
CT Enterography for Preoperative Evaluation of Peritoneal Carcinomatosis Index in Advanced Ovarian Cancer

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
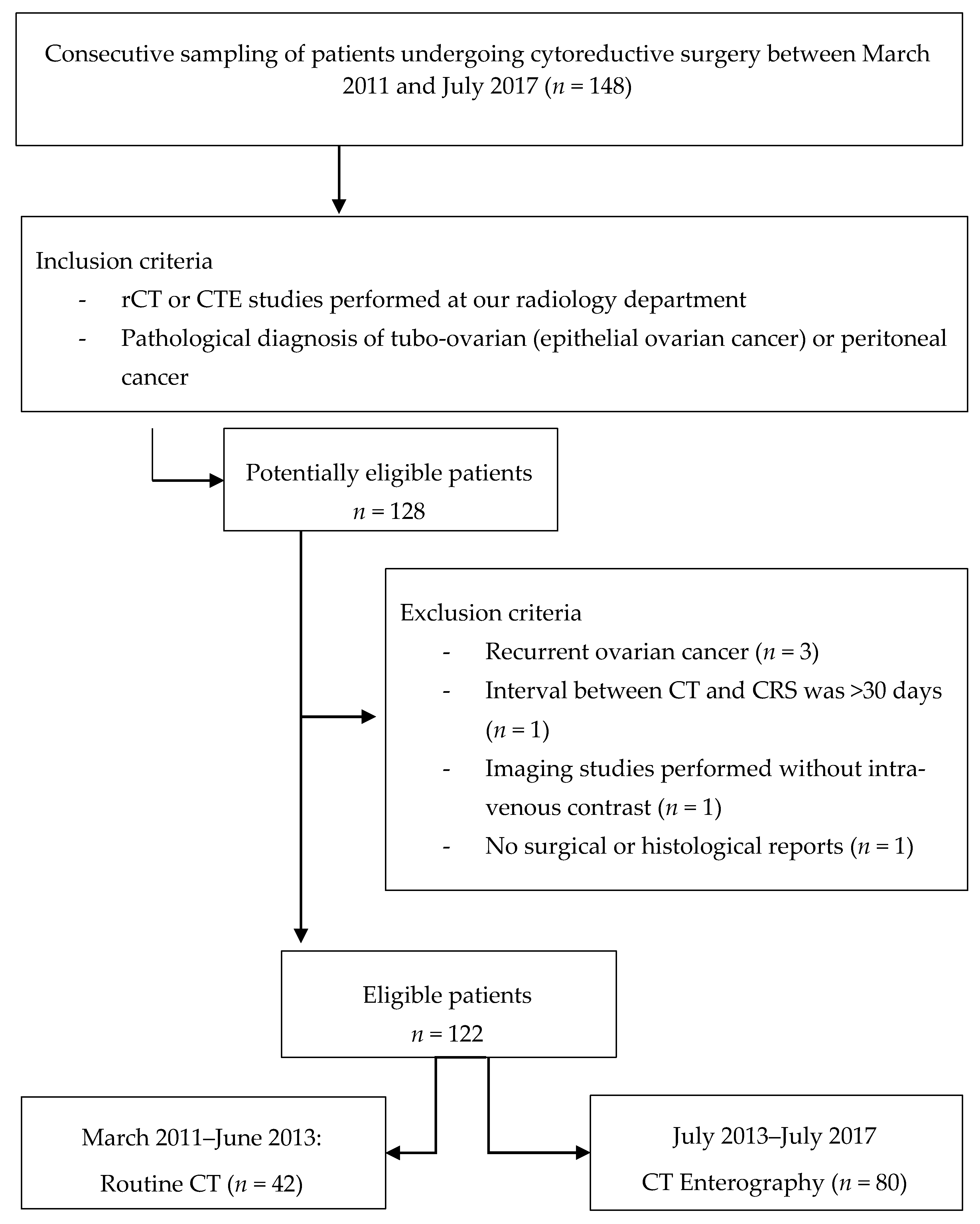
2.1. Participants
2.2. Disease Measurement: Assessment of the Peritoneal Carcinomatosis Index (PCI)
2.3. Pre-Surgical Radiological Assessment: CT Study Protocols
2.3.1. Routine CT (rCT)
2.3.2. CT Enterography (CTE)
2.4. Image Interpretation
2.5. Intraoperative Assessment
2.6. Pathological Assessment
2.7. Data Analysis
2.8. Statistical Analysis
2.8.1. Concordance (Agreement)
2.8.2. Statistics Summary for a Diagnostic Test
3. Results
3.1. Analysis of Diagnostic Performance Based on Lesion Detection at the Regional Level
3.2. Concordance Analysis Based on PCI Determination
3.3. Staging by PCI Levels: Overestimation, Underestimation, and Agreements
3.4. Diagnostic Performance Measures in Categorised PCI Scoring
3.5. PCI image Staging and Degree of Cytoreduction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aherne, E.A.; Fenlon, H.M.; Shields, C.J.; Mulsow, J.J.; Cronin, C.G. What the Radiologist Should Know About Treatment of Peritoneal Malignancy. AJR Am. J. Roentgenol. 2017, 208, 531–543. [Google Scholar] [CrossRef]
- Llueca, A.; Escrig, J.; MUAPOS Working Group (Multidisciplinary Unit of Abdominal Pelvic Oncology Surgery). Prognostic value of peritoneal cancer index in primary advanced ovarian cancer. Eur. J. Surg. Oncol. 2018, 44, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, A.; Yonemura, Y.; Mehta, S.; Benzerdjeb, N.; Kammar, P.; Parikh, L.; Prabhu, A.; Mishra, S.; Shah, M.; Shaikh, S.; et al. The Pathologic Peritoneal Cancer Index (PCI) Strongly Differs from the Surgical PCI in Peritoneal Metastases Arising From Various Primary Tumors. Ann. Surg. Oncol. 2020, 27, 2985–2996. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S.; del Grande, M.; Manganaro, L.; Papadia, A.; del Grande, F. Imaging before cytoreductive surgery in advanced ovarian cancer patients. Int. J. Gynecol. Cancer 2020, 30, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Courcoutsakis, N.; Tentes, A.A.; Astrinakis, E.; Zezos, P.; Prassopoulos, P. CT-Enteroclysis in the preoperative assessment of the small-bowel involvement in patients with peritoneal carcinomatosis, candidates for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Abdom. Imaging 2013, 38, 56–63. [Google Scholar] [CrossRef]
