
Hypothermia for Cardioprotection in Patients with St-Elevation Myocardial Infarction: Do Not Give It the Cold Shoulder Yet!

 ,
,  , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Pathophysiology and Clinical Expression of Reperfusion Injury
3. Preclinical Studies
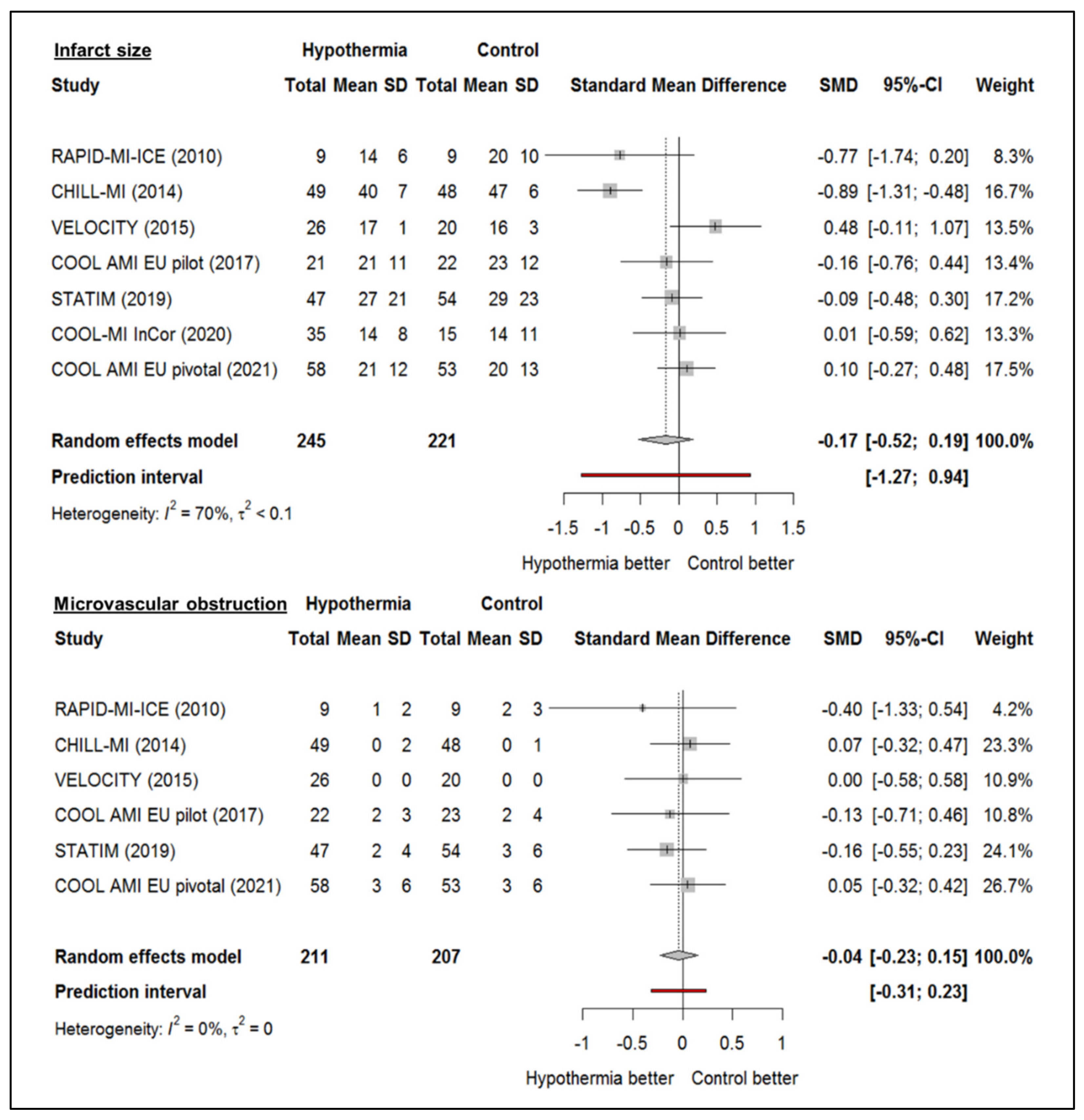
4. Clinical Studies
5. Improving Hypothermic Cardioprotection
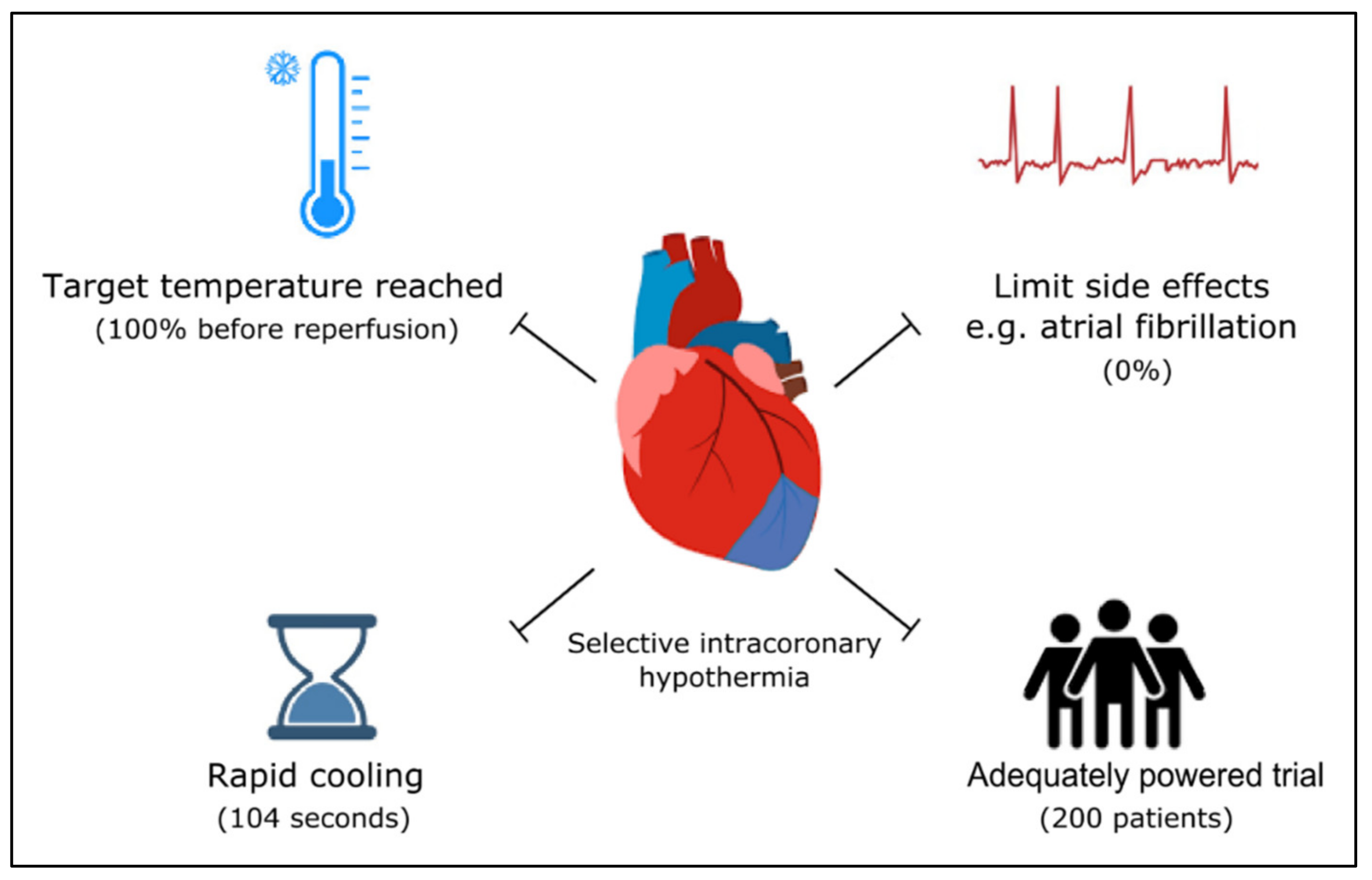
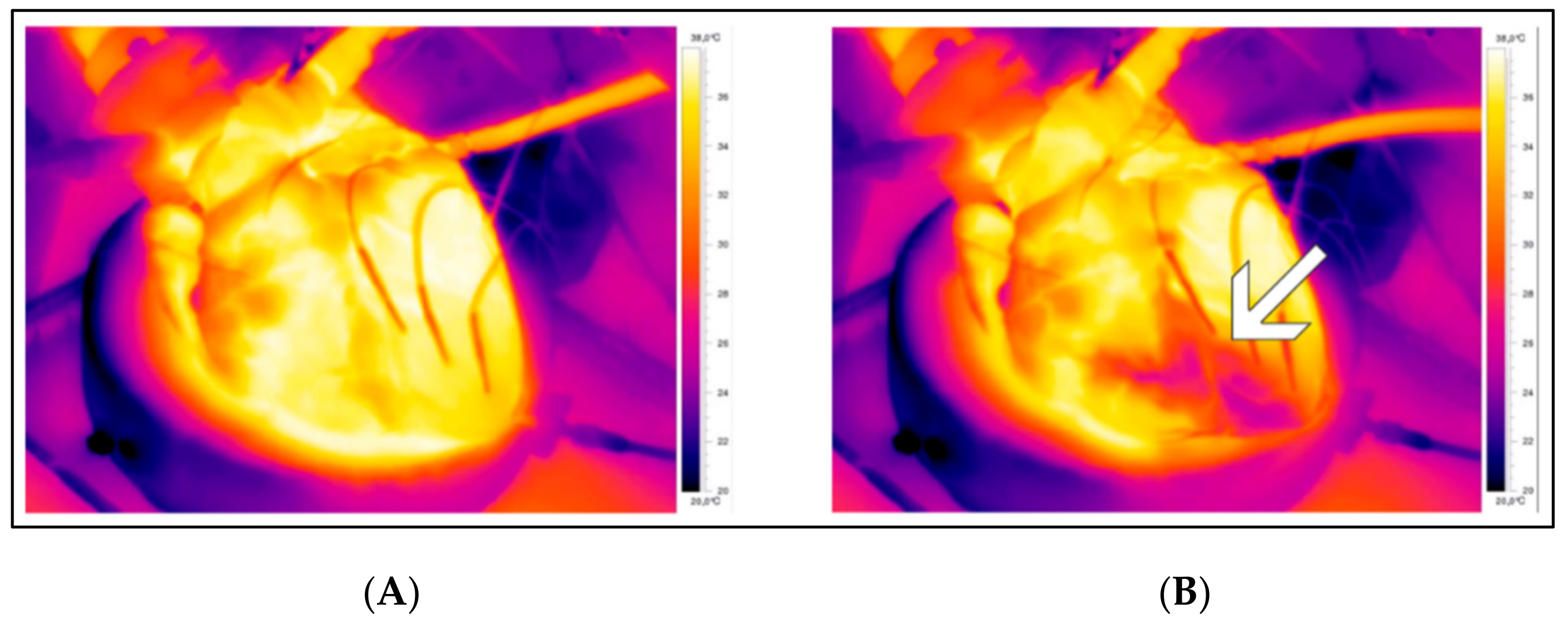
6. Selective Intracoronary Hypothermia
7. Ongoing Studies
8. The Future of Therapeutic Hypothermia in STEMI
9. Conclusions
Funding
Informed Consent Statement
Conflicts of Interest
Abbreviations
| AMI | Acute myocardial infarction |
| STEMI | ST-elevation myocardial infarction |
| PCI | Percutaneous coronary intervention |
| IS | Infarct size |
| MaR | Myocardium at risk |
| MVO | Microvascular obstruction |
References
- World Health Organization. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2016; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- O’Gara, P.T.; Kushner, F.G.; Ascheim, D.D.; Casey, D.E., Jr.; Chung, M.K.; de Lemos, J.A.; Ettinger, S.M.; Fang, J.C.; Fesmire, F.M.; Franklin, B.A.; et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 61, 485–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, G.W.; Selker, H.P.; Thiele, H.; Patel, M.R.; Udelson, J.E.; Ohman, E.M.; Maehara, A.; Eitel, I.; Granger, C.B.; Jenkins, P.L.; et al. Relationship Between Infarct Size and Outcomes Following Primary PCI: Patient-Level Analysis From 10 Randomized Trials. J. Am. Coll. Cardiol. 2016, 67, 1674–1683. [Google Scholar] [CrossRef] [PubMed]
- Yellon, D.M.; Hausenloy, D.J. Myocardial reperfusion injury. N. Engl. J. Med. 2007, 357, 1121–1135. [Google Scholar] [CrossRef] [PubMed]
