
Update on Management of Cardiovascular Diseases in Women

 , , , , and
, , , , and
Abstract
1. Introduction
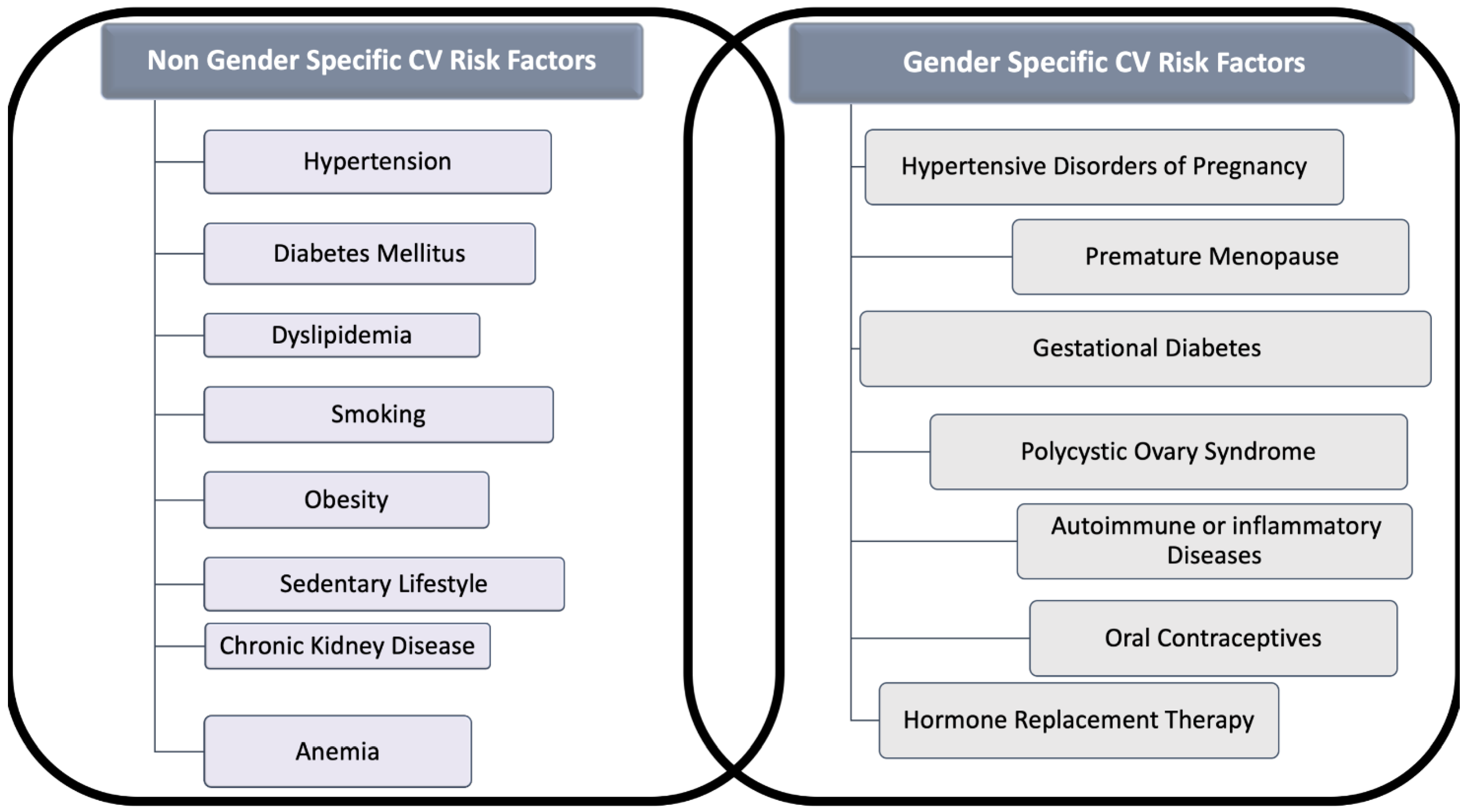
2. Cardiovascular Risk Factors in Women
2.1. Hypertension
Gender Differences in Hypertension-Related Target Organ Damage
2.2. Diabetes Mellitus
2.3. Cholesterol
2.4. Smoking
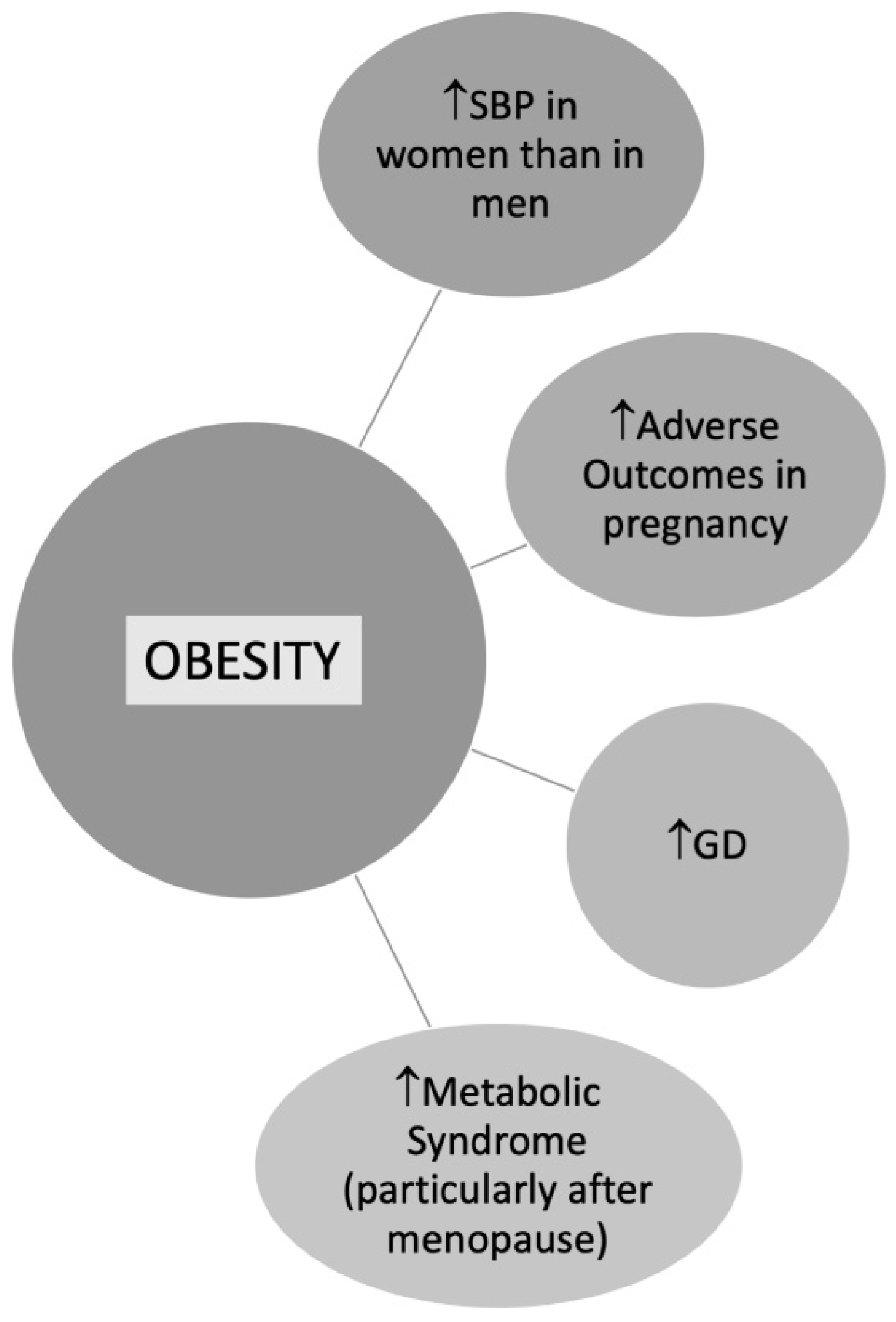
2.5. Obesity
2.6. Physical Activity
2.7. Chronic Kidney Disease
2.8. Anemia
3. Cardiovascular Gender-Specific Risk Factors
3.1. Hypertensive Disorders during Pregnancy (HPD)
3.2. Preeclampsia
3.3. Gestational Diabetes (GD)
3.4. Polycystic Ovary Syndrome(PCOS)
3.5. Autoimmune or Inflammatory Diseases
3.6. Oral Contraceptives
3.7. Menopause and Hormone Replacement Therapy (HRT)
4. Gender Differences in Cardiovascular Diseases: From Epidemiology to Prognosis
4.1. Coronary Heart Disease (CAD)
4.2. Takotsubo Syndrome (TS)
4.3. Spontaneous Coronary Artery Dissection (SCAD)
4.4. Ischemia with Non-Obstructive Coronary Arteries (INOCA)
4.5. Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease (MINOCA)
4.6. Heart Failure (HF)
4.7. Valvular Heart Diseases (VHD)
4.8. Atrial Fibrillation
5. Treatment of Cardiovascular Risk Factors in Both Sexes: Differences and Relative Prognostic Impact
6. Treatment of Cardiovascular Diseases in Both Sexes: Differences and Relative Prognostic Impact
6.1. Under-Treatment
6.2. Cardiac Rehabilitation
6.3. Gender Disparities in Adherence and Responses to Treatments
6.4. Outcomes
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Di Giosia, P.; Passacquale, G.; Petrarca, M.; Giorgini, P.; Marra, A.M.; Ferro, A. Gender differences in cardiovascular prophylaxis: Focus on antiplatelet treatment. Pharm. Res. 2017, 119, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Mendirichaga, R.; Jacobs, A.K. Sex Differences in Ischemic Heart Disease-the Paradox Persists. JAMA Cardiol. 2020, 5, 754–756. [Google Scholar] [CrossRef] [PubMed]
- Timmis, A.; Townsend, N.; Gale, C.; Grobbee, R.; Maniadakis, N.; Flather, M.; Wilkins, E.; Wright, L.; Vos, R.; Bax, J.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2017. Eur. Heart J. 2018, 39, 508–579. [Google Scholar] [CrossRef]
- Ghare, M.I.; Chandrasekhar, J.; Mehran, R.; Ng, V.; Grines, C.; Lansky, A. Sex Disparities in Cardiovascular Device Evaluations: Strategies for Recruitment and Retention of Female Patients in Clinical Device Trials. JACC Cardiovasc. Interv. 2019, 12, 301–308. [Google Scholar] [CrossRef]
- Connelly, P.J.; Azizi, Z.; Alipour, P.; Delles, C.; Pilote, L.; Raparelli, V. The Importance of Gender to Understand Sex Differences in Cardiovascular Disease. Can. J. Cardiol. 2021, 37, 699–710. [Google Scholar] [CrossRef]
- Calabrò, P.; Niccoli, G.; Gragnano, F.; Grove, E.L.; Vergallo, R.; Mikhailidis, D.P.; Patti, G.; Spaccarotella, C.; Katsiki, N.; Masiero, G.; et al. Are we ready for a gender-specific approach in interventional cardiology? Int. J. Cardiol. 2019, 286, 226–233. [Google Scholar] [CrossRef]
- Steinberg, J.R.; Turner, B.E.; Weeks, B.T.; Magnani, C.J.; Wong, B.O.; Rodriguez, F.; Yee, L.M.; Cullen, M.R. Analysis of Female Enrollment and Participant Sex by Burden of Disease in US Clinical Trials Between 2000 and 2020. JAMA Netw. Open 2021, 4, e2113749. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.T.; James, S.K.; Wang, T.Y. A review of sex-specific benefits and risks of antithrombotic therapy in acute coronary syndrome. Eur. Heart J. 2017, 38, 165–171. [Google Scholar] [CrossRef]
- Mazurek, M.; Huisman, M.V.; Rothman, K.J.; Paquette, M.; Teutsch, C.; Diener, H.C.; Dubner, S.J.; Halperin, J.L.; Zint, K.; França, L.R.; et al. Gender Differences in Antithrombotic Treatment for Newly Diagnosed Atrial Fibrillation: The GLORIA-AF Registry Program. Am. J. Med. 2018, 131, 945–955.e943. [Google Scholar] [CrossRef]
- De Smedt, D.; De Bacquer, D.; De Sutter, J.; Dallongeville, J.; Gevaert, S.; De Backer, G.; Bruthans, J.; Kotseva, K.; Reiner, Ž.; Tokgözoğlu, L.; et al. The gender gap in risk factor control: Effects of age and education on the control of cardiovascular risk factors in male and female coronary patients. The EUROASPIRE IV study by the European Society of Cardiology. Int. J. Cardiol. 2016, 209, 284–290. [Google Scholar] [CrossRef]
- De Smedt, D.; Kotseva, K.; De Backer, G.; Wood, D.; Van Wilder, L.; De Bacquer, D. EQ-5D in coronary patients: What are they suffering from? Results from the ESC EORP European Survey of Cardiovascular Disease Prevention and Diabetes (EUROASPIRE IV) Registry. Qual. Life Res. 2020, 29, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Kotseva, K.; De Backer, G.; De Bacquer, D.; Rydén, L.; Hoes, A.; Grobbee, D.; Maggioni, A.; Marques-Vidal, P.; Jennings, C.; Abreu, A.; et al. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: Results from the European Society of Cardiology ESC-EORP EUROASPIRE V registry. Eur. J. Prev. Cardiol. 2019, 26, 824–835. [Google Scholar] [CrossRef] [PubMed]
- Vynckier, P.; Ferrannini, G.; Rydén, L.; Jankowski, P.; De Backer, T.; Gevaert, S.; De Bacquer, D.; De Smedt, D. Gender gap in risk factor control of coronary patients far from closing: Results from the European Society of Cardiology EUROASPIRE V registry. Eur. J. Prev. Cardiol. 2021. [Google Scholar] [CrossRef]
- Vynckier, P.; Kotseva, K.; Gevaert, S.; De Bacquer, D.; De Smedt, D.; Investigators, E.V. Gender differences in cardiovascular risk factor awareness: Results from the ESC EORP EUROASPIRE V Registry. Int. J. Cardiol. 2022, in press. [Google Scholar] [CrossRef]
- Fuchs, F.D.; Whelton, P.K. High Blood Pressure and Cardiovascular Disease. Hypertension 2020, 75, 285–292. [Google Scholar] [CrossRef]
- Srivaratharajah, K.; Abramson, B.L. Hypertension in menopausal women: The effect and role of estrogen. Menopause 2019, 26, 428–430. [Google Scholar] [CrossRef]
- Ramirez, L.A.; Sullivan, J.C. Sex Differences in Hypertension: Where We Have Been and Where We Are Going. Am. J. Hypertens. 2018, 31, 1247–1254. [Google Scholar] [CrossRef]
- Beale, A.L.; Meyer, P.; Marwick, T.H.; Lam, C.S.P.; Kaye, D.M. Sex Differences in Cardiovascular Pathophysiology: Why Women Are Overrepresented in Heart Failure with Preserved Ejection Fraction. Circulation 2018, 138, 198–205. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Sabbatini, A.R.; Kararigas, G. Estrogen-related mechanisms in sex differences of hypertension and target organ damage. Biol. Sex Differ. 2020, 11, 31. [Google Scholar] [CrossRef]
- Song, J.J.; Ma, Z.; Wang, J.; Chen, L.X.; Zhong, J.C. Gender Differences in Hypertension. J. Cardiovasc. Transl. Res. 2020, 13, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, F.; Woodward, M.; Neal, B.; Barzi, F.; Ninomiya, T.; Chalmers, J.; Perkovic, V.; Li, N.; MacMahon, S. Do men and women respond differently to blood pressure-lowering treatment? Results of prospectively designed overviews of randomized trials. Eur. Heart J. 2008, 29, 2669–2680. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.T., Jr.; Williamson, J.D.; Whelton, P.K.; Snyder, J.K.; Sink, K.M.; Rocco, M.V.; Reboussin, D.M.; Rahman, M.; Oparil, S.; Lewis, C.E.; et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N. Engl. J. Med. 2015, 373, 2103–2116. [Google Scholar] [CrossRef]