- Torkzad, M.; Casta, N.; Bergman, A.; Ahlström, H.; Påhlman, L.; Mahteme, H. Comparison between MRI and CT in prediction of peritoneal carcinomatosis index (PCI) in patients undergoing cytoreductive surgery in relation to the experience of the radiologist. J. Surg. Oncol. 2015, 111, 746–751. [Google Scholar] [CrossRef]
- Jacquet, P.; Sugarbaker, P.H. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat. Res. 1996, 82, 359–374. [Google Scholar] [CrossRef]
- Llueca, J.A.; Herraiz, J.L.; Catala, C.; Serra, A.; Rivadulla, I.; Escrig, J. Effectiveness and Safety of Cytoreduction Surgery in Advanced Ovarian Cancer: Initial Experience at a University General Hospital. J. Clin. Gynecol. Obstet. 2015, 4, 251–257. [Google Scholar] [CrossRef]
- Medina, C.M.; Morales, J.G.; Roselló-Sastre, E.; Barriga, K.D.; Sos, J.E.; Roda, J.L.H.; Abellá, J.A.L.; Grupo de Trabajo Unidad Multidisciplinar de Cirugía Oncológica Abdominopélvica (UMCOAP). Protocol for the examination of surgical specimens from patients with peritoneal carcinomatosis originating in ovary, fallopian tube and peritoneum. Rev. Esp. De Patol. 2018, 51, 216–223. [Google Scholar] [CrossRef]
- Lin, L.I. A concordance correlation coefficient to evaluate reproducibility. Biometrics 1989, 45, 255–268. [Google Scholar] [CrossRef]
- Steichen, T.J.; Cox, N.J. A note on the concordance correlation coefficient. Stata J. 2002, 2, 183–189. [Google Scholar] [CrossRef] [Green Version]
- McBride, G.B. NIWA Client Report: HAM2005-062; National Institute of Water & Atmospheric Research: Auckland, New Zealand, 2005. [Google Scholar]
- Fischer, J.E.; Bachmann, L.M.; Jaeschke, R. A readers’ guide to the interpretation of diagnostic test properties: Clinical example of sepsis. Intensive Care Med. 2003, 29, 1043–1051. [Google Scholar] [CrossRef] [Green Version]
- Paulsen, S.R.; Huprich, J.E.; Fletcher, J.G.; Booya, F.; Young, B.M.; Fidler, J.L.; Johnson, C.D.; Barlow, J.M.; Earnest IV, F. CT Enterography as a Diagnostic Tool in Evaluating Small Bowel Disorders: Review of Clinical Experience with over 700 Cases1. Radiographics 2006, 26, 641–657. [Google Scholar] [CrossRef]
- Fletcher, J.G. CT enterography technique: Theme and variations. Abdom. Imaging 2008, 34, 283–288. [Google Scholar] [CrossRef]
- Berger, Y.; Jacoby, H.; Kaufmann, M.I.; Ben-Yaacov, A.; Westreich, G.; Sharon, I.; Barda, L.; Sharif, N.; Nadler, R.; Horesh, N.; et al. Correlation Between Intraoperative and Pathological Findings for Patients Undergoing Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. Ann. Surg. Oncol. 2019, 26, 1103–1109. [Google Scholar] [CrossRef]
