
Vitamin D Level in Patients with Consecutive Acute Coronary Syndrome Is Not Correlated with the Parameters of Platelet Activity

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Examinations
2.3. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Comparison between Patients with Stable Coronary Artery Disease and Patients with Acute Coronary Syndrome
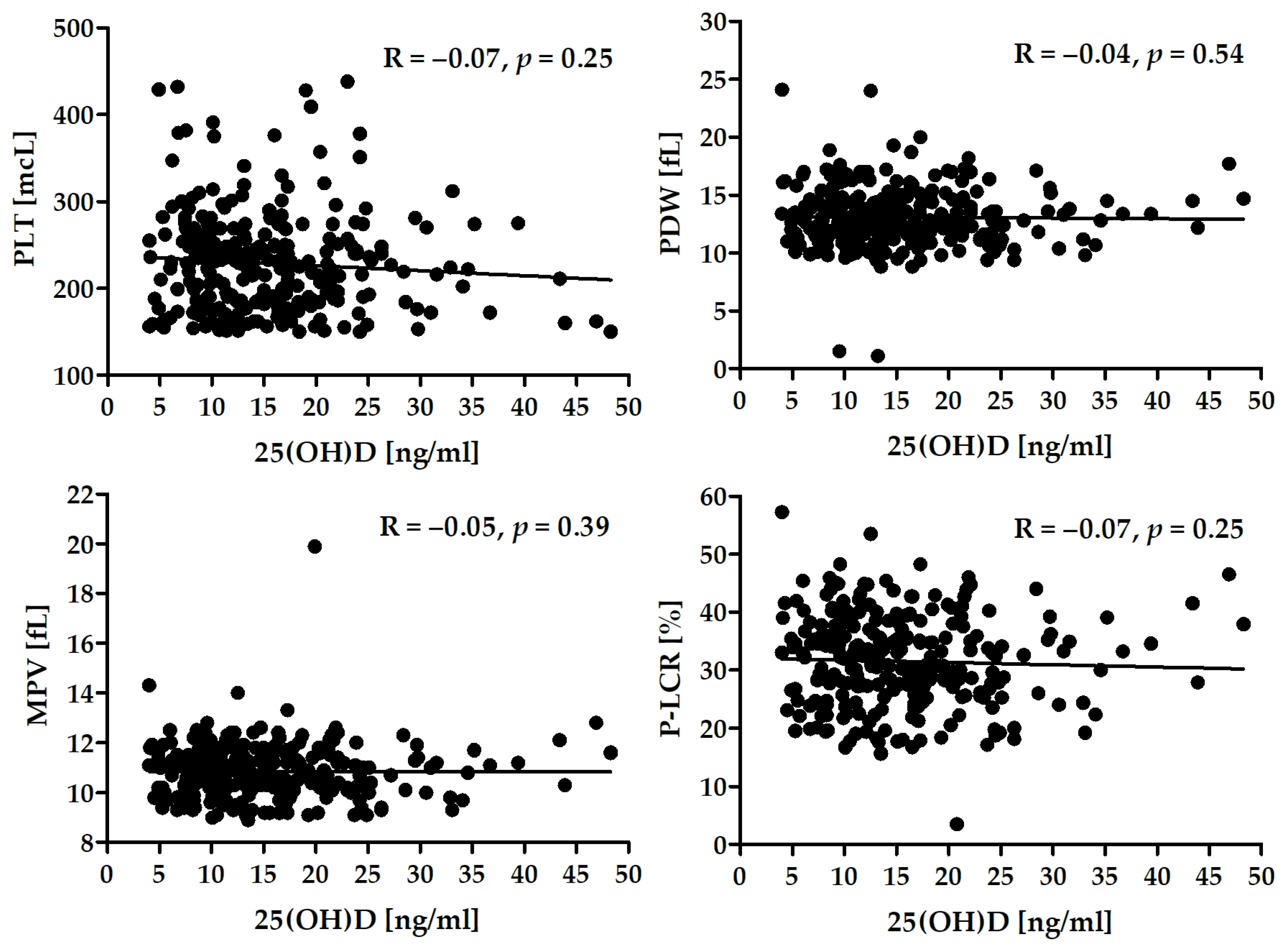
3.3. Correlation between Vitamin D Levels and Platelet Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gawaz, M.; Langer, H.; May, A.E. Platelets in inflammation and atherogenesis. J. Clin. Investig. 2005, 115, 3378–3384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.; Schoene, N.; Harris, W. Mean platelet volume as an indicator of platelet activation: Methodological issues. Platelets 2002, 13, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Varol, E.; Ozaydin, M.; Türker, Y.; Alaca, S. Mean platelet volume, an indicator of platelet activation, is increased in patients with mitral stenosis and sinus rhythm. Scand. J. Clin. Lab. Investig. 2009, 69, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Desai, K.N.; Patel, K.; Shah, M.; Ranapurwala, M.; Chaudhari, S.; Shah, M.; Shah, M. A study of platelet volume indices (PVI) in patients of coronary artery disease and acute myocardial infarction in tertiary care hospital. Int. J. Adv. Res. 2013, 1, 185–191. [Google Scholar]
- Kanbay, A.; Tutar, N.; Kaya, E.; Buyukoglan, H.; Ozdogan, N.; Oymak, F.S.; Gulmez, I.; Demir, R. Mean platelet volume in patients with obstructive sleep apnea syndrome and its relationship with cardiovascular diseases. Blood Coagul. Fibrinolysis 2013, 24, 532–536. [Google Scholar] [CrossRef]
- Debili, N.; Massé, J.M.; Katz, A.; Guichard, J.; Breton-Gorius, J.; Vainchenker, W. Effects of the recombinant hematopoietic growth factors interleukin-3. interleukin-6. stem cell factor. and leukemia inhibitory factor on the megakaryocytic differentiation of CD34+ cells. Blood 1993, 82, 84–95. [Google Scholar] [CrossRef] [Green Version]
- Burstein, S.A.; Downs, T.; Friese, P.; Lynam, S.; Anderson, S.; Henthorn, J.; Epstein, R.B.; Savage, K. Thrombocytopoiesis in normal and sublethally irradiated dogs: Response to human interleukin-6. Blood 1992, 80, 420–428. [Google Scholar] [CrossRef]
- Khandekar, M.M.; Khurana, A.S.; Deshmukh, S.D.; Kakrani, A.L.; Katdare, A.D.; Inamdar, A.K. Platelet volume indices in patients with coronary artery disease and acute myocardial infarction: An Indian scenario. J. Clin. Pathol. 2006, 59, 146–149. [Google Scholar] [CrossRef] [Green Version]
