
Assessment of the Risk of Nodal Involvement in Rectal Neuroendocrine Neoplasms: The NOVARA Score, a Multicentre Retrospective Study


 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
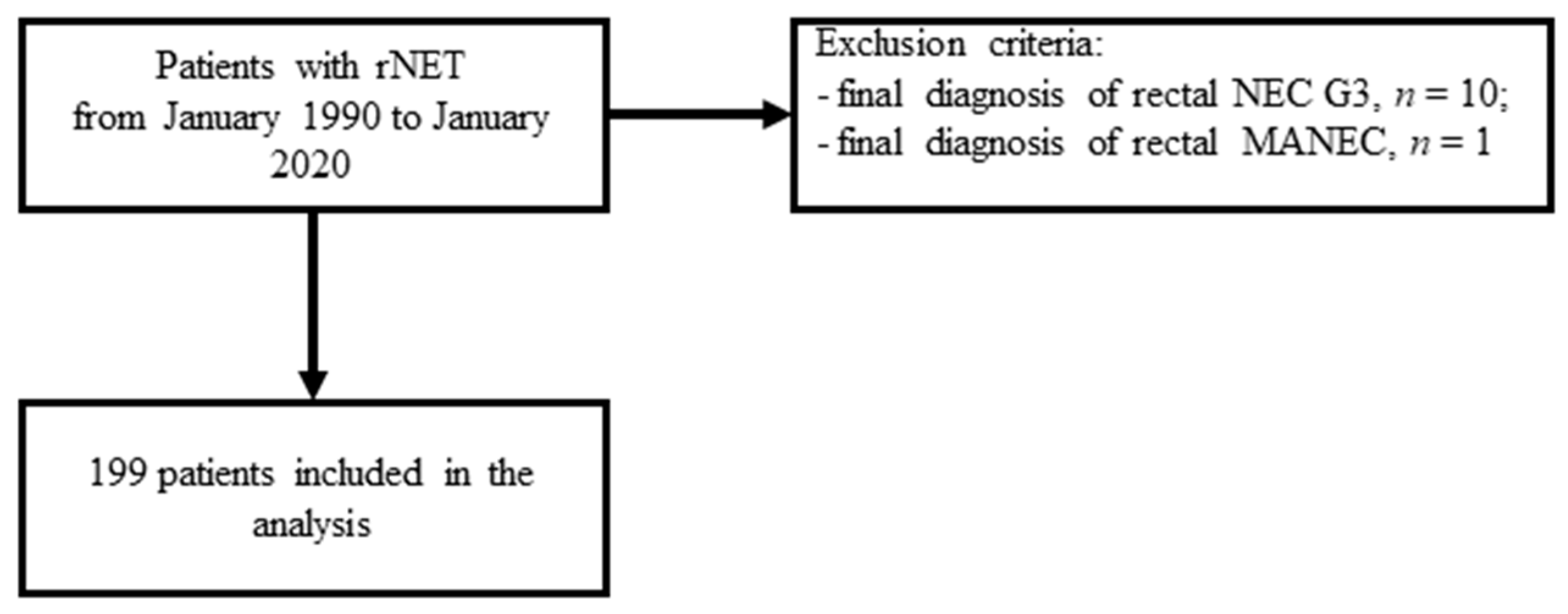
2.1. Study Design and Participants
2.2. Data Collection
2.3. Pathology Assessment
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. ROC Curves
3.3. Univariate Analysis, Multivariate Analysis, and Prognostic Score Development
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Modlin, I.M.; Lye, K.D.; Kidd, M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer 2003, 97, 934–959. [Google Scholar] [CrossRef] [PubMed]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Basuroy, R.; Haji, A.; Ramage, J.K.; Quaglia, A.; Srirajaskanthan, R. Review article: The investigation and management of rectal neuroendocrine tumours. Aliment. Pharmacol. Ther. 2016, 44, 332–345. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.N.; Sohn, D.K.; Hong, C.W.; Han, K.S.; Chang, H.J.; Jung, K.H.; Lim, S.-B.; Choi, H.S.; Jeong, S.-Y.; Park, J.-G. Atypical endoscopic features can be associated with metastasis in rectal carcinoid tumors. Surg. Endosc. 2008, 22, 1992–1996. [Google Scholar] [CrossRef] [PubMed]
- Ramage, J.K.; De Herder, W.W.; Delle Fave, G.; Ferolla, P.; Ferone, D.; Ito, T.; Ruszniewski, P.; Sundin, A.; Weber, W.; Zheng-Pei, Z.; et al. ENETS Consensus Guidelines update for colorectal neuroendocrine neoplasms. Neuroendocrinology 2016, 103, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Pagano, N.; Ricci, C.; Brighi, N.; Ingaldi, C.; Pugliese, F.; Santini, D.; Campana, D.; Mosconi, C.; Ambrosini, V.; Casadei, R. Incidental diagnosis of very small rectal neuroendocrine neoplasms: When should endoscopic submucosal dissection be performed? A single ENETS centre experience. Endocrine 2019, 65, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Chablaney, S.; Zator, Z.A.; Kumta, N.A. Diagnosis and management of rectal neuroendocrine tumors. Clin. Endosc. 2017, 50, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Bertani, E.; Ravizza, D.; Milione, M.; Massironi, S.; Grana, C.M.; Zerini, D.; Piccioli, A.N.; Spinoglio, G.; Fazio, N. Neuroendocrine neoplasms of rectum: A management update. Cancer Treat. Rev. 2018, 66, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Maione, F.; Chini, A.; Milone, M.; Gennarelli, N.; Manigrasso, M.; Maione, R.; Cassese, G.; Pagano, G.; Tropeano, F.P.; Luglio, G.; et al. Diagnosis and management of rectal neuroendocrine tumors (NETs). Diagnostics 2021, 11, 771. [Google Scholar] [CrossRef]
