
Spectrum of Kidney Disorders Associated with T-Cell Immunoclones

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Patients’ Characteristics
2.2. Immunological Analyses
2.3. STAT3 and TCR Sequencing
2.4. Statistical Analyses
3. Results
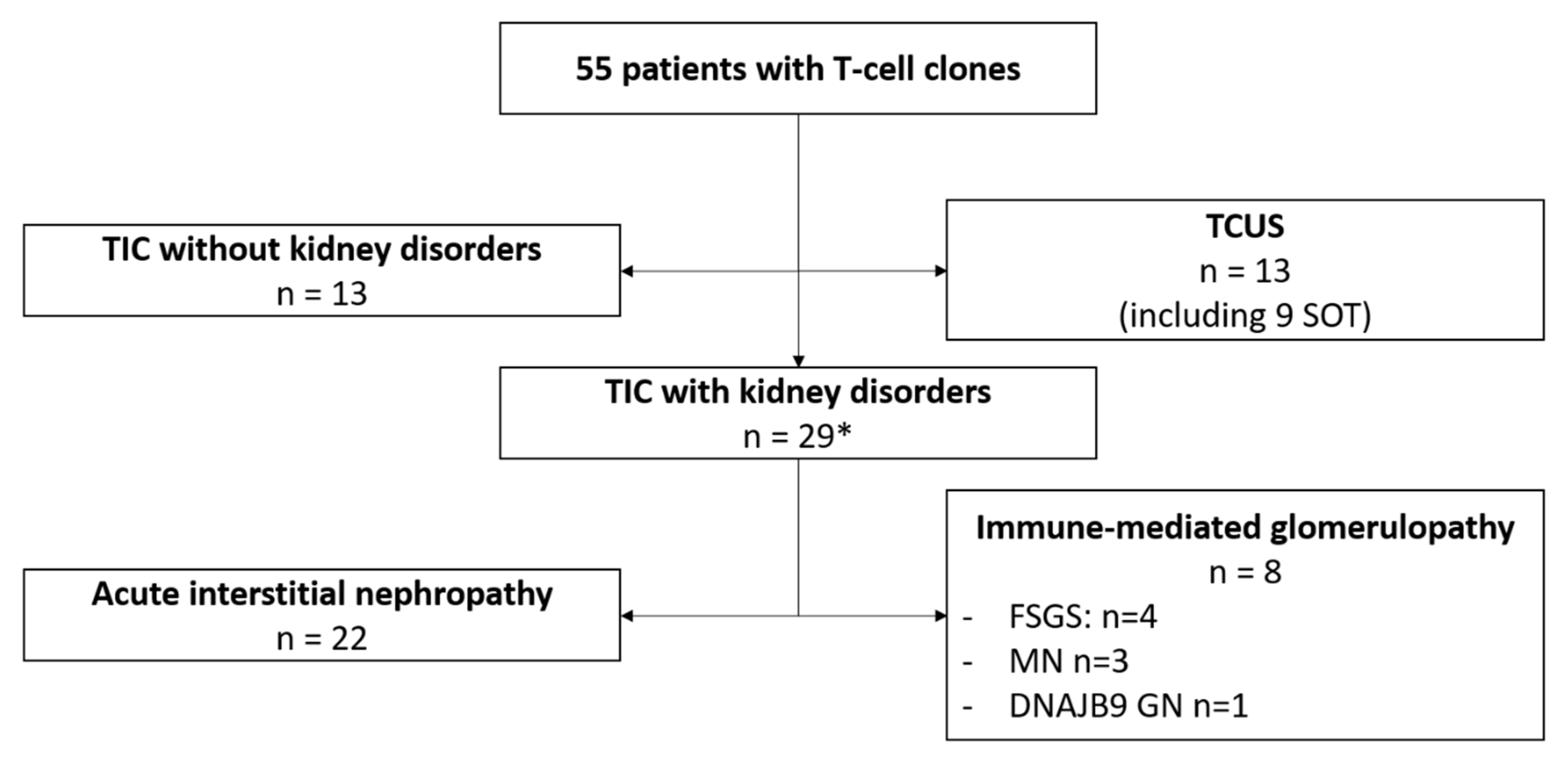
3.1. Patients
3.2. Kidney Presentation
3.3. Characteristics of the Immunoclones
3.4. Outcomes
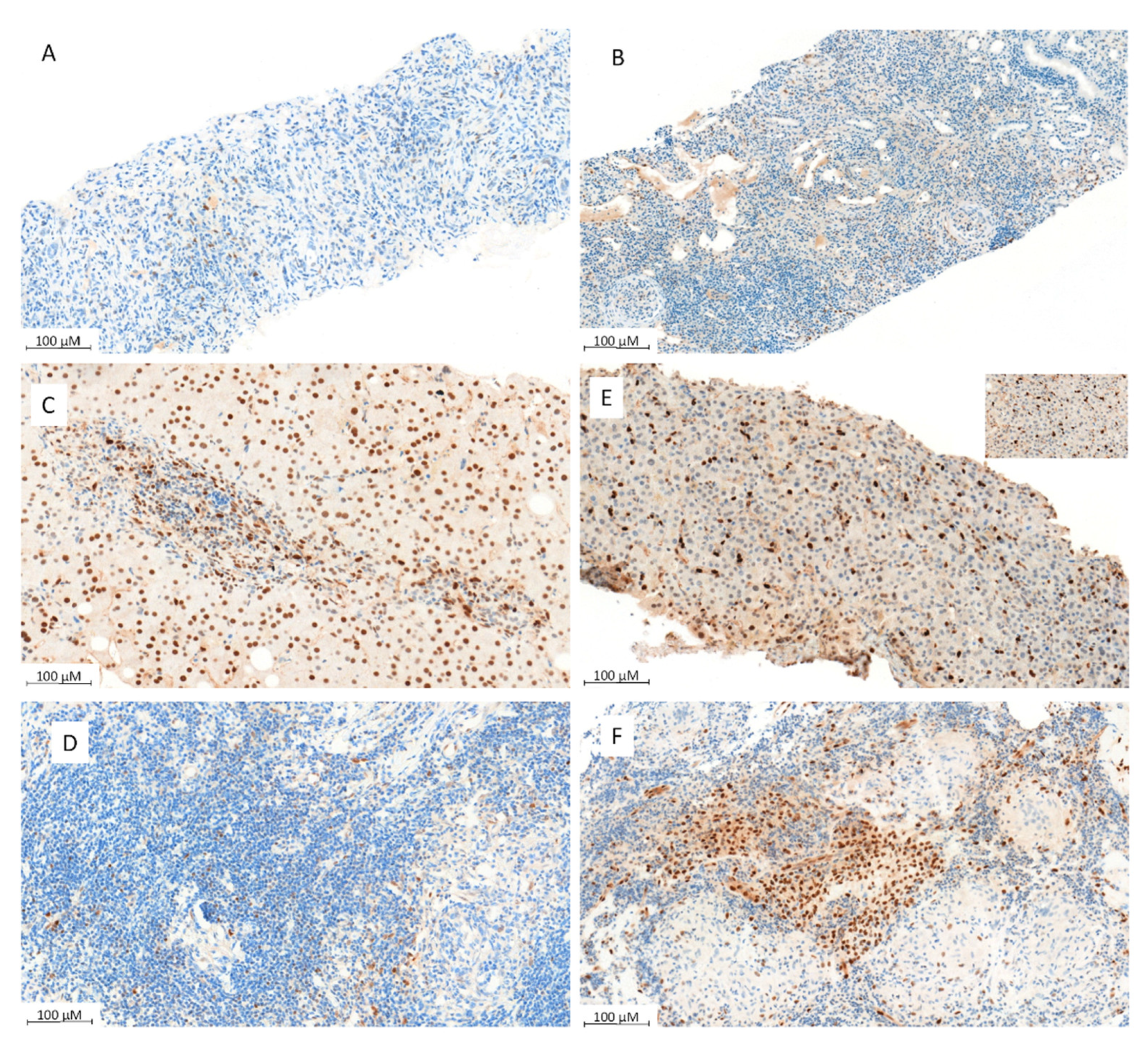
3.5. Mechanisms of Inflammatory Fibrosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lamy, T.; Moignet, A.; Loughran, T.P. LGL leukemia: From pathogenesis to treatment. Blood 2017, 129, 1082–1094. [Google Scholar] [CrossRef]
- Clemente, M.J.; Wlodarski, M.W.; Makishima, H.; Viny, A.D.; Bretschneider, I.; Shaik, M.; Bejanyan, N.; Lichtin, A.E.; Hsi, E.D.; Paquette, R.L.; et al. Clonal drift demonstrates unexpected dynamics of the T-cell repertoire in T-large granular lymphocyte leukemia. Blood 2011, 118, 4383–4393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jerez, A.; Clemente, M.J.; Makishima, H.; Rajala, H.; Gómez-Seguí, I.; Olson, T.; McGraw, K.; Przychodzen, B.; Kulasekararaj, A.; Afable, M.; et al. STAT3 mutations indicate the presence of subclinical T-cell clones in a subset of aplastic anemia and myelodysplastic syndrome patients. Blood 2013, 122, 2453–2459. [Google Scholar] [CrossRef] [PubMed]
- Kerr, C.M.; Clemente, M.J.; Chomczynski, P.W.; Przychodzen, B.; Nagata, Y.; Adema, V.; Visconte, V.; Lichtin, A.E.; Mustjoki, S.; Radivoyevitch, T.; et al. Subclonal STAT3 mutations solidify clonal dominance. Blood Adv. 2019, 3, 917–921. [Google Scholar] [CrossRef] [PubMed]
- Jerez, A.; Clemente, M.J.; Makishima, H.; Koskela, H.; LeBlanc, F.; Ng, K.P.; Olson, T.; Przychodzen, B.; Afable, M.; Gomez-Segui, I.; et al. STAT3 mutations unify the pathogenesis of chronic lymphoproliferative disorders of NK cells and T-cell large granular lymphocyte leukemia. Blood 2012, 120, 3048–3057. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Guan, N.; Zhu, P.; Chen, T.; Liu, S.; Hao, C.; Xue, J. Recurrent anti-GBM disease with T-cell large granular lymphocytic leukemia: A case report. Medicine 2019, 98, e16649. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Lee, L.X.; Zhou, P.; Fogaren, T.; Varga, C.; Comenzo, R.L. A case of T-cell large granular lymphocytic leukemia and renal immunoglobulin heavy chain amyloidosis. Am. J. Case Rep. 2019, 20, 43–47. [Google Scholar] [CrossRef]