- Murat, S.N.; Duran, M.; Kalay, N.; Gunebakmaz, O.; Akpek, M.; Doger, C.; Elcik, D.; Ocak, A.; Vatankulu, M.A.; Turfan, M.; et al. Relation between mean platelet volume and severity of atherosclerosis in patients with acute coronary syndromes. Angiology 2013, 64, 131–136. [Google Scholar] [CrossRef]
- Ekici, B.; Erkan, A.F.; Alhan, A.; Sayın, I.; Aylı, M.; Töre, H.F. Is mean platelet volume associated with the angiographic severity of coronary artery disease? Kardiol. Pol. 2013, 71, 832–838. [Google Scholar] [CrossRef]
- Pal, R.; Bagarhatta, R.; Gulati, S.; Rathore, M.; Sharma, N. Mean platelet volume in patients with acute coronary syndromes: A supportive diag-nostic predictor. J. Clin. Diagn. Res. 2014, 8, MC01–MC04. [Google Scholar] [CrossRef] [PubMed]
- Khode, V.; Sindhur, J.; Kanbur, D.; Ruikar, K.; Nallulwar, S. Mean platelet volume and other platelet volume indices in patients with stable coronary artery disease and acute myocardial infarction: A case control study. J. Cardiovasc. Dis. Res. 2012, 3, 272–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gawlita, M.; Wasilewski, J.; Osadnik, T.; Reguła, R.; Bujak, K.; Gonera, M. Mean platelet volume and platelet-large cell ratio as prognostic factors for coronary artery disease and myocardial infarction. Folia Cardiol. 2015, 10, 418–422. [Google Scholar] [CrossRef] [Green Version]
- Rechciński, T.; Jasińska, A.; Foryś, J.; Krzemińska-Pakuła, M.; Wierzbowska-Drabik, K.; Plewka, M.; Peruga, J.Z.; Kasprzak, J.D. Prognostic value of platelet indices after acute myocardial infarction treated with primary percutaneous coronary intervention. Cardiol. J. 2013, 20, 491–498. [Google Scholar] [CrossRef] [Green Version]
- Kırbaş, Ö.; Kurmuş, Ö.; Köseoğlu, C.; Duran Karaduman, B.; Saatçi Yaşar, A.; Alemdar, R.; Ali, S.; Bilge, M. Association between admission mean platelet volume and ST segment resolution after thrombolytic therapy for acute myocardial infarction. Anadolu. Kardiyol. Derg. 2014, 14, 728–732. [Google Scholar] [CrossRef] [Green Version]