- Al Natour, R.H.; Saund, M.S.; Sanchez, V.M.; Whang, E.E.; Sharma, A.M.; Huang, Q.; Boosalis, V.A.; Gold, J.S. Tumor size and depth predict rate of lymph node metastasis in colon carcinoids and can be used to select patients for endoscopic resection. J. Gastrointest. Surg. 2012, 16, 595–602. [Google Scholar] [CrossRef]
- Weinstock, B.; Ward, S.C.; Harpaz, N.; Warner, R.R.P.; Itzkowitz, S.; Kim, M.K. Clinical and prognostic features of rectal neuroendocrine tumors. Neuroendocrinology 2013, 98, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Sohn, B.; Kwon, Y.; Ryoo, S.-B.; Song, I.; Kwon, Y.-H.; Lee, D.W.; Moon, S.H.; Park, J.W.; Jeong, S.-Y.; Park, K.J. Predictive factors for lymph node metastasis and prognostic factors for survival in rectal neuroendocrine tumors. J. Gastrointest. Surg. 2017, 21, 2066–2074. [Google Scholar] [CrossRef] [PubMed]
- Chida, K.; Watanabe, J.; Hirasawa, K.; Inayama, Y.; Misumi, T.; Kunisaki, C.; Endo, I. A novel risk-scoring system for predicting lymph node metastasis of rectal neuroendocrine tumors. Ann. Gastroenterol. Surg. 2020, 4, 562–570. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, Y.; Lin, H.; Xu, M.; Zhou, X.; Zhuang, J.; Yang, Y.; Chen, B.; Liu, X.; Guan, G. Risk factors for lymph node metastasis in rectal neuroendocrine tumors: A recursive partitioning analysis based on multicenter data. J. Surg. Oncol. 2021, 124, 1098–1105. [Google Scholar] [CrossRef] [PubMed]
- Schmoll, H.J.; Van Cutsem, E.; Stein, A.; Valentini, V.; Glimelius, B.; Haustermans, K.; Nordlinger, B.; van de Velde, C.J.; Balmana, J.; Regula, J.; et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann. Oncol. 2012, 23, 2479–2516. [Google Scholar] [CrossRef]
- Bosman, F.T.; Carneiro, F.; Hruban, R.H.; Theise, N.D. WHO classification of tumours of the digestive system. In WHO Classification of Tumours of the Digestive System; World Health Organization: Geneva, Switzerland, 2010; ISBN 9789283224327. [Google Scholar]
- Rindi, G.; Klöppel, G.; Couvelard, A.; Komminoth, P.; Körner, M.; Lopes, J.M.; McNicol, A.-M.; Nilsson, O.; Perren, A.; Scarpa, A.; et al. TNM staging of midgut and hindgut (neuro) endocrine tumors: A consensus proposal including a grading system. Virchows Arch. 2007, 451, 757–762. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.S.; Chen, L.-T.; Shan, Y.-S.; Chu, P.-Y.; Tsai, C.-R.; Tsai, H.-J. An updated analysis of the epidemiologic trends of neuroendocrine tumors in Taiwan. Sci. Rep. 2021, 11, 7881. [Google Scholar] [CrossRef]
- Konishi, T.; Watanabe, T.; Kishimoto, J.; Kotake, K.; Muto, T.; Nagawa, H. Japanese Society for Cancer of the Colon and Rectum Prognosis and risk factors of metastasis in colorectal carcinoids: Results of a nationwide registry over 15 years. Gut 2007, 56, 863–868. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Xie, H.; Xie, L.; Li, J.; Fu, W. Factors associated with lymph node metastasis in radically resected rectal carcinoids: A systematic review and meta-analysis. J. Gastrointest. Surg. 2013, 17, 1689–1697. [Google Scholar] [CrossRef]