- Bernard, S.A.; Gray, T.W.; Buist, M.D.; Jones, B.M.; Silvester, W.; Gutteridge, G.; Smith, K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N. Engl. J. Med. 2002, 346, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Lascarrou, J.B.; Merdji, H.; Le Gouge, A.; Colin, G.; Grillet, G.; Girardie, P.; Coupez, E.; Dequin, P.F.; Cariou, A.; Boulain, T.; et al. Targeted Temperature Management for Cardiac Arrest with Nonshockable Rhythm. N. Engl. J. Med. 2019, 381, 2327–2337. [Google Scholar] [CrossRef]
- Allen, D.G.; Xiao, X.H. Role of the cardiac Na+/H+ exchanger during ischemia and reperfusion. Cardiovasc. Res. 2003, 57, 934–941. [Google Scholar] [CrossRef] [Green Version]
- Kalogeris, T.; Baines, C.P.; Krenz, M.; Korthuis, R.J. Cell biology of ischemia/reperfusion injury. Int. Rev. Cell Mol. Biol. 2012, 298, 229–317. [Google Scholar]
- Di Lisa, F.; Canton, M.; Menabo, R.; Kaludercic, N.; Bernardi, P. Mitochondria and cardioprotection. Heart Fail Rev. 2007, 12, 249–260. [Google Scholar] [CrossRef]
- Griffiths, E.J.; Halestrap, A.P. Mitochondrial non-specific pores remain closed during cardiac ischaemia, but open upon reperfusion. Biochem. J. 1995, 307 Pt 1, 93–98. [Google Scholar] [CrossRef] [Green Version]
- Halestrap, A.P.; Clarke, S.J.; Javadov, S.A. Mitochondrial permeability transition pore opening during myocardial reperfusion--a target for cardioprotection. Cardiovasc. Res. 2004, 61, 372–385. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Dorado, D.; Ruiz-Meana, M.; Inserte, J.; Rodriguez-Sinovas, A.; Piper, H.M. Calcium-mediated cell death during myocardial reperfusion. Cardiovasc. Res. 2012, 94, 168–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemasters, J.J.; Bond, J.M.; Chacon, E.; Harper, I.S.; Kaplan, S.H.; Ohata, H.; Trollinger, D.R.; Herman, B.; Cascio, W.E. The pH paradox in ischemia-reperfusion injury to cardiac myocytes. EXS 1996, 76, 99–114. [Google Scholar]
