
Cholestatic Liver Disease and Pregnancy: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Inclusion Criteria
2.3. Study Exclusion Criteria
2.4. Quality Assessment of Included Studies
2.5. Outcomes
2.6. Definitions
2.7. Data Extraction
2.8. Statistical Analysis
3. Results
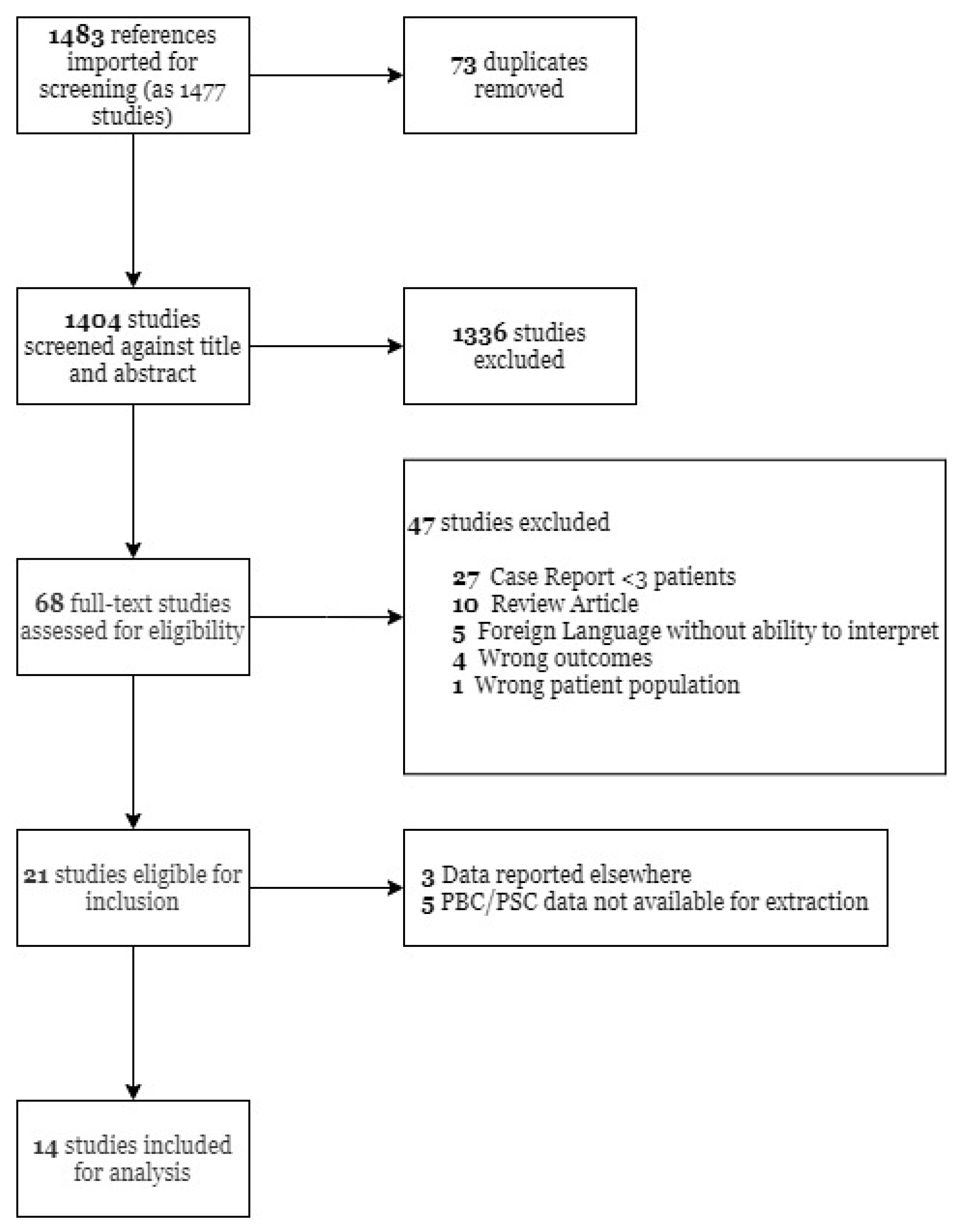
3.1. Study Research Results
3.2. Description of Included Studies
3.3. Maternal and Fetal Outcomes
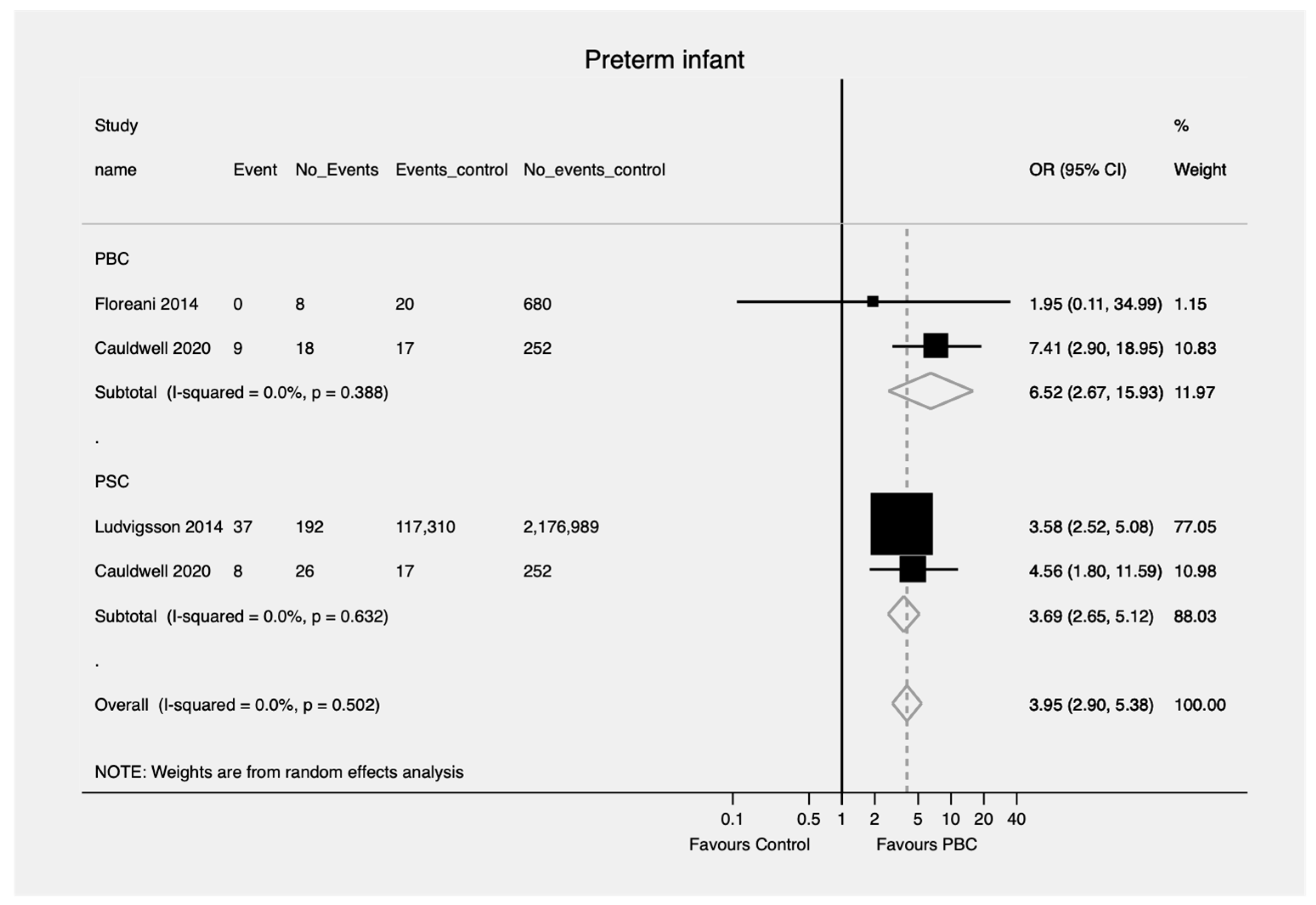
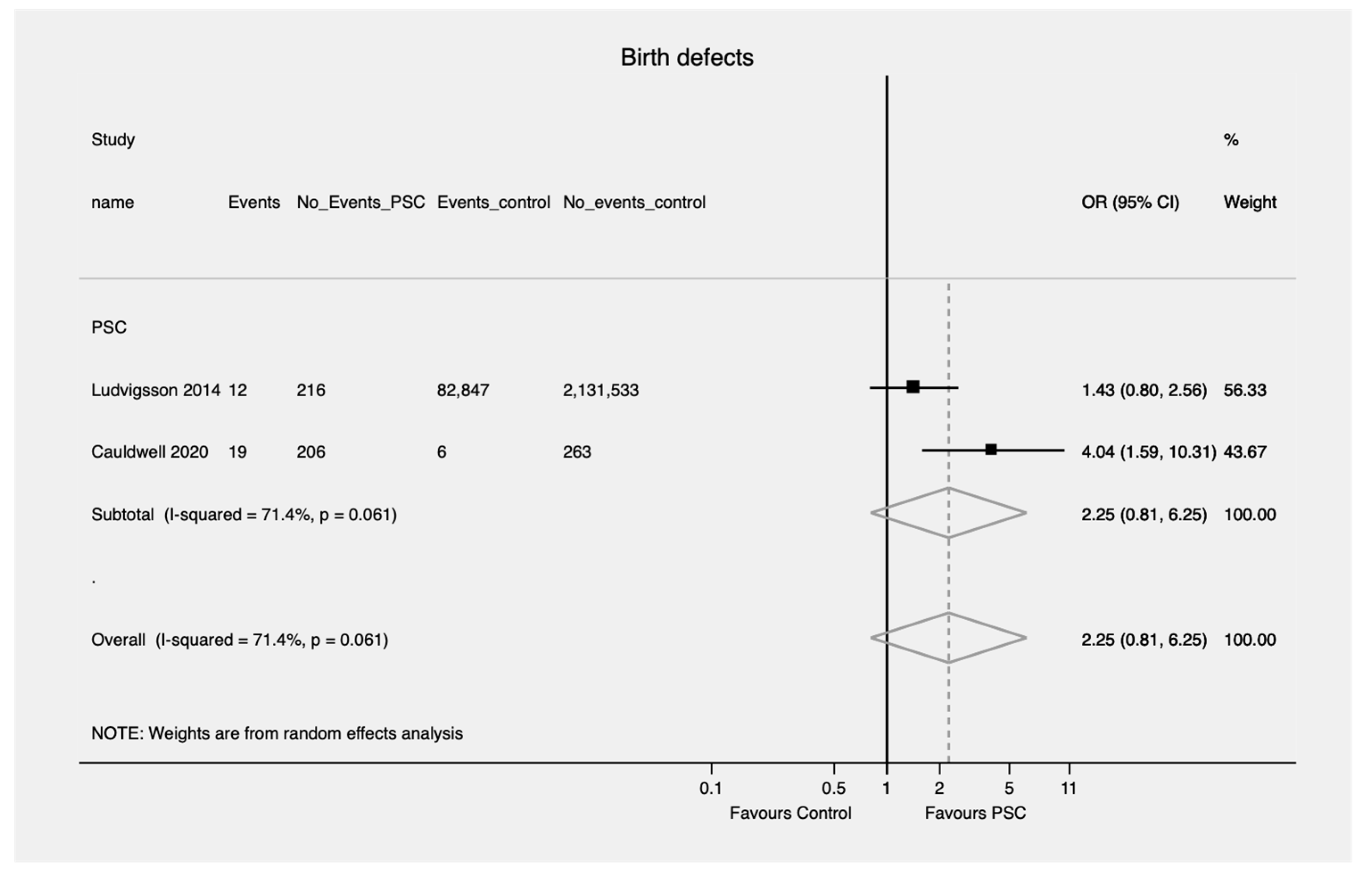
3.3.1. Fetal Outcomes
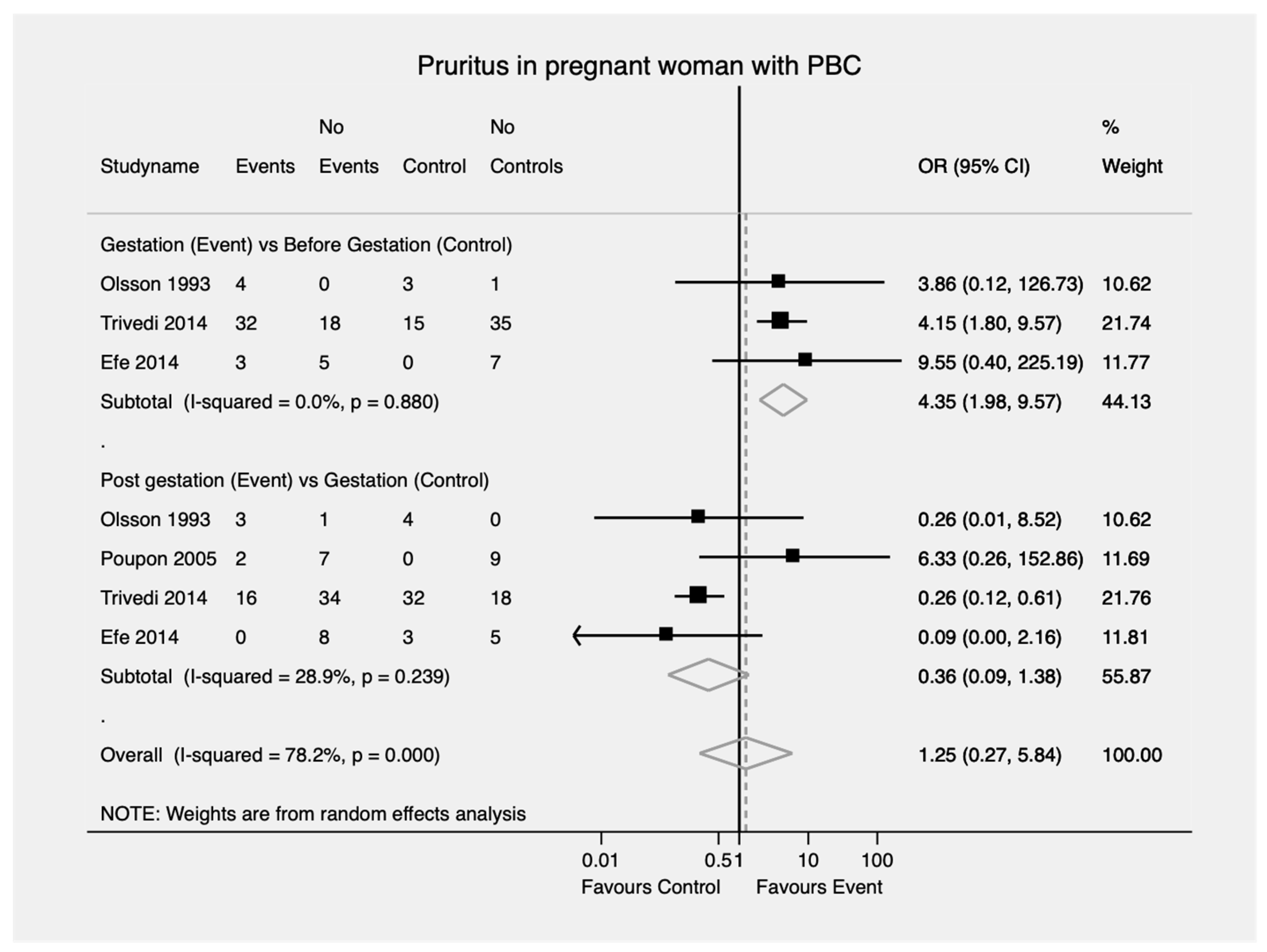
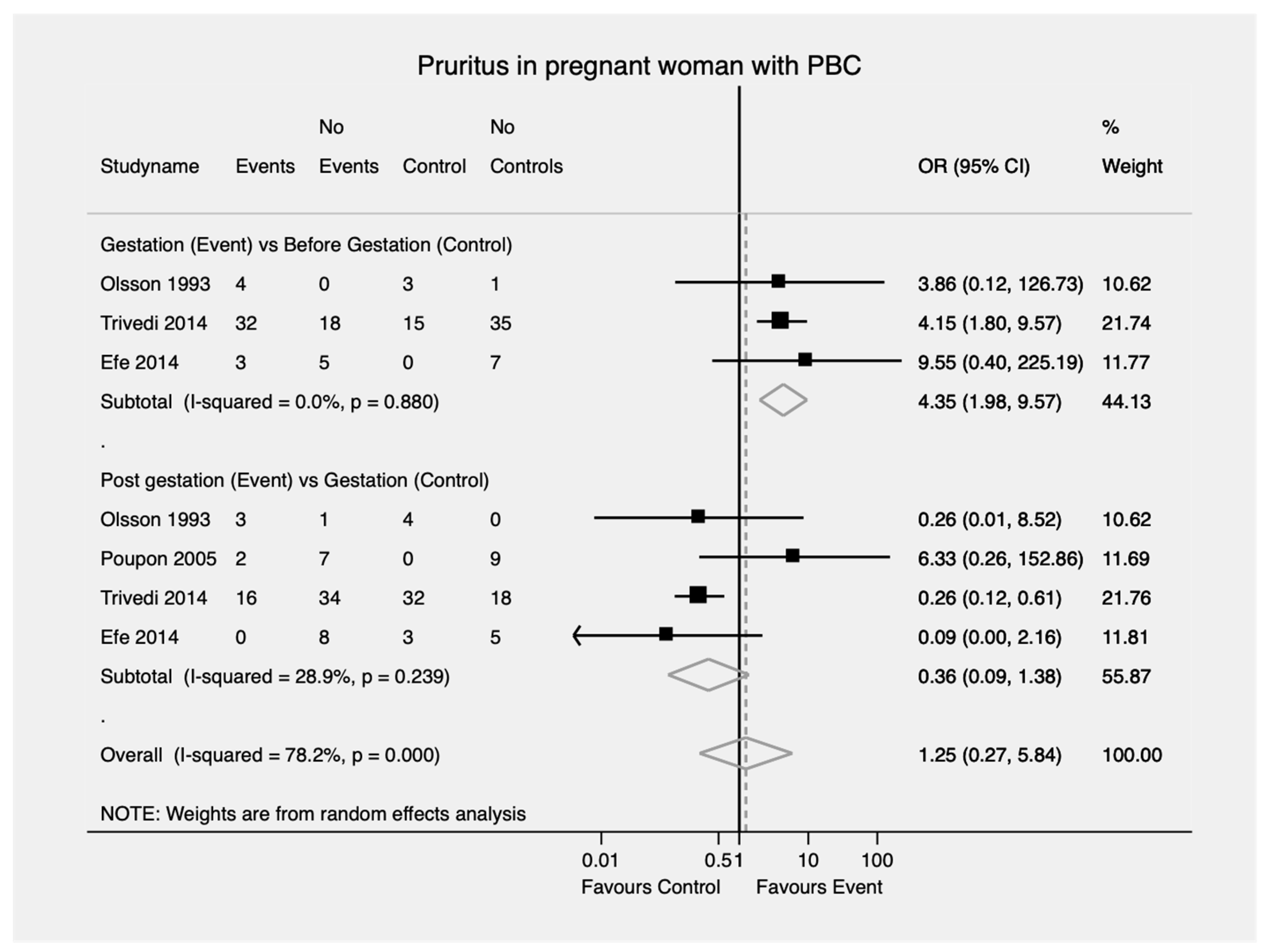
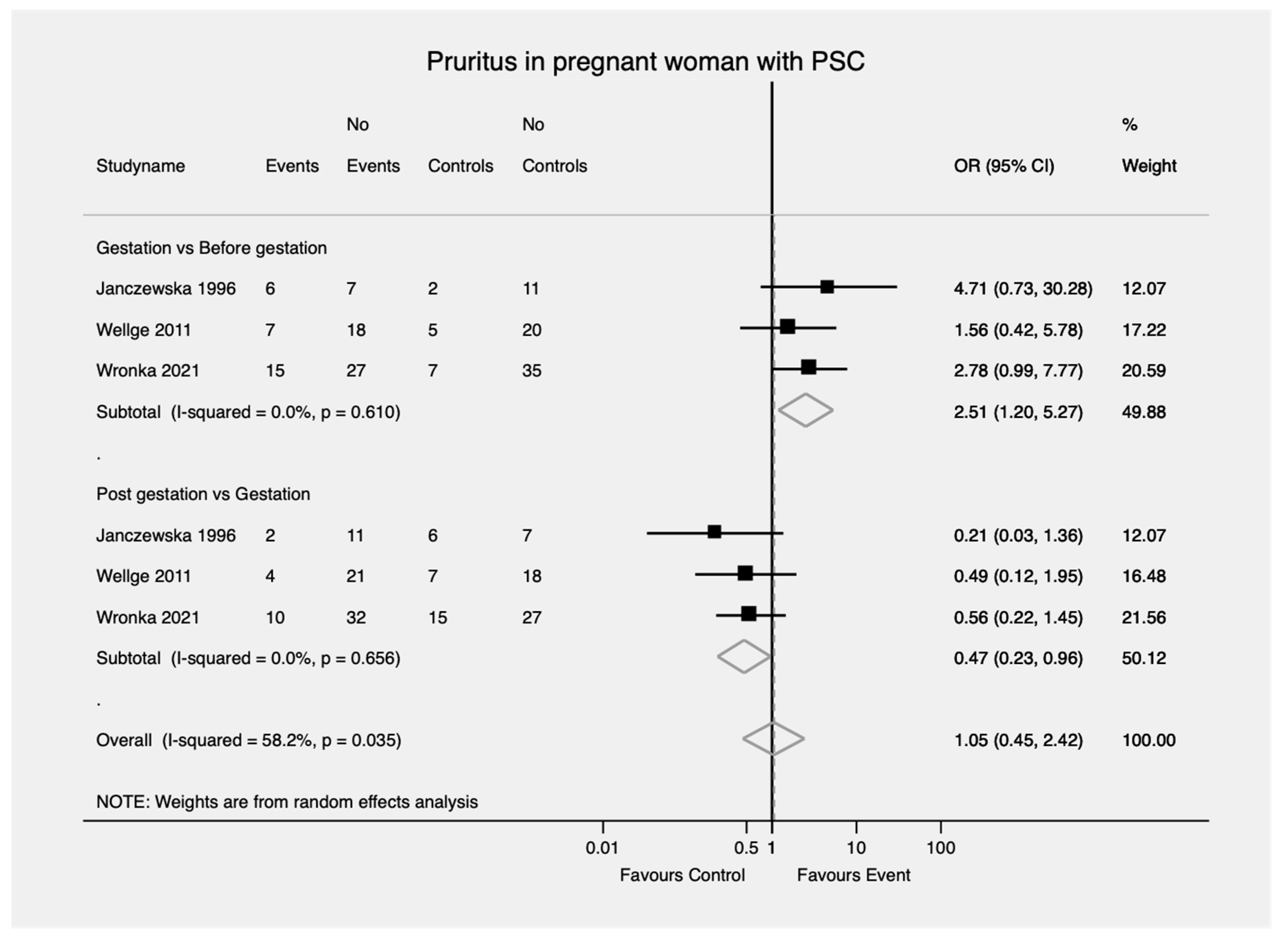
3.3.2. Pruritus
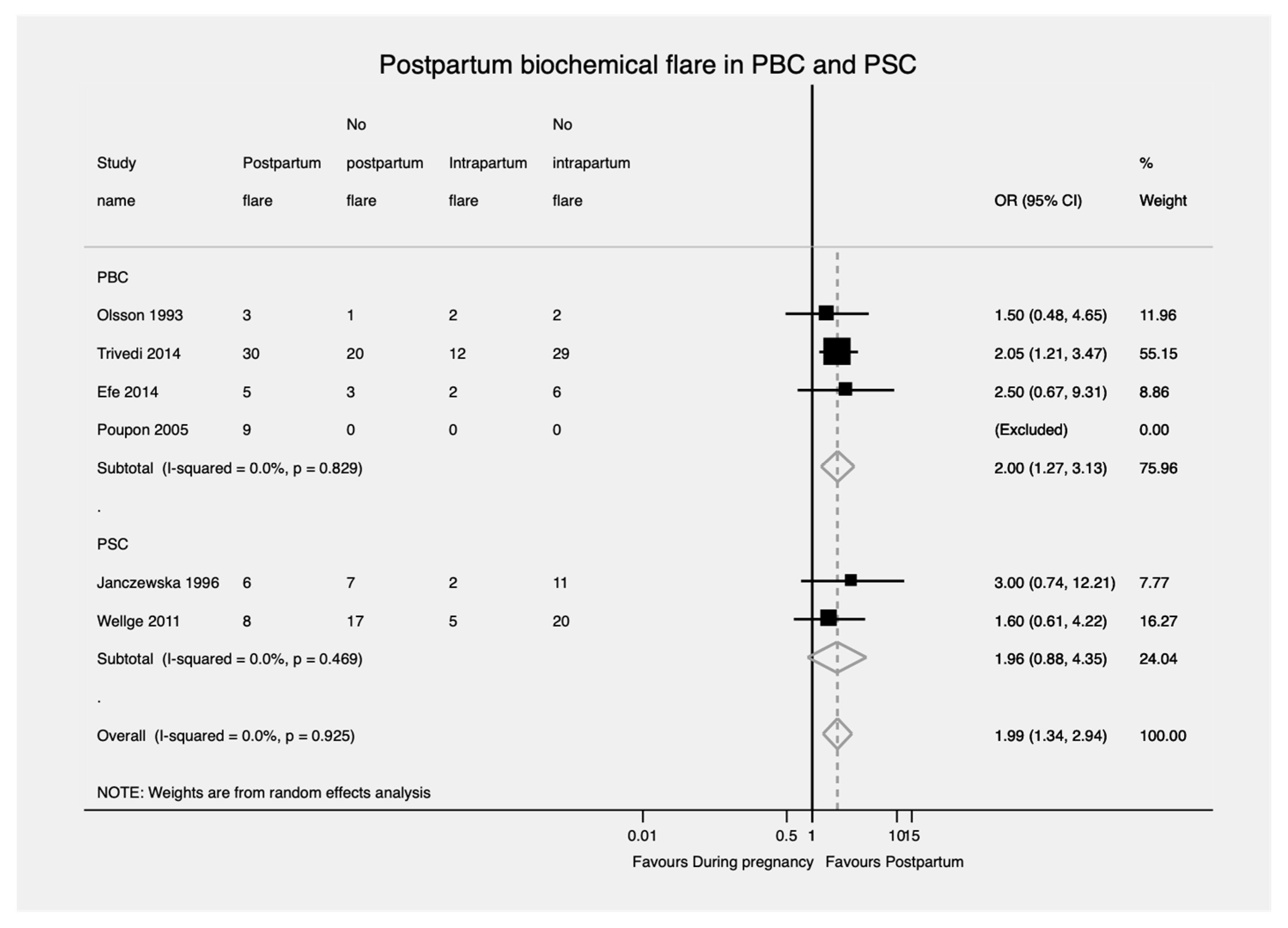
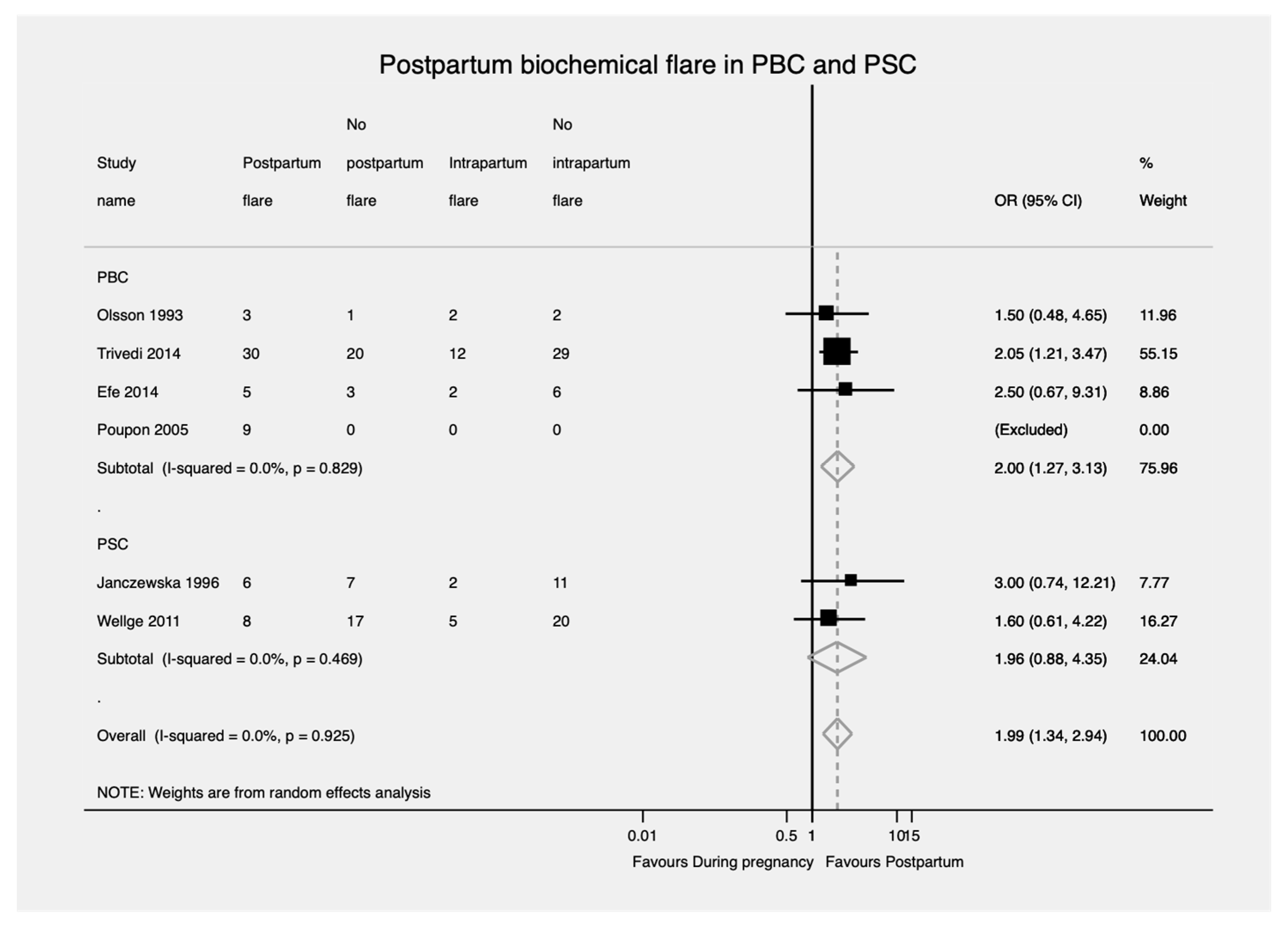
3.3.3. Biochemical Flare Rate
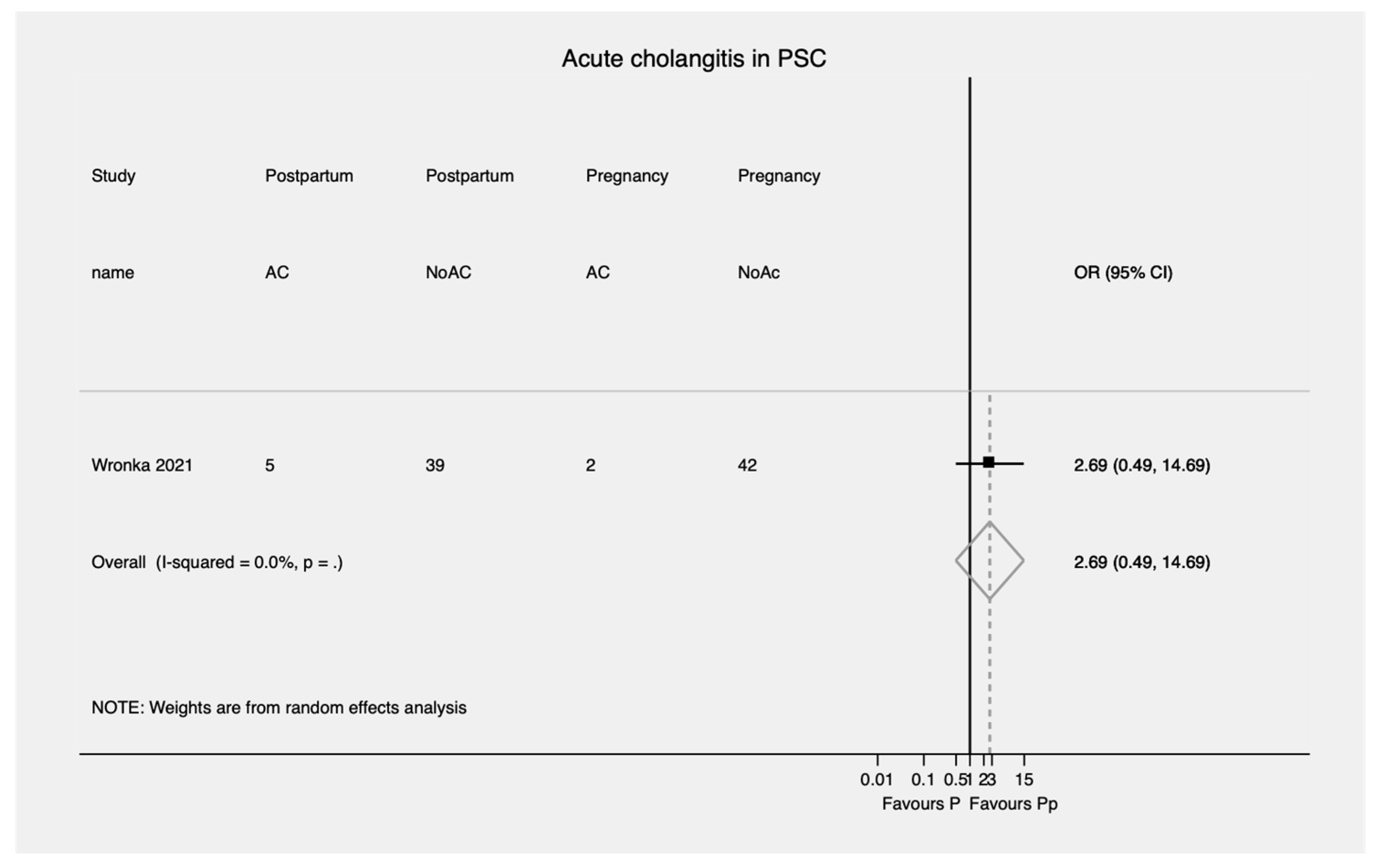
3.3.4. Acute Cholangitis in PSC
3.4. Quality Assessment of Included Studies and Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, Y.-M.; Kaplan, M.M. Primary Sclerosing Cholangitis. N. Engl. J. Med. 1995, 332, 924–933. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, M.M. Primary Biliary Cirrhosis. N. Engl. J. Med. 1996, 335, 1570–1580. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.R.; Lindor, K.D.; Locke, G.R., III; Therneau, T.M.; Homburger, H.A.; Batts, K.P.; Yawn, B.P.; Petz, J.L.; Melton, L.J., III; Dickson, E.R. Epidemiology and Natural History of Primary Biliary Cirrhosis in a US Community. Gastroenterology 2000, 119, 1631–1636. [Google Scholar] [CrossRef]