- Elzarkaa, A.A.; Shaalan, W.; Elemam, D.; Mansour, H.; Melis, M.; Malik, E.; Soliman, A.A. Peritoneal cancer index as a predictor of survival in advanced stage serous epithelial ovarian cancer: A prospective study. J. Gynecol. Oncol. 2018, 29, e47. [Google Scholar] [CrossRef] [PubMed]
- Duhr, C.D.; Kenn, W.; Kickuth, R.; Kerscher, A.G.; Germer, C.T.; Hahn, D.; Pelz, J.O. Optimizing of preoperative computed tomography for diagnosis in patients with peritoneal carcinomatosis. World J. Surg. Oncol. 2011, 9, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llueca, A.; Serra, A.; Rivadulla, I.; Gomez, L.; Escrig, J. Prediction of suboptimal cytoreductive surgery in patients with advanced ovarian cancer based on preoperative and intraoperative determination of the peritoneal carcinomatosis index. World J. Surg. Oncol. 2018, 16, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Gadelhak, B.; Tawfik, A.M.; Saleh, G.A.; Batouty, N.M.; Sobh, D.M.; Hamdy, O.; Refky, B. Extended abdominopelvic MRI versus CT at the time of adnexal mass characterization for assessing radiologic peritoneal cancer index (PCI) prior to cytoreductive surgery. Abdom. Radiol. 2019, 44, 2254–2261. [Google Scholar] [CrossRef]
- Lee, E.Y.P.; An, H.; Tse, K.Y.; Khong, P.-L. Molecular Imaging of Peritoneal Carcinomatosis in Ovarian Carcinoma. Am. J. Roentgenol. 2020, 215, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Laghi, A.; Bellini, D.; Rengo, M.; Accarpio, F.; Caruso, D.; Biacchi, D.; Di Giorgio, A.; Sammartino, P. Diagnostic performance of computed tomography and magnetic resonance imaging for detecting peritoneal metastases: Systematic review and meta-analysis. Radiol. Med. 2017, 122, 1–15. [Google Scholar] [CrossRef] [PubMed]
- de Bree, E.; Koops, W.; Kröger, R.; van Ruth, S.; Verwaal, V.J.; Zoetmulder, F.A.N. Preoperative computed tomography and selection of patients with colorectal peritoneal carcinomatosis for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Eur. J. Surg. Oncol. 2006, 32, 65–71. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| rCT (n = 42) | CTE (n = 80) | |
|---|---|---|
| Age (years) | ||
| Median | 60 | 65 |
| Range | 27–44 | 31–84 |
| CA 125 | ||
| Median | 276 | 368 |
| Range | 27–890 | 30–1200 |
| Tumor origin | ||
| Ovarian | 40 (95.2%) | 76 (95%) |
| Fallopian tube | 2 (4.8%) | 2 (2.5%) |
| Peritoneum | 0 (0%) | 2 (2.5%) |
| Histologic findings | ||
| Serous carcinoma | 32 (76.2%) | 64 (80%) |
| Mucinosus carcinoma | 4 (9.5%) | 6 (7.5%) |
| Endometrioid carcinoma | 6 (14.3%) | 10 (12.5%) |
| Adverse Effects on CT | ||
| None | - | 106 (87%) |
| Nausea | - | 9 (7%) |
| Diarrhea | - | 4 (3%) |
| Intestinal subocclusion | - | 4 (3%) |
| Radiological PCI | ||
