1. Introduction
Epilepsy is one of the most common chronic neurological disorders, affecting more than 70 million people of all ages, races, and social status, with neurobiological, cognitive, psychological, and social consequences [
1,
2,
3]. Drug resistant epilepsy (DRE) is defined as the failure of trials of at least two appropriately chosen, administered, and tolerated anti-seizure medications (ASMs) [
4]. Surgery is an effective treatment for DRE, and includes resection, disconnection, and neuromodulation. When resection is ineffective, palliative surgery and neuromodulation therapy are advised. The efficacy and safety of VNS have been reported by many epilepsy centers [
5,
6,
7,
8]. VNS treatment has been found more effective than best medical practice (BMP) alone, with significantly improved health-related quality of life (QOL) and reduced use of hospital services in patients with DRE [
9,
10].
Many studies have focused on the efficacy and safety of VNS [
5,
6,
7,
8,
11,
12,
13]. Various epilepsy centers have reached consensus in terms of efficacy, but few studies have touched on prognostic factors in VNS treatment. Arcos et al. did not find statistical differences in the factors of “age at surgery” and “duration of epilepsy” [
14]. However, duration of epilepsy of less than 15 years and age at surgery less than 18 years were subgroups with a statistically better outcome in Colicchio et al.’s study [
15]. The assessment results of previous studies have been inconsistent about prognostic factors, due to the heterogeneity of patients.
The objective of this study was threefold: (1) to assess the clinical outcome of VNS treatment in DRE, including changes in seizure burden, QOL, and number of ASMs, (2) to discover potential prognostic factors, and (3) to summarize adverse events that occurred during follow-up.
2. Materials and Methods
2.1. Patient Data Collection
This was an observational retrospective study through medical records and interviews on the patients with DRE who underwent VNS implantation (Cybernetics, Houston, TX, USA) between November 2016 and August 2021 at the Department of Neurosurgery in The First Affiliated Hospital of Anhui Medical University. The study was approved by the Ethics Committee of The First Affiliated Hospital of Anhui Medical University (Ethics Committee Approval code: 2019H022). Informed consent was obtained from the patients (or their guardian) before collecting patient data.
Before implantation, all patients underwent a full evaluation of epilepsy surgery including magnetic resonance imaging (MRI), video-electroencephalogram (VEEG), 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) of the brain and neuropsychology. In these postoperative patients, we developed retrospective study exclusion criteria as follows: (1) incomplete seizure data; (2) follow-up duration less than 3 months; (3) patients or guardians refused the interview. Finally, a total of 45 patients were eligible for this study.
We reviewed the baseline data including demographic information, epilepsy etiology, mean monthly seizure frequency, dominant seizure type, current ASM regimen and QOL information. At specified intervals (3, 6, 12, 24, 36, 48, and 60 months), ASM regimen, VNS parameters, seizure frequency, response time, and QOL and adverse event information was recorded in the patient’s medical records, and the modified McHugh classification was used to assess seizure outcomes. QOL was assessed and quantified according to the QOLIE-31 questionnaire, with questionnaires filled by patients or their guardians. In addition, physicians were asked to rate each patient’s overall condition as better, unchanged or worse than pre-implantation. If patients had a cognitive or intellectual dysfunction or impairment, details were provided by guardians. Based on VEEG, dominant seizure types were divided into two groups, generalized and focal, and multifocal was subsumed into generalized. The etiology of epilepsy was classified according to the latest ILAE guidelines as genetic, structural, metabolic, immune, infectious, or unknown [
16]. Patients were considered as responders if they had a reduction of ≥50% in seizure frequency compared with baseline.
2.2. Device Implantation and Settings
All surgical procedures were performed at the Epilepsy Center of The First Affiliated Hospital of Anhui Medical University. Bipolar electrodes were placed around the left vagus nerve and connected to a programmable pulse generator, which was implanted subcutaneously below the collarbone.
Stimulation started 2 weeks after implantation, with an output current of 0.25 mA, frequency 30 Hz, on-time 30 s and off-time 5 min as the initial parameters, with magnet stimulation on demand (0.25 mA higher than device output current). Depending on patient’s toleration, the output current was increased in increments of 0.25–0.5 mA, eventually reaching the maximum intensity of 2.5 mA.