- Christopoulos, P.D.; Katsoudas, S.; Androulaki, A.; Nakopoulou, L.; Economopoulos, T.; Vlahakos, D.V. T-cell large granular lymphocyte leukemia presenting as end-stage renal disease: The diagnostic role of flow-cytometric and clonality analysis of the urine sediment. Clin. Nephrol. 2009, 71, 198–202. [Google Scholar] [CrossRef]
- Sibal, J.; Valenzuela, R.; Tubbs, R.; Hodge, E.; Nally, J. Successful Renal Transplantation in a Patient with Large Granular Lymphocytic Leukemia with Natural Killer Cell Proliferation. Nephron 1996, 72, 292–297. [Google Scholar] [CrossRef]
- Airò, P.; Rossi, G.; Facchetti, F.; Marocolo, D.; Garza, L.; Lanfranchi, A.; Prati, E.; Brugnoni, D.; Malacarne, F.; Cattaneo, R. Monoclonal expansion of large granular lymphocytes with a CD4+ CD8dim+/− phenotype associated with hairy cell leukemia. Haematologica 1995, 80, 146–149. [Google Scholar]
- Bassan, R.; Rambaldi, A.; Abbate, M.; Biondi, A.; Allavena, P.; Barbui, T.; Bertani, T. Association of NK-cell lymphoproliferative disease and nephrotic syndrome. Am. J. Clin. Pathol. 1990, 94, 334–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotta, O.; Miyazawa, S.; Taguma, Y.; Onodera, S.; Kitamura, H.; Yusa, N.; Nakamura, K. Mesangiolysis associated with severe glomerular endocapillary proliferation of CD57 large granular lymphocytes. Clin. Nephrol. 1995, 43, 297–302. [Google Scholar] [PubMed]
- Ribes, D.; Casemayou, A.; El Hachem, H.; Laurent, C.; Guilbeau-Frugier, C.; Vergez, F.; Tavitian, S.; Schanstra, J.P.; Chauveau, D.; Bascands, J.L.; et al. Asymptomatic circulating T-cell clone cause renal polymorphic inflammatory fibrosis. Clin. Exp. Nephrol. 2017, 21, 781–786. [Google Scholar] [CrossRef]