- Kalibala, J.; Pechère-Bertschi, A.; Desmeules, J. Gender Differences in Cardiovascular Pharmacotherapy—The Example of Hypertension: A Mini Review. Front. Pharmacol. 2020, 11, 564. [Google Scholar] [CrossRef]
- Barochiner, J.; Martínez, R.; Aparicio, L.S. Novel Indices of Home Blood Pressure Variability and Hypertension-Mediated Organ Damage in Treated Hypertensive Patients. High Blood Press Cardiovasc. Prev. 2021, 28, 365–372. [Google Scholar] [CrossRef]
- DuPont, J.J.; Kenney, R.M.; Patel, A.R.; Jaffe, I.Z. Sex differences in mechanisms of arterial stiffness. Br. J. Pharm. 2019, 176, 4208–4225. [Google Scholar] [CrossRef]
- Cífková, R. Left ventricular hypertrophy in females with hypertension is associated with a poor prognosis. Int. J. Cardiol. 2018, 258, 277–278. [Google Scholar] [CrossRef]
- Muiesan, M.L.; Paini, A.; Aggiusti, C.; Bertacchini, F.; Rosei, C.A.; Salvetti, M. Hypertension and Organ Damage in Women. High Blood Press Cardiovasc. Prev. 2018, 25, 245–252. [Google Scholar] [CrossRef]
- Rexrode, K. Sex Differences in Sex Hormones, Carotid Atherosclerosis, and Stroke. Circ. Res. 2018, 122, 17–19. [Google Scholar] [CrossRef]
- Singh, N.; Moody, A.R.; Zhang, B.; Kaminski, I.; Kapur, K.; Chiu, S.; Tyrrell, P.N. Age-Specific Sex Differences in Magnetic Resonance Imaging-Depicted Carotid Intraplaque Hemorrhage. Stroke 2017, 48, 2129–2135. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, T.; Mielniczuk, L.M.; Srivaratharajah, K.; deKemp, R.; Wells, G.A.; Beanlands, R.S. Coronary artery microvascular dysfunction: Role of sex and arterial load. Int. J. Cardiol. 2018, 270, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Bairey Merz, C.N.; Pepine, C.J.; Shimokawa, H.; Berry, C. Treatment of coronary microvascular dysfunction. Cardiovasc. Res. 2020, 116, 856–870. [Google Scholar] [CrossRef] [PubMed]
- Padro, T.; Manfrini, O.; Bugiardini, R.; Canty, J.; Cenko, E.; De Luca, G.; Duncker, D.J.; Eringa, E.C.; Koller, A.; Tousoulis, D.; et al. ESC Working Group on Coronary Pathophysiology and Microcirculation position paper on ‘coronary microvascular dysfunction in cardiovascular disease’. Cardiovasc. Res. 2020, 116, 741–755. [Google Scholar] [CrossRef]
- Bruno, R.M.; Grassi, G.; Seravalle, G.; Savoia, C.; Rizzoni, D.; Virdis, A. Age- and Sex-Specific Reference Values for Media/Lumen Ratio in Small Arteries and Relationship with Risk Factors. Hypertension 2018, 71, 1193–1200. [Google Scholar] [CrossRef]
- Aimo, A.; Panichella, G.; Barison, A.; Maffei, S.; Cameli, M.; Coiro, S.; D’Ascenzi, F.; Di Mario, C.; Liga, R.; Marcucci, R.; et al. Sex-related differences in ventricular remodeling after myocardial infarction. Int. J. Cardiol. 2021, 339, 62–69. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Carrero, J.J.; Hecking, M.; Chesnaye, N.C.; Jager, K.J. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat. Rev. Nephrol. 2018, 14, 151–164. [Google Scholar] [CrossRef]
- Sullivan, J.C.; Gillis, E.E. Sex and gender differences in hypertensive kidney injury. Am. J. Physiol. Ren. Physiol. 2017, 313, F1009–F1017. [Google Scholar] [CrossRef]
- Dziedziak, J.; Zaleska-Żmijewska, A.; Szaflik, J.P.; Cudnoch-Jędrzejewska, A. Impact of Arterial Hypertension on the Eye: A Review of the Pathogenesis, Diagnostic Methods, and Treatment of Hypertensive Retinopathy. Med. Sci. Monit. 2022, 28, e935135. [Google Scholar] [CrossRef]
- Tsukikawa, M.; Stacey, A.W. A Review of Hypertensive Retinopathy and Chorioretinopathy. Clin. Optom. 2020, 12, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Mondal, R.; Matin, M.; Rani, M.; Hossain, M.; Shaha, A.; Singh, R.; Das, A. Prevalence and risk factors of hypertensive retinopathy in hypertensive patients. J. Hypertens. Open Access 2017, 6, 241. [Google Scholar] [CrossRef]
- Garcia, M.; Mulvagh, S.L.; Merz, C.N.; Buring, J.E.; Manson, J.E. Cardiovascular Disease in Women: Clinical Perspectives. Circ. Res. 2016, 118, 1273–1293. [Google Scholar] [CrossRef]
- Sattar, N.; Rawshani, A.; Franzén, S.; Rawshani, A.; Svensson, A.M.; Rosengren, A.; McGuire, D.K.; Eliasson, B.; Gudbjörnsdottir, S. Age at Diagnosis of Type 2 Diabetes Mellitus and Associations with Cardiovascular and Mortality Risks. Circulation 2019, 139, 2228–2237. [Google Scholar] [CrossRef]
- Harjasouliha, A.; Raiji, V.; Garcia Gonzalez, J.M. Review of hypertensive retinopathy. Dis. Mon. 2017, 63, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Dannenberg, L.; Weske, S.; Kelm, M.; Levkau, B.; Polzin, A. Cellular mechanisms and recommended drug-based therapeutic options in diabetic cardiomyopathy. Pharmacol. Ther. 2021, 228, 107920. [Google Scholar] [CrossRef]
- Cho, L.; Davis, M.; Elgendy, I.; Epps, K.; Lindley, K.J.; Mehta, P.K.; Michos, E.D.; Minissian, M.; Pepine, C.; Vaccarino, V.; et al. Summary of Updated Recommendations for Primary Prevention of Cardiovascular Disease in Women: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 2602–2618. [Google Scholar] [CrossRef]
- Chait, A.; den Hartigh, L.J. Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease. Front. Cardiovasc. Med. 2020, 7, 22. [Google Scholar] [CrossRef]
- Kautzky-Willer, A.; Harreiter, J.; Pacini, G. Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocr. Rev. 2016, 37, 278–316. [Google Scholar] [CrossRef]
- Cooper, A.J.; Gupta, S.R.; Moustafa, A.F.; Chao, A.M. Sex/Gender Differences in Obesity Prevalence, Comorbidities, and Treatment. Curr. Obes. Rep. 2021, 10, 458–466. [Google Scholar] [CrossRef]
- Nordström, A.; Hadrévi, J.; Olsson, T.; Franks, P.W.; Nordström, P. Higher Prevalence of Type 2 Diabetes in Men Than in Women Is Associated with Differences in Visceral Fat Mass. J. Clin. Endocrinol. Metab. 2016, 101, 3740–3746. [Google Scholar] [CrossRef] [PubMed]
- Gambineri, A.; Pelusi, C. Sex hormones, obesity and type 2 diabetes: Is there a link? Endocr. Connect 2019, 8, R1–R9. [Google Scholar] [CrossRef] [PubMed]
- Tramunt, B.; Smati, S.; Grandgeorge, N.; Lenfant, F.; Arnal, J.F.; Montagner, A.; Gourdy, P. Sex differences in metabolic regulation and diabetes susceptibility. Diabetologia 2020, 63, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Mascarenhas-Melo, F.; Marado, D.; Palavra, F.; Sereno, J.; Coelho, Á.; Pinto, R.; Teixeira-Lemos, E.; Teixeira, F.; Reis, F. Diabetes abrogates sex differences and aggravates cardiometabolic risk in postmenopausal women. Cardiovasc. Diabetol. 2013, 12, 61. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N. Type 2 diabetes-related sex differences in cardiovascular risk: Reasons, ramifications, and clinical realities. Eur. Heart J. 2020, 41, 1354–1356. [Google Scholar] [CrossRef]
- National Center for Health Statistics. Health, United States. In Health, United States, 2009: With Special Feature on Medical Technology; National Center for Health Statistics: Hyattsville, MD, USA, 2010. [Google Scholar]
- Giampaoli, S.; Vanuzzo, D.; Palmieri, L.; Lo Noce, C.; Dima, F.; De Sanctis Caiola, P.; Donfrancesco, C.; Ciccarelli, P.; Toccaceli, V. Progetto Cuore. Epidemiologia e Prevenzione delle Malattie Cerebro e Cardiovascolari. Available online: http://www.cuore.iss.it/ehes/default.asp (accessed on 13 February 2022).
