1. Introduction
Lung cancer is the leading cause of death from cancer worldwide [
1]. Approximately 70% of patients have advanced disease at the time of diagnosis, and only 15% of patients with lung cancer are alive five years after diagnosis [
2]. Thus, early detection of lung cancer is very important; for this purpose, low-dose computed tomography (LDCT) screening is performed in high-risk groups for lung cancer [
3].
Tobacco smoking is the most important risk factor for lung cancer, although exposures to other agents such as radon, asbestos, and environmental tobacco smoke (ETS) also are involved [
4]. In addition, chronic obstructive pulmonary disease (COPD) and other smoking-related diseases have been found to be associated with higher rate of lung cancer in several studies [
5,
6,
7,
8]. Additionally, obstructive lung function impairment based on forced expiratory volume in one second (FEV1) has been reported to be associated with lung cancer risk in smokers or groups of men with other characteristics [
9,
10,
11,
12,
13]. However, it is unclear whether the presence of minimal lung function impairment can be considered an independent risk factor for the development of lung cancer in general populations.
The pulmonary function test (PFT) is a cost-effective, easy, and fast tool for diagnosing lung function impairment. With this tool, the identification of individuals with higher lung cancer risk on the basis of lung function decline can be used as a determining parameter and establish cut-off values for the prediction and early detection of lung cancer [
9].
The aim of the present study is to identify an association between lung function and lung cancer development in a large, nationwide database using linkages between the 2010–2016 Korea National Health and Nutrition Examination Survey (KNHANES) and the National Health Insurance Service (NHIS) claims database in the Korean population.
3. Results
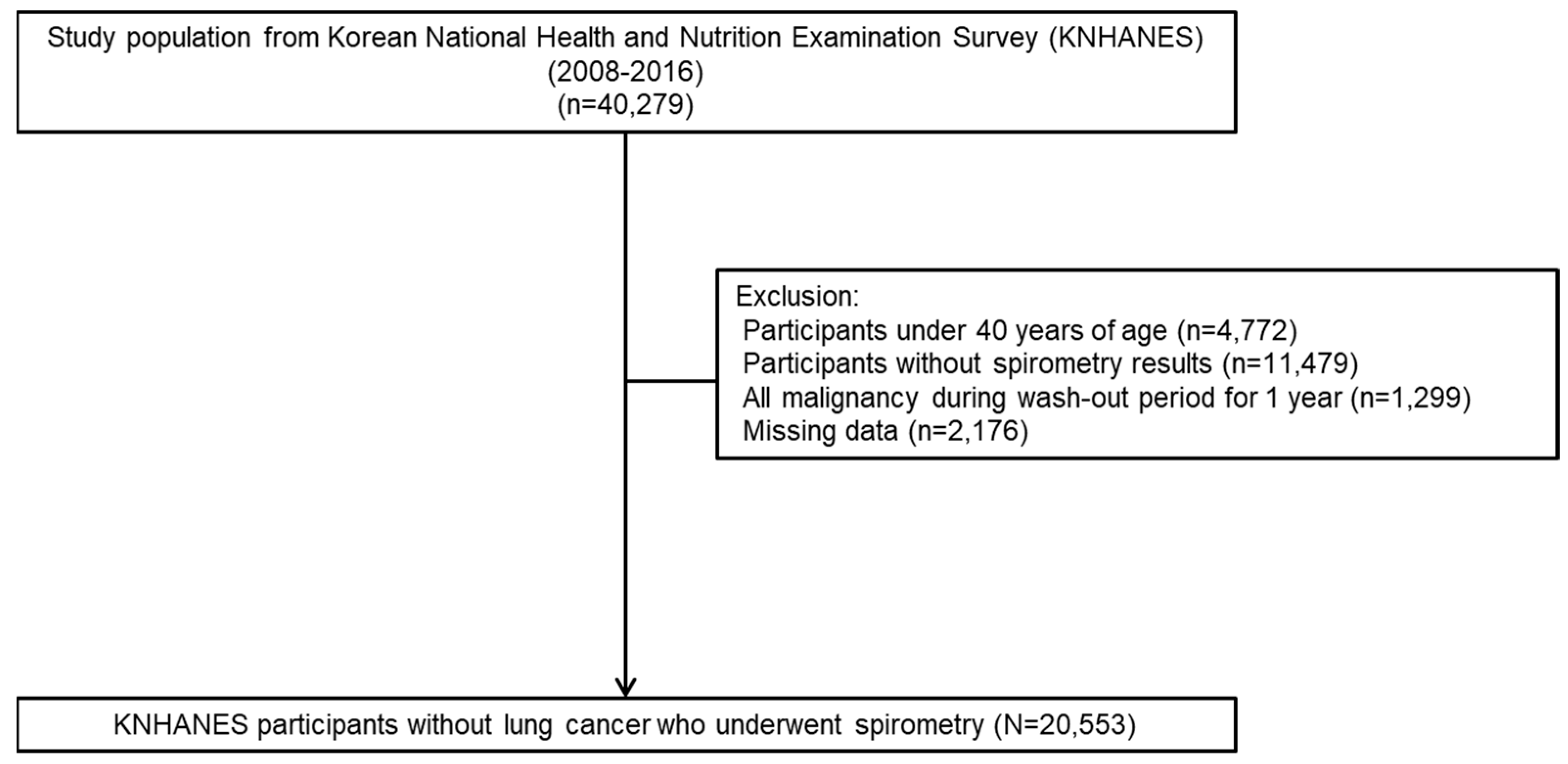
We identified 40,279 participants by linking KNHANES and NHIS datasets from 2008 to 2016. Of these, 4772 participants under the age of 40, 11,479 participants with missing PFT records, 1299 participants with history of malignancy, and 2176 participants with missing data were excluded. Finally, 20,553 participants were analyzed (
Figure 1).
3.1. Baseline Characteristics of Study Participants