- Shao, Z.H.; Sharp, W.W.; Wojcik, K.R.; Li, C.Q.; Han, M.; Chang, W.T.; Ramachandran, S.; Li, J.; Hamann, K.J.; Vanden Hoek, T.L. Therapeutic hypothermia cardioprotection via Akt- and nitric oxide-mediated attenuation of mitochondrial oxidants. Am. J. Physiol. Heart Circ. Physiol. 2010, 298, H2164–H2173. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Bian, X.; Li, Y.; Xiao, X.; Yin, Y.; Du, X.; Wang, C.; Li, L.; Bai, Y.; Liu, X. Moderate hypothermia induces protection against hypoxia/reoxygenation injury by enhancing SUMOylation in cardiomyocytes. Mol. Med. Rep. 2020, 22, 2617–2626. [Google Scholar] [CrossRef]
- El Farissi, M.; Buscone, S.; Bax, N.A.; van Rijswijk, J.W.; Veenendaal, T.; Keulards, D.C.; Otterspoor, L.C.; Zelis, J.M.; van Tuijl, S.; Eerdekens, R.; et al. Ultrastructural Characteristics of Myocardial Reperfusion Injury and Effect of Selective Intracoronary Hypothermia: An Observational Study in Isolated Beating Porcine Hearts. Ther. Hypothermia Temp. Manag. 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Botker, H.E.; Hausenloy, D.; Andreadou, I.; Antonucci, S.; Boengler, K.; Davidson, S.M.; Deshwal, S.; Devaux, Y.; Di Lisa, F.; Di Sante, M.; et al. Practical guidelines for rigor and reproducibility in preclinical and clinical studies on cardioprotection. Basic Res. Cardiol. 2018, 113, 39. [Google Scholar] [CrossRef] [Green Version]
- Dae, M.W.; Gao, D.W.; Sessler, D.I.; Chair, K.; Stillson, C.A. Effect of endovascular cooling on myocardial temperature, infarct size, and cardiac output in human-sized pigs. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, H1584–H1591. [Google Scholar] [CrossRef]
- Otake, H.; Shite, J.; Paredes, O.L.; Shinke, T.; Yoshikawa, R.; Tanino, Y.; Watanabe, S.; Ozawa, T.; Matsumoto, D.; Ogasawara, D.; et al. Catheter-based transcoronary myocardial hypothermia attenuates arrhythmia and myocardial necrosis in pigs with acute myocardial infarction. J. Am. Coll. Cardiol. 2007, 49, 250–260. [Google Scholar] [CrossRef] [Green Version]
