
Mitral Paravalvular Leak: Clinical Implications, Diagnosis and Management

 ,
,  ,
,
Abstract
:1. Introduction
2. Clinical Manifestations
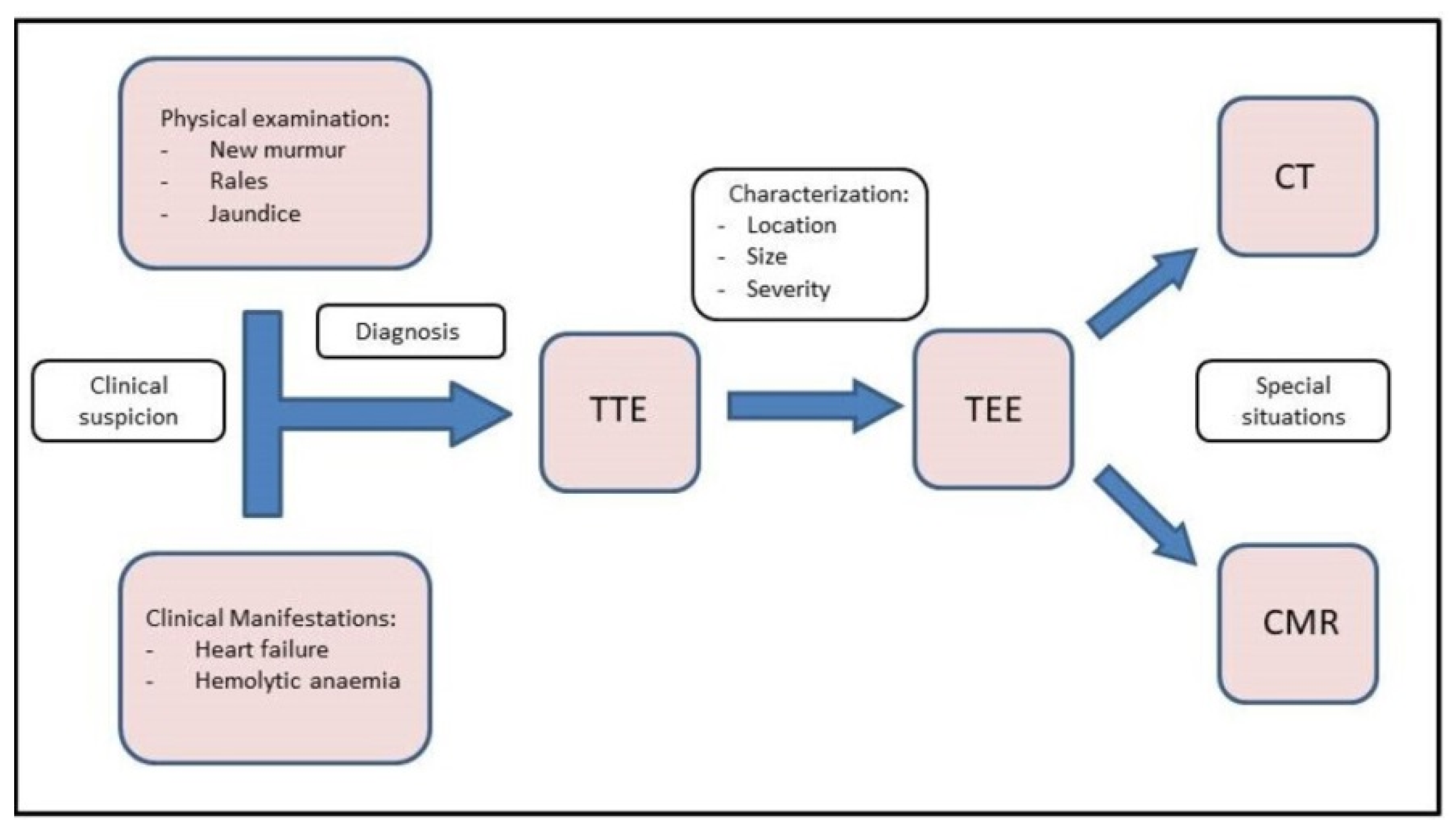
3. Diagnosis
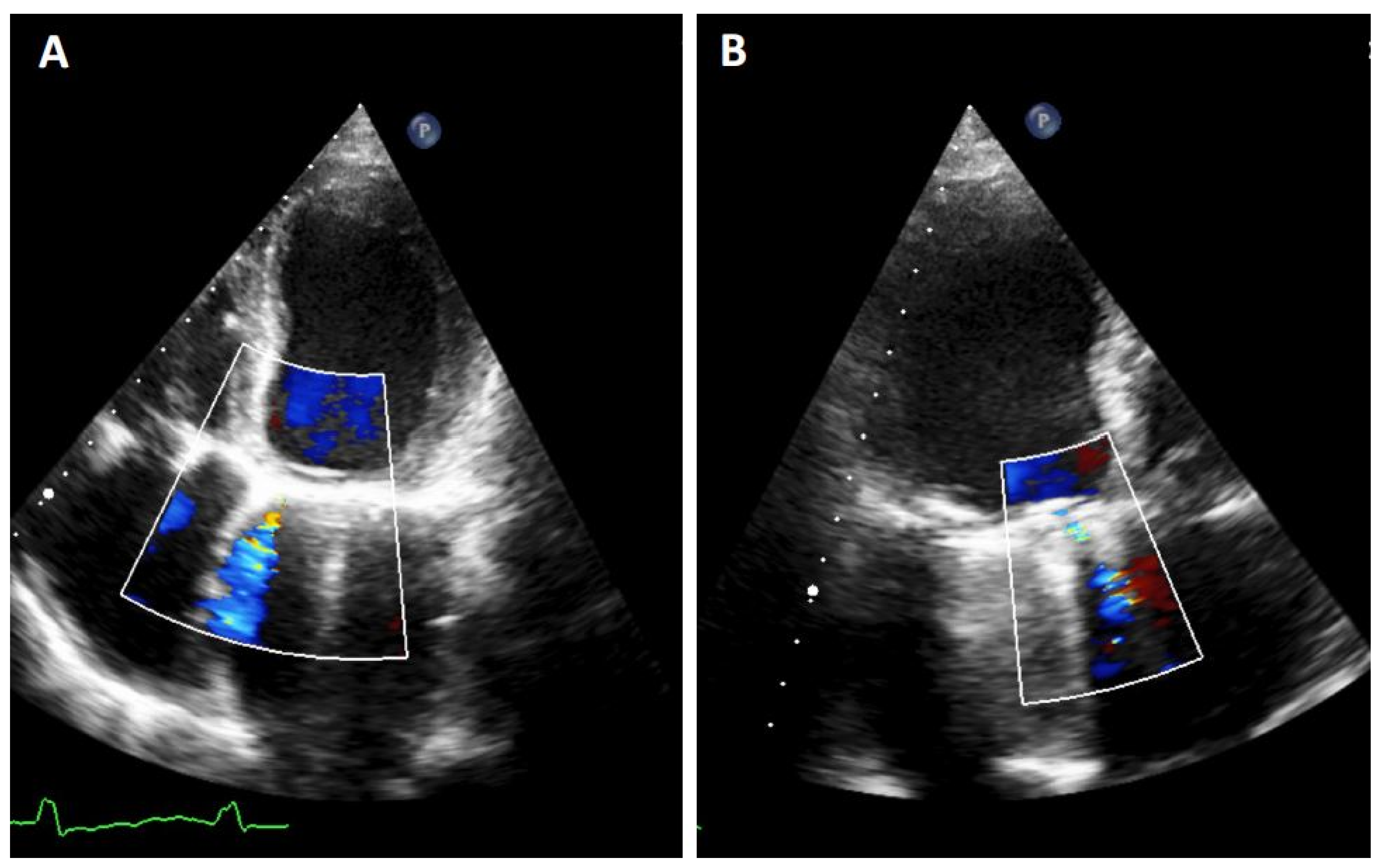
3.1. TTE
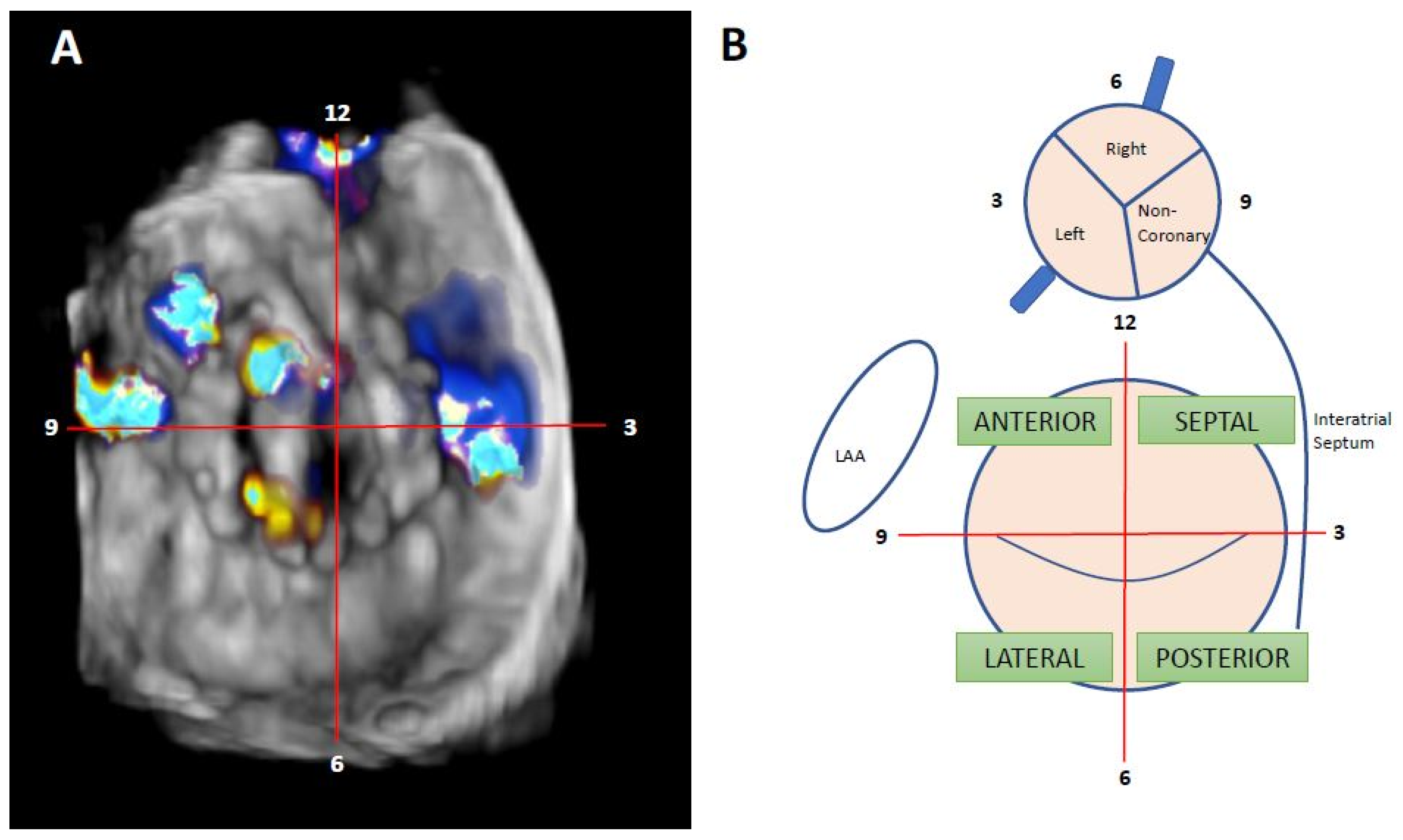
3.2. TEE
3.3. CMR
3.4. Cardiac CT
4. Management
4.1. Treatment
4.2. Devices
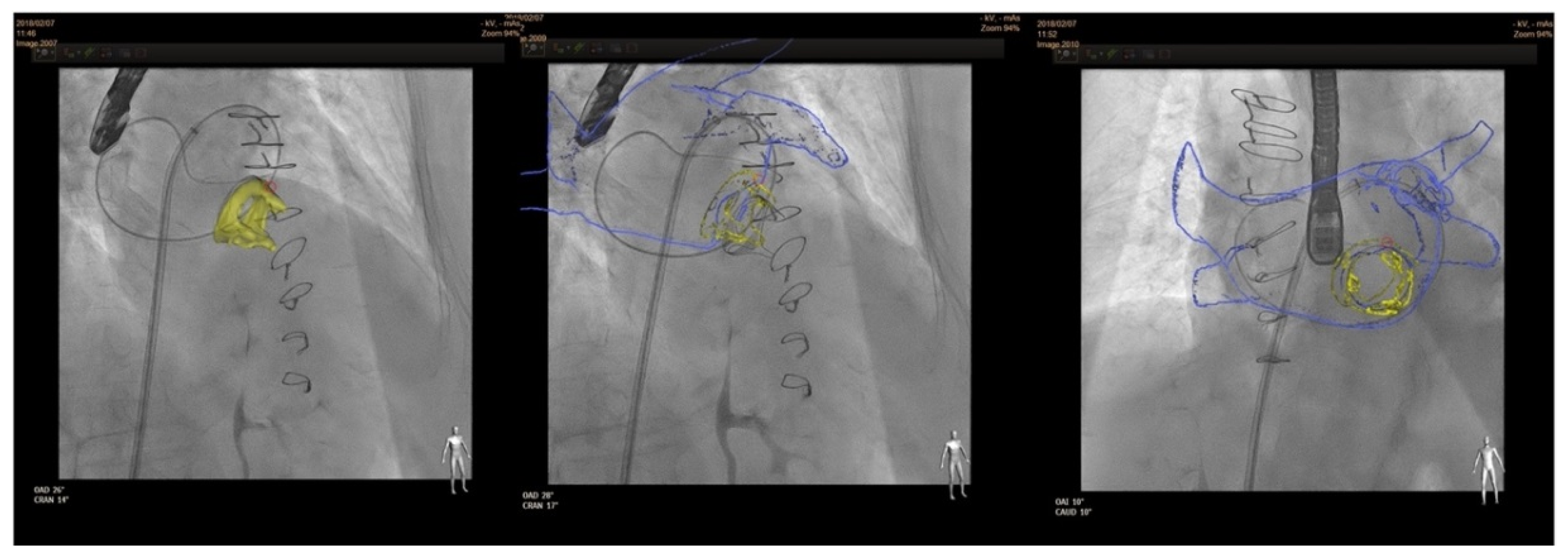
4.3. Procedure
4.3.1. Anterograde Approach
4.3.2. Retrograde Approach
4.3.3. Transapical Approach
4.4. Final Result Assesment
4.5. Post-Procedural Medical Therapy and Follow-Up
5. Outcomes
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Desai, A.; John, C. Messenger, Robert Quaife, John Carroll. Update in Paravalvular Leak Closure. Curr. Cardiol. Rep. 2021, 23, 122. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Gonzalez, I.; Rama-Merchan, J.C.; Rodríguez-Collado, J.; Martín-Moreiras, J.; Diego-Nieto, A.; Barreiro-Pérez, M.; Sánchez, P.L. Transcatheter closure of paravalvular leaks: State of the art. Neth. Heart J. 2017, 25, 116–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernard, S.; Yucel, E. Paravalvular Leaks-From Diagnosis to Management. Curr Treat. Options Cardiovasc. Med. 2019, 21, 67. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, 172. [Google Scholar]
- Writing Committee Members; Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, I.I.I.J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease. Circulation 2021, 143, e72–e227. [Google Scholar]
- Lopez-Pais, J.; Lopez-Otero, D.; Garcia-Touchard, A.; Coronel, B.I.; Muiños, P.J.A.; Mendioroz, X.C.; Pérez-Poza, M.; Garcia, Ó.O.; Peredo, C.G.M.; Flores, C.A.; et al. Impact of significant paravalvular leaks after transcatheter aortic valve implantation on anaemia and mortality. Heart 2020, 107, 497–502. [Google Scholar] [CrossRef]