- Sugimoto, S.; Hotta, K.; Shimoda, T.; Imai, K.; Yamaguchi, Y.; Nakajima, T.; Oishi, T.; Mori, K.; Takizawa, K.; Kakushima, N.; et al. The Ki-67 labeling index and lymphatic/venous permeation predict the metastatic potential of rectal neuroendocrine tumors. Surg. Endosc. 2016, 30, 4239–4248. [Google Scholar] [CrossRef]
- McConnell, Y.J. Surgical management of rectal carcinoids: Trends and outcomes from the Surveillance, Epidemiology, and End Results database (1988 to 2012). Am. J. Surg. 2016, 211, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Wang, Z.; Zheng, Z.; Bi, J.; Wang, X.; Feng, Q. Risk factors for lymph node metastasis and survival outcomes in colorectal neuroendocrine tumors. Cancer Manag. Res. 2020, 12, 7151–7164. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Liu, Z.; Wen, Z.; Li, R.; An, K.; Mei, S.; Chen, J.; Shen, H.; Li, J.; Zhao, F.; et al. Evaluation of radical surgical treatment in the management of 58 locally advanced rectal neuroendocrine neoplasms, one multicenter retrospective study. Eur. J. Surg. Oncol. 2021, 47, 3166–3174. [Google Scholar] [CrossRef] [PubMed]
- Son, J.; Park, I.J.; Yang, D.-H.; Kim, J.; Kim, K.-J.; Byeon, J.-S.; Hong, S.M.; Kim, Y.I.; Kim, J.B.; Lim, S.-B.; et al. Oncological outcomes according to the treatment modality based on the size of rectal neuroendocrine tumors: A single-center retrospective study. Surg. Endosc. 2021. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Takahashi, K.; Yamada, K.; Bando, H.; Baba, H.; Ito, M.; Funahashi, K.; Ueno, H.; Fujita, S.; Hasegawa, S.; et al. A nationwide, multi-institutional collaborative retrospective study of colorectal neuroendocrine tumors in Japan. Ann. Gastroenterol. Surg. 2021, 5, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Nam, S.-J.; Kim, B.C.; Chang, H.J.; Jeon, H.H.; Kim, J.; Kim, S.Y. Risk factors for lymph node metastasis and oncologic outcomes in small rectal neuroendocrine tumors with lymphovascular invasion. Gut Liver ahead of print. 2021. [Google Scholar] [CrossRef] [PubMed]
- Sappenfield, R.; Gonzalez, I.A.; Cao, D.; Chatterjee, D. Well-differentiated rectal neuroendocrine tumors: Analysis of histology, including insulinoma-associated protein 1 expression, and biologic behavior, involving a large cohort of 94 cases. Hum. Pathol. 2020, 104, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.H.; Goldner, W.S.; Benson, A.B.; Bergsland, E.; Blaszkowsky, L.S.; Brock, P.; Chan, J.; Das, S.; Dickson, P.V.; Fanta, P.; et al. Neuroendocrine and adrenal tumors, version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 839–868. [Google Scholar] [CrossRef] [PubMed]