- Sarli, B.; Baktir, A.O.; Saglam, H.; Arinc, H.; Kurtul, S.; Sivgin, S.; Akpek, M.; Kaya, M.G. Mean platelet volume is associated with poor postinterventional myocardial blush grade in patients with ST-segment elevation myocardial infarction. Coron. Artery Dis. 2013, 24, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Sezer, M.; Okcular, I.; Goren, T.; Oflaz, H.; Nisanci, Y.; Umman, B.; Mercanoglu, F.; Bilge, A.K.; Meric, M.; Umman, S. Association of haematological indices with the degree of microvascular injury in patients with acute anterior wall myocardial infarction treated with primary percutaneous coronary intervention. Heart 2007, 93, 313–318. [Google Scholar] [CrossRef] [Green Version]
- Slavka, G.; Perkmann, T.; Haslacher, H.; Greisenegger, S.; Marsik, C.; Wagner, O.F.; Endler, G. Mean platelet volume may represent a predictive parameter for overall vascular mortality and ischemic heart disease. Arter. Thromb. Vasc. Biol. 2011, 31, 1215–1218. [Google Scholar] [CrossRef] [Green Version]
- Gang, L.; Yanyan, Z.; Zhongwei, Z.; Juan, D. Association between mean platelet volume and hypertension incidence. Hypertens. Res. 2017, 40, 779–784. [Google Scholar] [CrossRef]
- Tekin, G.; Tekin, Y.K.; Sivri, N.; Yetkin, E. Mean platelet volume in patients with nonvalvular atrial fibrillation. Blood Coagul. Fibrinolysis 2013, 24, 537–539. [Google Scholar] [CrossRef]
- Hekimsoy, Z.; Payzin, B.; Ornek, T.; Kandoğan, G. Mean platelet volume in Type 2 diabetic patients. J. Diabetes Complicat. 2004, 18, 173–176. [Google Scholar] [CrossRef]
- Ju, H.Y.; Kim, J.K.; Hur, S.M.; Woo, S.A.; Park, K.A.; Park, M.Y.; Choi, S.J.; Hwang, S.D. Could mean platelet volume be a promising biomarker of progression of chronic kidney disease? Platelets 2015, 26, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Coban, E.; Ozdogan, M.; Yazicioglu, G.; Akcit, F. The mean platelet volume in patients with obesity. Int. J. Clin. Pract. 2005, 59, 981–982. [Google Scholar] [CrossRef] [PubMed]
- Kassi, E.; Adamopoulos, C.; Basdra, E.; Papavassiliou, A.G. Role of vitamin D in atherosclerosis. Circulation 2013, 128, 2517–2531. [Google Scholar] [CrossRef] [Green Version]
- Brandenburg, V.M.; Vervloet, M.G.; Marx, N. The role of vitamin D in cardiovascular disease: From present evidence to future perspectives. Atherosclerosis 2012, 225, 253–263. [Google Scholar] [CrossRef]
- Prietl, B.; Treiber, G.; Pieber, T.R.; Amrein, K. Vitamin D and immune function. Nutrients 2013, 5, 2502–2521. [Google Scholar] [CrossRef]
- Müller, K.; Haahr, P.M.; Diamant, M.; Rieneck, K.; Kharazmi, A.; Bendtzen, K. 1.25-Dihydroxyvitamin D3 inhibits cytokine production by human blood monocytes at the post-transcriptional level. Cytokine 1992, 4, 506–512. [Google Scholar] [CrossRef]
