200. [Google Scholar] [CrossRef]
- Steinberg, B.A.; Shrader, P.; Pieper, K.; Thomas, L.; Allen, L.A.; Ansell, J.; Chan, P.S.; Ezekowitz, M.D.; Fonarow, G.C.; Freeman, J.V.; et al. Frequency and Outcomes of Reduced Dose Non–Vitamin K Antagonist Anticoagulants: Results From ORBIT-AF II (The Outcomes Registry for Better Informed Treatment of Atrial Fibrillation II). J. Am. Heart Assoc. 2018, 7, e007633. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, B.A.; Shrader, P.; Thomas, L.; Ansell, J.; Fonarow, G.C.; Gersh, B.J.; Kowey, P.R.; Mahaffey, K.W.; Naccarelli, G.; Reiffel, J.; et al. Off-Label Dosing of Non-Vitamin K Antagonist Oral Anticoagulants and Adverse Outcomes: The ORBIT-AF II Registry. J. Am. Coll. Cardiol. 2016, 68, 2597–2604. [Google Scholar] [CrossRef]
- Arbel, R.; Sergienko, R.; Hammerman, A.; Greenberg-Dotan, S.; Batat, E.; Avnery, O.; Ellis, M.H. Effectiveness and Safety of Off-Label Dose-Reduced Direct Oral Anticoagulants in Atrial Fibrillation. Am. J. Med. 2019, 132, 847–855.e3. [Google Scholar] [CrossRef]
- Alnsasra, H.; Haim, M.; Senderey, A.B.; Reges, O.; Leventer-Roberts, M.; Arnson, Y.; Leibowitz, M.; Hoshen, M.; Avgil-Tsadok, M. Net clinical benefit of anticoagulant treatments in elderly patients with nonvalvular atrial fibrillation: Experience from the real world. Heart Rhythm 2019, 16, 31–37. [Google Scholar] [CrossRef]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.V.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Ave-zum, A.; et al. Apixaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [Green Version]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. Edoxaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, A.H.; Yandrapalli, S.; Shetty, S.; Aronow, W.S.; Jain, D.; Frishman, W.H.; Cooper, H.A.; Panza, J.A.; on behalf of MAGIC (Meta-Analysis and Original Investigations in Cardiology) Investigators. Impact of weight on the efficacy and safety of direct-acting oral anticoagulants in patients with non-valvular atrial fibrillation: A meta-analysis. Europace 2020, 22, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Steffel, J.; Collins, R.; Antz, M.; Cornu, P.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; Rowell, N.; et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Europace 2021, 23, 1612–1676. [Google Scholar] [CrossRef]
- Wilkinson, C.; Todd, O.; Clegg, A.; Gale, C.P.; Hall, M. Management of atrial fibrillation for older people with frailty: A systematic review and meta-analysis. Age Ageing 2018, 48, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Botto, G.; Ameri, P.; Cappellari, M.; Dentali, F.; Ferri, N.; Parrini, I.; Porto, I.; Squizzato, A.; Camporese, G. Unmet Clinical Needs in Elderly Patients Receiving Direct Oral Anticoagulants for Stroke Prevention in Non-valvular Atrial Fibrillation. Adv. Ther. 2021, 38, 2891–2907. [Google Scholar] [CrossRef]
- Friberg, L.; Andersson, T.; Rosenqvist, M. Less dementia and stroke in low-risk patients with atrial fibrillation taking oral anticoagulation. Eur. Heart J. 2019, 40, 2327–2335. [Google Scholar] [CrossRef] [Green Version]
- Cheng, W.; Liu, W.; Li, B.; Li, D. Relationship of Anticoagulant Therapy with Cognitive Impairment Among Patients with Atrial Fibrillation: A Meta-Analysis and Systematic Review. J. Cardiovasc. Pharmacol. 2018, 71, 380–387. [Google Scholar] [CrossRef]
- Bezabhe, W.M.; Bereznicki, L.R.; Radford, J.; Wimmer, B.C.; Salahudeen, M.S.; Garrahy, E.; Bindoff, I.; Peterson, G.M. Oral Anticoagulant Treatment and the Risk of Dementia in Patients with Atrial Fibrillation: A Population-Based Cohort Study. J. Am. Heart Assoc. 2022, 11, e23098. [Google Scholar] [CrossRef]