Table 1 details the baseline characteristics of participants included in this study. Among the study participants, the proportions of obstructive and non-obstructive lung function impairment were 13.1% and 10.2%, respectively. The proportions of older age, male, current smoker, heavy alcohol consumption, less educated, lowest quartile of income, DM, and hypertension were significantly higher in subjects with obstructive or non-obstructive lung function impairment than in those with normal lung function. Subjects with non-obstructive lung function impairment had a higher mean BMI and waist circumference than subjects with obstructive lung function impairment or normal lung function.
Of the study participants, 169 (0.82%) were diagnosed with lung cancer during the follow-up period (
Table 2). The median duration of follow-up was 6.5 (interquartile range 4.5–8.5) years. Subjects with lung cancer had significantly higher percentages of older age, male, smoking history (ex- or current smoker), less educated, lowest quartile of income, DM, and hypertension. In PFT, mean FVC (88.97% vs. 92.71%,
p < 0.0001), mean FEV1 (83.81% vs. 92.25%,
p < 0.0001), and mean FEV1/FVC (0.7 vs. 0.78,
p < 0.0001) were lower in the lung cancer group than in the control group.
3.2. Risk of Lung Cancer According to Lung Function Impairment Pattern
Table 3 shows adjusted hazard ratios (HRs) and 95% CIs for the association between lung function and the risk of incident lung cancer. We grouped participants into three groups (normal, obstructive, and non-obstructive lung function impairment) based on PFT. In comparison to participants with normal PFT results, the unadjusted HR was 5.817 (4.222–8.014) in the obstructive lung function impairment group and 1.837 (1.112–3.033) in the non-obstructive lung function impairment group. After adjusting for age, sex, BMI, income, smoking, alcohol consumption, and moderate physical activity (model 2), the adjusted HR (95% CI) was 2.518 (1.739–3.648) in the obstructive lung function impairment group and 1.296 (0.776–2.166) in the non-obstructive lung function impairment group in comparison to the normal lung function group. When DM, hypertension, and hypercholesterolemia were additionally controlled (model 3), the adjusted HR (95% CI) was 2.505 (1.729–3.629) in the obstructive lung function impairment group and 1.273 (0.761–2.129) in the non-obstructive lung function impairment group in comparison to the group with normal lung function.