- Bertrand, P.B.; Levine, R.A.; Isselbacher, E.M.; Vandervoort, P.M. Fact or artifact in two-dimensional echocardiography: Avoiding misdiagnosis and missed diagnosis. J. Am. Soc. Echocardiogr. 2016, 29, 381–391. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Gonzalez, I.; Rama-Merchan, J.C.; Calvert, P.A.; Rodríguez-Collado, J.; Barreiro-Pérez, M.; Martín-Moreiras, J.; Diego-Nieto, A.; Hildick-Smith, D.; Sánchez, P.L. Percutaneous Closure of Paravalvular Leaks: A Systematic Review. J. Interv. Cardiol. 2016, 29, 382–392. [Google Scholar] [CrossRef]
- Kronzon, I.; Sugeng, L.; Perk, G.; Hirsh, D.; Weinert, L.; Garcia Fernandez, M.A.; Lang, R.M. Real-time 3-dimensional transesophageal echocardiography in the evaluation of post-operative mitral annuloplasty ring and prosthetic valve dehiscence. J. Am. Coll. Cardiol. 2009, 53, 1543–1547. [Google Scholar] [CrossRef] [Green Version]
- García-Fernández, M.A.; Cortés, M.; García-Robles, J.A.; de Diego, J.J.; Perez-David, E.; García, E. Utility of real-time three-dimensional transesophageal echocar- diography in evaluating the success of percutaneous transcatheter closure of mitral paravalvular leaks. J. Am. Soc. Echocardiogr. 2010, 23, 26–32. [Google Scholar] [CrossRef]
- Arribas-Jimenez, A.; Rama-Merchan, J.C.; Barreiro-Pérez, M.; Merchan-Gómez, S.; Iscar-Galán, A.; Martín-García, A.; Nieto-Ballestero, F.; Sánchez-Corral, E.; Rodriguez-Collado, J.; Cruz-González, I.; et al. Utility of Real-Time 3-Dimensional Transesophageal Echocardiography in the Assessment of Mitral Paravalvular Leak. Circ. J. 2016, 80, 738–744. [Google Scholar] [CrossRef] [Green Version]