- Sood, S.; Gow, P.J.; Christie, J.M.; Angus, P.W. Clinical–Liver, Pancreas, and Biliary Tract. Gastroenterology 2004, 127, 6. [Google Scholar]
- Liang, H.; Manne, S.; Shick, J.; Lissoos, T.; Dolin, P. Incidence, Prevalence, and Natural History of Primary Sclerosing Cholangitis in the United Kingdom. Medicine 2017, 96, e7116. [Google Scholar] [CrossRef]
- Cauldwell, M.; Mackie, F.L.; Steer, P.J.; Henehghan, M.A.; Baalman, J.H.; Brennand, J.; Johnston, T.; Dockree, S.; Hedley, C.; Jarvis, S. Pregnancy Outcomes in Women with Primary Biliary Cholangitis and Primary Sclerosing Cholangitis: A Retrospective Cohort Study. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Bergquist, A.; Ajne, G.; Kane, S.; Ekbom, A.; Stephansson, O. A Population-Based Cohort Study of Pregnancy Outcomes among Women with Primary Sclerosing Cholangitis. Clin. Gastroenterol. Hepatol. 2014, 12, 95–100.e1. [Google Scholar] [CrossRef] [PubMed]
- Efe, C.; Kahramanoğlu-Aksoy, E.; Yılmaz, B.; Ozseker, B.; Takcı, S.; Roach, E.C.; Purnak, T.; Kav, T.; Ozaslan, E.; Wahlin, S. Pregnancy in Women with Primary Biliary Cirrhosis. Autoimmun. Rev. 2014, 13, 931–935. [Google Scholar] [CrossRef]
- Floreani, A.; Infantolino, C.; Franceschet, I.; Tene, I.M.; Cazzagon, N.; Buja, A.; Baldo, V.; Gershwin, M.E.; Gervasi, M.T. Pregnancy and Primary Biliary Cirrhosis: A Case-Control Study. Clin. Rev. Allergy Immunol. 2015, 48, 236–242. [Google Scholar] [CrossRef]