- Talmor, Y.; Golan, E.; Benchetrit, S.; Bernheim, J.; Klein, O.; Green, J.; Rashid, G. Calcitriol blunts the deleterious impact of advanced glycation end products on en-dothelial cells. Am. J. Physiol. Renal Physiol. 2008, 294, F1059–F1064. [Google Scholar] [CrossRef] [Green Version]
- Young, J.L.; Libby, P.; Schönbeck, U. Cytokines in the pathogenesis of atherosclerosis. Thromb. Haemost. 2002, 88, 554–567. [Google Scholar] [CrossRef]
- Robertson, A.K.; Hansson, G.K. T cells in atherogenesis: For better or for worse? Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2421–2432. [Google Scholar] [CrossRef]
- Stach, K.; Kälsch, A.I.; Nguyen, X.D.; Elmas, E.; Kralev, S.; Lang, S.; Weiss, C.; Borggrefe, M.; Kälsch, T. 1α,25-Dihydroxyvitamin D3 attenuates platelet activation and the expression of VCAM-1 and MT1-MMP in human endothelial cells. Cardiology 2011, 118, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Cumhur Cure, M.; Cure, E.; Yuce, S.; Yazici, T.; Karakoyun, I.; Efe, H. Mean platelet volume and vitamin D level. Ann. Lab. Med. 2014, 34, 98–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dziedzic, E.A.; Gąsior, J.S.; Saniewski, T. Dąbrowski, M. Vitamin D deficiency among Polish patients with angiographically confirmed coronary heart disease. Pol. Merkur. Lek. 2021, 49, 278–282. [Google Scholar]
- Dziedzic, E.A.; Gąsior, J.S.; Pawłowski, M.; Dąbrowski, M. Association of Vitamin D Deficiency and Degree of Coronary Artery Disease in Cardiac Patients with Type 2 Diabetes. J. Diabetes Res. 2017, 2017, 3929075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dziedzic, E.A.; Gąsior, J.S.; Pawłowski, M.; Wodejko-Kucharska, B.; Saniewski, T.; Marcisz, A.; Dąbrowski, M.J. Vitamin D level is associated with severity of coronary artery atherosclerosis and incidence of acute coronary syndromes in non-diabetic cardiac patients. Arch. Med. Sci. 2019, 15, 359–368. [Google Scholar] [CrossRef]
- Dziedzic, E.A.; Przychodzeń, S.; Dąbrowski, M. The effects of vitamin D on severity of coronary artery atherosclerosis and lipid profile of cardiac patients. Arch. Med. Sci. 2016, 12, 1199–1206. [Google Scholar] [CrossRef] [Green Version]
- Dziedzic, E.A.; Smyk, W.; Sowińska, I.; Dąbrowski, M.; Jankowski, P. Serum Level of Vitamin D Is Associated with Severity of Coronary Atherosclerosis in Postmenopausal Women. Biology 2021, 10, 1139. [Google Scholar] [CrossRef]
- Krzywanski, J.; Mikulski, T.; Krysztofiak, H.; Mlynczak, M.; Gaczynska, E.; Ziemba, A. Seasonal vitamin D status in polish elite athletes in relation to sun exposure and oral supplementation. PLoS ONE 2016, 11, e0164395. [Google Scholar] [CrossRef]
