
Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) in Non-Traumatic Cardiac Arrest: A Narrative Review of Known and Potential Physiological Effects

 , ,
, , {kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. REBOA in Non-Traumatic Cardiac Arrest
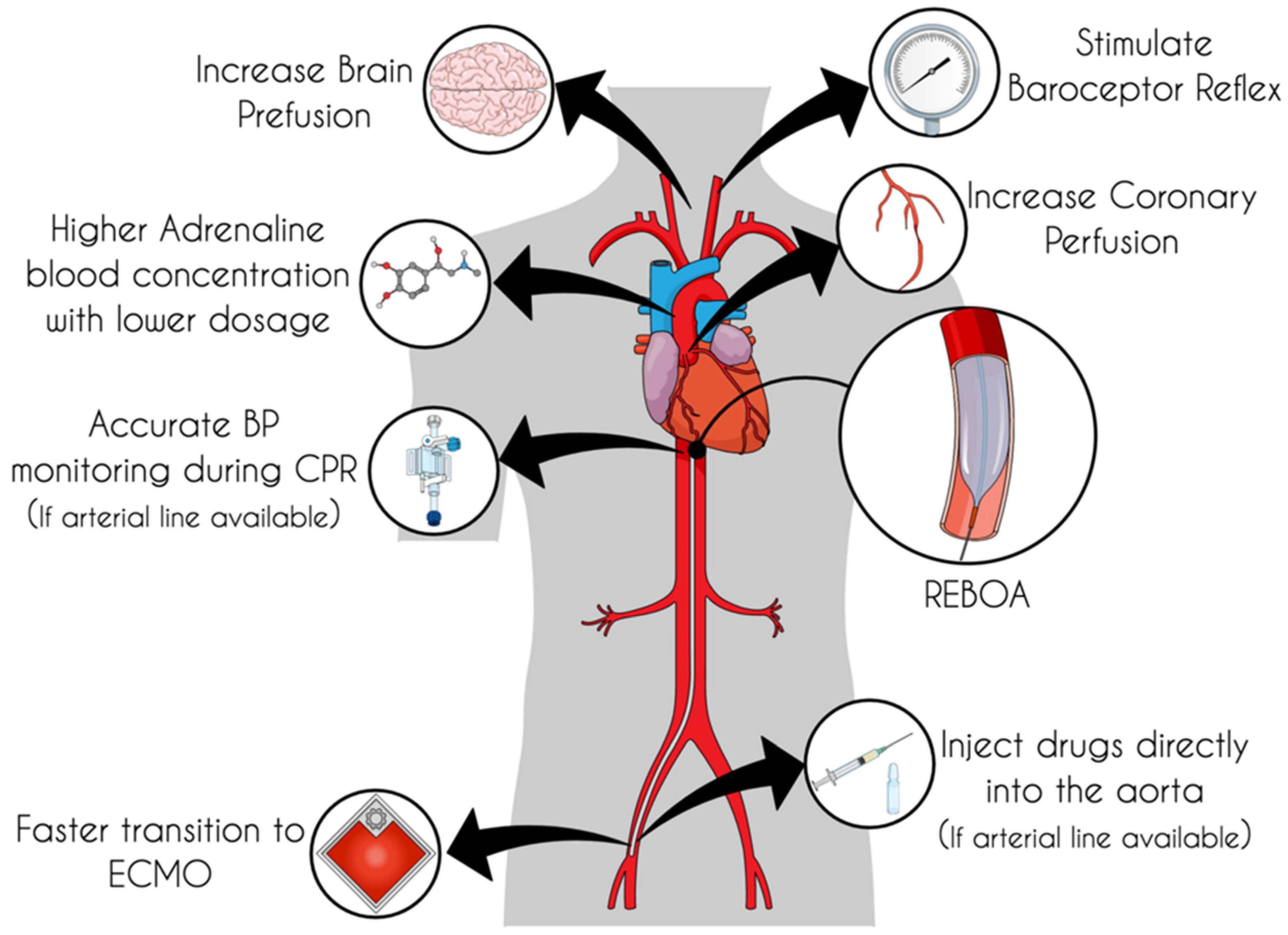
4. Physiological Effects of REBOA in Non-Traumatic Cardiac Arrest
Coronary Perfusion
5. Potential Effects of REBOA in Non-Traumatic Cardiac Arrest
5.1. Baroreceptor Reflex
5.2. Adrenaline Blood Concentration
6. Pitfalls and Caveats
7. Discussions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Petrone, P.; Pérez-Jiménez, A.; Rodríguez-Perdomo, M.; Brathwaite, C.E.M.; Joseph, D.K. Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) in the Management of Trauma Patients: A Systematic Literature Review. Am. Surg. 2019, 85, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Lott, C.; Truhlář, A.; Alfonzo, A.; Barelli, A.; González-Salvado, V.; Hinkelbein, J.; Nolan, J.P.; Paal, P.; Perkins, G.D.; Thies, K.C.; et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation 2021, 161, 152–219. [Google Scholar] [CrossRef] [PubMed]
- Van der Burg, B.B.; Kessel, B.; DuBose, J.J.; Hörer, T.M.; Hoencamp, R. Consensus on resuscitative endovascular balloon occlusion of the Aorta: A first consensus paper using a Delphi method. Injury 2019, 50, 1186–1191. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Hsu, C.H. The who, where, and when of REBOA for refractory out-of-hospital cardiac arrest. Resuscitation 2021, 165, 179–181. [Google Scholar] [CrossRef]
- Klee, T.E.; Kern, K.B. A review of ECMO for cardiac arrest. Resusc. Plus 2021, 5, 100083. [Google Scholar] [CrossRef]
- Oude Lansink-Hartgring, A.; van Minnen, O.; Vermeulen, K.M.; van den Bergh, W.M.; Oude Lansink-Hartgring, A.; Vermeulen, K.M.; Dos Reis Miranda, D.; Delnoij, T.S.R.; Elzo Kraemer, C.V.; Maas, J.J.; et al. Hospital Costs of Extracorporeal Membrane Oxygenation in Adults: A Systematic Review. Pharm.—Open 2021, 5, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Brede, J.R.; Lafrenz, T.; Klepstad, P.; Skjærseth, E.A.; Nordseth, T.; Søvik, E.; Krüger, A.J. Feasibility of Pre-Hospital Resuscitative Endovascular Balloon Occlusion of the Aorta in Non-Traumatic Out-of-Hospital Cardiac Arrest. J. Am. Heart Assoc. 2019, 8, e014394. [Google Scholar] [CrossRef] [PubMed]
- Daley, J.; Morrison, J.J.; Sather, J.; Hile, L. The role of resuscitative endovascular balloon occlusion of the aorta (REBOA) as an adjunct to ACLS in non-traumatic cardiac arrest. Am. J. Emerg. Med. 2017, 35, 731–736. [Google Scholar] [CrossRef]