- Wellge, B.E.; Sterneck, M.; Teufel, A.; Rust, C.; Franke, A.; Schreiber, S.; Berg, T.; Günther, R.; Kreisel, W.; Zu Eulenburg, C. Pregnancy in Primary Sclerosing Cholangitis. Gut 2011, 60, 1117–1121. [Google Scholar] [CrossRef]
- Trivedi, P.J.; Kumagi, T.; Al-Harthy, N.; Coltescu, C.; Ward, S.; Cheung, A.; Hirschfield, G.M. Good Maternal and Fetal Outcomes for Pregnant Women with Primary Biliary Cirrhosis. Clin. Gastroenterol. Hepatol. 2014, 12, 1179–1185.e1. [Google Scholar] [CrossRef]
- Janczewska, I.; Olsson, R.; Hultcrantz, R.; Broome, U. Pregnancy in Patients with Primary Sclerosing Cholangitis. Liver 1996, 16, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B.; et al. Meta-Analysis of Observational Studies in Epidemiology—A Proposal for Reporting. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Lindor, K.D.; Bowlus, C.L.; Boyer, J.; Levy, C.; Mayo, M. Primary Biliary Cholangitis: 2018 Practice Guidance from the American Association for the Study of Liver Diseases. Hepatology 2019, 69, 394–419. [Google Scholar] [PubMed] [Green Version]
- Chapman, R.W.; Arborgh, B.A.; Rhodes, J.M.; Summerfield, J.A.; Dick, R.; Scheuer, P.J.; Sherlock, S. Primary Sclerosing Cholangitis: A Review of Its Clinical Features, Cholangiography, and Hepatic Histology. Gut 1980, 21, 870–877. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: The Diagnosis and Management of Patients with Primary Biliary Cholangitis. J. Hepatol. 2017, 67, 145–172. [Google Scholar] [CrossRef]