- Mailloux, A.W.; Zhang, L.; Moscinski, L.; Bennett, J.M.; Yang, L.; Yoder, S.J.; Bloom, G.; Wei, C.; Wei, S.; Sokol, L.; et al. Fibrosis and Subsequent Cytopenias Are Associated with Basic Fibroblast Growth Factor–Deficient Pluripotent Mesenchymal Stromal Cells in Large Granular Lymphocyte Leukemia. J. Immunol. 2013, 191, 3578–3593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singleton, T.P.; Yin, B.; Teferra, A.; Mao, J.Z. Spectrum of Clonal Large Granular Lymphocytes (LGLs) of αβ T Cells: T-Cell Clones of Undetermined Significance, T-Cell LGL Leukemias, and T-Cell Immunoclones. Am. J. Clin. Pathol. 2015, 144, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhodapkar, M.V.; Li, C.Y.; Lust, J.A.; Tefferi, A.; Phyliky, R.L. Clinical spectrum of clonal proliferations of T-large granular lymphocytes: A T-cell clonopathy of undetermined significance? Blood 1994, 84, 1620–1627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bigouret, V.; Hoffmann, T.; Arlettaz, L.; Villard, J.; Colonna, M.; Ticheli, A.; Gratwohl, A.; Samii, K.; Chapuis, B.; Rufer, N.; et al. Monoclonal T-cell expansions in asymptomatic individuals and in patients with large granular leukemia consist of cytotoxic effector T cells expressing the activating CD94:NKG2C/E and NKD2D killer cell receptors. Blood 2003, 101, 3198–3204. [Google Scholar] [CrossRef] [Green Version]
- Van Dongen, J.J.M.; Langerak, A.W.; Brüggemann, M.; Evans, P.A.S.; Hummel, M.; Lavender, F.L.; Delabesse, E.; Davi, F.; Schuuring, E.; García-Sanz, R.; et al. Design and standardization of PCR primers and protocols for detection of clonal immunoglobulin and T-cell receptor gene recombinations in suspect lymphoproliferations: Report of the BIOMED-2 Concerted Action BMH4-CT98-3936. Leukemia 2003, 17, 2257–2317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duez, M.; Giraud, M.; Herbert, R.; Rocher, T.; Salson, M.; Thonier, F. Vidjil: A web platform for analysis of high-Throughput repertoire sequencing. PLoS ONE 2016, 11, e0166126. [Google Scholar] [CrossRef]
- Bilori, B.; Thota, S.; Clemente, M.J.; Patel, B.; Jerez, A.; Afable, M., II; Maciejewski, J.P. Tofacitinib as a novel salvage therapy for refractory T-cell large granular lymphocytic leukemia. Leukemia 2015, 29, 2427–2429. [Google Scholar] [CrossRef]
- Damsky, W.; Thakral, D.; Emeagwali, N.; Galan, A.; King, B. Tofacitinib Treatment and Molecular Analysis of Cutaneous Sarcoidosis. N. Engl. J. Med. 2018, 379, 2540–2546. [Google Scholar] [CrossRef] [PubMed]