2.3. Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD), and categorical variables were presented as frequencies. The Student’s paired t-test was used for statistical comparison of continuous variables. Fisher’s exact test was used for the comparison of categorical variables. We identified the optimal cutoff value of pre-implantation number of ASMs using receiver operating characteristic (ROC) analysis to convert continuous variables to categorical variables, and stratified patients based on the following potential prognostic factors:
Age of onset of epilepsy: 1–51 years old;
Age at implant: 5–54 years old;
Duration of epilepsy prior to VNS: 0.25–39 years;
Gender: female (n = 15), male (n = 30);
Pre-implantation number of ASMs: ≥3 (n = 24), =2 (n = 21);
Dominant seizure type: generalized (n = 28) and focal (n = 17).
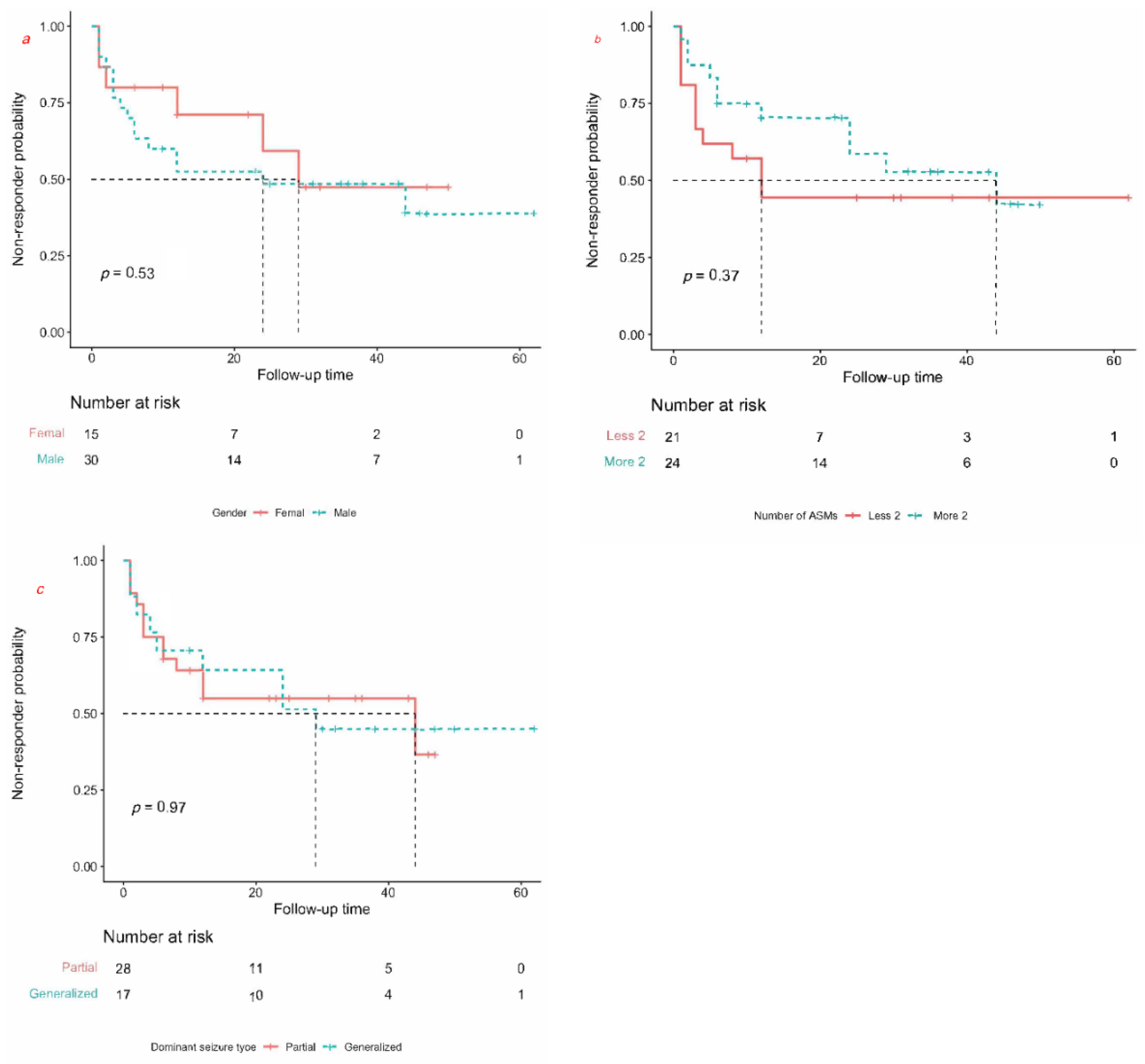
Different non-responder rates (lower non-responder rate means higher responder rate) were shown based on a log rank test and Cox proportional hazards regression for hazard ratios, and were visualized via Kaplan–Meier curves.