- Chapman, M.H.; Thorburn, D.; Hirschfield, G.M.; Webster, G.G.; Rushbrook, S.M.; Alexander, G.; Collier, J.; Dyson, J.K.; Jones, D.E.; Patanwala, I. British Society of Gastroenterology and UK-PSC Guidelines for the Diagnosis and Management of Primary Sclerosing Cholangitis. Gut 2019, 68, 1356–1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of Cholestatic Liver Diseases. J. Hepatol. 2009, 51, 237–267. [Google Scholar] [CrossRef]
- Covidence. Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, VIC, Australia, 2021. [Google Scholar]
- Ottawa Hospital Research Institute. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 6 October 2021).
- Guo, B.; Moga, C.; Harstall, C.; Schopflocher, D. A Principal Component Analysis Is Conducted for a Case Series Quality Appraisal Checklist. J. Clin. Epidemiol. 2016, 69, 199–207.e2. [Google Scholar] [CrossRef] [PubMed]
- GRADEpro Guideline Development Tool [Software]. McMaster University (Developed by Evidence Prime, Inc.). 2015. Available online: https://www.gradepro.org (accessed on 16 November 2021).
- American College of Obstetricians and Gynecologists. Definition of Term Pregnancy. Committee Opinion No. 579. Obs. Gynecol. 2013, 122, 1139–1140. [Google Scholar] [CrossRef] [PubMed]
- Dugas, C.; Slane, V.H. Miscarriage. StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK532992/ (accessed on 29 June 2021).