- Vogel, B.; Acevedo, M.; Appelman, Y.; Bairey Merz, C.N.; Chieffo, A.; Figtree, G.A.; Guerrero, M.; Kunadian, V.; Lam, C.S.P.; Maas, A.; et al. The Lancet women and cardiovascular disease Commission: Reducing the global burden by 2030. Lancet 2021, 397, 2385–2438. [Google Scholar] [CrossRef]
- Matthews, K.A.; Crawford, S.L.; Chae, C.U.; Everson-Rose, S.A.; Sowers, M.F.; Sternfeld, B.; Sutton-Tyrrell, K. Are changes in cardiovascular disease risk factors in midlife women due to chronological aging or to the menopausal transition? J. Am. Coll. Cardiol. 2009, 54, 2366–2373. [Google Scholar] [CrossRef]
- Matthews, K.A.; El Khoudary, S.R.; Brooks, M.M.; Derby, C.A.; Harlow, S.D.; Barinas-Mitchell, E.J.; Thurston, R.C. Lipid Changes Around the Final Menstrual Period Predict Carotid Subclinical Disease in Postmenopausal Women. Stroke 2017, 48, 70–76. [Google Scholar] [CrossRef]
- Joakimsen, O.; Bønaa, K.H.; Stensland-Bugge, E.; Jacobsen, B.K. Population-based study of age at menopause and ultrasound assessed carotid atherosclerosis: The Tromsø Study. J. Clin. Epidemiol. 2000, 53, 525–530. [Google Scholar] [CrossRef]
- Matthews, K.A.; Kuller, L.H.; Sutton-Tyrrell, K.; Chang, Y.F. Changes in cardiovascular risk factors during the perimenopause and postmenopause and carotid artery atherosclerosis in healthy women. Stroke 2001, 32, 1104–1111. [Google Scholar] [CrossRef]
- McQueen, M.J.; Hawken, S.; Wang, X.; Ounpuu, S.; Sniderman, A.; Probstfield, J.; Steyn, K.; Sanderson, J.E.; Hasani, M.; Volkova, E.; et al. Lipids, lipoproteins, and apolipoproteins as risk markers of myocardial infarction in 52 countries (the INTERHEART study): A case-control study. Lancet 2008, 372, 224–233. [Google Scholar] [CrossRef]
- Fulcher, J.; O’Connell, R.; Voysey, M.; Emberson, J.; Blackwell, L.; Mihaylova, B.; Simes, J.; Collins, R.; Kirby, A.; Colhoun, H.; et al. Efficacy and safety of LDL-lowering therapy among men and women: Meta-analysis of individual data from 174,000 participants in 27 randomised trials. Lancet 2015, 385, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- WHO Report on the Global Tobacco Epidemic. Available online: http://www.who.int/tobacco/global_report/2015/summary/en/) (accessed on 13 February 2022).
- Anand, S.S.; Islam, S.; Rosengren, A.; Franzosi, M.G.; Steyn, K.; Yusufali, A.H.; Keltai, M.; Diaz, R.; Rangarajan, S.; Yusuf, S. Risk factors for myocardial infarction in women and men: Insights from the INTERHEART study. Eur. Heart J. 2008, 29, 932–940. [Google Scholar] [CrossRef] [PubMed]
- Gallucci, G.; Tartarone, A.; Lerose, R.; Lalinga, A.V.; Capobianco, A.M. Cardiovascular risk of smoking and benefits of smoking cessation. J. Thorac. Dis. 2020, 12, 3866–3876. [Google Scholar] [CrossRef]
- Health 2020 Indicators by World Health Organization. Available online: https://gateway.euro.who.int/en/datasets/health-2020-indicators/ (accessed on 13 February 2022).
- Reilly, J.J.; El-Hamdouchi, A.; Diouf, A.; Monyeki, A.; Somda, S.A. Determining the worldwide prevalence of obesity. Lancet 2018, 391, 1773–1774. [Google Scholar] [CrossRef]
- Garawi, F.; Devries, K.; Thorogood, N.; Uauy, R. Global differences between women and men in the prevalence of obesity: Is there an association with gender inequality? Eur. J. Clin. Nutr. 2014, 68, 1101–1106. [Google Scholar] [CrossRef]
- Lewandowska, M.; Więckowska, B.; Sajdak, S. Pre-Pregnancy Obesity, Excessive Gestational Weight Gain, and the Risk of Pregnancy-Induced Hypertension and Gestational Diabetes Mellitus. J. Clin. Med. 2020, 9, 1980. [Google Scholar] [CrossRef]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist circumference as a vital sign in clinical practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef]
- Wilson, P.W.; D’Agostino, R.B.; Sullivan, L.; Parise, H.; Kannel, W.B. Overweight and obesity as determinants of cardiovascular risk: The Framingham experience. Arch. Intern. Med. 2002, 162, 1867–1872. [Google Scholar] [CrossRef]
- Chen, G.C.; Arthur, R.; Iyengar, N.M.; Kamensky, V.; Xue, X.; Wassertheil-Smoller, S.; Allison, M.A.; Shadyab, A.H.; Wild, R.A.; Sun, Y.; et al. Association between regional body fat and cardiovascular disease risk among postmenopausal women with normal body mass index. Eur. Heart J. 2019, 40, 2849–2855. [Google Scholar] [CrossRef]
- Oyewande, A.A.; Iqbal, B.; Abdalla, L.F.; Karim, F.; Khan, S. An Overview of the Pathophysiology of Metabolic Changes and Their Sequence of Occurrence in Obese Diabetic Females: A Narrative Review. Cureus 2020, 12, e10947. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Jefferis, B.J.; Sartini, C.; Lee, I.M.; Choi, M.; Amuzu, A.; Gutierrez, C.; Casas, J.P.; Ash, S.; Lennnon, L.T.; Wannamethee, S.G.; et al. Adherence to physical activity guidelines in older adults, using objectively measured physical activity in a population-based study. BMC Public Health 2014, 14, 382. [Google Scholar] [CrossRef] [PubMed]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Jankowski, J.; Floege, J.; Fliser, D.; Böhm, M.; Marx, N. Cardiovascular Disease in Chronic Kidney Disease: Pathophysiological Insights and Therapeutic Options. Circulation 2021, 143, 1157–1172. [Google Scholar] [CrossRef]
- Carney, E.F. The impact of chronic kidney disease on global health. Nat. Rev. Nephrol. 2020, 16, 251. [Google Scholar] [CrossRef]
- Bikbov, B.; Perico, N.; Remuzzi, G. Disparities in Chronic Kidney Disease Prevalence among Males and Females in 195 Countries: Analysis of the Global Burden of Disease 2016 Study. Nephron 2018, 139, 313–318. [Google Scholar] [CrossRef]
- Franco-Acevedo, A.; Echavarria, R.; Melo, Z. Sex Differences in Renal Function: Participation of Gonadal Hormones and Prolactin. Endocrines 2021, 2, 19. [Google Scholar] [CrossRef]
- Rider, V.; Abdou, N.I.; Kimler, B.F.; Lu, N.; Brown, S.; Fridley, B.L. Gender Bias in Human Systemic Lupus Erythematosus: A Problem of Steroid Receptor Action? Front. Immunol. 2018, 9, 611. [Google Scholar] [CrossRef]
- Ramírez Sepúlveda, J.I.; Bolin, K.; Mofors, J.; Leonard, D.; Svenungsson, E.; Jönsen, A.; Bengtsson, C.; Nordmark, G.; Rantapää Dahlqvist, S.; Bengtsson, A.A.; et al. Sex differences in clinical presentation of systemic lupus erythematosus. Biol. Sex Differ. 2019, 10, 60. [Google Scholar] [CrossRef]
- Bomback, A.S. Nonproliferative Forms of Lupus Nephritis: An Overview. Rheum. Dis. Clin. N. Am. 2018, 44, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Peoples, C.; Medsger, T.A., Jr.; Lucas, M.; Rosario, B.L.; Feghali-Bostwick, C.A. Gender differences in systemic sclerosis: Relationship to clinical features, serologic status and outcomes. J. Scleroderma Relat. Disord. 2016, 1, 177–240. [Google Scholar] [CrossRef] [PubMed]
- Herness, J.; Buttolph, A.; Hammer, N.C. Acute Pyelonephritis in Adults: Rapid Evidence Review. Am. Fam. Physician 2020, 102, 173–180. [Google Scholar] [PubMed]
- Szczepanski, J.; Griffin, A.; Novotny, S.; Wallace, K. Acute Kidney Injury in Pregnancies Complicated with Preeclampsia or HELLP Syndrome. Front. Med. 2020, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Prado, R.; Fernandez-Fernandez, B.; Ortiz, A. Women and renal replacement therapy in Europe: Lower incidence, equal access to transplantation, longer survival than men. Clin. Kidney J. 2018, 11, 1–6. [Google Scholar] [CrossRef]
- Brar, A.; Markell, M. Impact of gender and gender disparities in patients with kidney disease. Curr. Opin. Nephrol. Hypertens 2019, 28, 178–182. [Google Scholar] [CrossRef]
- Benson, C.; Shah, A.; Stanworth, S.; Frise, C.; Spiby, H.; Lax, S.; Murray, J.; Klein, A. The effect of iron deficiency and anaemia on women’s health. Anaesthesia 2021, 76, 84–95. [Google Scholar] [CrossRef]
- Percy, L.; Mansour, D.; Fraser, I. Iron deficiency and iron deficiency anaemia in women. Best Pract. Res. Clin. Obs. Gynaecol. 2017, 40, 55–67. [Google Scholar] [CrossRef]
- Daru, J.; Zamora, J.; Fernández-Félix, B.M.; Vogel, J.; Oladapo, O.T.; Morisaki, N.; Tunçalp, Ö.; Torloni, M.R.; Mittal, S.; Jayaratne, K.; et al. Risk of maternal mortality in women with severe anaemia during pregnancy and post partum: A multilevel analysis. Lancet Glob. Health 2018, 6, e548–e554. [Google Scholar] [CrossRef]