Differences were considered significant at a bilateral p < 0.05. Statistical analyses were conducted using the freely accessible statistical program R (version 4.1.2).
4. Discussion
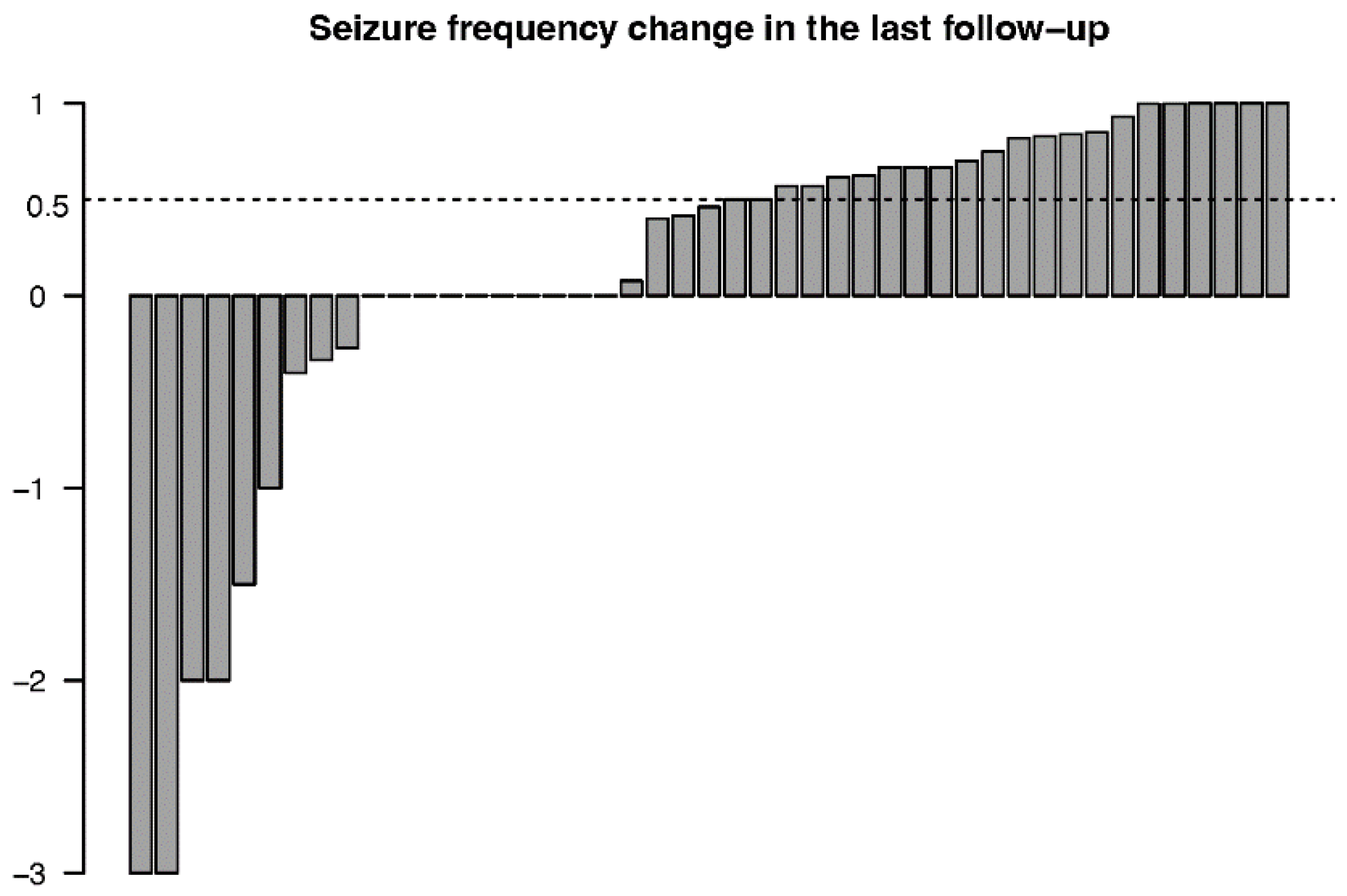
In this study we reported on the efficacy and safety of VNS for 45 consecutive patients with DRE, 5–62 months after implantation. Nearly half (48.9%) of the patients had a decrease in overall seizure frequency, rising to over 50% at the final follow-up, and four of them (8.9%) became seizure-free. The results indicated a cumulative effect of VNS, with the responder rate increasing (from 15.6% to 48.9%) as the period of stimulation extended. Monthly seizure frequency decreased 24.2% after 3 months of stimulation and 70.3% after 60 months of stimulation compared with baseline. Our recent meta-analysis, which featured 5223 pediatric and adult patients, also confirmed the efficacy of VNS. Overall responder rates at 3, 6, 12, 24, 36, 48, and 60 months postoperatively were 42.1%, 45.5%, 40.1%, 45.1%, 48.2%, 50.2%, and 50.8%, respectively, demonstrating a tendency of increasing effectiveness with the extension of duration of stimulation [
17]. Hence, we assumed that the duration of follow-up was associated with seizure reduction.