| 1–10 | 34 (81%) | 44 (55%) |
| 11–20 | 8 (19%) | 28 (35%) |
| >20 | 0 (0%) | 8 (10%) |
| Surgical PCI | ||
| 1–10 | 20 (47.6%) | 26 (32.5%) |
| 11–20 | 14 (33.4%) | 28 (35%) |
| >20 | 8 (19%) | 26 (32.5%) |
| Pathological PCI | ||
| 1–10 | 30 (71.5%) | 38 (47.5%) |
| 11–20 | 8 (19%) | 28 (35%) |
| >20 | 4 (9.5%) | 14 (17.5%) |
| Cytoreduction | ||
| CC-0 | 34 (81%) | 76 (95%) |
| CC-1 (<2 cm) | 4 (9.4%) | 4 (5%) |
| CC-2 (2.6–5 cm) | 2 (4.8%) | 0 (0%) |
| CC-3 (>5 cm) | 2 (4.8%) | 0 (0%) |
| Routine CT (rCT) | CT Enterography (CTE) | |
|---|---|---|
| Aquilion 64 Toshiba | Equipment | Aquilion 64 Toshiba |
| 32 × 1 mm | Collimation | 64 × 0.5 mm |
| 5 mm | Slice thickness | 3 mm |
| 5 mm | Reconstruction interval | 3 mm |
| 100 mL | Intravenous (IV) contrast | 130 mL |
| Portal phase | Biphasic (one-time acquisition) | |
| No | Intestinal preparation | Low-residue diet + laxative formulation |
| 800 mL | Oral contrast quantity | 1800 mL |
| Water | Oral contrast | Solution Mannitol 2.5% |
| Free demand | Frequency of administration (oral contrast) | 300 mL every 10–20 min |
| No | Spasmolytic | Buscapina® |
| Sensitivity (95% CI) | Specificity (95% CI) | AUC (95% CI) | |||||
|---|---|---|---|---|---|---|---|
| Surg | Path | Surg | Path | Surg | Path | ||
| R0 a R12 | rCT | 32% (24–40) | 39% (29–48) | 97% (94–100) | 96% (93–99) | 65% (59–70) | 67% (61–74) |
| CTE | 64% (58–70) | 71% (65–77) | 89% (85–93) | 82% (77–86) | 76% (71–81) | 76% (71–82) | |
| R0 a R8 | rCT | 40% (31–49) | 44% (34–55) | 95% 90–100) | 93% (88–98) | 68% (61–75) | 69% (61–76) |
| CTE | 73% (67–79) | 77% (70–83) | 84% (78–90) | 78% (72–84) | 78% (72–84) | 77% (71–83) | |
| R9 a R12 | rCT | NC * | NC * | NC * | NC * | NC * | NC * |
| CTE | 39% (28–51) | 44% (28–61) | 97% (93–100) | 88% (82–94) | 68% (60–75) | 66% (55–77) | |
| Surgical PCI | Pathological PCI | ||||
|---|---|---|---|---|---|
| rCT | CTE | rCT | CTE | Surgical PCI | |
| Lin (rho_c) | 0.49 | 0.65 | 0.62 | 0.86 | 0.78 |
| Lin p value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Pearson (r) | 0.83 | 0.77 | 0.80 | 0.87 | 0.85 |
| Pearson p value | <0.001 | <0.001 | 0.002 | <0.001 | <0.001 |
| C_b | 0.59 | 0.84 | 0.78 | 0.98 | 0.82 |
| Total agreement * | 0.52 | 0.48 | 0.71 | 0.70 | 0.64 |
| Kappa (agreement not due to chance) * | 0.14 | 0.21 | 0.26 | 0.50 | 0.44 |
| Kappa p value * | 0.160 | 0.020 | 0.070 | <0.001 | <0.001 |
| Low-PCI | Mod-PCI | High-PCI | |||||
|---|---|---|---|---|---|---|---|
| Surg | Path | Surg | Path | Surg | Path | ||
| Low-PCI 1–10 | rCT | (≈) 100% | (≈) 93% | (⇓) 86% | (⇓) 75% | (⇓) 25% | - |