- Mansour, D.; Hofmann, A.; Gemzell-Danielsson, K. A Review of Clinical Guidelines on the Management of Iron Deficiency and Iron-Deficiency Anemia in Women with Heavy Menstrual Bleeding. Adv. Ther. 2021, 38, 201–225. [Google Scholar] [CrossRef]
- Coad, J.; Pedley, K. Iron deficiency and iron deficiency anemia in women. Scand. J. Clin. Lab. Investig. Suppl. 2014, 244, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, C.M.; Suchdev, P.S. Anemia epidemiology, pathophysiology, and etiology in low- and middle-income countries. Ann. N. Y. Acad. Sci. 2019, 1450, 15–31. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Anaemia Reduction Efforts among Women of Reproductive Age: Impact, Achievement of Targets and the Way forward for Optimizing Efforts; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Sebastiani, G.; Herranz Barbero, A.; Borrás-Novell, C.; Alsina Casanova, M.; Aldecoa-Bilbao, V.; Andreu-Fernández, V.; Pascual Tutusaus, M.; Ferrero Martínez, S.; Gómez Roig, M.D.; García-Algar, O. The Effects of Vegetarian and Vegan Diet during Pregnancy on the Health of Mothers and Offspring. Nutrients 2019, 11, 557. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Ye, H.; Liu, J.; Ma, Q.; Yuan, Y.; Pang, Q.; Liu, J.; Kong, C.; Liu, M. Prevalence of anemia and sociodemographic characteristics among pregnant and non-pregnant women in southwest China: A longitudinal observational study. BMC Pregnancy Childbirth 2020, 20, 535. [Google Scholar] [CrossRef]
- Ru, Y.; Pressman, E.K.; Cooper, E.M.; Guillet, R.; Katzman, P.J.; Kent, T.R.; Bacak, S.J.; O’Brien, K.O. Iron deficiency and anemia are prevalent in women with multiple gestations. Am. J. Clin. Nutr. 2016, 104, 1052–1060. [Google Scholar] [CrossRef]
- Sonoda, K. Iron Deficiency Anemia: Guidelines from the American Gastroenterological Association. Am. Fam. Physician 2021, 104, 211–212. [Google Scholar]
- Khedagi, A.M.; Bello, N.A. Hypertensive Disorders of Pregnancy. Cardiol. Clin. 2021, 39, 77–90. [Google Scholar] [CrossRef]
- Abrignani, M.G. Searching Novel Approaches to Cardiovascular Risk: Hypertensive Disorders of Pregnancy. Cardiology 2020, 145, 648–651. [Google Scholar] [CrossRef]
- Ahmad, A.; Oparil, S. Hypertension in Women: Recent Advances and Lingering Questions. Hypertension 2017, 70, 19–26. [Google Scholar] [CrossRef]
- Morikawa, M.; Mayama, M.; Noshiro, K.; Saito, Y.; Nakagawa-Akabane, K.; Umazume, T.; Chiba, K.; Kawaguchi, S.; Watari, H. Earlier onset of proteinuria or hypertension is a predictor of progression from gestational hypertension or gestational proteinuria to preeclampsia. Sci. Rep. 2021, 11, 12708. [Google Scholar] [CrossRef]
- Hu, X.; Zhang, L. Uteroplacental Circulation in Normal Pregnancy and Preeclampsia: Functional Adaptation and Maladaptation. Int. J. Mol. Sci. 2021, 22, 8622. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.D.; Malinowski, A.; Zhou, Q.; Yusuf, S.; Devereaux, P.J. Cardiovascular sequelae of preeclampsia/eclampsia: A systematic review and meta-analyses. Am. Heart J. 2008, 156, 918–930. [Google Scholar] [CrossRef] [PubMed]
- Tobias, D.K.; Stuart, J.J.; Li, S.; Chavarro, J.; Rimm, E.B.; Rich-Edwards, J.; Hu, F.B.; Manson, J.E.; Zhang, C. Association of History of Gestational Diabetes with Long-term Cardiovascular Disease Risk in a Large Prospective Cohort of US Women. JAMA Intern. Med. 2017, 177, 1735–1742. [Google Scholar] [CrossRef] [PubMed]
- Clemmensen, T.S.; Christensen, M.; Løgstrup, B.B.; Kronborg, C.J.S.; Knudsen, U.B. Reduced coronary flow velocity reserve in women with previous pre-eclampsia: Link to increased cardiovascular disease risk. Ultrasound Obs. Gynecol. 2020, 55, 786–792. [Google Scholar] [CrossRef]
- Lui, N.A.; Jeyaram, G.; Henry, A. Postpartum Interventions to Reduce Long-Term Cardiovascular Disease Risk in Women after Hypertensive Disorders of Pregnancy: A Systematic Review. Front. Cardiovasc. Med. 2019, 6, 160. [Google Scholar] [CrossRef]
- Witchel, S.F.; Oberfield, S.E.; Peña, A.S. Polycystic Ovary Syndrome: Pathophysiology, Presentation, and Treatment with Emphasis on Adolescent Girls. J. Endocr. Soc. 2019, 3, 1545–1573. [Google Scholar] [CrossRef]
- Bozdag, G.; Mumusoglu, S.; Zengin, D.; Karabulut, E.; Yildiz, B.O. The prevalence and phenotypic features of polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. 2016, 31, 2841–2855. [Google Scholar] [CrossRef]
- Sadeghi, H.M.; Adeli, I.; Calina, D.; Docea, A.O.; Mousavi, T.; Daniali, M.; Nikfar, S.; Tsatsakis, A.; Abdollahi, M. Polycystic Ovary Syndrome: A Comprehensive Review of Pathogenesis, Management, and Drug Repurposing. Int. J. Mol. Sci. 2022, 23, 583. [Google Scholar] [CrossRef]
- Boomsma, C.M.; Eijkemans, M.J.; Hughes, E.G.; Visser, G.H.; Fauser, B.C.; Macklon, N.S. A meta-analysis of pregnancy outcomes in women with polycystic ovary syndrome. Hum. Reprod. Update 2006, 12, 673–683. [Google Scholar] [CrossRef]
- Osibogun, O.; Ogunmoroti, O.; Michos, E.D. Polycystic ovary syndrome and cardiometabolic risk: Opportunities for cardiovascular disease prevention. Trends Cardiovasc. Med. 2020, 30, 399–404. [Google Scholar] [CrossRef]
- Sohn, E. Why autoimmunity is most common in women. Nature 2021, 595, S51–S53. [Google Scholar] [CrossRef]
- Young, L.; Cho, L. Unique cardiovascular risk factors in women. Heart 2019, 105, 1656–1660. [Google Scholar] [CrossRef] [PubMed]
- DeMizio, D.J.; Geraldino-Pardilla, L.B. Autoimmunity and Inflammation Link to Cardiovascular Disease Risk in Rheumatoid Arthritis. Rheumatology 2020, 7, 19–33. [Google Scholar] [CrossRef]
- Morimont, L.; Haguet, H.; Dogné, J.-M.; Gaspard, U.; Douxfils, J. Combined Oral Contraceptives and Venous Thromboembolism: Review and Perspective to Mitigate the Risk. Front. Endocrinol. 2021, 12, 769187. [Google Scholar] [CrossRef] [PubMed]
- ACOG Practice Bulletin No. 206: Use of Hormonal Contraception in Women with Coexisting Medical Conditions. Obs. Gynecol. 2019, 133, e128–e150. [CrossRef]
- Xu, Z.; Yue, Y.; Bai, J.; Shen, C.; Yang, J.; Huang, X.; Zhao, Y.; Li, Y. Association between oral contraceptives and risk of hemorrhagic stroke: A meta-analysis of observational studies. Arch. Gynecol. Obs. 2018, 297, 1181–1191. [Google Scholar] [CrossRef]
- Demel, S.L.; Kittner, S.; Ley, S.H.; McDermott, M.; Rexrode, K.M. Stroke Risk Factors Unique to Women. Stroke 2018, 49, 518–523. [Google Scholar] [CrossRef]
- Li, F.; Zhu, L.; Zhang, J.; He, H.; Qin, Y.; Cheng, Y.; Xie, Z. Oral Contraceptive Use and Increased Risk of Stroke: A Dose-Response Meta-Analysis of Observational Studies. Front. Neurol. 2019, 10, 993. [Google Scholar] [CrossRef]
- Sacco, S.; Merki-Feld, G.S.; Ægidius, K.L.; Bitzer, J.; Canonico, M.; Kurth, T.; Lampl, C.; Lidegaard, Ø.; Anne MacGregor, E.; MaassenVanDenBrink, A.; et al. Hormonal contraceptives and risk of ischemic stroke in women with migraine: A consensus statement from the European Headache Federation (EHF) and the European Society of Contraception and Reproductive Health (ESC). J. Headache Pain 2017, 18, 108. [Google Scholar] [CrossRef]
- Yemisci, M.; Eikermann-Haerter, K. Aura and Stroke: Relationship and what we have learnt from preclinical models. J. Headache Pain 2019, 20, 1–8. [Google Scholar] [CrossRef]
- Allen, A.M.; Weinberger, A.H.; Wetherill, R.R.; Howe, C.L.; McKee, S.A. Oral Contraceptives and Cigarette Smoking: A Review of the Literature and Future Directions. Nicotine Tob. Res. 2019, 21, 592–601. [Google Scholar] [CrossRef] [PubMed]
- Wenger, N.K.; Arnold, A.; Bairey Merz, C.N.; Cooper-DeHoff, R.M.; Ferdinand, K.C.; Fleg, J.L.; Gulati, M.; Isiadinso, I.; Itchhaporia, D.; Light-McGroary, K.; et al. Hypertension Across a Woman’s Life Cycle. J. Am. Coll. Cardiol. 2018, 71, 1797–1813. [Google Scholar] [CrossRef] [PubMed]
- Serfaty, D. Update on the contraceptive contraindications. J. Gynecol. Obs. Hum. Reprod. 2019, 48, 297–307. [Google Scholar] [CrossRef]
- Glenn, T.; Kallen, A. Early menopause: Diagnosis and management. In Psychological and Medical Perspectives on Fertility Care and Sexual Health; Elsevier: Amsterdam, The Netherlands, 2022; pp. 93–104. [Google Scholar]