- Levis, A.; Greif, R.; Hautz, W.E.; Lehmann, L.E.; Hunziker, L.; Fehr, T.; Haenggi, M. Resuscitative endovascular balloon occlusion of the aorta (REBOA) during cardiopulmonary resuscitation: A pilot study. Resuscitation 2020, 156, 27–34. [Google Scholar] [CrossRef]
- Gamberini, L.; Coniglio, C.; Lupi, C.; Tartaglione, M.; Mazzoli, C.A.; Baldazzi, M.; Cecchi, A.; Ferri, E.; Chiarini, V.; Semeraro, F.; et al. Resuscitative endovascular occlusion of the aorta (REBOA) for refractory out of hospital cardiac arrest. Utstein-Based Case Ser. Resusc. 2021, 165, 161–169. [Google Scholar] [CrossRef]
- Nowadly, C.D.; Johnson, M.A.; Hoareau, G.L.; Manning, J.E.; Daley, J.I. The use of resuscitative endovascular balloon occlusion of the aorta (REBOA) for non-traumatic cardiac arrest: A review. J. Am. Coll. Emerg. Physicians Open 2020, 1, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Berg, R.A.; Hilwig, R.W.; Ewy, G.A.; Kern, K.B. Precountershock cardiopulmonary resuscitation improves initial response to defibrillation from prolonged ventricular fibrillation: A randomized, controlled swine study. Crit. Care Med. 2004, 32, 1352–1357. [Google Scholar] [CrossRef] [PubMed]
- Wik, L.; Hansen, T.B.; Fylling, F.; Steen, T.; Vaagenes, P.; Auestad, B.H.; Steen, P.A. Delaying defibrillation to give basic cardiopulmonary resuscitation to patients with out-of-hospital ventricular fibrillation: A randomized trial. JAMA 2003, 289, 1389–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meaney, P.A.; Bobrow, B.J.; Mancini, M.E.; Christenson, J.; De Caen, A.R.; Bhanji, F.; Abella, B.S.; Kleinman, M.E.; Edelson, D.P.; Berg, R.A.; et al. Cardiopulmonary resuscitation quality: Improving cardiac resuscitation outcomes both inside and outside the hospital: A consensus statement from the American heart association. Circulation 2013, 128, 417–435. [Google Scholar] [CrossRef] [PubMed]
- Paradis, N.A.; Martin, G.B.; Rivers, E.P.; Goetting, M.G.; Appleton, T.J.; Feingold, M.; Nowak, R.M. Coronary perfusion pressure and the return of spontaneous circulation in human cardiopulmonary resuscitation. JAMA 1990, 263, 1106–1113. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, J.C.; Salcido, D.D.; Menegazzi, J.J. Coronary perfusion pressure and return of spontaneous circulation after prolonged cardiac arrest. Prehospital Emerg. Care Off. J. Natl. Assoc. EMS Physicians Natl. Assoc. State EMS Dir. 2010, 14, 78–84. [Google Scholar] [CrossRef] [Green Version]
- Paradis, N.A.; Martin, G.B.; Goetting, M.G.; Rosenberg, J.M.; Rivers, E.P.; Appleton, T.J.; Nowak, R.M. Simultaneous aortic, jugular bulb, and right atrial pressures during cardiopulmonary resuscitation in humans. Insights into mechanisms. Circulation 1989, 80, 361–368. [Google Scholar] [CrossRef] [Green Version]
- Khir, A.W.; Parker, K.H. Wave intensity in the ascending aorta: Effects of arterial occlusion. J. Biomech. 2005, 38, 647–655. [Google Scholar] [CrossRef]
