Abstract
Background: This systematic review and metanalysis was conducted to assess differences between perioperative and functional outcomes in patients undergoing minimally-invasive partial (mi-PA) and total adrenalectomy (mi-TA) for unilateral primary aldosteronism (uPHA). Material and Methods: Multiple scientific databases (PUBMED, Web of Science, and Cochrane Library) were searched up to November 2021 for surgical series comparing mi-PA vs. mi-TA for uPHA according to the PRISMA statement. Primary outcomes of interest were perioperative and functional outcomes. Results: Overall, a total of 802 patients from six eligible studies were identified, with mi-PA and mi-TA performed in 40.4% (n = 324) and 59.6% (n = 478) of cases, respectively. No differences were recorded between the two groups according to number of transfusions, EBL and Clavien–Dindo complications ≥2. Similarly, no differences in clinical success, persistence of postoperative hypokalemia and improvement in HTN were reported between mi-PA and mi-TA. Conclusions: In a uPHA setting, mi-PA and mi-TA provide comparable perioperative and functional outcomes despite the use of mi-PA remains limited to patients with small adenoma size, or hereditary/bilateral disease. Due to limited use of standardized reporting criteria in most of current series, the quest for a superiority of mi-PA over mi-TA in the treatment of uPHA still remains open.
1. Introduction
Hypertension (HTN) represents a major cardiovascular risk factor [1]. Although many patients may suffer of essential HTN (eHTN), up to 15% are affected by undetected primary hyperaldosteronism (PHA), which represents the most common form of secondary HTN [2]. In recent years, the introduction of plasma aldosterone-to-plasma renin activity ratio (ARR), as a screening test in selected patients with HTN, has led to a 5–15-fold increase in the diagnosis of PHA, resulting in an estimated prevalence of 4% in the general population [3,4,5]. To parity of blood pressure elevation, patients affected by PHA have higher morbidity and mortality than patients with eHTN [6].
Clinical subtypes of PHA include unilateral, aldosterone producing adenoma (uPHA), unilateral adrenal hyperplasia (uAH), and bilateral adrenal hyperplasia (bAH) [7]. According to urological guidelines, minimally-invasive total adrenalectomy (mi-TA) represents the gold standard treatment for unilateral subtypes of PHA. Conversely, mineral corticoid receptor antagonists (MRAs) are recommended for medical treatment of bAH [8,9]. Nowadays, several authors have reported feasibility of adrenal-sparing techniques for uPHA with satisfactory outcomes for partial adrenalectomy (PA) vs. standard total adrenalectomy (TA) [10,11].
PA was originally described for the treatment of hereditary and sporadic bilateral tumors in order to reduce the risk of Addisonian crisis and to obviate the need for steroid replacement [12]. Nonetheless, promising results from the first randomized trial comparing PA versus TA [13] plus the wider adoption of minimally-invasive techniques have supported an increasing trend toward PA in the last two decades [14,15]. Although the feasibility of an adrenal-sparing approach has been reported by previous series, indications to PA remain limited [16,17]. In this context, the current literature has been recently subjected to meta-analysis, but not exclusively in the setting of minimally-invasive surgery [18,19,20].
To overcome these limitations, we sought to perform a systematic review and metanalysis of all available data from mi-PA and mi-TA series to evaluate differences in perioperative and functional outcomes between these surgical approaches for the management of uPHA.
2. Material and Methods
A systematic search was conducted to find relevant studies from PubMed, Web of Science, Cochrane Central Register of Controlled Trials—CENTRAL (in the Cochrane Library, Issue 1, 2011), and Clinicaltrials.gov (accessed on 20 December 2021) according to the PRISMA statement [21]. The research was restricted to English language studies, published between January 2005 and November 2021. We used the Population, Intervention, Comparator, and Outcome (PICO) approach to define study eligibility [22,23], as following:
- Population: patients affected by uPHA with indication to surgical treatment;
- Intervention: minimally-invasive partial adrenalectomy (mi-PA);
- Comparator: minimally-invasive total adrenalectomy (mi-TA);
- Outcomes: perioperative and functional results.
2.1. Search Strategy
The searching strategy was designed using both free text and mesh terms. We used the following keywords: partial adrenalectomy, adrenal-sparing surgery, (Adrenal Cortex Neoplasms [MeSH Terms] AND partial adrenalectomy), (Adrenocortical Adenoma [MeSH Terms] AND partial adrenalectomy), (Hyperaldosteronism [Mesh Terms] AND partial adrenalectomy), (Laparoscopy [Mesh Terms] AND partial adrenalectomy), (Minimally Invasive Surgical Procedures [Mesh Terms] AND partial adrenalectomy), and (Robotic Surgical Procedures [Mesh Terms] AND partial adrenalectomy).