- Lampropoulos, K.; Aggeli, C.; Megalou, A.; Barbetseas, J.; Budts, W. Diagnosis and Treatment of Left-Sided Prosthetic Paravalvular Regurgitation. Cardiology 2016, 133, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Lazaro, C.; Hinojar, R.; Zamorano, J.L. Cardiac imaging in prosthetic paravalvular leaks. Cardiovasc. Diagn. Ther. 2014, 4, 307–313. [Google Scholar] [PubMed]
- Faletra, F.F.; Pedrazzini, G.; Pasotti, E.; Muzzarelli, S.; Dequarti, M.C.; Murzilli, R.; Schlossbauer, S.A.; Slater, I.P.; Moccetti, T. 3D TEE during catheter-based interventions. JACC Cardiovasc. Imaging 2014, 7, 292–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barreiro-Perez, M.; Cruz-González, I.; Gil-Ortega, M.V.; Rasco, A.G.; Sánchez, P.L. Photo-Realistic Echocardiography Imaging During Percutaneous Paravalvular Leak Closure. JACC Cardiovasc. Interv. 2020, 13, e185–e187. [Google Scholar] [CrossRef]
- Karagodin, I.; Shah, A.P.; Lang, R.M. Guided by the Light-Transillumination of a Paravalvular Leak. JAMA Cardiol. 2020, 5, e203260. [Google Scholar] [CrossRef]
- Kumar, R.; Jelnin, V.; Kliger, C.; Ruiz, C.E. Percutaneous paravalvular leak closure. Cardiol. Clin. 2013, 31, 431–440. [Google Scholar] [CrossRef]
- Kliger, C.; Eiros, R.; Isasti, G.; Einhorn, B.; Jelnin, V.; Cohen, H.; Kronzon, I.; Perk, G.; Fontana, G.P.; Ruiz, C.E. Review of surgical prosthetic paravalvular leaks: Diagnosis and catheter-based closure. Eur. Heart J. 2013, 34, 638–649. [Google Scholar] [CrossRef] [Green Version]
- Ruparelia, N.; Cao, J.; Newton, J.D.; Wilson, N.; Daniels, M.J.; Ormerod, O.J. Paravalvular leak closure under intracardiac echocardiographic guidance. Catheter. Cardiovasc. Interv. 2018, 91, 958–965. [Google Scholar] [CrossRef]