- Wielders, J.P.; Carter, G.F.; Eberl, H.; Morris, G.; Roth, H.J.; Vogl, C. Automated Competitive Protein-Binding Assay for Total 25-OH Vitamin D. Multicenter Evaluation and Practical Performance. J. Clin. Lab. Anal. 2015, 29, 451–461. [Google Scholar] [CrossRef]
- Abdel-Wareth, L.; Haq, A.; Turner, A.; Khan, S.; Salem, A.; Mustafa, F.; Hussein, N.; Pallinalakam, F.; Grundy, L.; Patras, G.; et al. Total vitamin D assay comparison of the Roche Diagnostics “Vitamin D total” electrochemiluminescence protein binding assay with the Chromsystems HPLC method in a population with both D2 and D3 forms of vitamin D. Nutrients 2013, 5, 971–980. [Google Scholar] [CrossRef]
- Knudsen, C.S.; Nexo, E.; Højskov, C.S.; Heickendorff, L. Analytical validation of the Roche 25-OH Vitamin D Total assay. Clin. Chem. Lab. Med. 2012, 50, 1965–1968. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.Y.; Kwon, M.J.; Song, J.; Park, H.; Woo, H.Y. Measurement of serum total vitamin D (25-OH) using automated immunoassay in comparison [corrected] with liquid chromatography tandem-mass spectrometry. J. Clin. Lab. Anal. 2013, 27, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Sahota, O. Understanding vitamin D deficiency. Age Ageing 2014, 43, 589–591. [Google Scholar] [PubMed] [Green Version]
- Heaney, R.P. Vitamin D in health and disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1535–1541. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Al-Khalidi, B.; Kimball, S.M.; Rotondi, M.A.; Ardern, C.I. Standardized serum 25-hydroxyvitamin D concentrations are inversely associated with cardiometabolic disease in U.S. adults: A cross-sectional analysis of NHANES, 2001–2010. Nutr. J. 2017, 16, 16. [Google Scholar] [CrossRef] [Green Version]
- Engelsen, O. The relationship between ultraviolet radiation exposure and vitamin D status. Nutrients 2010, 2, 482–495. [Google Scholar] [CrossRef] [Green Version]
- Ringqvist, I.; Fisher, L.D.; Mock, M.; Davis, K.B.; Wedel, H.; Chaitman, B.R.; Passamani, E.; Russell, R.O., Jr.; Alderman, E.L.; Kouchoukas, N.T.; et al. Prognostic value of angiographic indices of coronary artery disease from the Coronary Artery Surgery Study (CASS). J. Clin. Investig. 1983, 71, 1854–1866. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Sansanayudh, N.; Anothaisintawee, T.; Muntham, D.; McEvoy, M.; Attia, J.; Thakkinstian, A. Mean platelet volume and coronary artery disease: A systematic review and meta-analysis. Int. J. Cardiol. 2014, 175, 433–440. [Google Scholar] [CrossRef]