2.2. Selection of Eligible Studies and Data Extraction
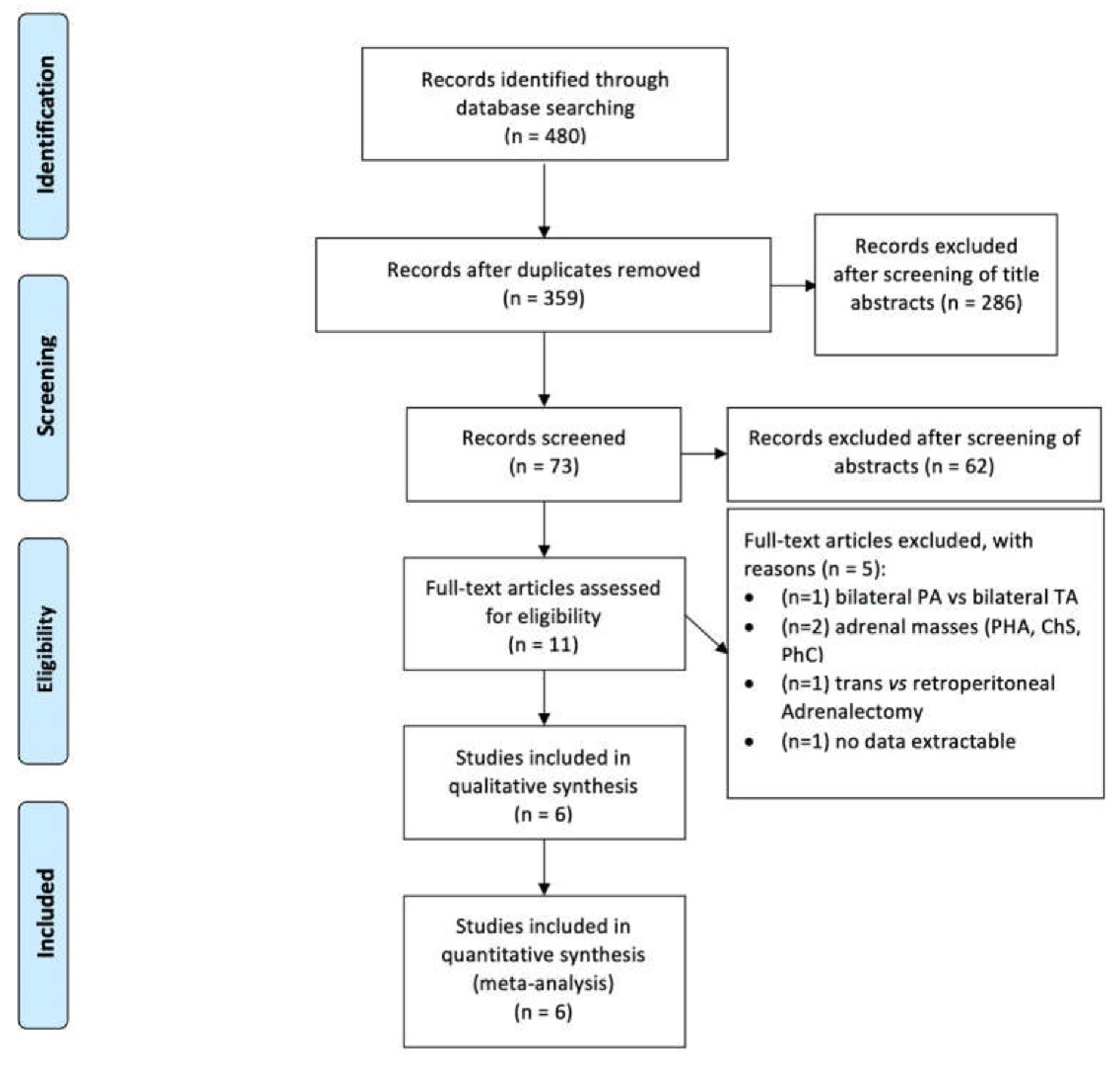
References of selected papers were retrieved for preliminary inclusion. The full-text screening and data extraction were subsequently performed by two independent reviewers (A.T. and R.S.F.). Discrepancy was resolved by internal discussion or by supervision of an independent arbiter (U.A.). Article selection was performed according to the PRISMA flow-chart (Figure 1). Studies comparing mi-TA with mi-PA were identified (n = 6).