- Zhu, D.; Chung, H.F.; Dobson, A.J.; Pandeya, N.; Giles, G.G.; Bruinsma, F.; Brunner, E.J.; Kuh, D.; Hardy, R.; Avis, N.E.; et al. Age at natural menopause and risk of incident cardiovascular disease: A pooled analysis of individual patient data. Lancet Public Health 2019, 4, e553–e564. [Google Scholar] [CrossRef]
- Ueda, K.; Fukuma, N.; Adachi, Y.; Numata, G.; Tokiwa, H.; Toyoda, M.; Otani, A.; Hashimoto, M.; Liu, P.Y.; Takimoto, E. Sex Differences and Regulatory Actions of Estrogen in Cardiovascular System. Front. Physiol. 2021, 12, 738218. [Google Scholar] [CrossRef] [PubMed]
- Chester, R.C.; Kling, J.M.; Manson, J.E. What the Women’s Health Initiative has taught us about menopausal hormone therapy. Clin. Cardiol. 2018, 41, 247–252. [Google Scholar] [CrossRef]
- Hulley, S.; Grady, D.; Bush, T.; Furberg, C.; Herrington, D.; Riggs, B.; Vittinghoff, E. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. Heart and Estrogen/progestin Replacement Study (HERS) Research Group. JAMA 1998, 280, 605–613. [Google Scholar] [CrossRef]
- El Khoudary, S.R.; Aggarwal, B.; Beckie, T.M.; Hodis, H.N.; Johnson, A.E.; Langer, R.D.; Limacher, M.C.; Manson, J.E.; Stefanick, M.L.; Allison, M.A. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement from the American Heart Association. Circulation 2020, 142, e506–e532. [Google Scholar] [CrossRef]
- Mehta, J.; Kling, J.M.; Manson, J.E. Risks, Benefits, and Treatment Modalities of Menopausal Hormone Therapy: Current Concepts. Front. Endocrinol. 2021, 12, 564781. [Google Scholar] [CrossRef]
- Dam, V.; van der Schouw, Y.T.; Onland-Moret, N.C.; Groenwold, R.H.H.; Peters, S.A.E.; Burgess, S.; Wood, A.M.; Chirlaque, M.D.; Moons, K.G.M.; Oliver-Williams, C.; et al. Association of menopausal characteristics and risk of coronary heart disease: A pan-European case-cohort analysis. Int. J. Epidemiol. 2019, 48, 1275–1285. [Google Scholar] [CrossRef]
- Honigberg, M.C.; Zekavat, S.M.; Aragam, K.; Finneran, P.; Klarin, D.; Bhatt, D.L.; Januzzi, J.L., Jr.; Scott, N.S.; Natarajan, P. Association of Premature Natural and Surgical Menopause with Incident Cardiovascular Disease. JAMA 2019, 322, 2411–2421. [Google Scholar] [CrossRef] [PubMed]
- Rossouw, J.E.; Anderson, G.L.; Prentice, R.L.; LaCroix, A.Z.; Kooperberg, C.; Stefanick, M.L.; Jackson, R.D.; Beresford, S.A.; Howard, B.V.; Johnson, K.C.; et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results from the Women’s Health Initiative randomized controlled trial. JAMA 2002, 288, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Capewell, S. Coronary heart disease mortality among young adults in the U.S. from 1980 through 2002: Concealed leveling of mortality rates. J. Am. Coll. Cardiol. 2007, 50, 2128–2132. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B.; Hjortland, M.C.; McNamara, P.M.; Gordon, T. Menopause and risk of cardiovascular disease: The Framingham study. Ann. Intern. Med. 1976, 85, 447–452. [Google Scholar] [CrossRef]
- Setny, M.; Jankowski, P.; Kamiński, K.; Gąsior, Z.; Haberka, M.; Czarnecka, D.; Pająk, A.; Kozieł, P.; Szóstak-Janiak, K.; Sawicka, E.; et al. Secondary prevention of coronary heart disease in Poland: Does gender matter? Results from POLASPIRE survey. Pol. Arch. Intern. Med. 2021. [Google Scholar] [CrossRef]
- Vaccarino, V.; Parsons, L.; Every, N.R.; Barron, H.V.; Krumholz, H.M. Sex-based differences in early mortality after myocardial infarction. National Registry of Myocardial Infarction 2 Participants. N. Engl. J. Med. 1999, 341, 217–225. [Google Scholar] [CrossRef]
- Puymirat, E.; Simon, T.; Steg, P.G.; Schiele, F.; Guéret, P.; Blanchard, D.; Khalife, K.; Goldstein, P.; Cattan, S.; Vaur, L.; et al. Association of changes in clinical characteristics and management with improvement in survival among patients with ST-elevation myocardial infarction. JAMA 2012, 308, 998–1006. [Google Scholar] [CrossRef]
- Shehab, A.; Bhagavathula, A.S.; Alhabib, K.F.; Ullah, A.; Suwaidi, J.A.; Almahmeed, W.; AlFaleh, H.; Zubaid, M. Age-Related Sex Differences in Clinical Presentation, Management, and Outcomes in ST-Segment-Elevation Myocardial Infarction: Pooled Analysis of 15 532 Patients from 7 Arabian Gulf Registries. J. Am. Heart Assoc. 2020, 9, e013880. [Google Scholar] [CrossRef]
- Gao, Z.; Chen, Z.; Sun, A.; Deng, X. Gender differences in cardiovascular disease. Med. Nov. Technol. Devices 2019, 4, 100025. [Google Scholar] [CrossRef]
- Dey, S.; Flather, M.D.; Devlin, G.; Brieger, D.; Gurfinkel, E.P.; Steg, P.G.; Fitzgerald, G.; Jackson, E.A.; Eagle, K.A. Sex-related differences in the presentation, treatment and outcomes among patients with acute coronary syndromes: The Global Registry of Acute Coronary Events. Heart 2009, 95, 20–26. [Google Scholar] [CrossRef]
- Hao, Y.; Liu, J.; Liu, J.; Yang, N.; Smith, S.C., Jr.; Huo, Y.; Fonarow, G.C.; Ge, J.; Taubert, K.A.; Morgan, L.; et al. Sex Differences in In-Hospital Management and Outcomes of Patients with Acute Coronary Syndrome. Circulation 2019, 139, 1776–1785. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.M.; Zhang, R.; Findlay, I.; Robertson, K.; Lindsay, M.; Morris, T.; Forbes, B.; Papworth, R.; McConnachie, A.; Mangion, K.; et al. Healthcare disparities for women hospitalized with myocardial infarction and angina. Eur. Heart J. Qual. Care Clin. Outcomes 2020, 6, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Spirito, A.; Gragnano, F.; Corpataux, N.; Vaisnora, L.; Galea, R.; Svab, S.; Gargiulo, G.; Siontis, G.C.M.; Praz, F.; Lanz, J.; et al. Sex-Based Differences in Bleeding Risk After Percutaneous Coronary Intervention and Implications for the Academic Research Consortium High Bleeding Risk Criteria. J. Am. Heart Assoc. 2021, 10, e021965. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.O.; Kim, C.J.; Kim, W.; Cho, J.M.; Soeda, T.; Takano, M.; Yan, B.P.; Crea, F.; Niccoli, G.; Vergallo, R.; et al. Relative risk of plaque erosion among different age and sex groups in patients with acute coronary syndrome. J. Thromb. Thrombolysis 2020, 49, 352–359. [Google Scholar] [CrossRef]
- Tamis-Holland, J.E.; Jneid, H.; Reynolds, H.R.; Agewall, S.; Brilakis, E.S.; Brown, T.M.; Lerman, A.; Cushman, M.; Kumbhani, D.J.; Arslanian-Engoren, C. Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: A scientific statement from the American Heart Association. Circulation 2019, 139, e891–e908. [Google Scholar] [CrossRef]
- Vancheri, F.; Longo, G.; Vancheri, S.; Henein, M. Coronary microvascular dysfunction. J. Clin. Med. 2020, 9, 2880. [Google Scholar] [CrossRef]
- Vogel, B.; Goel, R.; Kunadian, V.; Kalkman, D.N.; Chieffo, A.; Appelman, Y.; Mehran, R. Residual angina in female patients after coronary revascularization. Int. J. Cardiol. 2019, 286, 208–213. [Google Scholar] [CrossRef]
- Rawish, E.; Stiermaier, T.; Santoro, F.; Brunetti, N.D.; Eitel, I. Current Knowledge and Future Challenges in Takotsubo Syndrome: Part 1—Pathophysiology and Diagnosis. J. Clin. Med. 2021, 10, 479. [Google Scholar] [CrossRef]
- Medina de Chazal, H.; Del Buono, M.G.; Keyser-Marcus, L.; Ma, L.; Moeller, F.G.; Berrocal, D.; Abbate, A. Stress Cardiomyopathy Diagnosis and Treatment: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 1955–1971. [Google Scholar] [CrossRef]
- Hayes, S.N.; Tweet, M.S.; Adlam, D.; Kim, E.S.; Gulati, R.; Price, J.E.; Rose, C.H. Spontaneous coronary artery dissection: JACC state-of-the-art review. J. Am. Coll. Cardiol. 2020, 76, 961–984. [Google Scholar] [CrossRef]
- Daoulah, A.; Al-Faifi, S.M.; Hersi, A.S.; Dinas, P.C.; Youssef, A.A.; Alshehri, M.; Baslaib, F.; Maghrabi, M.; Al-Murayeh, M.; Ghani, M.A.; et al. Spontaneous Coronary Artery Dissection in Relation to Physical and Emotional Stress: A Retrospective Study in 4 Arab Gulf Countries. Curr. Probl. Cardiol. 2021, 46, 100484. [Google Scholar] [CrossRef] [PubMed]
- Aziz, S. Spontaneous Coronary Artery Dissection. E. J. Cardiol. Pract. 2017, 14. Available online: https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-14 (accessed on 13 February 2022).