- Søgaard, M.; Skjøth, F.; Jensen, M.; Kjældgaard, J.N.; Lip, G.Y.H.; Larsen, T.B.; Nielsen, P.B. Nonvitamin K Antagonist Oral Anticoagulants Versus Warfarin in Atrial Fibrillation Patients and Risk of Dementia: A Nationwide Propensity-Weighted Cohort Study. J. Am. Heart Assoc. 2019, 8, e011358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, M.P.; Vinereanu, D.; Wojdyla, D.M.; Alexander, J.H.; Atar, D.; Hylek, E.M.; Hanna, M.; Wallentin, L.; Lopes, R.D.; Gersh, B.J.; et al. Clinical Outcomes and History of Fall in Patients with Atrial Fibrillation Treated with Oral Anticoagulation: Insights from the ARISTOTLE Trial. Am. J. Med. 2018, 131, 269–275.e2. [Google Scholar] [CrossRef] [PubMed]
- Steffel, J.; Giugliano, R.P.; Braunwald, E.; Murphy, S.A.; Mercuri, M.; Choi, Y.; Aylward, P.; White, H.; Zamorano, J.L.; Antman, E.M.; et al. Edoxaban Versus Warfarin in Atrial Fibrillation Patients at Risk of Falling: EN-GAGE AF-TIMI 48 Analysis. J. Am. Coll. Cardiol. 2016, 68, 1169–1178. [Google Scholar] [CrossRef]
- Altavilla, R.; Caso, V.; Bandini, F.; Agnelli, G.; Tsivgoulis, G.; Yaghi, S.; Furie, K.L.; Tadi, P.; Becattini, C.; Zedde, M.; et al. Anticoagulation After Stroke in Patients with Atrial Fibrillation: To Bridge or Not with Low-Molecular-Weight Heparin? Stroke 2019, 50, 2093–2100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smetana, K.S.; Dunne, J.; Parrott, K.; Davis, G.A.; Collier, A.C.S.; Covell, M.; Smyth, S. Oral factor Xa inhibitors for the treatment of left ventricular thrombus: A case series. J. Thromb. Thrombolysis 2017, 44, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Mano, Y.; Koide, K.; Sukegawa, H.; Kodaira, M.; Ohki, T. Successful resolution of a left ventricular thrombus with apixaban treatment following acute myocardial infarction. Heart Vessels 2014, 31, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.A.; Wright, P.; Alizadeh, M.A.; Fhadil, S.; Rathod, K.S.; Guttmann, O.; Knight, C.; Timmis, A.; Baumbach, A.; Wragg, A.; et al. The use of novel oral anticoagulants compared to vitamin K antagonists (warfarin) in patients with left ventricular thrombus after acute myocardial infarction. Eur. Heart J.—Cardiovasc. Pharmacother. 2020, 7, 398–404. [Google Scholar] [CrossRef]
- Berry, A.; Brancheau, D.; Zughaib, M. Rapid resolution of left ventricular thrombus with apixaban therapy. SAGE Open Med. Case Rep. 2017, 5, 2050313x17745211. [Google Scholar] [CrossRef] [Green Version]
- Bass, M.E.; Kiser, T.H.; Page, R.L.; McIlvennan, C.K.; Allen, L.A.; Wright, G.; Shakowski, C. Comparative effectiveness of direct oral anticoagulants and warfarin for the treatment of left ventricular thrombus. J. Thromb. Thrombolysis 2021, 52, 517–522. [Google Scholar] [CrossRef]
- Alcalai, R.; Butnaru, A.; Moravsky, G.; Yagel, O.; Rashad, R.; Ibrahimli, M.; Planer, D.; Amir, O.; Elbaz-Greener, G.; Leibowitz, D. Apixaban vs. warfarin in patients with left ventricular thrombus: A prospective multicentre randomized clinical trial. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 8, 660–667. [Google Scholar] [CrossRef]
- Connolly, S.J.; Crowther, M.; Eikelboom, J.W.; Gibson, C.M.; Curnutte, J.T.; Lawrence, J.H.; Yue, P.; Bronson, M.D.; Lu, G.; Conley, P.B.; et al. Full Study Report of Andexanet Alfa for Bleeding Associated with Factor Xa Inhibitors. N. Engl. J. Med. 2019, 380, 1326–1335. [Google Scholar] [CrossRef] [PubMed]