- Stokland, O.; Miller, M.M.; Ilebekk, A.; Kiil, F. Mechanism of hemodynamic responses to occlusion of the descending thoracic aorta. Am. J. Physiol. Hear. Circ. Physiol. 1980, 7, 423–429. [Google Scholar] [CrossRef]
- Sesma, J.; Labandeira, J.; Sara, M.J.; Espila, J.L.; Arteche, A.; Saez, M.J. Effect of intra-aortic occlusion balloon in external thoracic compressions during CPR in pigs. Am. J. Emerg. Med. 2002, 20, 453–462. [Google Scholar] [CrossRef]
- Hutin, A.; Levy, Y.; Lidouren, F.; Kohlhauer, M.; Carli, P.; Ghaleh, B.; Lamhaut, L.; Tissier, R. Resuscitative endovascular balloon occlusion of the aorta vs epinephrine in the treatment of non-traumatic cardiac arrest in swine. Ann. Intensive Care 2021, 11, 81. [Google Scholar] [CrossRef] [PubMed]
- Olsen, M.H.; Olesen, N.D.; Karlsson, M.; Holmlöv, T.; Søndergaard, L.; Boutelle, M.; Mathiesen, T.; Møller, K. Randomized blinded trial of automated REBOA during CPR in a porcine model of cardiac arrest. Resuscitation 2021, 160, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Belz, G.G. Elastic properties and Windkessel function of the human aorta. Cardiovasc. Drugs Ther. 1995, 9, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Wieling, W.; Krediet, C.T.P.; Solari, D.; De Lange, F.J.; Van Dijk, N.; Thijs, R.D.; Van Dijk, J.G.; Brignole, M.; Jardine, D.L. At the heart of the arterial baroreflex: A physiological basis for a new classification of carotid sinus hypersensitivity. J. Intern. Med. 2013, 273, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Gilfoil, T.M. Effects of Sudden Aortic Occlusion on Heart Rate after Sino-Aortic Denervation. Circ. Res. 1958, 6, 501–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.; Qian, J.; Yao, W.; Wang, N.; Zhang, Z.; Cao, C.; Song, B.; Zhang, Z. Vagus nerve stimulation reverses ventricular electrophysiological changes induced by hypersympathetic nerve activity. Exp. Physiol. 2015, 100, 239–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brack, K.E.; Winter, J.; Ng, G.A. Mechanisms underlying the autonomic modulation of ventricular fibrillation initiation—Tentative prophylactic properties of vagus nerve stimulation on malignant arrhythmias in heart failure. Heart Fail. Rev. 2013, 18, 389–408. [Google Scholar] [CrossRef] [Green Version]
- St-John, W.M.; Paton, J.F.R. Respiratory-modulated neuronal activities of the rostral medulla which may generate gasping. Respir. Physiol. Neurobiol. 2003, 135, 97–101. [Google Scholar] [CrossRef]
- Van Harreveld, A.; Feigen, G.A.; Lerman, L.S. Hemodynamics of aortic occlusion. Am. J. Physiol. 1949, 157, 168–176. [Google Scholar] [CrossRef] [Green Version]