- Maione, F.; Chini, A.; Aprea, G.; Dinuzzi, V.P.; De Palma, G.D. Indication and results of endoscopic submucosal dissection for right located lateral spreading tumors. Ann. Laparosc. Endosc. Surg. 2021, 6, 2518. [Google Scholar] [CrossRef]
- Caplin, M.; Sundin, A.; Nillson, O.; Baum, R.P.; Klose, K.J.; Kelestimur, F.; Plöckinger, U.; Papotti, M.; Salazar, R.; Pascher, A.; et al. ENETS Consensus Guidelines for the management of patients with digestive neuroendocrine neoplasms: Colorectal neuroendocrine neoplasms. Neuroendocrinology 2012, 95, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Concors, S.J.; Sinnamon, A.J.; Folkert, I.W.; Mahmoud, N.N.; Fraker, D.L.; Carter Paulson, E.; Roses, R.E. Predictors of metastases in rectal neuroendocrine tumors: Results of a national cohort study. Dis. Colon Rectum 2018, 61, 1372–1379. [Google Scholar] [CrossRef] [PubMed]
- Ngamruengphong, S.; Kamal, A.; Akshintala, V.; Hajiyeva, G.; Hanada, Y.; Chen, Y.I.; Sanaei, O.; Fluxa, D.; Haito Chavez, Y.; Kumbhari, V.; et al. Prevalence of metastasis and survival of 788 patients with T1 rectal carcinoid tumors. Gastrointest. Endosc. 2019, 89, 602–606. [Google Scholar] [CrossRef] [PubMed]
- Gamboa, A.C.; Liu, Y.; Lee, R.M.; Zaidi, M.Y.; Staley, C.A.; Russell, M.C.; Cardona, K.; Sullivan, P.S.; Maithel, S.K. A novel preoperative risk score to predict lymph node positivity for rectal neuroendocrine tumors: An NCDB analysis to guide operative technique. J. Surg. Oncol. 2019, 120, 932–939. [Google Scholar] [CrossRef] [PubMed]
- Fine, C.; Roquin, G.; Terrebonne, E.; Lecomte, T.; Coriat, R.; Do Cao, C.; de Mestier, L.; Coffin, E.; Cadiot, G.; Nicolli, P.; et al. Endoscopic management of 345 small rectal neuroendocrine tumours: A national study from the French group of endocrine tumours (GTE). United Eur. Gastroenterol. J. 2019, 7, 1102–1112. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.S.; Kwon, M.J.; Kim, T.H.; Han, J.; Ju, Y.S. Lymphovascular invasion as a prognostic value in small rectal neuroendocrine tumor treated by local excision: A systematic review and meta-analysis. Pathol. Res. Pract. 2019, 215, 152642. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.H.; Jung, D.H.; Kim, J.H.; Youn, Y.H.; Park, H.; Park, J.J.; Um, Y.J.; Park, S.J.; Cheon, J.H.; Il Kim, T.; et al. Long-term outcomes according to additional treatments after endoscopic resection for rectal small neuroendocrine tumors. Sci. Rep. 2019, 9, 4911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, M.J.; Kang, H.S.; Soh, J.S.; Lim, H.; Kim, J.H.; Park, C.K.; Park, H.-R.; Nam, E.S. Lymphovascular invasion in more than one-quarter of small rectal neuroendocrine tumors. World J. Gastroenterol. 2016, 22, 9400–9410. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients (n = 199) |