- Gotberg, M.; Olivecrona, G.K.; Engblom, H.; Ugander, M.; van der Pals, J.; Heiberg, E.; Arheden, H.; Erlinge, D. Rapid short-duration hypothermia with cold saline and endovascular cooling before reperfusion reduces microvascular obstruction and myocardial infarct size. BMC Cardiovasc. Disord. 2008, 8, 7. [Google Scholar] [CrossRef] [Green Version]
- Gotberg, M.; van der Pals, J.; Gotberg, M.; Olivecrona, G.K.; Kanski, M.; Koul, S.; Otto, A.; Engblom, H.; Ugander, M.; Arheden, H.; et al. Optimal timing of hypothermia in relation to myocardial reperfusion. Basic Res. Cardiol. 2011, 106, 697–708. [Google Scholar] [CrossRef] [PubMed]
- Hale, S.L.; Herring, M.J.; Kloner, R.A. Delayed treatment with hypothermia protects against the no-reflow phenomenon despite failure to reduce infarct size. .J Am. Heart Assoc. 2013, 2, e004234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, W.; Hale, S.; Kloner, R.A. Delayed therapeutic hypothermia protects against the myocardial no-reflow phenomenon independently of myocardial infarct size in a rat ischemia/reperfusion model. Int. J. Cardiol. 2017, 236, 400–404. [Google Scholar] [CrossRef]
- Kim, H.; Lee, J.; Song, W.; Shin, J.; Oh, D.; Harrison, K.; Jakkula, M.; Wong, S.C.; Hong, M.K. Feasibility and safety of regional myocardial hypothermia during myocardial ischemia and infarction in pigs. Coron. Artery Dis. 2005, 16, 125–129. [Google Scholar] [CrossRef]
- Gotberg, M.; Olivecrona, G.K.; Koul, S.; Carlsson, M.; Engblom, H.; Ugander, M.; van der Pals, J.; Algotsson, L.; Arheden, H.; Erlinge, D. A pilot study of rapid cooling by cold saline and endovascular cooling before reperfusion in patients with ST-elevation myocardial infarction. Circ. Cardiovasc. Interv. 2010, 3, 400–407. [Google Scholar] [CrossRef] [Green Version]