- Pollack, C.V.; Reilly, P.A.; van Ryn, J.; Eikelboom, J.W.; Glund, S.; Bernstein, R.A.; Dubiel, R.; Huisman, M.V.; Hylek, E.M.; Kam, C.-W.; et al. Idarucizumab for Dabigatran Reversal—Full Cohort Analysis. N. Engl. J. Med. 2017, 377, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, J.W.; Wallentin, L.; Connolly, S.J.; Ezekowitz, M.; Healey, J.S.; Oldgren, J.; Yang, S.; Alings, M.; Kaatz, S.; Hohnloser, S.H.; et al. Risk of Bleeding With 2 Doses of Dabigatran Compared with Warfarin in Older and Younger Patients With Atrial Fibrillation: An analysis of the randomized evaluation of long-term anticoagulant therapy (RE-LY) Trial. Circulation 2011, 123, 2363–2372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, D.J.; Reichman, M.E.; Wernecke, M.; Zhang, R.; Southworth, M.R.; Levenson, M.; Sheu, T.-C.; Mott, K.; Goulding, M.R.; Houstoun, M.; et al. Cardiovascular, bleeding, and mortality risks in elderly medicare patients treated with dabigatran or warfarin for nonvalvular atrial fibrillation. Circulation 2015, 131, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Kato, E.T.; Giugliano, R.P.; Ruff, C.T.; Koretsune, Y.; Yamashita, T.; Kiss, R.G.; Nordio, F.; Murphy, S.A.; Kimura, T.; Jin, J.; et al. Efficacy and Safety of Edoxaban in Elderly Patients with Atrial Fibrillation in the ENGAGE AF–TIMI 48 Trial. J. Am. Heart Assoc. 2016, 5, e003432. [Google Scholar] [CrossRef]
- Halvorsen, S.; Atar, D.; Yang, H.; De Caterina, R.; Erol, C.; Garcia, D.; Granger, C.B.; Hanna, M.; Held, C.; Husted, S.; et al. Efficacy and safety of apixaban compared with warfarin according to age for stroke prevention in atrial fibrillation: Observations from the ARISTOTLE trial. Eur. Heart J. 2014, 35, 1864–1872. [Google Scholar] [CrossRef]
- Renda, G.; di Nicola, M.; De Caterina, R. Net Clinical Benefit of Non-vitamin K Antagonist Oral Anticoagulants Versus Warfarin in Phase III Atrial Fibrillation Trials. Am. J. Med. 2015, 128, 1007–1014.e2. [Google Scholar] [CrossRef]
- Sardar, P.; Chatterjee, S.; Chaudhari, S.; Lip, G.Y.H. New Oral Anticoagulants in Elderly Adults: Evidence from a Meta-Analysis of Randomized Trials. J. Am. Geriatr. Soc. 2014, 62, 857–864. [Google Scholar] [CrossRef]
- Lin, L.; Lim, W.S.; Zhou, H.J.; Khoo, A.L.; Tan, K.T.; Chew, A.P.; Foo, D.; Chin, J.J.; Lim, B.P. Clinical and Safety Outcomes of Oral Antithrombotics for Stroke Prevention in Atrial Fibrillation: A Systematic Review and Network Meta-analysis. J. Am. Med. Dir. Assoc. 2015, 16, 1103.e1–1103.e19. [Google Scholar] [CrossRef]
- Bonanad, C.; Esteve-Claramunt, F.; García-Blas, S.; Ayesta, A.; Díez-Villanueva, P.; Pérez-Rivera, J.; Ferreiro, J.L.; Cánoves, J.; López-Fornás, F.; Solé, A.A.; et al. Antithrombotic Therapy in Elderly Patients with Acute Coronary Syndromes. J. Clin. Med. 2022, 11, 3008. [Google Scholar] [CrossRef]
- Bonanad, C.; García-Blas, S.; Llergo, J.T.; Fernández-Olmo, R.; Díez-Villanueva, P.; Ariza-Solé, A.; Martínez-Sellés, M.; Raposeiras, S.; Ayesta, A.; Bertomeu-González, V.; et al. Direct Oral Anticoagulants versus Warfarin in Octogenarians with Nonvalvular Atrial Fibrillation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 5268. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Specialty | |
| Internal medicine | 27 (34.2) |
| Cardiology | 25 (31.6) |
| Geriatrics | 14 (17.7) |
| Neurology | 7 (8.9) |
| Haematology | 6 (7.6) |
| Workplace | |
| Private consultation | 1 (1.3) |
| Consultation in specialised centre | 1 (1.3) |
| Hospital | 77 (97.5) |
| Experience in the management of elderly patients (>75 years) with NVAF | |
| 5–9 years | 5 (6.3) |
| 10–14 years | 17 (21.5) |
| 15–19 years | 18 (22.8) |
| 20–24 years | 15 (19.0) |
| 25–29 years | 13 (16.5) |
| 30–35 years | 11 (13.9) |