3.3. Risk of Lung Cancer According to Lung Function Quartile
Table 4 shows adjusted HRs and 95% CIs for the risk of incident lung cancer according to lung function quartile. For FEV1 quartiles, the unadjusted HR (95% CI) was 3.528 (2.217–5.613) in the lowest quartile (Q4) of FEV1 in comparison to the highest quartile (Q1). When age, sex, BMI, income, smoking, alcohol consumption, and moderate physical activity were controlled (model 2), the adjusted HR (95% CI) was 2.854 (1.776–4.589) in the lowest quartile of FEV1 in comparison to the highest quartile. With additional adjustment for DM, hypertension, and hypercholesterolemia (model 3), the adjusted HR (95% CI) was 2.845 (1.769–4.575) in the lowest quartile of FEV1 in comparison to the highest quartile.
For FVC quartiles, the unadjusted HR was 2.141 (1.403–3.265) in the lowest quartile of FVC in comparison to the highest quartile. However, lung cancer incidence was not different between the highest quartile and the rest of the quartiles with model 2 or model 3.
For FEV1/FVC, adjusted HRs (95% CIs) in the lowest quartile of FEV1/FVC, in comparison to the highest quartile, according to model 1, model 2, and model 3, were 7.696 (4.395–13.476), 2.886 (1.571–5.301), and 2.891 (1.573–5.312), respectively.
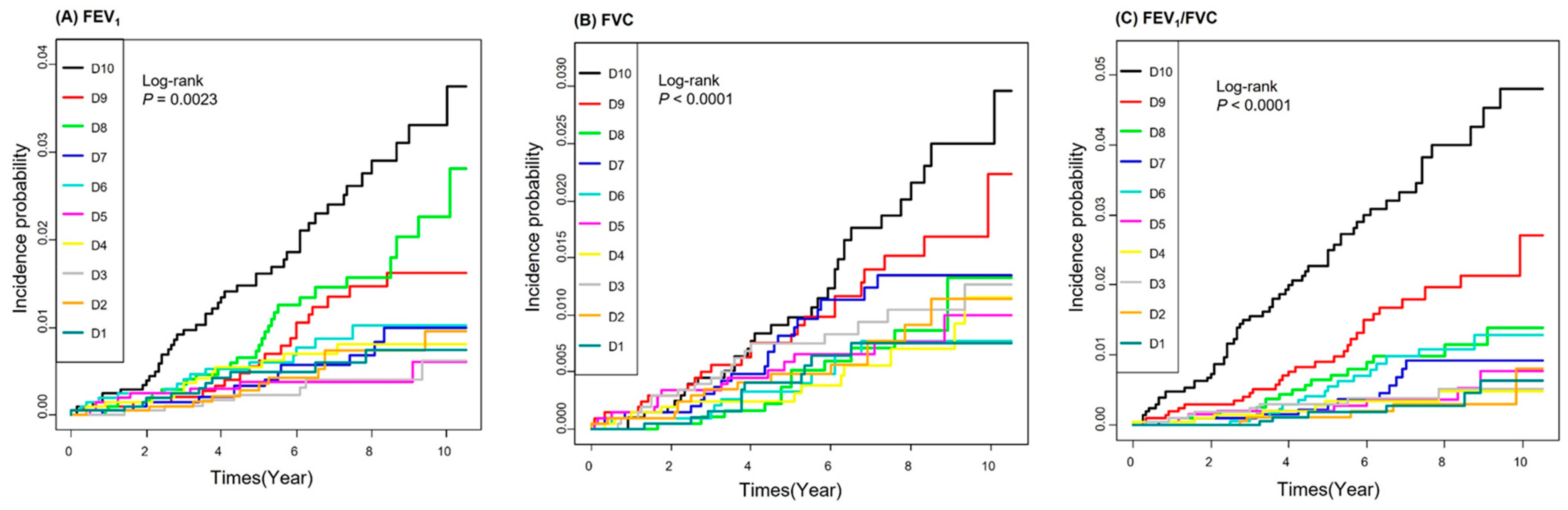
3.4. Risk of Lung Cancer According to Lung Function Decile
The cumulative incidence function curves of lung cancer according to lung function decile are plotted in
Figure 2. Patients in the lower deciles of FEV1, FVC, and FEV1/FVC were at a higher cumulative incidence of lung cancer (
p < 0.0001).