- Hayes, S.N.; Kim, E.S.H.; Saw, J.; Adlam, D.; Arslanian-Engoren, C.; Economy, K.E.; Ganesh, S.K.; Gulati, R.; Lindsay, M.E.; Mieres, J.H.; et al. Spontaneous Coronary Artery Dissection: Current State of the Science: A Scientific Statement from the American Heart Association. Circulation 2018, 137, e523–e557. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.; Samuel, R.; Starovoytov, A.; Lee, C.; Aymong, E.; Saw, J. Outcomes of Percutaneous Coronary Intervention in Patients with Spontaneous Coronary Artery Dissection. J. Interv. Cardiol. 2021, 2021, 6686230. [Google Scholar] [CrossRef] [PubMed]
- Ingrassia, J.; Diver, D.; Vashist, A. Update in Spontaneous Coronary Artery Dissection. J. Clin. Med. 2018, 7, 228. [Google Scholar] [CrossRef]
- Kunadian, V.; Chieffo, A.; Camici, P.G.; Berry, C.; Escaned, J.; Maas, A.; Prescott, E.; Karam, N.; Appelman, Y.; Fraccaro, C.; et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. EuroIntervention 2021, 16, 1049–1069. [Google Scholar] [CrossRef]
- Reynolds, H.R.; Shaw, L.J.; Min, J.K.; Spertus, J.A.; Chaitman, B.R.; Berman, D.S.; Picard, M.H.; Kwong, R.Y.; Bairey-Merz, C.N.; Cyr, D.D.; et al. Association of Sex with Severity of Coronary Artery Disease, Ischemia, and Symptom Burden in Patients with Moderate or Severe Ischemia: Secondary Analysis of the ISCHEMIA Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 773–786. [Google Scholar] [CrossRef]
- Bergami, M.; Scarpone, M.; Cenko, E.; Varotti, E.; Amaduzzi, P.L.; Manfrini, O. Gender Differences in Non-Obstructive Coronary Artery Disease. Curr. Pharm. Des. 2021, 27, 3198–3209. [Google Scholar] [CrossRef]
- Taqueti, V.R.; Di Carli, M.F. Coronary Microvascular Disease Pathogenic Mechanisms and Therapeutic Options: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 2625–2641. [Google Scholar] [CrossRef]
- Agewall, S.; Beltrame, J.F.; Reynolds, H.R.; Niessner, A.; Rosano, G.; Caforio, A.L.; De Caterina, R.; Zimarino, M.; Roffi, M.; Kjeldsen, K.; et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur. Heart J. 2017, 38, 143–153. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Mahajan, A.M.; Roe, M.T.; Hellkamp, A.S.; Chiswell, K.; Gulati, M.; Reynolds, H.R. Mortality of Myocardial Infarction by Sex, Age, and Obstructive Coronary Artery Disease Status in the ACTION Registry-GWTG (Acute Coronary Treatment and Intervention Outcomes Network Registry-Get with the Guidelines). Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003443. [Google Scholar] [CrossRef] [PubMed]
- Bainey, K.R.; Welsh, R.C.; Alemayehu, W.; Westerhout, C.M.; Traboulsi, D.; Anderson, T.; Brass, N.; Armstrong, P.W.; Kaul, P. Population-level incidence and outcomes of myocardial infarction with non-obstructive coronary arteries (MINOCA): Insights from the Alberta contemporary acute coronary syndrome patients invasive treatment strategies (COAPT) study. Int. J. Cardiol. 2018, 264, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Andersson, H.B.; Pedersen, F.; Engstrøm, T.; Helqvist, S.; Jensen, M.K.; Jørgensen, E.; Kelbæk, H.; Räder, S.; Saunamäki, K.; Bates, E.; et al. Long-term survival and causes of death in patients with ST-elevation acute coronary syndrome without obstructive coronary artery disease. Eur. Heart J. 2018, 39, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Eisenberg, E.; Di Palo, K.E.; Piña, I.L. Sex differences in heart failure. Clin. Cardiol. 2018, 41, 211–216. [Google Scholar] [CrossRef]
- Sotomi, Y.; Hikoso, S.; Nakatani, D.; Mizuno, H.; Okada, K.; Dohi, T.; Kitamura, T.; Sunaga, A.; Kida, H.; Oeun, B. Sex differences in heart failure with preserved ejection fraction. J. Am. Heart Assoc. 2021, 10, e018574. [Google Scholar] [CrossRef]
- Chandra, A.; Skali, H.; Claggett, B.; Solomon, S.D.; Rossi, J.S.; Russell, S.D.; Matsushita, K.; Kitzman, D.W.; Konety, S.H.; Mosley, T.H.; et al. Race- and Gender-Based Differences in Cardiac Structure and Function and Risk of Heart Failure. J. Am. Coll. Cardiol. 2022, 79, 355–368. [Google Scholar] [CrossRef]
- Hall, P.S.; Nah, G.; Howard, B.V.; Lewis, C.E.; Allison, M.A.; Sarto, G.E.; Waring, M.E.; Jacobson, L.T.; Manson, J.E.; Klein, L.; et al. Reproductive Factors and Incidence of Heart Failure Hospitalization in the Women’s Health Initiative. J. Am. Coll. Cardiol. 2017, 69, 2517–2526. [Google Scholar] [CrossRef]
- Lam, C.S.P.; Arnott, C.; Beale, A.L.; Chandramouli, C.; Hilfiker-Kleiner, D.; Kaye, D.M.; Ky, B.; Santema, B.T.; Sliwa, K.; Voors, A.A. Sex differences in heart failure. Eur. Heart J. 2019, 40, 3859–3868c. [Google Scholar] [CrossRef]
- Davis, M.B.; Arany, Z.; McNamara, D.M.; Goland, S.; Elkayam, U. Peripartum Cardiomyopathy: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 207–221. [Google Scholar] [CrossRef]
- Bauersachs, J.; König, T.; van der Meer, P.; Petrie, M.C.; Hilfiker-Kleiner, D.; Mbakwem, A.; Hamdan, R.; Jackson, A.M.; Forsyth, P.; de Boer, R.A.; et al. Pathophysiology, diagnosis and management of peripartum cardiomyopathy: A position statement from the Heart Failure Association of the European Society of Cardiology Study Group on peripartum cardiomyopathy. Eur. J. Heart Fail. 2019, 21, 827–843. [Google Scholar] [CrossRef] [PubMed]
- Frazier, C.G.; Alexander, K.P.; Newby, L.K.; Anderson, S.; Iverson, E.; Packer, M.; Cohn, J.; Goldstein, S.; Douglas, P.S. Associations of gender and etiology with outcomes in heart failure with systolic dysfunction: A pooled analysis of 5 randomized control trials. J. Am. Coll. Cardiol. 2007, 49, 1450–1458. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, J.; Cautela, J.; Ederhy, S.; Damaj, G.L.; Salem, J.E.; Barlesi, F.; Farnault, L.; Charbonnier, A.; Mirabel, M.; Champiat, S.; et al. Cardiovascular Toxicity Related to Cancer Treatment: A Pragmatic Approach to the American and European Cardio-Oncology Guidelines. J. Am. Heart Assoc. 2020, 9, e018403. [Google Scholar] [CrossRef] [PubMed]
- Savarese, G.; D’Amario, D. Sex Differences in Heart Failure. Adv. Exp. Med. Biol. 2018, 1065, 529–544. [Google Scholar] [CrossRef] [PubMed]
- Postigo, A.; Martínez-Sellés, M. Sex Influence on Heart Failure Prognosis. Front. Cardiovasc. Med. 2020, 7, 616273. [Google Scholar] [CrossRef]
- Ni, H.; Xu, J. Recent Trends in Heart Failure—Related Mortality: United States, 2000–2014; NCHS Data Brief No. 231; CDC: Atlanta, GA, USA, 2015; pp. 1–8. [Google Scholar]
- Chandra, A.; Vaduganathan, M.; Lewis, E.F.; Claggett, B.L.; Rizkala, A.R.; Wang, W.; Lefkowitz, M.P.; Shi, V.C.; Anand, I.S.; Ge, J. Health-related quality of life in heart failure with preserved ejection fraction: The PARAGON-HF trial. JACC Heart Fail. 2019, 7, 862–874. [Google Scholar]
- Garay, A.; Tapia, J.; Anguita, M.; Formiga, F.; Almenar, L.; Crespo-Leiro, M.G.; Manzano, L.; Muñiz, J.; Chaves, J.; De Frutos, T.; et al. Gender Differences in Health-Related Quality of Life in Patients with Systolic Heart Failure: Results of the VIDA Multicenter Study. J. Clin. Med. 2020, 9, 2825. [Google Scholar] [CrossRef]
- Klein, L.; Grau-Sepulveda, M.V.; Bonow, R.O.; Hernandez, A.F.; Williams, M.V.; Bhatt, D.L.; Fonarow, G.C. Quality of care and outcomes in women hospitalized for heart failure. Circ. Heart Fail. 2011, 4, 589–598. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Santema, B.T.; Ouwerkerk, W.; Tromp, J.; Sama, I.E.; Ravera, A.; Regitz-Zagrosek, V.; Hillege, H.; Samani, N.J.; Zannad, F.; Dickstein, K.; et al. Identifying optimal doses of heart failure medications in men compared with women: A prospective, observational, cohort study. Lancet 2019, 394, 1254–1263. [Google Scholar] [CrossRef]
- Bots, S.H.; Onland-Moret, N.C.; Tulevski, II; van der Harst, P.; Cramer, M.J.M.; Asselbergs, F.W.; Somsen, G.A.; den Ruijter, H.M. Heart failure medication dosage and survival in women and men seen at outpatient clinics. Heart 2021, 107, 1748–1755. [Google Scholar] [CrossRef] [PubMed]
- Santangeli, P.; Pelargonio, G.; Dello Russo, A.; Casella, M.; Bisceglia, C.; Bartoletti, S.; Santarelli, P.; Di Biase, L.; Natale, A. Gender differences in clinical outcome and primary prevention defibrillator benefit in patients with severe left ventricular dysfunction: A systematic review and meta-analysis. Heart Rhythm. 2010, 7, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Arshad, A.; Moss, A.J.; Foster, E.; Padeletti, L.; Barsheshet, A.; Goldenberg, I.; Greenberg, H.; Hall, W.J.; McNitt, S.; Zareba, W.; et al. Cardiac resynchronization therapy is more effective in women than in men: The MADIT-CRT (Multicenter Automatic Defibrillator Implantation Trial with Cardiac Resynchronization Therapy) trial. J. Am. Coll. Cardiol. 2011, 57, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Mackall, J.A.; Cakulev, I. What Is It About Women? The Antiarrhythmic Effect of Cardiac Resynchronization Therapy. Clin. Electrophysiol. 2021, 7, 716–718. [Google Scholar] [CrossRef] [PubMed]
- Tamargo, J.; Caballero, R.; Delpón, E. Sex-related differences in the pharmacological treatment of heart failure. Pharmacol. Ther. 2021, 107891. [Google Scholar] [CrossRef]
- Nitsche, C.; Koschutnik, M.; Kammerlander, A.; Hengstenberg, C.; Mascherbauer, J. Gender-specific differences in valvular heart disease. Wien. Klin. Wochenschr. 2020, 132, 61–68. [Google Scholar] [CrossRef]
- Avierinos, J.F.; Inamo, J.; Grigioni, F.; Gersh, B.; Shub, C.; Enriquez-Sarano, M. Sex differences in morphology and outcomes of mitral valve prolapse. Ann. Intern. Med. 2008, 149, 787–795. [Google Scholar] [CrossRef]
- Redberg, R.F.; Schiller, N.B. Gender and valvular surgery. J. Thorac. Cardiovasc. Surg. 2004, 127, 1–3. [Google Scholar] [CrossRef][Green Version]
- Movahed, M.R.; Ahmadi-Kashani, M.; Kasravi, B.; Saito, Y. Increased prevalence of mitral stenosis in women. J. Am. Soc. Echocardiogr. 2006, 19, 911–913. [Google Scholar] [CrossRef]
- Pasca, I.; Dang, P.; Tyagi, G.; Pai, R.G. Survival in Patients with Degenerative Mitral Stenosis: Results from a Large Retrospective Cohort Study. J. Am. Soc. Echocardiogr. 2016, 29, 461–469. [Google Scholar] [CrossRef]