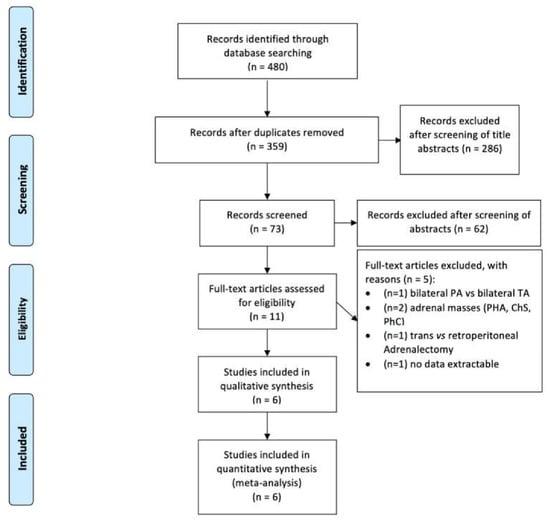
Figure 1.
PRISMA flow chart.
2.3. Data Quality Assessment
Quality of the included studies was assessed by the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool [24] and Risk-of-Bias tool for randomized trials (RoB 2) [25] as suggested by Cochrane handbook (Supplementary Figure S1).
Moreover, all studies were classified according to the grade of evidence for therapy/prevention/etiology/harm studies by Phillips and Sackett [26] with the following order: meta-analyses of randomized clinical trials (RCTs) representing the highest evidence (level 1a), adequately sampled single RCT (level 1b), systematic review of cohort studies (level 2a), and low-quality RCT or observational studies (level 2b), surgical series (level 4), and expert opinion (level 5).
The following variables were extracted from each study:
- -
- Baseline characteristics: age, BMI, gender, ASA score, HTN duration, number of antihypertensive medications, preoperative systolic blood pressure (SBP), diastolic blood pressure (DBP), serum Aldosterone (sA), serum Renin Activity (sRA), serum Aldosterone Renin Activity Ratio (ARR), and serum Potassium (sP);
- -
- Perioperative outcomes: surgical approach (retro/transperitoneal), minimally-invasive technique (laparoscopic/robot-assisted), tumor size, operating time (OR), estimated blood loss (EBL), length of hospital stay (LOS), intraoperative transfusions rate, postoperative complications, and histopathological diagnosis;
- -
- Functional outcomes: clinical and biochemical success according to standardized PASO criteria [27] (complete, partial, absent), postoperative SBP, DBP, postoperative hypokalemia, sA, sRA, sP, and recurrence rate.
2.4. Data Analysis
Cumulative meta-analysis of comparative studies was performed as follows. For continuous variables, a Mantel–Haenszel Chi-square test was used and expressed as the mean difference (MD) with 95% confidence interval (CI). For dichotomous variables, an inverse variance was used and expressed as odds ratio (OR) with 95% CI. In both cases p-value < 0.05 was considered significant. Both MD and OR were calculated comparing PA (experimental group) versus TA (control group). In case of positive outcomes, such as complete, partial clinical success, and improved hypertension; an OR > 1 indicated an advantage in the experimental arm (mi-PA). Heterogeneity was analyzed using a Chi-square test on n-of−1 degree of freedom, with a p-value < 0.05 used for statistical significance and with the I2 test for assessment of heterogeneity [28]. I2 values of 25%, 50%, and 90% corresponded to low, medium, and high levels of heterogeneity, respectively. Random effects and fixed effects were used in case of presence or absence of heterogeneity, respectively. RevMan (Review Manager) 5.4 was used for statistical analysis. Due to intrinsic limitations of this software, analysis of continuous variables was possible only when data were presented as mean and standard deviation (SD). Since some studies reported continuous variables in “median” and “interquartile range” or “min/max” range, we used a validated mathematical method (McGrath) to estimate “mean” and “SD” [29].
3. Results
3.1. Study Selection
The original search strategy retrieved 480 studies, published between January 2005 and November 2021, from which 469 were excluded based on titles and abstracts review. After evaluation of full manuscripts (11), only six studies comparing mi-PA to mi-TA were considered (Table 1).

Table 1.
Summary of published research: eligible studies testing perioperative and functional outcomes of mi-PA versus mi-TA.
Considering excluded studies, Liao et al. compared only bilateral PA versus bilateral TA [30], while Chen et al. focused on differences between retroperitoneal and transperitoneal approach [31]. Furthermore, two studies compared mi-PA and mi-TA in adrenal masses associated to different etiologies (Conn’s syndrome, Cushing’s syndrome, and Pheochromocytoma) [32,33]. Finally, Waltz et al. reported their experience on minimally-invasive adrenalectomy for PHA, without providing a comparison between PA vs. TA [14]. Conversely, among eligible studies, we identified only one randomized controlled trial (level of evidence 1b) [34]; one prospective non-randomized study (level of evidence: 2b) [35]; and four retrospective studies (level of evidence: 3b [10,11,36] or 4 [37]), respectively.