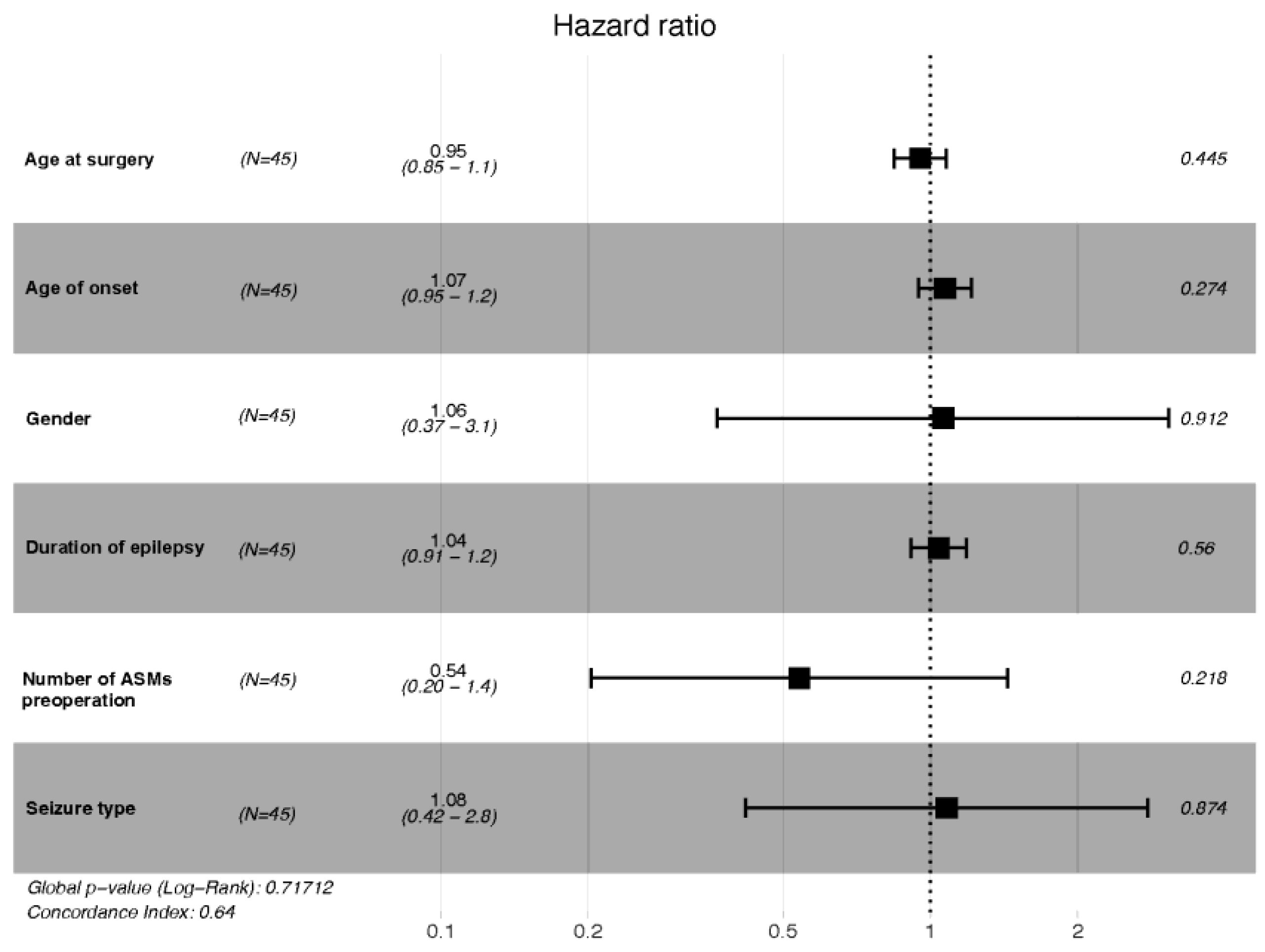
To date, there has been no conclusive evidence on prognostic factors for VNS, so we established a Cox proportional hazard ratio regression model to provide convincing results. We performed analysis of Kaplan–Meier curves to ascertain the non-responder rates among groups. We found no significant categorical prognostic factors associated with better clinical outcome. Then we conducted a Cox regression analysis (including six preselected variates) using a stepwise procedure and found that neither the duration of epilepsy, the age at onset, nor the age at surgery had an effect on clinical outcome. It is noted that there was no positive association between shorter duration of epilepsy and better response to VNS for our cohort (
p = 0.519, LR-test). Consistent with our study findings, a shorter duration of epilepsy was not associated with a better response to VNS treatment in a cohort of 70 patients with DRE [
18]. However, a meta-analysis conducted by Wang et al. found that shorter duration of epilepsy was associated with a favorable outcome for patients with DRE [
19].