- Kong, W.K.; Regeer, M.V.; Ng, A.C.; McCormack, L.; Poh, K.K.; Yeo, T.C.; Shanks, M.; Parent, S.; Enache, R.; Popescu, B.A.; et al. Sex Differences in Phenotypes of Bicuspid Aortic Valve and Aortopathy: Insights from a Large Multicenter, International Registry. Circ. Cardiovasc. Imaging 2017, 10. [Google Scholar] [CrossRef] [PubMed]
- Bassareo, P.P.; Crisafulli, A. Gender Differences in Hemodynamic Regulation and Cardiovascular Adaptations to Dynamic Exercise. Curr. Cardiol. Rev. 2020, 16, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Tornos, P.; Sambola, A.; Permanyer-Miralda, G.; Evangelista, A.; Gomez, Z.; Soler-Soler, J. Long-term outcome of surgically treated aortic regurgitation: Influence of guideline adherence toward early surgery. J. Am. Coll. Cardiol. 2006, 47, 1012–1017. [Google Scholar] [CrossRef]
- Chandrasekhar, J.; Dangas, G.; Yu, J.; Vemulapalli, S.; Suchindran, S.; Vora, A.N.; Baber, U.; Mehran, R. Sex-Based Differences in Outcomes with Transcatheter Aortic Valve Therapy: TVT Registry from 2011 to 2014. J. Am. Coll. Cardiol. 2016, 68, 2733–2744. [Google Scholar] [CrossRef] [PubMed]
- Ko, D.; Rahman, F.; Schnabel, R.B.; Yin, X.; Benjamin, E.J.; Christophersen, I.E. Atrial fibrillation in women: Epidemiology, pathophysiology, presentation, and prognosis. Nat. Rev. Cardiol. 2016, 13, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Piccini, J.P.; Simon, D.N.; Steinberg, B.A.; Thomas, L.; Allen, L.A.; Fonarow, G.C.; Gersh, B.; Hylek, E.; Kowey, P.R.; Reiffel, J.A.; et al. Differences in Clinical and Functional Outcomes of Atrial Fibrillation in Women and Men: Two-Year Results from the ORBIT-AF Registry. JAMA Cardiol. 2016, 1, 282–291. [Google Scholar] [CrossRef]
- Mukai, Y. Sex Differences in Atrial Fibrillation. Circ. J. 2022. [Google Scholar] [CrossRef]
- Senoo, K.; Lip, G.Y. Female Sex, Time in Therapeutic Range, and Clinical Outcomes in Atrial Fibrillation Patients Taking Warfarin. Stroke 2016, 47, 1665–1668. [Google Scholar] [CrossRef]
- Patel, N.; Deshmukh, A.; Thakkar, B.; Coffey, J.O.; Agnihotri, K.; Patel, A.; Ainani, N.; Nalluri, N.; Patel, N.; Patel, N.; et al. Gender, Race, and Health Insurance Status in Patients Undergoing Catheter Ablation for Atrial Fibrillation. Am. J. Cardiol. 2016, 117, 1117–1126. [Google Scholar] [CrossRef]
- Ganesan, A.N.; Shipp, N.J.; Brooks, A.G.; Kuklik, P.; Lau, D.H.; Lim, H.S.; Sullivan, T.; Roberts-Thomson, K.C.; Sanders, P. Long-term outcomes of catheter ablation of atrial fibrillation: A systematic review and meta-analysis. J. Am. Heart Assoc. 2013, 2, e004549. [Google Scholar] [CrossRef]
- Cheung, J.W.; Cheng, E.P.; Wu, X.; Yeo, I.; Christos, P.J.; Kamel, H.; Markowitz, S.M.; Liu, C.F.; Thomas, G.; Ip, J.E.; et al. Sex-based differences in outcomes, 30-day readmissions, and costs following catheter ablation of atrial fibrillation: The United States Nationwide Readmissions Database 2010–14. Eur. Heart J. 2019, 40, 3035–3043. [Google Scholar] [CrossRef] [PubMed]
- Kuck, K.H.; Brugada, J.; Fürnkranz, A.; Chun, K.R.J.; Metzner, A.; Ouyang, F.; Schlüter, M.; Elvan, A.; Braegelmann, K.M.; Kueffer, F.J.; et al. Impact of Female Sex on Clinical Outcomes in the FIRE AND ICE Trial of Catheter Ablation for Atrial Fibrillation. Circ. Arrhythm. Electrophysiol. 2018, 11, e006204. [Google Scholar] [CrossRef] [PubMed]
- Akoum, N.; Mahnkopf, C.; Kholmovski, E.G.; Brachmann, J.; Marrouche, N.F. Age and sex differences in atrial fibrosis among patients with atrial fibrillation. Europace 2018, 20, 1086–1092. [Google Scholar] [CrossRef] [PubMed]
- Koopman, C.; Vaartjes, I.; Heintjes, E.M.; Spiering, W.; van Dis, I.; Herings, R.M.; Bots, M.L. Persisting gender differences and attenuating age differences in cardiovascular drug use for prevention and treatment of coronary heart disease, 1998–2010. Eur. Heart J. 2013, 34, 3198–3205. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Shen, X.; DiMario, S.; Philip, K. Gender Disparities in Health Resource Utilization in Patients with Atherosclerotic Cardiovascular Disease: A Retrospective Cross-Sectional Study. Adv. Ther. 2019, 36, 3424–3434. [Google Scholar] [CrossRef]
- Santosa, A.; Zhang, Y.; Weinehall, L.; Zhao, G.; Wang, N.; Zhao, Q.; Wang, W.; Ng, N. Gender differences and determinants of prevalence, awareness, treatment and control of hypertension among adults in China and Sweden. BMC Public Health 2020, 20, 1763. [Google Scholar] [CrossRef]
- Humphries, K.H.; Izadnegahdar, M.; Sedlak, T.; Saw, J.; Johnston, N.; Schenck-Gustafsson, K.; Shah, R.; Regitz-Zagrosek, V.; Grewal, J.; Vaccarino, V.; et al. Sex differences in cardiovascular disease—Impact on care and outcomes. Front. Neuroendocrinol. 2017, 46, 46–70. [Google Scholar] [CrossRef]
- Ridker, P.M.; Cook, N.R.; Lee, I.-M.; Gordon, D.; Gaziano, J.M.; Manson, J.E.; Hennekens, C.H.; Buring, J.E. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N. Engl. J. Med. 2005, 352, 1293–1304. [Google Scholar] [CrossRef]
- Group, A.S.C. Effects of aspirin for primary prevention in persons with diabetes mellitus. N. Engl. J. Med. 2018, 379, 1529–1539. [Google Scholar]
- Gaziano, J.M.; Brotons, C.; Coppolecchia, R.; Cricelli, C.; Darius, H.; Gorelick, P.B.; Howard, G.; Pearson, T.A.; Rothwell, P.M.; Ruilope, L.M. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): A randomised, double-blind, placebo-controlled trial. Lancet 2018, 392, 1036–1046. [Google Scholar] [CrossRef]
- McNeil, J.J.; Wolfe, R.; Woods, R.L.; Tonkin, A.M.; Donnan, G.A.; Nelson, M.R.; Reid, C.M.; Lockery, J.E.; Kirpach, B.; Storey, E.; et al. Effect of Aspirin on Cardiovascular Events and Bleeding in the Healthy Elderly. N. Engl. J. Med. 2018, 379, 1509–1518. [Google Scholar] [CrossRef] [PubMed]
- McNeil, J.J.; Nelson, M.R.; Woods, R.L.; Lockery, J.E.; Wolfe, R.; Reid, C.M.; Kirpach, B.; Shah, R.C.; Ives, D.G.; Storey, E.; et al. Effect of Aspirin on All-Cause Mortality in the Healthy Elderly. N. Engl. J. Med. 2018, 379, 1519–1528. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.L.; Roddick, A.J. Association of Aspirin Use for Primary Prevention with Cardiovascular Events and Bleeding Events: A Systematic Review and Meta-analysis. JAMA 2019, 321, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Faller, J.; Majmudar, I.; Nguyen, P.; Moodie, M. Are interventions to improve cardiovascular disease risk factors in premenopausal women effective? A systematic review and meta-analysis. BMJ Open 2021, 11, e042103. [Google Scholar] [CrossRef]
- García, R.; Muñoz, M.A.; Navas, E.; Vinyoles, E.; Verdú-Rotellar, J.M.; Del Val, J.L. Variability in Cardiovascular Risk Factor Control in Patients with Heart Failure According to Gender and Socioeconomic Status. J. Women’s Health 2022. [Google Scholar] [CrossRef]
- Sciomer, S.; Moscucci, F.; Dessalvi, C.C.; Deidda, M.; Mercuro, G. Gender differences in cardiology: Is it time for new guidelines? J. Cardiovasc. Med. 2018, 19, 685–688. [Google Scholar] [CrossRef]
- Mosca, L.; Benjamin, E.J.; Berra, K.; Bezanson, J.L.; Dolor, R.J.; Lloyd-Jones, D.M.; Newby, L.K.; Piña, I.L.; Roger, V.L.; Shaw, L.J.; et al. Effectiveness-based guidelines for the prevention of cardiovascular disease in women—2011 update: A guideline from the american heart association. Circulation 2011, 123, 1243–1262. [Google Scholar] [CrossRef]
- Lundberg, G.P.; Dunbar, S.B.; Wenger, N.K. Guidelines for the Reduction of Cardiovascular Disease in Women. J. Obs. Gynecol. Neonatal. Nurs. 2016, 45, 402–412. [Google Scholar] [CrossRef]
- Tannenbaum, C.; Norris, C.M.; McMurtry, M.S. Sex-Specific Considerations in Guidelines Generation and Application. Can. J. Cardiol. 2019, 35, 598–605. [Google Scholar] [CrossRef]
- Schamroth Pravda, N.; Karny-Rahkovich, O.; Shiyovich, A.; Schamroth Pravda, M.; Rapeport, N.; Vaknin-Assa, H.; Eisen, A.; Kornowski, R.; Porter, A. Coronary Artery Disease in Women: A Comprehensive Appraisal. J. Clin. Med. 2021, 10, 4664. [Google Scholar] [CrossRef]
- Safdar, B. Influence of Sex and Gender on Lifestyle Interventions for Cardiovascular Disease. Clin. Ther. 2021. [Google Scholar] [CrossRef]
- Banks, E.; Welsh, J.; Joshy, G.; Martin, M.; Paige, E.; Korda, R.J. Comparison of cardiovascular disease risk factors, assessment and management in men and women, including consideration of absolute risk: A nationally representative cross-sectional study. BMJ Open 2020, 10, e038761. [Google Scholar] [CrossRef]
- Tran, H.V.; Waring, M.E.; McManus, D.D.; Erskine, N.; Do, V.T.H.; Kiefe, C.I.; Goldberg, R.J. Underuse of Effective Cardiac Medications Among Women, Middle-Aged Adults, and Racial/Ethnic Minorities with Coronary Artery Disease (from the National Health and Nutrition Examination Survey 2005 to 2014). Am. J. Cardiol. 2017, 120, 1223–1229. [Google Scholar] [CrossRef]
- Virani, S.S.; Woodard, L.D.; Ramsey, D.J.; Urech, T.H.; Akeroyd, J.M.; Shah, T.; Deswal, A.; Bozkurt, B.; Ballantyne, C.M.; Petersen, L.A. Gender disparities in evidence-based statin therapy in patients with cardiovascular disease. Am. J. Cardiol. 2015, 115, 21–26. [Google Scholar] [CrossRef]
- Ngo-Metzger, Q.; Zuvekas, S.; Shafer, P.; Tracer, H.; Borsky, A.E.; Bierman, A.S. Statin Use in the U.S. for Secondary Prevention of Cardiovascular Disease Remains Suboptimal. J. Am. Board Fam. Med. 2019, 32, 807–817. [Google Scholar] [CrossRef]
- Peters, S.A.; Colantonio, L.D.; Zhao, H.; Bittner, V.; Dai, Y.; Farkouh, M.E.; Monda, K.L.; Safford, M.M.; Muntner, P.; Woodward, M. Sex differences in high-intensity statin use following myocardial infarction in the United States. J. Am. Coll. Cardiol. 2018, 71, 1729–1737. [Google Scholar] [CrossRef]
- Lewey, J.; Shrank, W.H.; Bowry, A.D.; Kilabuk, E.; Brennan, T.A.; Choudhry, N.K. Gender and racial disparities in adherence to statin therapy: A meta-analysis. Am. Heart J. 2013, 165, 665–678.e1. [Google Scholar] [CrossRef]