- Suchá, D.; Symersky, P.; Tanis, W.; Mali, W.P.; Leiner, T.; van Herwerden, L.A.; Budde, R.P. Multimodality Imaging Assessment of Prosthetic Heart Valves. Circ. Cardiovasc. Imaging 2015, 8, e003703. [Google Scholar] [CrossRef] [Green Version]
- Orwat, S.; Diller, G.P.; Kaleschke, G.; Kerckhoff, G.; Kempny, A.; Radke, R.M.; Buerke, B.; Burg, M.; Schülke, C.; Baumgartner, H. Aortic regurgitation severity after transcatheter aortic valve implantation is underestimated by echocardiography compared with MRI. Heart 2014, 100, 1933–1938. [Google Scholar] [CrossRef] [PubMed]
- Suh, Y.J.; Hong, G.R.; Han, K.; Im, D.J.; Chang, S.; Hong, Y.J.; Lee, H.J.; Hur, J.; Choi, B.W.; Chang, B.C.; et al. Assessment of mitral paravalvular leakage after mitral valve replacement using cardiac computed tomography: Comparison with surgical findings. Circ. Cardiovasc. Imaging 2016, 9, e004153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnaswamy, A.; Tuzcu, E.M.; Kapadia, S.R. Three-dimensional computed tomography in the cardiac catheterization laboratory. Catheter. Cardiovasc. Interv. 2011, 77, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Cruz-González, I.; Barreiro-Pérez, M.; Valverde, I. 3D-printing in Preprocedural Planning of Paravalvular Leak Closure: Feasibility/Proof-of-concept. Rev. Esp. Cardiol. Engl. Ed. 2019, 72, 342. [Google Scholar] [CrossRef] [PubMed]
- Onorato, E.M.; Muratori, M.; Smolka, G.; Zakarkaite, D.; Mussayev, A.; Christos, C.P.; Bauer, F.; Gandet, T.; Luca, G.; Martinelli, M.D.; et al. Midterm procedural and clinical outcomes of percutaneous paravalvular leak closure with the Occlutech Paravalvular Leak Device. EuroIntervention 2020, 15, e1251–e1259. [Google Scholar] [CrossRef]