Table 5 shows adjusted HRs and 95% CIs for the risk of incident lung cancer according to lung function decile. For FEV1 deciles, the unadjusted HR (95% CI) was 4.118 (2.13–7.961) in the lowest decile (D10) in comparison to the highest decile (D1). When age, sex, BMI, income, smoking, alcohol consumption, and moderate physical activity were controlled (model 2), the adjusted HR (95% CI) was 3.269 (1.67–6.397) in the lowest decile of FEV1 in comparison to the highest decile. With additional adjustment for DM, hypertension, and hypercholesterolemia (model 3), the adjusted HR (95% CI) was 3.277 (1.674–6.416) in the lowest decile of FEV1 in comparison to the highest decile.
For FVC deciles, the unadjusted HR was 2.961 (1.493–5.875) in the lowest decile compared to the highest decile. However, lung cancer incidence was not different between the lowest and the rest of the deciles with model 2 or model 3.
For FEV1/FVC, adjusted HRs (95% CIs) in the lowest decile of FEV1/FVC in comparison to the highest deciles according to model 1, model 2, and model 3 were 11.742 (5.078–27.151), 3.579 (1.462–8.761), and 3.593 (1.467–8.801), respectively.
3.5. Risk of Lung Cancer According to Continuous Variables of Lung Function
We further analyzed the risk of lung cancer according to increase in lung function based on continuous variables of FEV1, FVC and FEV1/FVC values. For FEV1, the adjusted HRs for every 1% increase in FEV1 was 0.974 (
p < 0.0001) in Model 2 and Model 3, respectively. Similarly, the adjusted HRs for every 0.01 increase in FEV1/FVC was 0.95 (
p < 0.0001) in Model 2 and Model 3. The unadjusted HR for every 1% increase in FVC was 0.973 (
p < 0.0001), but there was no statistically significant difference according to increase in FVC after adjustment (
Table 6).
3.6. Risk of Lung Cancer According to Quartile Combination of FEV1 and FVC
To determine which of FEV1 or FVC has a greater impact on lung cancer incidence, the risk of lung cancer by quartile combination of FEV1 and FVC was analyzed (higher three quartiles: Q1–3 vs. lowest quartile: Q4) (
Table 7). A group with the higher three quartiles (Q1–Q3) for both FEV1 and FVC served as the reference. When FEV1 values were in the lowest quartile (Q4), the incidence of lung cancer was significantly increased regardless of FVC. In particular, the incidence of lung cancer was highest in the group with the lowest quartiles for both FEV1 and FVC (FEV1 Q4 and FVC Q4: aHR 1.889; 95% CI 1.331–2.681). However, when only FVC values were in the lowest quartile, there was no significant difference in the incidence rate of lung cancer (FEV1 Q1–3 and FVC Q4: aHR 0.672; 95% CI 0.334–1.351).
4. Discussion
In this study using nationally representative data in the Korean population, we observed that decreased lung function was associated with increased risk of lung cancer after adjusting for various confounding factors. Individuals with obstructive or non-obstructive lung function impairment showed a higher risk of lung cancer compared with those with normal lung function. Further, we found that those with lower quartiles or deciles of FEV1 or FEV1/FVC had a higher risk of lung cancer.
The relationship between COPD and lung cancer has been recognized. In a cohort of male construction workers, a high rate of lung cancer was observed in a COPD group relative to a group with normal lung function [
6]. Additionally, the presence of COPD has been associated with a higher risk for lung cancer incidence in adult general populations in the US and UK [
7,
8]. In a nationwide population-based cohort, COPD was an independent risk factor for development of lung cancer regardless of smoking status [
5].
Several studies have suggested that airway obstruction, based on FEV1 reduction, increases lung cancer risk. In a community-based cohort of Japanese-American men, the percentage of predicted FEV1 was inversely associated with risk of lung cancer [
10]. Additionally, FEV1 was inversely associated with risk of lung cancer among former and current smokers but not in never-smokers [
9,
11,
12]. Further, a strong linear relationship was observed between increasing severity of airflow limitation and risk of lung cancer in heavy smokers [
13]. In never-smokers, impaired lung function in the risk prediction model for lung cancer showed a limited improvement in predictive performance [
24]. However, it is unclear whether the presence of minimal lung function impairment should be considered an independent risk factor for the development of lung cancer in general populations.