- Chu, S.G.; Becker, R.C.; Berger, P.B.; Bhatt, D.L.; Eikelboom, J.W.; Konkle, B.; Mohler, E.R.; Reilly, M.P.; Berger, J.S. Mean platelet volume as a predictor of cardiovascular risk: A systematic review and meta-analysis. J. Thromb. Haemost. 2010, 8, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Korzonek-Szlacheta, I.; Hudzik, B.; Nowak, J.; Szkodzinski, J.; Nowak, J.; Gąsior, M.; Zubelewicz-Szkodzinska, B. Mean platelet volume is associated with serum 25-hydroxyvitamin D concentrations in patients with stable coronary artery disease. Heart Vessel. 2018, 33, 1275–1281. [Google Scholar] [CrossRef] [PubMed]
- Kebapcilar, A.G.; Kulaksizoglu, M.; Ipekci, S.H.; Korkmaz, H.; Kebapcilar, L.; Akyurek, F.; Taner, C.E.; Gonen, M.S. Relationship between mean platelet volume and low-grade systemic coagulation with vitamin D deficiency in primary ovarian insufficiency. Arch. Gynecol. Obstet. 2013, 288, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Verdoia, M.; Pergolini, P.; Rolla, R.; Sartori, C.; Nardin, M.; Schaffer, A.; Barbieri, L.; Daffara, V.; Marino, P.; Bellomo, G.; et al. Vitamin D levels and high-residual platelet reactivity in patients receiving dual antiplatelet therapy with clopidogrel or ticagrelor. Platelets 2016, 27, 576–582. [Google Scholar] [CrossRef]
- Giovannucci, E.; Liu, Y.; Hollis, B.W.; Rimm, E.B. 25-hydroxyvitamin D and risk of myocardial infarction in men: A prospective study. Arch. Intern. Med. 2008, 168, 1174–1180. [Google Scholar] [CrossRef] [Green Version]
- Ng, L.L.; Sandhu, J.K.; Squire, I.B.; Davies, J.E.; Jones, D.J. Vitamin D and prognosis in acute myocardial infarction. Int. J. Cardiol. 2013, 168, 2341–2346. [Google Scholar] [CrossRef]
- Wang, T.J.; Pencina, M.J.; Booth, S.L.; Jacques, P.F.; Ingelsson, E.; Lanier, K.; Benjamin, E.J.; D’Agostino, R.B.; Wolf, M.; Vasan, R.S. Vitamin D deficiency and risk of cardiovascular disease. Circulation 2008, 117, 503–511. [Google Scholar] [CrossRef] [Green Version]
- Selby, R. “TEG talk”: Expanding clinical roles for thromboelastography and rotational thromboelastometry. Hematol. Am. Soc. Hematol. Educ. Program 2020, 2020, 67–75. [Google Scholar] [CrossRef]
- Lu, B.C.; Shi, X.J.; Liang, L.; Dong, N.; Liu, Z.Z. Platelet Surface CD62p and Serum Vitamin D Levels are Associated with Clopidogrel Resistance in Chinese Patients with Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 1323–1328. [Google Scholar] [CrossRef]