- Fermand, J.P.; Bridoux, F.; Dispenzieri, A.; Jaccard, A.; Kyle, R.A.; Leung, N.; Merlini, G. Monoclonal gammopathy of clinical significance: A novel concept with therapeutic implications. Blood 2018, 132, 1478–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohn, M.; Karras, A.; Zaidan, M.; Bénière, C.; de Fréminville, J.B.; Laribi, K.; Perrin, M.C.; Malphettes, M.; le Calloch, R.; Anglaret, B.; et al. Lymphomas with kidney involvement: The French multicenter retrospective LyKID study. Leuk. Lymphoma 2020, 61, 887–895. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Pt | Age | Kidney Disease | Extra-Kidney Disorders | Clone Size | Treatment | eGFR at Last Follow-Up |
|---|---|---|---|---|---|---|
| 1 | 70 | Acute interstitial nephropathy | Tissue | Cst | CR | |
| 2 | 62 | Acute interstitial nephropathy | 23% | Cst, RTX | CR | |
| 3 | 55 | Acute interstitial nephropathy | Thyroiditis, cholangitis | Tissue | Cst | ESKD |
| 4 | 78 | Acute interstitial nephropathy | Chronic myelomonocytic leukemia | 16% | CsA | Stable |
| 5 | 79 | Acute interstitial nephropathy | Hepatitis, chronic neutropenia | 27% | None | Early death |
| 6 | 52 | Acute interstitial nephropathy | Psoriasis | 20% | None | Loss of follow-up |
| 7 | 71 | Acute interstitial nephropathy | Interstitial lung disease | 31% | Cst | Steroid dependency |
| 8 | 76 | Acute interstitial nephropathy | Psoriatic arthritis, pleura infiltration | 27% | Leflunomide, HCQ, MTX, anti-TNFa, Cst | Stable |
| 9 | 49 | Acute interstitial nephropathy | Tissue | Cst | ESKD | |
| 10 | 35 | Acute interstitial nephropathy | Uveitis | 11% | Cst, CsA | CR |
| 11 | 52 | Acute interstitial nephropathy | IgG4 syndrome | 12% | Cst, RTX | Steroid dependency |
| 12 | 48 | Acute interstitial nephropathy | Tissue | Cst | CR | |
| 13 | 67 | Acute interstitial nephropathy | 15% | Cst | CR | |
| 14 | 81 | Acute interstitial nephropathy | 31% | Cst | CR | |
| 15 | 50 | Acute interstitial nephropathy | 14% | Cst, CsA | CR | |
| 16 | 66 | Acute interstitial nephropathy | IgG4 syndrome | 22% | Cst, RTX | CR |
| 17 | 69 | Acute interstitial nephropathy | Bullous pemphigoid, cholangitis | 42% | Cst, CsA | CR |