- Sorajja, P. Mitral Paravalvular Leak Closure. Interv. Cardiol. Clin. 2016, 5, 45–54. [Google Scholar] [CrossRef]
- Ruiz, C.E.; Jelnin, V.; Kronzon, I.; Dudiy, Y.; Del Valle-Fernandez, R.; Einhorn, B.N.; Chiam, P.T.; Martinez, C.; Eiros, R.; Roubin, G.; et al. Clinical outcomes in patients undergoing percutaneous closure of periprosthetic paravalvular leaks. J. Am. Coll. Cardiol. 2011, 58, 2210–2217. [Google Scholar] [CrossRef] [Green Version]
- García, E.; Arzamendi, D.; Jimenez-Quevedo, P.; Sarnago, F.; Martí, G.; Sanchez-Recalde, A.; Lasa-Larraya, G.; Sancho, M.; Iñiguez, A.; Goicolea, J.; et al. Outcomes and predictors of success and complicationsfor paravalvular leak closure: An analysis of the SpanisH real-wOrld paravalvular LEaks closure (HOLE)registry. EuroIntervention 2017, 12, 1962–1968. [Google Scholar] [CrossRef]
- Calvert, P.A.; Northridge, D.B.; Malik, I.S.; Shapiro, L.; Ludman, P.; Qureshi, S.A.; Mullen, M.; Henderson, R.; Turner, M.; Been, M.; et al. Percutaneous Device Closure of Paravalvular Leak. Combined Experience From the United Kingdom and Ireland. Circulation 2016, 134, 934–944. [Google Scholar] [CrossRef]
- Millán, X.; Skaf, S.; Joseph, L.; Ruiz, C.; García, E.; Smolka, G.; Noble, S.; Cruz-González, I.; Arzamendi, D.; Serra, A.; et al. Transcatheter Reduction of Paravalvular Leaks: A Systematic Review and Metaanalysis. Can. J. Cardiol. 2015, 31, 260–269. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MILD | MODERATE | SEVERE | |
|---|---|---|---|
| Colour Flow Area | <4 cm2, <20% LA area | Variable | >8 cm2, >40% LA area |