- Verdoia, M.; Pergolini, P.; Rolla, R.; Nardin, M.; Schaffer, A.; Barbieri, L.; Daffara, V.; Marino, P.; Bellomo, G.; Suryapranata, H.; et al. Impact of high-dose statins on vitamin D levels and platelet function in patients with coronary artery disease. Thromb. Res. 2017, 150, 90–95. [Google Scholar] [CrossRef]
- Barbarawi, M.; Kheiri, B.; Zayed, Y.; Barbarawi, O.; Dhillon, H.; Swaid, B.; Yelangi, A.; Sundus, S.; Bachuwa, G.; Alkotob, M.L.; et al. Vitamin D Supplementation and Cardiovascular Disease Risks in More Than 83 000 Individuals in 21 Randomized Clinical Trials: A Meta-analysis. JAMA Cardiol. 2019, 4, 765–776. [Google Scholar] [PubMed]
- Quyyumi, A.A.; Al Mheid, I. The Demise of Vitamin D for Cardiovascular Prevention. JAMA Cardiol. 2019, 4, 776–777. [Google Scholar] [CrossRef] [PubMed]
- Scragg, R. Emerging Evidence of Thresholds for Beneficial Effects from Vitamin D Supplementation. Nutrients 2018, 10, 561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, A.; Selvanayagam, J.B.; Hyppönen, E. Non-linear Mendelian randomization analyses support a role for vitamin D deficiency in cardiovascular disease risk. Eur. Heart J. 2021, ehab809. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
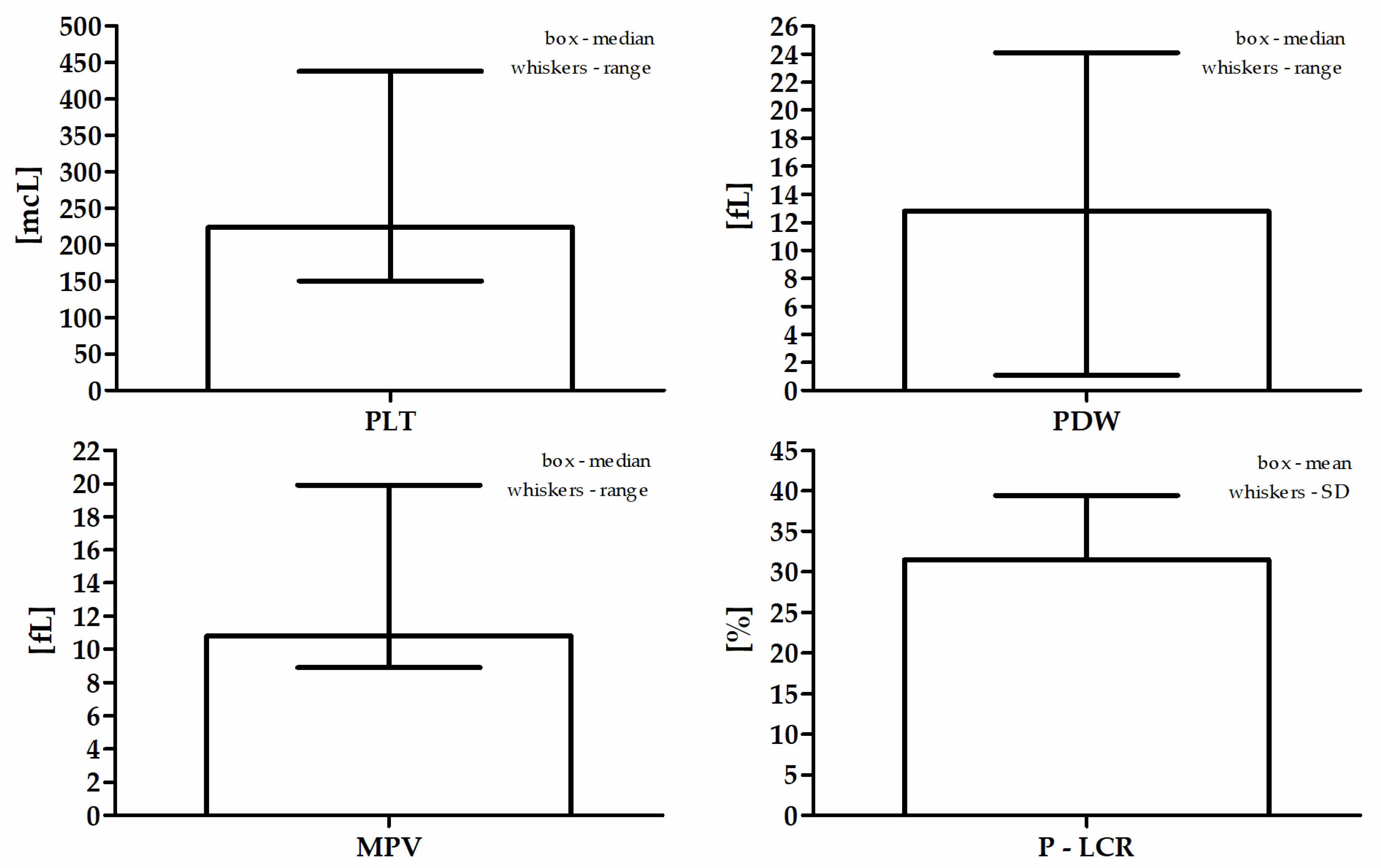
| Parameter | Values |
|---|---|
| PLT (mcL) a | 224 (150–438) |
| PDW (fL) a | 12.8 (1.1–24.1) |
| MPV (fL) a | 10.8 (8.9–19.9) |
| P-LCR (%) b | 31.5 ± 8.0 |
| Factor | Estimate | Wald Statistics | 95% CI | p-Value | |
|---|---|---|---|---|---|
| Cause of hospitalization | Sex | 0.42 | 5.74 | 0.08–0.76 | <0.05 |
| Age | −0.04 | 5.04 | −0.07–−0.004 | <0.05 | |
| BMI | 0.01 | 0.14 | −0.06–0.09 | 0.71 | |
| Diabetes mellitus | 6.26 | 383.3 | 5.63–6.88 | <0.001 | |
| Hyperlipidemia | −0.02 | 0.01 | −0.34–0.30 | 0.91 | |
| Hypertension | −0.28 | 1.63 | −0.72–0.15 | 0.20 | |
| Smoking | 0.88 | 9.92 | 0.33–1.42 | <0.01 | |
| CASSS | −0.06 | 0.04 | −0.62–0.50 | 0.84 | |
| Serum 25(OH)D | −0.01 | 0.09 | −0.05–0.03 | 0.76 | |
| Season during the examination | 0.05 | 0.06 | −0.31–0.41 | 0.80 | |
| MPV | −0.12 | 0.10 | −0.88–0.63 | 0.75 | |
| P-LCR | −0.02 | 0.09 | −0.11–0.08 | 0.76 |
| Variable | Stable CAD | ACS | p-Value |
|---|---|---|---|
| N | 108 | 160 | - |
| Sex (♀/♂) | 27/81 | 60/100 | <0.05 |
| Age (years) | 68.4 ± 9.4 | 66.1 ± 12.2 | 0.10 |
| BMI (kg/m2) | 27.7 ± 4.3 | 28.3 ± 4.6 | 0.34 |
| BMI class (1/2/3) * | 28/52/28 | 33/59/47 | 0.41 |