- MacDorman, M.F.; Kirmeyer, S.; Gregory, E.C. Fetal and Perinatal Mortality: United States, 2006. Natl. Vital Stat. Rep. 2012, 60, 1–23. [Google Scholar]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata Command to Perform Meta-Analysis of Binomial Data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef] [Green Version]
- Whelton, M.J.; Sherlock, S. Pregnancy in Patients with Hepatic Cirrhosis: Management and Outcome. Lancet 1968, 292, 995–999. [Google Scholar] [CrossRef]
- Olsson, R.; Lööf, L.; Wallerstedt, S. Pregnancy in Patients with Primary Biliary Cirrhosis—A Case for Dissuasion? The Swedish Internal Medicine Liver Club. Liver 1993, 13, 316–318. [Google Scholar] [CrossRef]
- Poupon, R.; Chrétien, Y.; Chazouillères, O.; Poupon, R.E. Pregnancy in Women with Ursodeoxycholic Acid-Treated Primary Biliary Cirrhosis. J. Hepatol. 2005, 42, 418–419. [Google Scholar] [CrossRef] [PubMed]
- Kumagi, T.; Al-Harthy, N.; Coltescu, C.; Hirschfield, G. Pregnancy and Primary Biliary Cirrhosis: Cross-Sectional and Retrospective Analyses Demonstrate a High Prevalence of Symptoms and a Risk of Disease Progression: 1530. Hepatology 2009, 50, 1008A. [Google Scholar]
- Antoniazzi, S.; Gervasi, M.T.; Costa, L.; Cazzagon, N.; Egoue, J.; Floreani, A. 1285 the Outcome of Pregnancy in Patients with Primary Sclerosing Cholangitis. J. Hepatol. 2011, 54, S507. [Google Scholar] [CrossRef]