Age at onset (
p = 0.180, LR-test) and age at surgery (
p = 0.380, LR-test), also as continuous variables, were not found to be associated with prognosis. Consistent with our study, Wang et al. supposed that age at seizure onset had no significant statistical association with a favorable outcome [
19]. However, in a meta-analysis that recruited 5554 patients from the VNS therapy Patient Outcome Registry and 78 clinical studies, the authors found that patients with age of epilepsy onset >12 years were more likely to be seizure-free than the younger patients, by multivariate analysis (OR, 1.89; 95% CI, 1.01–1.85) [
20]. Xu et al. using a generalized linear mixed-effect model, found that earlier onset age (OR, 1.11; 95% CI, 1.06–1.16) and shorter duration of epilepsy (OR, 1.04; 95% CI, 1.00–1.07) presented a favorable clinical outcome [
21].
Notably, there were no significant differences in dominant seizure type, gender, age at VNS implantation, and number of ASMs in our cohort. In terms of detailed etiology, we also found no significant prognostic factors. The detailed adjust hazard ratios of six variates are presented in
Table 5. The detailed etiologies in our study were classified as post-traumatic in six patients, whose seizure frequency was 10.3 ± 5.5 per month at baseline and 0.79 ± 0.78 per month at the final follow-up, a decrease of 92.3%, and five of the post-traumatic patients were responders. Consistent with our study, a previous meta-analysis identified 74 clinical studies presenting significant benefits from VNS in post-traumatic epilepsy (a 79% reduction in seizures) [
22]. This leads us to believe that VNS has a better effect on epilepsy related to brain trauma, despite a lack of significant statistical difference at the final follow-up. We also found no statistical differences for other etiologies. Meanwhile, no significant differences were observed between focal and generalized EEG outcomes in our cohort. Arcos et al. performed an observational retrospective study that enrolled 40 patients with DRE and found no significant difference between focal and generalized epilepsy at the last revision (
p = 1) [
14]. As with Arcos et al., Englot et al. found that seizure type was not a predictive factor [
20].
In our study, the improvements in QOL were more pronounced among children than adults. In addition, eight of the 19 patients with unalleviated seizures showed subjective improvement in QOL. These results were somewhat subjective in that they were based entirely on reports from medical records that were based on interviews with parents or caregivers, rather than on standard criteria. Nonetheless, the reported improvement in QOL suggests that VNS treatment may have a meaningful impact on QOL in patients with VNS, independent of a reduction in seizures. The PuLsE study confirmed that VNS plus BMP was highly associated with a significant improvement in QOL compared with BMP alone [
23].