| Diabetes (no/yes/pre-diabetes) | 63/36/9 | 95/64/1 | <0.01 |
| TC (mg/dL) | 162.5 (84.8–327.3) | 171.9 (70.9–338.3) | 0.07 |
| HDL (mg/dL) | 46.5 (14.6–113.2) | 44.5 (19.5–92.9) | 0.11 |
| LDL (mg/dL) | 81.9 (27.3–257.9) | 101.4 (24.4–244.3) | <0.05 |
| TG (mg/dL) | 111.8 (37.9–417.0) | 115.4 (42.6–391.8) | 0.58 |
| Hyperlipidemia (no/yes) | 54/50 | 53/95 | <0.05 |
| Hypertension (no/yes) | 15/93 | 20/140 | 0.74 |
| Smoking (no/yes/ex-smokers) | 62/24/22 | 93/61/6 | <0.001 |
| CASSS (0/1/2/3) | 6/25/39/38 | 7/54/44/55 | 0.24 |
| Serum 25(OH)D (ng/mL) | 15.8 (4.0–46.9) | 13.1 (4.0–48.3) | <0.05 |
| Season of the examination(November to April/May to October) | 78/30 | 122/38 | 0.46 |
| Parameter | Stable CAD | MI | p-Value |
|---|---|---|---|
| PLT (mcL) | 216 (150–438) | 227 (150–432) | 0.20 |
| PDW (fL) | 12.9 (8.8–24.1) | 12.8 (1.1–20.0) | 0.24 |
| MPV (fL) | 10.9 (9.1–19.9) | 10.8 (8.9–13.3) | 0.32 |
| P-LCR (%) | 32.1 ± 8.3 | 31.0 ± 7.7 | 0.26 |
| Stable CAD | ACS | |
|---|---|---|
| PLT (mcL) | R = −0.07, p = 0.49 | R = −0.05, p = 0.53 |
| PDW (fL) | R = −0.11, p = 0.25 | R = −0.01, p = 0.89 |
| MPV (fL) | R = −0.13, p = 0.19 | R = −0.01, p = 0.86 |
| P-LCR (%) | R = −0.13, p = 0.18 | R = −0.04, p = 0.61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dziedzic, E.A.; Gąsior, J.S.; Sowińska, I.; Dąbrowski, M.; Jankowski, P. Vitamin D Level in Patients with Consecutive Acute Coronary Syndrome Is Not Correlated with the Parameters of Platelet Activity. J. Clin. Med. 2022, 11, 707. https://doi.org/10.3390/jcm11030707
Dziedzic EA, Gąsior JS, Sowińska I, Dąbrowski M, Jankowski P. Vitamin D Level in Patients with Consecutive Acute Coronary Syndrome Is Not Correlated with the Parameters of Platelet Activity. Journal of Clinical Medicine. 2022; 11(3):707. https://doi.org/10.3390/jcm11030707
Chicago/Turabian StyleDziedzic, Ewelina A., Jakub S. Gąsior, Izabela Sowińska, Marek Dąbrowski, and Piotr Jankowski. 2022. "Vitamin D Level in Patients with Consecutive Acute Coronary Syndrome Is Not Correlated with the Parameters of Platelet Activity" Journal of Clinical Medicine 11, no. 3: 707. https://doi.org/10.3390/jcm11030707
APA StyleDziedzic, E. A., Gąsior, J. S., Sowińska, I., Dąbrowski, M., & Jankowski, P. (2022). Vitamin D Level in Patients with Consecutive Acute Coronary Syndrome Is Not Correlated with the Parameters of Platelet Activity. Journal of Clinical Medicine, 11(3), 707. https://doi.org/10.3390/jcm11030707