| 18 | 69 | Acute interstitial nephropathy | Sjögren syndrome, myasthenia, interstitial lung disease | 20% | Cst, RTX | Stable |
| 19 | 56 | Acute interstitial nephropathy | Myositis | 14% | Cst, CsA | ESKD |
| 20 | 46 | Acute interstitial nephropathy | Uveitis, scleritis, thyroiditis | 21% | Cst | CR |
| 21 | 77 | Acute interstitial nephropathy | Immune thrombocytopenia, vitiligo, interstitial lung disease | 27% | Cst, RTX, IgIV, CsA, Tofacitinib | CR |
| 22 | 84 | Acute interstitial nephropathy | Anemia, thrombocytopenia | 17% | CSt, CsA | No |
| 23 | 75 | Focal and segmental glomerulosclerosis | 23% | CsA | CR | |
| 72 | Focal and segmental glomerulosclerosis | 21% | Cst, CsA | CR | ||
| 24 | 67 | Focal and segmental glomerulosclerosis | 22% | Cst, RTX, Tofacitinib | Steroid dependency | |
| 25 | 43 | PLA2R+ membranous nephropathy | Immune thrombocytopenia | 7% | RTX | CR |
| 26 | 71 | PLA2R+ membranous nephropathy | Polymyalgia rheumatica | 14% | RTX | CR |
| 27 | 76 | PLA2R+ membranous nephropathy | Granulomatous hepatitis | 12% | None | Loss of follow-up |
| 28 | 58 | Minimal change disease | Rheumatoid arthritis | 25% | Cst, RTX, CsA | CR |
| 29 | 44 | DNAJB9+ fibrillary glomerulonephritis | Myositis | 19% | None | Stable |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piedrafita, A.; Vergez, F.; Belliere, J.; Prades, N.; Colombat, M.; Huart, A.; Rieu, J.-B.; Lagarde, S.; Del Bello, A.; Kamar, N.; et al. Spectrum of Kidney Disorders Associated with T-Cell Immunoclones. J. Clin. Med. 2022, 11, 604. https://doi.org/10.3390/jcm11030604
Piedrafita A, Vergez F, Belliere J, Prades N, Colombat M, Huart A, Rieu J-B, Lagarde S, Del Bello A, Kamar N, et al. Spectrum of Kidney Disorders Associated with T-Cell Immunoclones. Journal of Clinical Medicine. 2022; 11(3):604. https://doi.org/10.3390/jcm11030604
Chicago/Turabian StylePiedrafita, Alexis, François Vergez, Julie Belliere, Nais Prades, Magali Colombat, Antoine Huart, Jean-Baptiste Rieu, Stéphanie Lagarde, Arnaud Del Bello, Nassim Kamar, and et al. 2022. "Spectrum of Kidney Disorders Associated with T-Cell Immunoclones" Journal of Clinical Medicine 11, no. 3: 604. https://doi.org/10.3390/jcm11030604