- Erlinge, D.; Gotberg, M.; Lang, I.; Holzer, M.; Noc, M.; Clemmensen, P.; Jensen, U.; Metzler, B.; James, S.; Botker, H.E.; et al. Rapid endovascular catheter core cooling combined with cold saline as an adjunct to percutaneous coronary intervention for the treatment of acute myocardial infarction. The CHILL-MI trial: A randomized controlled study of the use of central venous catheter core cooling combined with cold saline as an adjunct to percutaneous coronary intervention for the treatment of acute myocardial infarction. J. Am. Coll. Cardiol. 2014, 63, 1857–1865. [Google Scholar] [CrossRef] [Green Version]
- Nichol, G.; Strickland, W.; Shavelle, D.; Maehara, A.; Ben-Yehuda, O.; Genereux, P.; Dressler, O.; Parvataneni, R.; Nichols, M.; McPherson, J.; et al. Prospective, multicenter, randomized, controlled pilot trial of peritoneal hypothermia in patients with ST-segment- elevation myocardial infarction. Circ. Cardiovasc. Interv. 2015, 8, e001965. [Google Scholar] [CrossRef] [Green Version]
- Noc, M.; Erlinge, D.; Neskovic, A.N.; Kafedzic, S.; Merkely, B.; Zima, E.; Fister, M.; Petrovic, M.; Cankovic, M.; Veress, G.; et al. COOL AMI EU pilot trial: A multicentre, prospective, randomised controlled trial to assess cooling as an adjunctive therapy to percutaneous intervention in patients with acute myocardial infarction. EuroIntervention 2017, 13, e531–e539. [Google Scholar] [CrossRef] [Green Version]
- Testori, C.; Beitzke, D.; Mangold, A.; Sterz, F.; Loewe, C.; Weiser, C.; Scherz, T.; Herkner, H.; Lang, I. Out-of-hospital initiation of hypothermia in ST-segment elevation myocardial infarction: A randomised trial. Heart 2019, 105, 531–537. [Google Scholar] [CrossRef] [Green Version]
- Dallan, L.A.P.; Giannetti, N.S.; Rochitte, C.E.; Polastri, T.F.; San Martin, C.Y.B.; Hajjar, L.A.; Lima, F.G.; Nicolau, J.C.; Oliveira, M.T., Jr.; Dae, M.; et al. Cooling as an Adjunctive Therapy to Percutaneous Intervention in Acute Myocardial Infarction: COOL-MI InCor Trial. Ther. Hypothermia Temp. Manag. 2021, 11, 135–144. [Google Scholar] [CrossRef]