| Patients seen every month | |
| <25 | (13) |
| 25–50 | (50) |
| >50 | (37) |
| No. | STATEMENT | % Agreement | Round |
|---|---|---|---|
| Block 1. Anticoagulation in the elderly patient with NVAF | |||
| 1 | In patients with NVAF, advanced age per se should not influence the anticoagulation decision. | 99% | 2nd |
| 2 | In line with current ESC guidelines, the use of DOACs, rather than VKAs, is recommended for the prevention of stroke in older patients with NVAF (except for patients with mechanical valves or moderate to severe mitral stenosis). | 100% | 1st |
| 3 | Advanced age should not be the only criterion for avoiding the full dose of anticoagulation in patients with NVAF. | 99% | 1st |
| Block 2. Impact of body weight, drug interactions, and renal function on oral anticoagulation in older patients with NVAF | |||
| 4 | There is insufficient evidence to identify a DOAC of choice for use in elderly NVAF patients with low body weight (<60 kg). The dose will be adjusted, if necessary, according to the dose reduction criteria specified in the SmPC. | 73% | 2nd |
| 5 | Interactions that may be decisive for the choice of DOAC in older patients with NVAF are:
| 97% | 1st |
| 6 | The data currently available on the use of DOAC in patients with CKD with creatinine clearance 15–30 mL/min are limited by the exclusion of these patients from clinical trials, so the compound with the greatest net clinical benefit and least disease progression cannot be identified. | 94% | 2nd |
| 7 | Rivaroxaban, edoxaban or apixaban, in adjusted doses, are a viable option for severe CKD (CrCl 15–30 mL/min). The use of dabigatran is contraindicated in these patients. | 99% | 2nd |
| Block 3. Impact of frailty, dementia, and risk of falling on oral anticoagulation in older patients with NVAF | |||
| 8 | In older patients with NVAF, frailty without a disability should not be a determinant for avoiding anticoagulants in terms of net clinical benefit. | 99% | 2nd |
| 9 | DOACs have a more favourable risk-benefit profile than VKAs in frail older patients with NVAF. | 100% | 1st |
| 10 | Cognitive impairment should not generally be a reason to avoid anticoagulation in older patients with NVAF. | 85% | 1st |
| 11 | Avoiding anticoagulation is an option in older patients with NVAF and advanced dementia, provided the patient’s primary caregiver agrees. | 96% | 2nd |
| 12 | Apixaban may have a more favourable risk-benefit profile than VKAs in older patients with NVAF and risk of falls. | 100% | 2nd |
| 13 | Edoxaban may have a more favourable risk-benefit profile than VKAs in older patients with NVAF and risk of falls. | 95% | 2nd |
| Block 4. Impact of complex cardiological conditions on oral anticoagulation in older patients with NVAF | |||
| 14 | In older patients with CCS and NVAF, antiplatelet therapy should be withdrawn 12 months after the acute event and/or coronary revascularisation, and only an anticoagulant should be continued, preferably a DOAC. | 97% | 1st |
| 15 | Older patients without previous NVAF who have ACS and develop an isolated episode of peri-infarction NVAF should receive long-term anticoagulation. | 77% | 1st |
| 16 | In older patients with NVAF and aortic valve bioprosthesis, including TAVI, the use of DOACs is a plausible alternative to VKAs. | 95% | 1st |
| 17 | In older patients with NVAF and intraventricular thrombus associated with AMI, the gold standard is VKA, due to the lack of randomised clinical trials with DOAC. However, despite this lack of evidence, the use of DOAC could be considered in very special situations. | 70% | 2nd |