| Jet Density | Incomplete | Dense | Dense |
| Jet Contour | Parabolic | Variable | Early peaking, triangular, holosystolic |
| Pulmonary Venous Flow | Normal | Systolic blunting | Systolic flow reversal |
| PASP | Normal | Variable | Incremented |
| Vena contracta | <3 mm | 3–6.9 mm | >7 mm |
| Circumferential extent of PVL | <10% | 10–29% | >30% |
| Regurgitant Volume | <30 mL | 30–59 mL | >60 mL |
| Regurgitant Fraction * | <30% | 30–49% | >50% |
| EROA | <20 mm2 | 20–39 mm2 | >40 mm2 |
| Study | Country and Period | Type of Study | N Percutaneous vs. Surgical Closure | Endpoint | Results |
|---|---|---|---|---|---|
| Tamarasso et al., 2014 | Italy 2000–2013 | Single-centre, retrospective analysis | 17 vs. 122 | In-hospital death | Risk of death increased with surgical treatment (OR 8.0, 95% CI 1.8–13; p = 0.05) |
| Angulo-Llanos et al., 2016 | Spain 2008–2014 | Single-centre, retrospective, propensity-score matched analysis | 51 vs. 36 | Composite of death or readmission. (mean follow-up 784 days) | - Non-significant difference in composite end point. - Reduced in-hospital mortality with percutaneous approach. |
| Pinheiro et al., 2016 | Brazil 2011–2013 | Single-centre, retrospective analysis | 10 vs. 25 | Reintervention or death at 1 year | Non-significant difference between groups for either end point |
| Milan et al., 2017 | Canada 1994–2014 | Single-centre, retrospective, propensity-score matched analysis | 80 vs. 151 | Composite of all-cause death and hospitalization for heart failure. Median follow-up 3.5 years | Reduced risk of end point with surgical treatment (HR 0.28; 95% CI 0.18–0.44; p < 0.001) |