- Gelman, S.; Khazaeli, M.B.; Orr, R.; Henderson, T. Blood Volume Redistribution. Anesth. Analg. 1994, 78, 219–224. [Google Scholar] [CrossRef]
- Bender, A.D. Occlusion of the Thoracic Aorta and Abdominal Vena Cava. Arch. Surg. 1962, 84, 504. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Ji, C.; Deakin, C.D.; Quinn, T.; Nolan, J.P.; Scomparin, C.; Regan, S.; Long, J.; Slowther, A.; Pocock, H.; et al. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. N. Engl. J. Med. 2018, 379, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Mavroudis, C.D.; Ko, T.S.; Morgan, R.W.; Volk, L.E.; Landis, W.P.; Smood, B.; Xiao, R.; Hefti, M.; Boorady, T.W.; Marquez, A.; et al. Epinephrine’s effects on cerebrovascular and systemic hemodynamics during cardiopulmonary resuscitation. Crit. Care 2020, 24, 583. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro Junior, M.A.F.; Feng, C.Y.D.; Nguyen, A.T.M.; Rodrigues, V.C.; Bechara, G.E.K.; de-Moura, R.R.; Brenner, M. The complications associated with Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA). World J. Emerg. Surg. 2018, 13, 20. [Google Scholar] [CrossRef] [PubMed]
- Ordonez, C.A.; Nunez, R.M.; Parra, M.W.; Herrera Escobar, J.P.; Rodriguez, F.; Vidal, M.; Garcia, A.F.; Mejia, D.A.; Pino, L.L.; Puyana, J.C. Common Complications after the Use of Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA). J. Am. Coll. Surg. 2017, 225, S52–S53. [Google Scholar] [CrossRef] [Green Version]
- Davidson, A.J.; Russo, R.M.; Reva, V.A.; Brenner, M.L.; Moore, L.J.; Ball, C.; Bulger, E.; Fox, C.J.; DuBose, J.J.; Moore, E.E.; et al. The pitfalls of resuscitative endovascular balloon occlusion of the aorta: Risk factors and mitigation strategies. J. Trauma Acute Care Surg. 2018, 84, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, Y.; Matsumoto, J.; Kondo, H.; Idoguchi, K.; Ishida, T.; Kon, Y.; Tomita, K.; Ishida, K.; Hirose, T.; Umakoshi, K.; et al. Fewer REBOA complications with smaller devices and partial occlusion: Evidence from a multicentre registry in Japan. Emerg. Med. J. 2017, 34, 793–799. [Google Scholar] [CrossRef]
- Power, A.; Parekh, A.; Scallan, O.; Smith, S.; Novick, T.; Parry, N.; Moore, L. Size matters: First-in-human study of a novel 4 French REBOA device. Trauma Surg. Acute Care Open 2021, 6, e000617. [Google Scholar] [CrossRef]
- Madurska, M.J.; McLenithan, A.; Scalea, T.M.; Kundi, R.; White, J.M.; Morrison, J.J.; DuBose, J.J. A feasibility study of partial REBOA data in a high-volume trauma center. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2021. [Google Scholar] [CrossRef]
- Russo, R.M.; White, J.M.; Baer, D.G. Partial Resuscitative Endovascular Balloon Occlusion of the Aorta: A Systematic Review of the Preclinical and Clinical Literature. J. Surg. Res. 2021, 262, 101–114. [Google Scholar] [CrossRef]