- Chieffo, A.; Buchanan, G.L.; Mauri, F.; Mehilli, J.; Vaquerizo, B.; Moynagh, A.; Mehran, R.; Morice, M.C. ACS and STEMI treatment: Gender-related issues. EuroIntervention 2012, 8 (Suppl. P), P27–P35. [Google Scholar] [CrossRef]
- Eindhoven, D.C.; Hilt, A.D.; Zwaan, T.C.; Schalij, M.J.; Borleffs, C.J.W. Age and gender differences in medical adherence after myocardial infarction: Women do not receive optimal treatment—The Netherlands claims database. Eur. J. Prev. Cardiol. 2018, 25, 181–189. [Google Scholar] [CrossRef]
- Sabbag, A.; Matetzky, S.; Porter, A.; Iakobishvili, Z.; Moriel, M.; Zwas, D.; Fefer, P.; Asher, E.; Beigel, R.; Gottlieb, S.; et al. Sex Differences in the Management and 5-Year Outcome of Young Patients (<55 Years) with Acute Coronary Syndromes. Am. J. Med. 2017, 130, 1324.e1315–1324.e1322. [Google Scholar] [CrossRef]
- Alnsasra, H.; Zahger, D.; Geva, D.; Matetzky, S.; Beigel, R.; Iakobishvili, Z.; Alcalai, R.; Atar, S.; Shimony, A. Contemporary Determinants of Delayed Benchmark Timelines in Acute Myocardial Infarction in Men and Women. Am. J. Cardiol. 2017, 120, 1715–1719. [Google Scholar] [CrossRef] [PubMed]
- Ngiam, J.N.; Thong, E.H.; Loh, P.H.; Chan, K.H.; Chan, M.Y.; Lee, C.H.; Low, A.F.; Tan, H.C.; Loh, J.P.; Sim, H.W. An Asian Perspective on Gender Differences in In-Hospital and Long-Term Outcome of Cardiac Mortality and Ischemic Stroke after Primary Percutaneous Coronary Intervention for ST-Segment Elevation Myocardial Infarction. J. Stroke Cereb. Dis. 2022, 31, 106215. [Google Scholar] [CrossRef] [PubMed]
- Kerola, A.M.; Palomäki, A.; Rautava, P.; Nuotio, M.; Kytö, V. Sex Differences in Cardiovascular Outcomes of Older Adults After Myocardial Infarction. J. Am. Heart Assoc. 2021, 10, e022883. [Google Scholar] [CrossRef] [PubMed]
- Heydari, A.; Zahergivar, A.; Izadpanah, P.; Aquino, G.; Burt, J.R. Role of Gender on the Outcomes of ST-Elevation Myocardial Infarction Patients Following Primary Coronary Angioplasty. Cureus 2021, 13, e17892. [Google Scholar] [CrossRef]
- Ouellette, M.L.; Löffler, A.I.; Beller, G.A.; Workman, V.K.; Holland, E.; Bourque, J.M. Clinical characteristics, sex differences, and outcomes in patients with normal or near-normal coronary arteries, non-obstructive or obstructive coronary artery disease. J. Am. Heart Assoc. 2018, 7, e007965. [Google Scholar] [CrossRef]
- Stehli, J.; Dinh, D.; Dagan, M.; Duffy, S.J.; Brennan, A.; Smith, K.; Andrew, E.; Nehme, Z.; Reid, C.M.; Lefkovits, J.; et al. Sex Differences in Prehospital Delays in Patients with ST-Segment-Elevation Myocardial Infarction Undergoing Percutaneous Coronary Intervention. J. Am. Heart Assoc. 2021, 10, e019938. [Google Scholar] [CrossRef]
- Smith, L.R.; Salifu, M.O.; McFarlane, I.M. Non-Obstructive Coronary Artery Disease in Women: Current Evidence and Future Directions. Int. J. Clin. Res. Trials 2020, 5, 152. [Google Scholar] [CrossRef]
- Lanéelle, D.; Sauvet, G.; Guillaumat, J.; Trihan, J.E.; Mahé, G. Gender Differences in the Medical Treatment of Peripheral Artery Disease. J. Clin. Med. 2021, 10, 2855. [Google Scholar] [CrossRef]
- Eccleston, D.; Cehic, D.; Young, G.; Lin, T.; Pavia, S.; Chowdhury, E.K.; Reid, C.; Liew, D.; King, B.; Tan, I.; et al. Sex differences in Cardiac electronic device implantation: Outcomes from an Australian multi-centre clinical quality registry. Int. J. Cardiol. Heart Vasc. 2021, 35, 100828. [Google Scholar] [CrossRef]
- Samayoa, L.; Grace, S.L.; Gravely, S.; Scott, L.B.; Marzolini, S.; Colella, T.J. Sex differences in cardiac rehabilitation enrollment: A meta-analysis. Can. J. Cardiol. 2014, 30, 793–800. [Google Scholar] [CrossRef]
- Oosenbrug, E.; Marinho, R.P.; Zhang, J.; Marzolini, S.; Colella, T.J.; Pakosh, M.; Grace, S.L. Sex Differences in Cardiac Rehabilitation Adherence: A Meta-analysis. Can. J. Cardiol. 2016, 32, 1316–1324. [Google Scholar] [CrossRef] [PubMed]
- Mamataz, T.; Ghisi, G.L.M.; Pakosh, M.; Grace, S.L. Nature, availability, and utilization of women-focused cardiac rehabilitation: A systematic review. BMC Cardiovasc. Disord. 2021, 21, 459. [Google Scholar] [CrossRef] [PubMed]
- Chaker, Z.; Badhwar, V.; Alqahtani, F.; Aljohani, S.; Zack, C.J.; Holmes, D.R.; Rihal, C.S.; Alkhouli, M. Sex Differences in the Utilization and Outcomes of Surgical Aortic Valve Replacement for Severe Aortic Stenosis. J. Am. Heart Assoc. 2017, 6, e006370. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, F.; Olufade, T.O.; Ramey, D.R.; Friedman, H.S.; Navaratnam, P.; Heithoff, K.; Foody, J.M. Gender Disparities in Lipid-Lowering Therapy in Cardiovascular Disease: Insights from a Managed Care Population. J. Women’s Health 2016, 25, 697–706. [Google Scholar] [CrossRef]
- Tamargo, J.; Rosano, G.; Walther, T.; Duarte, J.; Niessner, A.; Kaski, J.C.; Ceconi, C.; Drexel, H.; Kjeldsen, K.; Savarese, G.; et al. Gender differences in the effects of cardiovascular drugs. Eur. Heart J. Cardiovasc. Pharm. 2017, 3, 163–182. [Google Scholar] [CrossRef]
- Levinsson, A.; Dubé, M.P.; Tardif, J.C.; de Denus, S. Sex, drugs, and heart failure: A sex-sensitive review of the evidence base behind current heart failure clinical guidelines. ESC Heart Fail. 2018, 5, 745–754. [Google Scholar] [CrossRef]
- Patti, G.; De Caterina, R.; Abbate, R.; Andreotti, F.; Biasucci, L.M.; Calabrò, P.; Cioni, G.; Davì, G.; Di Sciascio, G.; Golia, E.; et al. Platelet function and long-term antiplatelet therapy in women: Is there a gender-specificity? A ‘state-of-the-art’ paper. Eur. Heart J. 2014, 35, 2213–2223b. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.-P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Eur. J. Cardio-Thorac. Surg. 2018, 53, 34–78. [Google Scholar] [CrossRef]
- Saw, J.; Aymong, E.; Sedlak, T.; Buller, C.E.; Starovoytov, A.; Ricci, D.; Robinson, S.; Vuurmans, T.; Gao, M.; Humphries, K.; et al. Spontaneous coronary artery dissection: Association with predisposing arteriopathies and precipitating stressors and cardiovascular outcomes. Circ. Cardiovasc. Interv. 2014, 7, 645–655. [Google Scholar] [CrossRef]
- van der Meer, M.G.; Cramer, M.J.; van der Graaf, Y.; Doevendans, P.A.; Nathoe, H.M. Gender difference in long-term prognosis among patients with cardiovascular disease. Eur. J. Prev. Cardiol. 2014, 21, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Yin, F.; Fan, C.; Wang, Z. Gender difference in clinical outcomes of the patients with coronary artery disease after percutaneous coronary intervention: A systematic review and meta-analysis. Medicine 2018, 97, e11644. [Google Scholar] [CrossRef] [PubMed]
- Mateo-Rodríguez, I.; Danet, A.; Bolívar-Muñoz, J.; Rosell-Ortriz, F.; Garcia-Mochón, L.; Daponte-Codina, A. Gender differences, inequalities and biases in the management of Acute Coronary Syndrome. J. Healthc. Qual. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Sattar, Y.; Song, D.; Kompella, R.; Arshad, J.; Zghouzi, M.; Mir, T.; Ullah, W.; Elgendy, I.Y.; Alraies, M.C. Meta-Analysis Comparing Gender-Based Cardiovascular Outcomes of Transradial Versus Transfemoral Access of Percutaneous Coronary Intervention. Am. J. Cardiol. 2022, 162, 49–57. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Contest | Effects |
|---|---|
| ACS in Women | STEMI: ↑30-day mortality ↑ Bleeding [244] |
| After PCI: ↑Peri-procedural AMI ↑Major Bleeding ↑In-Hospital Mortality ↑2-years Mortality [208,244] | |
| Gp IIb/IIIa inhibitors: ↑Adverse effects ↓ Outcomes [208] | |
| Stable CAD in Women | After elective PCI: Similar contemporary outcomes in both sex [208] |
| Atrial Fibrillation and Stroke | NOACs: ↑Effectiveness ↓ Bleeding Risk |
| Warfarin in the correct TTR: No differences in CV mortality all-cause mortality and stroke risk between the sexes | |
| In stroke: Thrombolysis, antiplatelet and anticoagulant therapies ↑ beneficial | |
| Heart Failure | With comparable treatment: ↑Clinical Outcomes [208,246]. |
| BBs: ↑ Slightly survival benefit in elderly [208,246]. | |
| Digitalis: ↑Mortality [208,246] | |
| Spironolactone Eplerenone: Similar efficacy [208,246]. | |
| Valsartan/Sacubitril: Equal beneficial effect [246] | |
| After CV procedures: ↑Morbidity ↑Mortality ↓ Health-related quality of life ↓ Functional improvement [58] | |
| Surgical, Interventional, and Electrophysiology Treatments | TAVI: Beneficial in terms of short-, mid-, and long-term outcomes [243] |
| ICD in women: ↑Device-related complications ↑Death ↑All-Cause readmissions ↑HF readmissions | |
| CRT: ↓ Mortality ↑Reverse remodeling of LV [183] | |
| Cardiac Rehabilitation | ↑ Outcomes [255] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucà, F.; Abrignani, M.G.; Parrini, I.; Di Fusco, S.A.; Giubilato, S.; Rao, C.M.; Piccioni, L.; Cipolletta, L.; Passaretti, B.; Giallauria, F.; et al. Update on Management of Cardiovascular Diseases in Women. J. Clin. Med. 2022, 11, 1176. https://doi.org/10.3390/jcm11051176
Lucà F, Abrignani MG, Parrini I, Di Fusco SA, Giubilato S, Rao CM, Piccioni L, Cipolletta L, Passaretti B, Giallauria F, et al. Update on Management of Cardiovascular Diseases in Women. Journal of Clinical Medicine. 2022; 11(5):1176. https://doi.org/10.3390/jcm11051176
Chicago/Turabian StyleLucà, Fabiana, Maurizio Giuseppe Abrignani, Iris Parrini, Stefania Angela Di Fusco, Simona Giubilato, Carmelo Massimiliano Rao, Laura Piccioni, Laura Cipolletta, Bruno Passaretti, Francesco Giallauria, and et al. 2022. "Update on Management of Cardiovascular Diseases in Women" Journal of Clinical Medicine 11, no. 5: 1176. https://doi.org/10.3390/jcm11051176
APA StyleLucà, F., Abrignani, M. G., Parrini, I., Di Fusco, S. A., Giubilato, S., Rao, C. M., Piccioni, L., Cipolletta, L., Passaretti, B., Giallauria, F., Leone, A., Francese, G. M., Riccio, C., Gelsomino, S., Colivicchi, F., & Gulizia, M. M. (2022). Update on Management of Cardiovascular Diseases in Women. Journal of Clinical Medicine, 11(5), 1176. https://doi.org/10.3390/jcm11051176