- Noc, M.; Laanmets, P.; Neskovic, A.N.; Petrovic, M.; Stanetic, B.; Aradi, D.; Kiss, R.G.; Ungi, I.; Merkely, B.; Hudec, M.; et al. A multicentre, prospective, randomised controlled trial to assess the safety and effectiveness of cooling as an adjunctive therapy to percutaneous intervention in patients with acute myocardial infarction: The COOL AMI EU Pivotal Trial. EuroIntervention 2021, 17, 466–473. [Google Scholar] [CrossRef]
- El Farissi, M.; Keulards, D.C.J.; Zelis, J.M.; van’t Veer, M.; Zimmermann, F.M.; Pijls, N.H.J.; Otterspoor, L.C. Hypothermia for Reduction of Myocardial Reperfusion Injury in Acute Myocardial Infarction: Closing the Translational Gap. Circ. Cardiovasc. Interv. 2021, 14, e010326. [Google Scholar] [CrossRef] [PubMed]
- Otterspoor, L.C.; van Nunen, L.X.; Rosalina, T.T.; Veer, M.V.; Tuijl, S.V.; Stijnen, M.; Rutten, M.C.; van de Vosse, F.N.; Pijls, N.H. Intracoronary hypothermia for acute myocardial infarction in the isolated beating pig heart. Am. J. Transl. Res. 2017, 9, 558–568. [Google Scholar] [PubMed]
- Otterspoor, L.C.; Van’t Veer, M.; Van Nunen, L.X.; Brueren, G.R.G.; Tonino, P.A.L.; Wijnbergen, I.F.; Helmes, H.; Zimmermann, F.M.; Van Hagen, E.; Johnson, N.P.; et al. Safety and feasibility of selective intracoronary hypothermia in acute myocardial infarction. EuroIntervention 2017, 13, e1475–e1482. [Google Scholar] [CrossRef] [PubMed]
- El Farissi, M.; Keulards, D.C.J.; van ‘t Veer, M.; Zelis, J.M.; Berry, C.; De Bruyne, B.; Engstrom, T.; Frobert, O.; Piroth, Z.; Oldroyd, K.G.; et al. Selective intracoronary hypothermia in patients with ST-elevation myocardial infarction. Rationale and design of the EURO-ICE trial. EuroIntervention 2021, 16, 1444–1446. [Google Scholar] [CrossRef] [PubMed]
- El Farissi, M.; Good, R.; Engstrom, T.; Oldroyd, K.G.; Karamasis, G.V.; Vlaar, P.J.; Lonborg, J.T.; Teeuwen, K.; Keeble, T.R.; Mangion, K.; et al. Safety of Selective Intracoronary Hypothermia during Primary Percutaneous Coronary Intervention in Patients with Anterior STEMI. JACC Cardiovasc. Interv. 2021, 14, 2047–2055. [Google Scholar] [CrossRef]