| 18 | In older patients with NVAF and previous stroke, a DOAC should be preferred over a VKA. | 97% | 1st |
| Block 5. Impact of a high risk of bleeding complications on oral anticoagulation in older patients with NVAF | |||
| 19 | The use of DOAC may be associated with an increased risk of GIB compared with VKA. In older patients with NVAF and history or high risk of GIB who are candidates for DOAC treatment, the use of apixaban or dabigatran 110 mg is recommended, as a risk of GIB similar to that of warfarin has been demonstrated. | 91% | 1st |
| 20 | Treatment and correction of reversible causes and risk factors are key to minimising GIB. In patients with NVAF, the use of PPI combined with anticoagulation therapy is recommended to minimise the risk of GIB, especially in patients with a history of bleeding and/or ulcers. | 99% | 1st |
| 21 | Moderate-severe anaemia (Hb < 11 g/dL) is associated with an increased risk of bleeding complications in patients with NVAF receiving anticoagulation. However, it has not been associated with reduced antithrombotic efficacy. | 92% | 1st |
| 22 | All reversible causes of anaemia and predisposing causes (including drugs) that could increase the risk of bleeding before and during anticoagulant treatments should be investigated. | 99% | 1st |
| 23 | The use of anticoagulation in older patients with NVAF and thrombocytopenia should be performed by a multidisciplinary team, on an individualised basis, balancing the patient’s thrombotic and bleeding risk and correcting all reversible causes. | 99% | 1st |
| 24 | Anticoagulation should be avoided or used with extreme caution in patients with platelet counts below 50,000 platelets/mL. | 100% | 1st |
| 25 | DOACs appear to have a better safety and efficacy profile than VKA in patients with NVAF and thrombocytopenia. | 95% | 1st |
| 26 | A high bleeding risk due to comorbidities in older patients with NVAF is not an absolute contraindication to the use of oral anticoagulants. An individualised approach is essential. | 97% | 1st |
| 27 | A high bleeding risk should not automatically lead to the withdrawal of anticoagulants in older patients with NVAF and risk of stroke. In these patients, monitoring of all modifiable bleeding risk factors and close follow-up are essential. | 100% | 1st |
| 28 | Polypharmacy requires us to be more alert to drug interactions. | 100% | 1st |
| 29 | In older patients with NVAF and high bleeding risk, treatment with DOAC has been associated with a similar or lower risk of major bleeding, compared to VKA. | 94% | 1st |
| 30 | All DOACs are associated with a reduced risk of ICH compared with VKAs. | 90% | 1st |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonanad, C.; Formiga, F.; Anguita, M.; Petidier, R.; Gullón, A. Oral Anticoagulant Use and Appropriateness in Elderly Patients with Atrial Fibrillation in Complex Clinical Conditions: ACONVENIENCE Study. J. Clin. Med. 2022, 11, 7423. https://doi.org/10.3390/jcm11247423
Bonanad C, Formiga F, Anguita M, Petidier R, Gullón A. Oral Anticoagulant Use and Appropriateness in Elderly Patients with Atrial Fibrillation in Complex Clinical Conditions: ACONVENIENCE Study. Journal of Clinical Medicine. 2022; 11(24):7423. https://doi.org/10.3390/jcm11247423
Chicago/Turabian StyleBonanad, Clara, Francesc Formiga, Manuel Anguita, Roberto Petidier, and Alejandra Gullón. 2022. "Oral Anticoagulant Use and Appropriateness in Elderly Patients with Atrial Fibrillation in Complex Clinical Conditions: ACONVENIENCE Study" Journal of Clinical Medicine 11, no. 24: 7423. https://doi.org/10.3390/jcm11247423