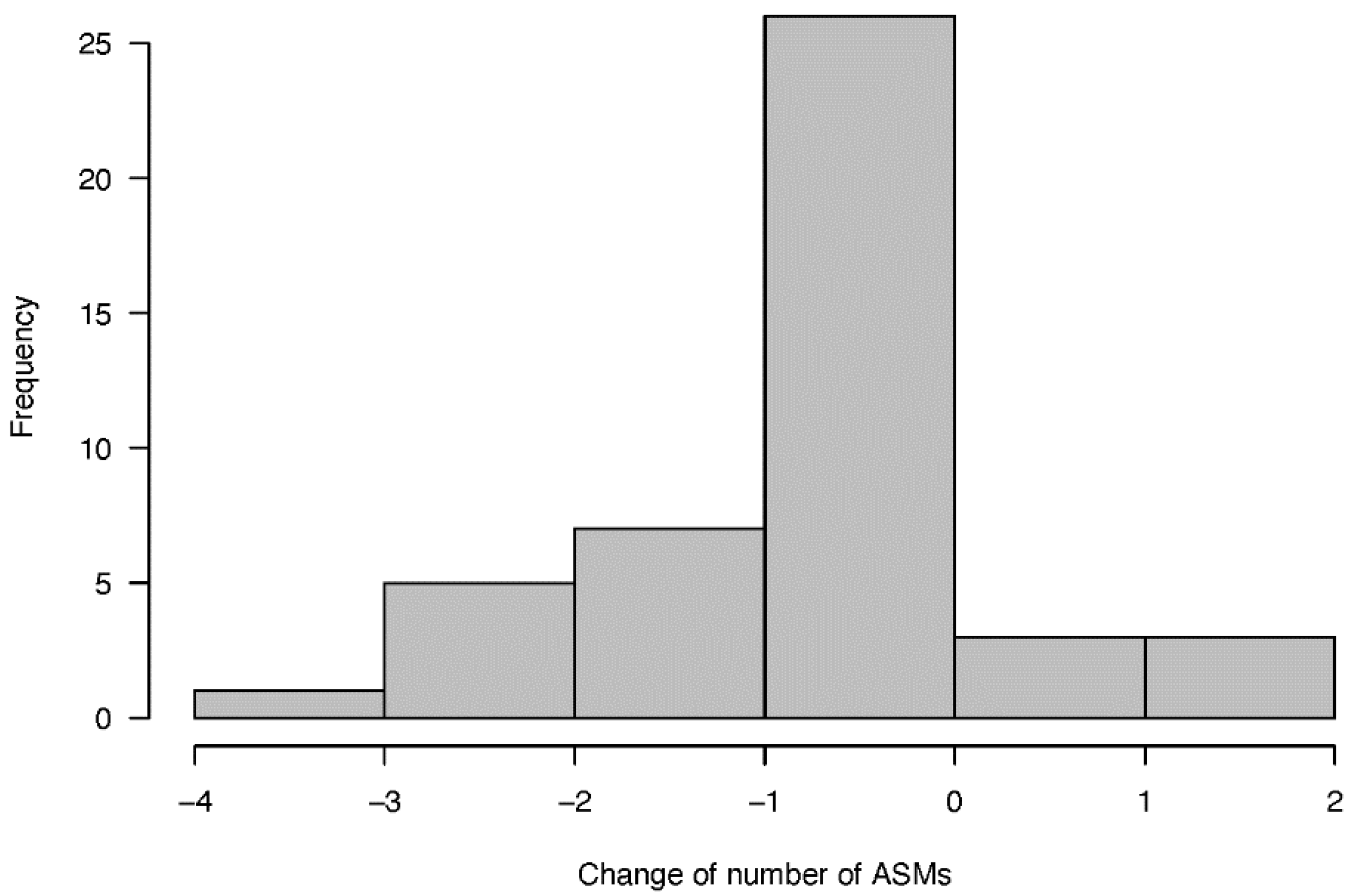
In general, we did not find a statistically significant reduction in the number of ASMs that patients with DRE were taking. Thirteen patients had varying degrees of reduction in number of ASMs during the follow-up period. Only one patient discontinued all ASMs, with this response occurring at 29 months post-implant. This result was consistent with previous uncontrolled studies, and the reduction of seizure frequency may be attributed to long-term VNS and ASM interactions [
24,
25].
No severe or life-threatening adverse events were observed in our study. Nearly half of the patients experienced adverse reactions after surgery, the most common being hoarseness (22.2%), discomfort at the surgical site (11.1%), and coughing (8.9%). Most adverse events were transient and frequently included hoarseness and/or coughing during the “on” period. One patient in our series had the stimulator removed because it was ineffective.
This study had several limitations. First, it was a single center retrospective study and thus subject to the limitations of single center and retrospective approaches. Second, we recruited more males (30/15), and thus a gender bias may have been present, although as far as we know gender does not affect the efficacy of VNS [
26]. Finally, the small sample size was a limitation. Hence, the results need to be further verified by future large prospective studies.

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}