| Alkhouli et al., 2017 | USA 1995–2015 | Single-centre, retrospective analysis | 195 vs. 186 | Technical success and long-term survival (mean follow-up 4 years) | - Technical success greater in the surgical group - Non-significant difference in long-term survival between groups. |
| Wells et al., 2017 | USA 2007–2016 | Single-centre, retrospective analysis | 56 vs. 58 | Composite of death, reintervention or heart failure admission at 1 year | No difference in primary end point or 1-year survival between groups |
| Zhang et al., 2017 | China 2009–2015 | Single-centre, retrospective analysis | 46 vs. 41 | Survival Mean follow-up 49 months | - Non-significant difference in survival - Fewer in-hospital major adverse events and more cost-effective with percutaneous treatment |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cruz-Gonzalez, I.; Antunez-Muiños, P.; Lopez-Tejero, S.; Sanchez, P.L. Mitral Paravalvular Leak: Clinical Implications, Diagnosis and Management. J. Clin. Med. 2022, 11, 1245. https://doi.org/10.3390/jcm11051245
Cruz-Gonzalez I, Antunez-Muiños P, Lopez-Tejero S, Sanchez PL. Mitral Paravalvular Leak: Clinical Implications, Diagnosis and Management. Journal of Clinical Medicine. 2022; 11(5):1245. https://doi.org/10.3390/jcm11051245
Chicago/Turabian StyleCruz-Gonzalez, Ignacio, Pablo Antunez-Muiños, Sergio Lopez-Tejero, and Pedro L. Sanchez. 2022. "Mitral Paravalvular Leak: Clinical Implications, Diagnosis and Management" Journal of Clinical Medicine 11, no. 5: 1245. https://doi.org/10.3390/jcm11051245
APA StyleCruz-Gonzalez, I., Antunez-Muiños, P., Lopez-Tejero, S., & Sanchez, P. L. (2022). Mitral Paravalvular Leak: Clinical Implications, Diagnosis and Management. Journal of Clinical Medicine, 11(5), 1245. https://doi.org/10.3390/jcm11051245