- Jackson, T.C.; Kochanek, P.M. A New Vision for Therapeutic Hypothermia in the Era of Targeted Temperature Management: A Speculative Synthesis. Ther. Hypothermia Temp. Manag. 2019, 9, 13–47. [Google Scholar] [CrossRef] [Green Version]
- Ye, S.; Shi, K.; Xu, J.; Wang, M.; Li, C.J. Cholecystokinin octapeptide inhibits the inflammatory response and improves neurological outcome in a porcine model of cardiopulmonary resuscitation. Exp. Ther. Med. 2018, 15, 2583–2588. [Google Scholar] [CrossRef] [Green Version]
- Schäfer, A.; Akin, M.; Diekmann, J.; König, T. Intracoronary application of super-saturated oxygen to reduce reperfusion injury following myocardial infarction. J. Clin. Med. 2022. inpress. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Farissi, M.; Mast, T.P.; van de Kar, M.R.D.; Dillen, D.M.M.; Demandt, J.P.A.; Vervaat, F.E.; Eerdekens, R.; Dello, S.A.G.; Keulards, D.C.; Zelis, J.M.; et al. Hypothermia for Cardioprotection in Patients with St-Elevation Myocardial Infarction: Do Not Give It the Cold Shoulder Yet! J. Clin. Med. 2022, 11, 1082. https://doi.org/10.3390/jcm11041082
El Farissi M, Mast TP, van de Kar MRD, Dillen DMM, Demandt JPA, Vervaat FE, Eerdekens R, Dello SAG, Keulards DC, Zelis JM, et al. Hypothermia for Cardioprotection in Patients with St-Elevation Myocardial Infarction: Do Not Give It the Cold Shoulder Yet! Journal of Clinical Medicine. 2022; 11(4):1082. https://doi.org/10.3390/jcm11041082
Chicago/Turabian StyleEl Farissi, Mohamed, Thomas P. Mast, Mileen R. D. van de Kar, Daimy M. M. Dillen, Jesse P. A. Demandt, Fabienne E. Vervaat, Rob Eerdekens, Simon A. G. Dello, Danielle C. Keulards, Jo M. Zelis, and et al. 2022. "Hypothermia for Cardioprotection in Patients with St-Elevation Myocardial Infarction: Do Not Give It the Cold Shoulder Yet!" Journal of Clinical Medicine 11, no. 4: 1082. https://doi.org/10.3390/jcm11041082