- Patel, D.; Liu, C.H.; Falahati, V.; Dubrovsky, A.; Gomel, R.; Safer, R.; Sarkar, M.; Bowlus, C.L. Pregnancy Experiences in Women with Primary Sclerosing Cholangitis. In Hepatology; Wiley: Hoboken, NJ, USA, 2019; Volume 70, pp. 775A–776A. [Google Scholar]
- Wronka, K.M.; Bik, E.; Milkiewicz, P. Outcome of Pregnancy in Patients with Primary Sclerosing Cholangitis. Dig. Liver Dis. 2021. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Prediction and Prevention of Spontaneous Preterm Birth: ACOG Practice Bulletin, Number 234. Obstet. Gynecol. 2021, 138, e65–e90. [Google Scholar] [CrossRef] [PubMed]
- Ovadia, C.; Seed, P.T.; Sklavounos, A.; Geenes, V.; Di Ilio, C.; Chambers, J.; Kohari, K.; Bacq, Y.; Bozkurt, N.; Brun-Furrer, R. Association of Adverse Perinatal Outcomes of Intrahepatic Cholestasis of Pregnancy with Biochemical Markers: Results of Aggregate and Individual Patient Data Meta-Analyses. Lancet 2019, 393, 899–909. [Google Scholar] [CrossRef] [Green Version]
- Borchers, A.T.; Naguwa, S.M.; Keen, C.L.; Gershwin, M.E. The Implications of Autoimmunity and Pregnancy. J. Autoimmun. 2010, 34, J287–J299. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.N.; Norwitz, E.R. Preterm Birth: Risk Factors, Interventions for Risk Reduction, and Maternal Prognosis. UpToDate. Available online: https://www.uptodate.com/contents/preterm-birth-risk-factors-interventions-for-risk-reduction-and-maternal-prognosis (accessed on 20 January 2022).