- Matsumura, Y.; Higashi, A.; Izawa, Y.; Hishikawa, S.; Kondo, H.; Reva, V.; Oda, S.; Matsumoto, J. Organ ischemia during partial resuscitative endovascular balloon occlusion of the aorta: Dynamic 4D Computed tomography in swine. Sci. Rep. 2020, 10, 5680. [Google Scholar] [CrossRef] [PubMed]
- Marquez, A.M.; Morgan, R.W.; Ross, C.E.; Berg, R.A.; Sutton, R.M. Physiology-directed cardiopulmonary resuscitation: Advances in precision monitoring during cardiac arrest. Curr. Opin. Crit. Care 2018, 24, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Kim, F.; Maynard, C.; Dezfulian, C.; Sayre, M.; Kudenchuk, P.; Rea, T.; Sampson, D.; Olsufka, M.; May, S.; Nichol, G. Effect of Out-of-Hospital Sodium Nitrite on Survival to Hospital Admission after Cardiac Arrest: A Randomized Clinical Trial. JAMA J. Am. Med. Assoc. 2021, 325, 138–145. [Google Scholar] [CrossRef]
- Brede, J.R.; Skulberg, A.K.; Rehn, M.; Thorsen, K.; Klepstad, P.; Tylleskär, I.; Farbu, B.; Dale, J.; Nordseth, T.; Wiseth, R.; et al. REBOARREST, resuscitative endovascular balloon occlusion of the aorta in non-traumatic out-of-hospital cardiac arrest: A study protocol for a randomised, parallel group, clinical multicentre trial. Res. Sq. 2021, 1–9. [Google Scholar] [CrossRef]
- Engberg, M.; Lönn, L.; Konge, L.; Mikkelsen, S.; Hörer, T.; Lindgren, H.; Søvik, E.; Svendsen, M.B.; Frendnø, M.; Taudorf, M.; et al. Reliable and valid assessment of procedural skills in resuscitative endovascular balloon occlusion of the aorta (REBOA). J. Trauma Acute Care Surg. 2021, 91, 663–671. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzoli, C.A.; Chiarini, V.; Coniglio, C.; Lupi, C.; Tartaglione, M.; Gamberini, L.; Semeraro, F.; Gordini, G. Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) in Non-Traumatic Cardiac Arrest: A Narrative Review of Known and Potential Physiological Effects. J. Clin. Med. 2022, 11, 742. https://doi.org/10.3390/jcm11030742
Mazzoli CA, Chiarini V, Coniglio C, Lupi C, Tartaglione M, Gamberini L, Semeraro F, Gordini G. Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) in Non-Traumatic Cardiac Arrest: A Narrative Review of Known and Potential Physiological Effects. Journal of Clinical Medicine. 2022; 11(3):742. https://doi.org/10.3390/jcm11030742
Chicago/Turabian StyleMazzoli, Carlo Alberto, Valentina Chiarini, Carlo Coniglio, Cristian Lupi, Marco Tartaglione, Lorenzo Gamberini, Federico Semeraro, and Giovanni Gordini. 2022. "Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) in Non-Traumatic Cardiac Arrest: A Narrative Review of Known and Potential Physiological Effects" Journal of Clinical Medicine 11, no. 3: 742. https://doi.org/10.3390/jcm11030742