One difference between our study and the existing research is that we separated the evaluation of obstructive and non-obstructive lung function impairment. In addition, pulmonary function parameters were subdivided into quartiles, deciles or change of continuous variables, and the relationship between lung function and lung cancer development was investigated by group of or change in lung function values. We showed that minimal and moderate obstructive lung function impairment confers an increased risk of lung cancer development in the general population after adjusting for confounding factors.
One important clinical application of our study is the use of spirometry to better target CT screening for early detection of lung cancer. In a previous similar approach, inclusion of spirometric criteria for CT screening eligibility resulted in an increase in lung cancer detection of 6.8%, which is higher than in other studies where screening populations were identified based on age and smoking history [
25,
26]. Lung cancer screening in individuals with lung function impairment is not recommended by the US Preventive Services Task Force [
27]. Similarly, the highest-risk group subject to screening comprises people between 54 and 74 years of age, who were recorded as current smokers with a smoking history of 30 pack years or more in the health checkup or smoking cessation treatment support project questionnaire in the previous year in Korea. The importance of lung cancer screening is emphasized by the mortality reduction seen in the recently published, large, randomized, NELSON screening trial [
3].
Smoking exposure is an important prerequisite for lung function impairment. Additionally, there is sufficient evidence to establish a causal association between smoking and lung cancer [
28]. However, the proportion of never-smoker lung cancer patients are increasing [
29]. Further, the contribution of smoking in comparison to the variance in ventilatory function is modest and much less meaningful than genetic factors in most lung cancer [
30,
31]. The higher susceptibility of the lungs to cancer due to smoking is due to the combined effects of inflammation and aberrant repair [
32]. Lung function decline and COPD also are caused by indoor air pollutants, poorly controlled chronic asthma, occupational exposures to dusts, poor socioeconomic status, malnutrition, childhood respiratory infections, and formerly treated pulmonary tuberculosis even without a smoking history [
33,
34]. In our study, minimal lung function impairment was one of the dependent risk factors for lung cancer risk after adjusting for confounding factors including smoking history. Even though smoking is one of attributable factor for lung cancer risk, our study suggests that minimal lung function impairment can be a dependent risk factor for lung cancer development and has clinical implications for lung cancer screening in the general population.
Some proposed mechanisms for poor lung function and lung cancer risk include the impaired pulmonary clearance of inhaled carcinogens and inflammation-induced production of genotoxic reactive oxygen species [
35]. In addition, chronic inflammation caused by accumulation of mucous exudates in the lumen, leading to the remodeling and thickening of bronchiolar walls associated with impaired tissue repair, could result in the production of several growth factors and growth of sporadically transformed cells [
36,
37].
Although it is clear that smoking plays an important role in the development of lung cancer and lung function decline, lung function deterioration not associated with smoking also contributes. Accordingly, if lung function parameters are added to the selection of subjects for lung cancer screening (currently based on smoking history and age), the specificity over sensitivity of lung cancer screening can be maximized to result in a more favorable trade-off between the harms and benefits of LDCT screening. The results of our study have the potential to be used as basic data for selecting high-risk groups for lung cancer screening based on lung function parameters.
A limitation of this study is that detailed history of ETS, e-cigarettes, and exposure to occupational dusts, which are associated with lung function impairment and/or lung cancer risk, was not included in the analysis. Additionally, other factors, such as drugs for airway disease and combined emphysema involved in lung cancer development, were not analyzed. We also did not consider smoking amounts, one of the confounding factors for lung cancer development, but considered current smoking status as an adjustment factor. Further, cell types and lung cancer stage were not investigated according to lung function impairment due to the limitations of data collection.
In conclusion, the findings from this nationally representative, Korean population-based large cohort study support the hypothesis that lower FEV1 or FEV1/FVC are associated with lung cancer incidence. The present study indicates the role of PFT as a noninvasive, affordable, and fast tool in screening for optimal candidates for the early detection of lung cancer.


 ,
, 


{kind=link}
{kind=link}