|---|---|
| Demographic | |
| Gender, male No. (%) | 105 (52.8%) |
| Gender, female No. (%) | 90 (47.2%) |
| Age, median (IQR), years | 55 (46–62) |
| Presence of symptoms | |
| Yes (%) | 66 (33.1%) |
| No (%) | 121 (60.8%) |
| Not available (%) | 12 (6.1%) |
| TNM staging | |
| Stage I-IIA (%) | 181 (91.0%) |
| Stage IIIB-IV (%) | 21 (9.0%) |
| Site | |
| High/medium rectum (%) | 111 (55.8%) |
| Low rectum (%) | 72 (36.2%) |
| Not available (%) | 16 (8.0%) |
| Resection | |
| Polypectomy (%) | 125 (62.8%) |
| EMR (%) | 22 (11.1%) |
| ESD (%) | 14 (7.0%) |
| TEMS (%) | 8 (4.0%) |
| LAR (%) | 12 (6.0%) |
| Not available (%) | 18 (9.1%) |
| Pathological features | |
| Size, median (IQR), mm | 6 (3.0–9.25) |
| Ulceration (%) | 18 (9.0%) |
| Depression (%) | 16 (8.0%) |
| Synchronous lesions (%) | 13 (6.5%) |
| Vascular invasion (%) | 16 (8.0%) |
| Perineural invasion (%) | 11 (5.5%) |
| Lymphatic invasion (%) | 11 (5.5%) |
| WHO 2010 Classification | |
| NET G1 (%) | 147 (73.9%) |
| NET G2 (%) | 41 (20.6%) |
| Not available (%) | 11 (5.5%) |
| Ki-67, median (%) | 1% (1–2%) |
| Nodal involvement | |
| Yes (%) | 18 (9.0%) |
| No (%) | 141 (70.9%) |
| Not available (%) | 40 (20.1%) |
| Characteristics | Multivariate Analysis | ||
|---|---|---|---|
| OR | IC 95% | p | |
| Size > 11.5 mm | 54.9 | 4.2–711.0 | 0.002 |
| Ki67 > 3.5% | - | - | ns |
| Muscle layer invasion | - | - | ns |
| Vascular invasion | 51.3 | 2.9–906.7 | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricci, A.D.; Pusceddu, S.; Panzuto, F.; Gelsomino, F.; Massironi, S.; De Angelis, C.G.; Modica, R.; Ricco, G.; Torchio, M.; Rinzivillo, M.; et al. Assessment of the Risk of Nodal Involvement in Rectal Neuroendocrine Neoplasms: The NOVARA Score, a Multicentre Retrospective Study. J. Clin. Med. 2022, 11, 713. https://doi.org/10.3390/jcm11030713
Ricci AD, Pusceddu S, Panzuto F, Gelsomino F, Massironi S, De Angelis CG, Modica R, Ricco G, Torchio M, Rinzivillo M, et al. Assessment of the Risk of Nodal Involvement in Rectal Neuroendocrine Neoplasms: The NOVARA Score, a Multicentre Retrospective Study. Journal of Clinical Medicine. 2022; 11(3):713. https://doi.org/10.3390/jcm11030713
Chicago/Turabian StyleRicci, Angela Dalia, Sara Pusceddu, Francesco Panzuto, Fabio Gelsomino, Sara Massironi, Claudio Giovanni De Angelis, Roberta Modica, Gianluca Ricco, Martina Torchio, Maria Rinzivillo, and et al. 2022. "Assessment of the Risk of Nodal Involvement in Rectal Neuroendocrine Neoplasms: The NOVARA Score, a Multicentre Retrospective Study" Journal of Clinical Medicine 11, no. 3: 713. https://doi.org/10.3390/jcm11030713