- Adams Waldorf, K.M.; Nelson, J.L. Autoimmune Disease during Pregnancy and the Microchimerism Legacy of Pregnancy. Immunol. Investig. 2008, 37, 631–644. [Google Scholar] [CrossRef]
- Nelson, J.L.; Østensen, M. Pregnancy and Rheumatoid Arthritis. Rheum. Dis. Clin. N. Am. 1997, 23, 195–212. [Google Scholar] [CrossRef]
- Østensen, M.; Brucato, A.; Carp, H.; Chambers, C.; Dolhain, R.J.; Doria, A.; Förger, F.; Gordon, C.; Hahn, S.; Khamashta, M. Pregnancy and Reproduction in Autoimmune Rheumatic Diseases. Rheumatology 2011, 50, 657–664. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Study Design | Country | Total Participants (Pregnancies) | Primary Outcome | Maternal Outcomes | Fetal Outcomes | Concurrent IBD | Biochemical/Immunological Parameters | Pregnancy Biochemical Exacerbation | Postpartum Biochemical Exacerbation |
|---|---|---|---|---|---|---|---|---|---|---|
| Whelton 1968 [28] | Case series | United Kingdom | 5 (6) | To investigate pregnancy outcomes in women with PBC and the influence of pregnancy on the course of their disease. | Jaundice Pruritus Toxaemia Maternal mortality | Mode of delivery Pre-term delivery Miscarriage Stillbirth Neonatal death | NR | Bilirubin | Unclear | Unclear |
| Olsson 1993 [29] | Case series | Sweden | 3 (4) | To report data from pregnancies in PBC patients | Jaundice occurrence Biochemical profile during pregnancy Pruritus | Mode of delivery Gestational age Miscarriage Fetal demise | NR | ALP Aminotransferases Bilirubin | Yes | Yes |
| Poupon 2005 [30] | Case series | France | 6 (9) | To report the experience of pregnancies in UDCA-treated PBC patients. | Pruritus Biochemical profile during pregnancy | Birth weight Mode of delivery Miscarriages Fetal complications | NR | ALP, ALT Serum bile acids Bilirubin Immunoglobulin G and M Antimitochondrial antibodies | Yes | Yes |
| Kumagi 2009 [31] | Retrospective cohort | Canada | 33 (107) | To delineate the clinical characteristics associated with pregnancy and PBC. | Pruritus Right upper quadrant pain Biochemical flares Cirrhosis/portal hypertension | Stillbirth Miscarriage | NR | NR | Unclear | Unclear |
| Floreani 2015 [9] | Case-control | Italy | 7 (8) | To analyze fertility in PBC and investigate the outcome of pregnancy in women with PBC. | Symptom profile during pregnancy Pruritus | Miscarriages Mode of delivery | NR | ALP, ALT, AST, GGT | NR | Yes |
| Trivedi 2014 [11] | Retrospective cohort | Canada | 32 (50) | To describe data on pregnancy, fetal, and maternal-related outcomes from PBC patients. | Pruritus Disease activity Hepatic decompensation | Miscarriage Stillbirth Elective abortion Birth defects Premature delivery Perinatal death Severe disability | NR | Bilirubin ALP, ALT, AST. | Yes | Yes |
| Efe 2014 [8] | Case series | Turkey | 6 (8) | To report experiences of PBC patients who had pregnancies while on UDCA treatment. | Gestational hypertension, gestational diabetes mellitus, pre-eclampsia Biochemical flare Pruritus Biochemical profile during pregnancy | Mode of delivery Stillbirth Miscarriage IUFD Pre-term labor Congenital malformations Small for gestational age | NR | Bilirubin ALP, AST Immunoglobulin G and M Antimitochondrial antibody | Yes | Yes |
| Cauldwell 2020 [6] | Retrospective cohort | United Kingdom | 27 (27) | To report pregnancy outcomes in women with PBC and PSC. | Gestational diabetes mellitus Pre-eclampsia Gestational hypertension Postpartum hemorrhage | Mode of delivery IUFD Pre-term birth Birth weight | NR | ALT, GGT Serum bile acids Platelets | Unclear | Unclear |
| Study (Year) | Study Design | Country | Total Participants (Pregnancies) | Primary Outcome | Maternal Outcomes | Fetal Outcomes | Concurrent IBD | Biochemical Parameters | Pregnancy Biochemical Exacerbation | Postpartum Biochemical Exacerbation |
|---|---|---|---|---|---|---|---|---|---|---|
| Janczewska 1996 [12] | Case series | Sweden | 10 (13) | To study the pregnancy outcomes in PSC patients and, conversely, the effect of pregnancy on the disease. | Pruritus Abdominal pain Fever Jaundice Biochemical flare | Gestational age Mode of delivery Pre-term delivery APGAR score Birth weight | Yes | Total bilirubin Albumin ALP, AST, ALT | Yes | Yes |
| Wellge 2011 [10] | Case series | Germany | 17 (25) | To study PSC activity during pregnancy and after delivery and the influence of medication on the fetal and maternal outcome. | Maternal death Biochemical disease activity IBD flare Pruritus | Miscarriage Pre-term delivery Perinatal death Severe disability Apgar score Cesarean section | Yes | Bilirubin ALP, ALT GGT | Yes | Yes |
| Antoniazzi 2011 [32] | Case-control | Italy | 10 (17) | To evaluate pregnancy outcomes in PSC patients and the effect of pregnancy on the disease. | Pruritus Transaminase increment IBD exacerbation Cesarean section | Miscarriage Birth weight Apgar index of the first and fifth minutes | Yes | Transaminases Total bile salts | Yes | NR |
| Ludvigsson 2014 [7] | Case-control | Sweden | 229 (229) | To examine pregnancy outcomes among women with PSC. | Spontaneous and induced pre-term birth. Pre-eclampsia Gestational diabetes mellitus | Mode of delivery IUFD Pre-term birth fetal growth Congenital abnormalities | Yes | NR | NR | NR |
| Patel 2019 [33] | Case-control | United States | 64 (109) | To evaluate maternal-fetal outcomes among women with PSC with and without concurrent IBD. | Pruritus Abdominal pain Gestational diabetes Pre-eclampsia | Spontaneous abortions Therapeutic abortions Mode of delivery IUFD Pre-term delivery Birth defects | Yes | NR | NR | NR |
| Cauldwell 2020 [6] | Retrospective cohort | United Kingdom | 34 (34) | To report pregnancy outcomes in women with PBC and PSC. | Gestational diabetes mellitus Pre-eclampsia Gestational hypertension Postpartum hemorrhage | Mode of delivery IUFD Pre-term birth Birth weight | Unclear | ALT, GGT Serum bile acids Platelets | Unclear | Unclear |