| 20 | 28 | 12 | 6 | 2 | 0 | ||
| CTE | (≈) 92% | (≈) 95% | (⇓) 64% | (⇓) 29% | (⇓) 8% | - | |
| 24 | 36 | 18 | 8 | 2 | 0 | ||
| Surgical | (≈) 65% | - | (⇓) 6% | - | - | ||
| 44 | 0 | 2 | 0 | ||||
| Mod-PCI 11–20 | rCT | - | (⇑) 7% | (≈) 14% | (≈) 25% | (⇓) 75% | (⇓) 100% |
| 0 | 2 | 2 | 2 | 6 | 4 | ||
| CTE | (⇑) 3% | (⇑) 5% | (≈) 29% | (≈) 57% | (⇓) 69% | (⇓) 71% | |
| 2 | 2 | 8 | 16 | 18 | 10 | ||
| Surgical | (⇑) 32% | - | (≈) 50% | (⇓) 11% | |||
| 22 | 0 | 0 | 2 | ||||
| High-PCI >20 | rCT | - | - | - | - | - | - |
| 0 | 0 | 0 | 0 | 0 | 0 | ||
| CTE | - | - | (⇑) 7% | (⇑) 14% | (≈) 23% | (≈) 29% | |
| 0 | 0 | 2 | 4 | 6 | 4 | ||
| Surgical | (⇑) 3% | (⇑) 44% | (≈) 89% | ||||
| 2 | 16 | 16 | |||||
| Sensitivity (95% CI) | Specificity (95% CI) | AUC (95% CI) | |||||
|---|---|---|---|---|---|---|---|
| Surg | Path | Surg | Path | Surg | Path | ||
| Low-PCI 1–10 | rCT | 100% (69–100) | 100% (78–100) | 27% (6–61) | 50% (12–88) | 64% (50–77) | 75% (53–97) |
| CTE | 92% (64–100) | 94% (73–100) | 63% (42–81) | 77% (55–92) | 78% (66–90) | 86% (75–96) | |
| Surg | - | 68% (48–82) | - | 96% (82–100) | - | 82% (73–90) | |
| Mod-PCI 11–20 | rCT | 25% (63–81) | 25% (63–81) | 65% (38–86) | 82% (57–96) | 45% (18–72) | 54% (28–80) |
| CTE | 29% (8–58) | 57% (29–82) | 62% (41–80) | 77% (56–91) | 45% (30–61) | 67% (51–83) | |
| Surg | - | 50% (26–74) | - | 72% (56–85) | - | 61% (47–75) | |
| High-PCI >20 | rCT | NC * | NC * | NC * | NC * | NC * | NC * |
| CTE | 75% (19–99) | 50% (7–93) | 72% (55–86) | 76% (81–95) | 74% (48–99) | 68% (39–97) | |
| Surg | - | 89% (52–100) | - | 83% (70–92) | - | 86% (74–98) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delgado-Barriga, K.; Medina, C.; Gomez-Quiles, L.; Marco-Domenech, S.F.; Escrig, J.; Llueca, A. CT Enterography for Preoperative Evaluation of Peritoneal Carcinomatosis Index in Advanced Ovarian Cancer. J. Clin. Med. 2022, 11, 476. https://doi.org/10.3390/jcm11030476
Delgado-Barriga K, Medina C, Gomez-Quiles L, Marco-Domenech SF, Escrig J, Llueca A. CT Enterography for Preoperative Evaluation of Peritoneal Carcinomatosis Index in Advanced Ovarian Cancer. Journal of Clinical Medicine. 2022; 11(3):476. https://doi.org/10.3390/jcm11030476
Chicago/Turabian StyleDelgado-Barriga, Katty, Carmen Medina, Luis Gomez-Quiles, Santiago F. Marco-Domenech, Javier Escrig, and Antoni Llueca. 2022. "CT Enterography for Preoperative Evaluation of Peritoneal Carcinomatosis Index in Advanced Ovarian Cancer" Journal of Clinical Medicine 11, no. 3: 476. https://doi.org/10.3390/jcm11030476