| Wronka 2021 [34] | Case series | Poland | 25 (42) | To investigate the outcomes of pregnancy in patients with PSC and the influence of pregnancy on disease course. | Death or liver transplantation during one year after Delivery Pruritus Cholangitis IBD flare | Live births Gestational age Apgar score Birth weight Mode of delivery Pre-term delivery Miscarriages Stillbirth Birth defects | Yes | AST, ALT, GGTP, ALP INR Bilirubin Albumin Platelets | NR | NR |
| Outcomes | Unit | Number of Cases | Total Number of Patients | Number of Studies | ER (95% CI; Heterogeneity) | Control Group Cases/Total Control | ER (95% CI; Heterogeneity) |
|---|---|---|---|---|---|---|---|
| Maternal outcomes | |||||||
| Pregnancy flare | P | 16 | 53 | n = 3 | 29% (16–43%) | NA | NA |
| Postpartum flare | P | 47 | 71 | n = 4 | 77% (50–0.96%) | NA | NA |
| Decompensated cirrhosis | P | 0 | 70 | n = 4 | 0% (0–10%) | NA | NA |
| Pruritus onset during pregnancy | P | 41 | 130 | n = 8 | 25% (8–46%) | NA | NA |
| Gestational hypertension | P | 8 | 31 | n = 2 | 23% (9–41%) | NA | NA |
| Gestational diabetes | P | 1 | 26 | n = 1 | 4% (1–19%) | NA | NA |
| C-Section | P | 8 | 37 | n = 3 | 19% (5–38%) | 83/351 | 24 (28–100%) |
| Postpartum hemorrhage | P | 23 | 43 | n = 3 | 53% (2–100%) | NA | NA |
| Fetal outcomes | |||||||
| Preterm infant | P | 15 | 97 | n = 5 | 16% (1–41%) | 37/969 | 4 (3–5%) |
| SA | P | 61 | 202 | n = 8 | 13% (0–34%) | 159/969 | 15 (13–17%) |
| IUFD | P | 5 | 202 | n = 8 | 0% (0–3%) | NA | NA |
| Birth defects | P | 1 | 50 | n = 1 | 2% (0–10%) | NA | NA |
| Low birth weight | P | 3 | 43 | n = 3 | 5% (0–16%) | NA | NA |
| Outcomes | Unit | Number of Cases | Total number of Patients | Number of Studies | ER (95% CI; Heterogeneity) | Control Group Cases/Total Control | ER (95% CI; Heterogeneity) |
|---|---|---|---|---|---|---|---|
| Maternal outcomes | |||||||
| Pregnancy flare | P | 8 | 55 | n = 3 | 14% (5–25%) | NA | NA |
| Postpartum flare | P | 14 | 38 | n = 2 | 37% (22–53%) | NA | NA |
| Pruritus onset during pregnancy | P | 6 | 38 | n = 2 | 14% (4–28%) | NA | NA |
| Gestational hypertension | P | 4 | 34 | n = 1 | 12% (5–27%) | NA | NA |
| Gestational diabetes | P | 2 | 263 | n = 2 | 0% (0–2%) | NA | NA |
| Preeclampsia | P | 8 | 263 | n = 2 | 3% (1–5%) | NA | NA |
| C-section | P | 100 | 312 | n = 5 | 34% (25–43%) | NA | NA |
| Postpartum hemorrhage | P | 30 | 81 | n = 3 | 26% (3–58%) | NA | NA |
| IBD flare | P | 6 | 42 | n = 4 | 13% (3–26%) | NA | NA |
| AC during pregnancy | P | 13 | 178 | n = 3 | 7% (3–11%) | NA | NA |
| AC during postpartum | P | 6 | 7 | n = 2 | 10% (3–20%) | NA | NA |
| Fetal outcomes | |||||||
| Preterm infant | P | 87 | 410 | n = 5 | 19% (9–30%) | 117,327/2,294,568 | 5% (5–5%) |
| SA | P | 6 | 326 | n = 5 | 2% (0–8%) | NA | NA |
| IUFD | P | 9 | 106 | n = 4 | 5% (0–18%) | 60,027/2,304,863 | 3 (3–3%) |
| Birth defects | P | 18 | 350 | n = 3 | 3% (2–5%) | 82,853/2,214,649 | 4% (4–4%) |
| Low birth weight | P | 48 | 544 | n = 6 | 8% (5–10%) | NA | NA |
| Case-Control | Selection | Comparability | Outcome | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Study | Is the Case Definition Adequate | Representativeness of the Cases | Selection of Controls | Definition of Controls | Comparability of Cases and Controls on the Basis of Design or the Analysis | Ascertainment of Exposure | Same Method of Ascertainment for Cases and Controls | Non-Response Rate | Overall Score |
| Antoniazzi 2011 | ✓ | ✓ | ✓ | ✕ | ✓✓ | ✓ | ✕ | ✕ | Fair (6) |
| Floreani 2014 | ✓ | ✓ | ✓ | ✓ | ✓✓ | ✓ | ✓ | ✕ | Good (8) |
| Ludvigsson 2014 | ✓ | ✓ | ✓ | ✓ | ✓✓ | ✓ | ✓ | ✓ | Good (8) |
| Patel 2019 | ✓ | ✓ | ✕ | ✕ | ✓ | ✓ | ✓ | ✕ | Fair (5) |
| Cohort | Selection | Comparability | Outcome | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Study | Representativeness of the Exposed Cohort | Selection of the Non-Exposed Cohort | Ascertainment of Exposure | Demonstration that Outcome of Interest was not Present at Start of Study | Comparability of Cohorts on the Basis of the Design or Analysis | Assessment of Outcome | Was Follow-up Long Enough for Outcomes to Occur | Adequacy of Follow-up of Cohorts | Overall Score |
| Trivedi 2014 | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | Good (7) |
| Kumagi 2009 | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | Good (7) |
| Cauldwell 2020 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | Good (8) |
| Study | Study Objective | Study Design | Study Population | Outcome Measures | Statistical Analysis | Results and Conclusions | Competing Interests and Sources of Support | Overall Score |
|---|---|---|---|---|---|---|---|---|
| Whelton 1968 | ✓ | ✓ | ✓ | ✓✓✓✓ | Partial | ✓✓✓ | ✕ | Fair (10) |
| Olsson 1993 | ✓ | ✓ | ✓✓ | ✓✓ | Partial | ✓✓✓ | ✕ | Poor (9) |
| Janczewska 1996 | ✓ | ✓ | ✓✓ | ✓✓✓✓ | Partial | ✓✓✓ | ✕ | Good (14) |
| Poupon 2005 | ✓ | ✓ | ✓✓ | ✓✓✓✓ | Partial | ✓✓✓✓ | ✕ | Fair (12) |
| Wellge 2011 | ✓ | ✓✓ | ✓✓✓ | ✓✓✓✓ | ✓ | ✓✓✓✓ | ✓ | Good (16) |
| Efe 2014 | ✓ | ✓ | ✓✓ | ✓✓✓✓ | ✓ | ✓✓✓ | ✓ | Fair (13) |
| Wronka 2021 | ✓ | ✓✓ | ✓✓✓ | ✓✓✓✓ | ✓ | ✓✓✓✓ | ✓ | Good (16) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrigno, B.; Barba, R.; Medina-Morales, E.; Trivedi, H.; Patwardhan, V.; Bonder, A. Cholestatic Liver Disease and Pregnancy: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 1068. https://doi.org/10.3390/jcm11041068
Ferrigno B, Barba R, Medina-Morales E, Trivedi H, Patwardhan V, Bonder A. Cholestatic Liver Disease and Pregnancy: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(4):1068. https://doi.org/10.3390/jcm11041068
Chicago/Turabian StyleFerrigno, Bryan, Romelia Barba, Esli Medina-Morales, Hirsh Trivedi, Vilas Patwardhan, and Alan Bonder. 2022. "Cholestatic Liver Disease and Pregnancy: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 4: 1068. https://doi.org/10.3390/jcm11041068
APA StyleFerrigno, B., Barba, R., Medina-Morales, E., Trivedi, H., Patwardhan, V., & Bonder, A. (2022). Cholestatic Liver Disease and Pregnancy: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(4), 1068. https://doi.org/10.3390/jcm11041068