Overall, 802 patients were enrolled in these studies, with mi-PA and mi-TA performed in 324 (40.4%) and 478 (59.6%) patients, respectively. Among cohorts, 778 (97%) patients were treated by laparoscopic adrenalectomy while 24 (3%) with a robotic-assisted technique. Demographic and surgical characteristics of patients were analyzed including age, gender, BMI, ASA, tumor size, side, surgical approach, HTN duration, preoperative anti-HTN drugs, SBP, DBP, sP, sA, and sRA (Table 2).
Table 2.
Summary of published research: Baseline characteristics among eligible studies testing perioperative and functional outcomes of PA vs. TA.
We did not find any significant difference between the two cohorts except for BMI (MD: 0.92; 95% CI: 0.24, 1.61; kg/mt2; p = 0.008), DBP (MD: −4.87; 95% CI: −7.96, −1.79; mmHg; p = 0.002;), and HTN duration (MD: 0.30; 95% CI: 0.58–0.01; years; p = 0.04) (Supplementary Figure S2).
3.2. Perioperative Outcomes
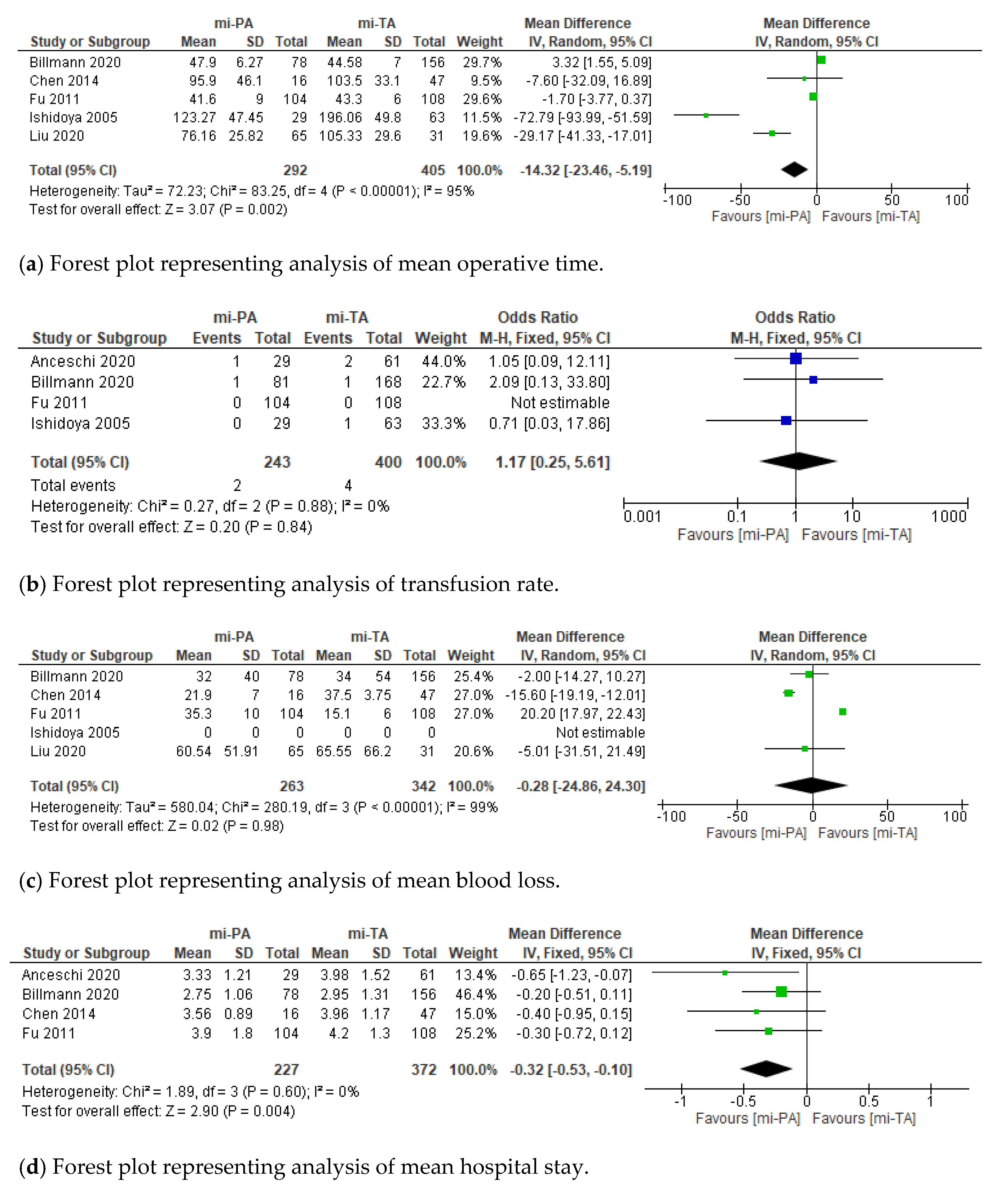
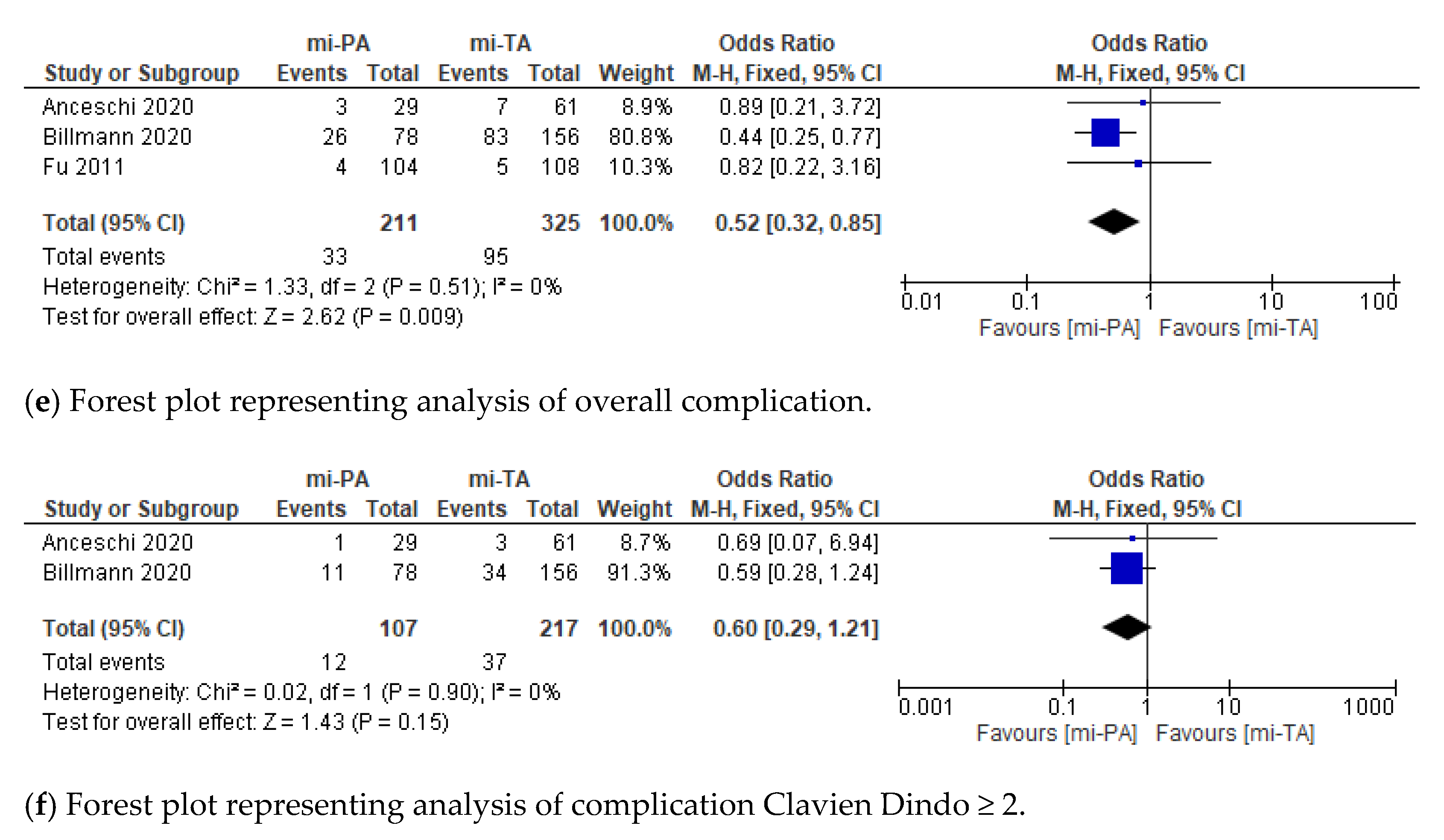
With regard to perioperative outcomes, we recorded a significant statistical difference between mi-PA and mi-TA according to mean operative time (MD: 14.32; 95% CI: −23.46, 5.19; minutes; p = 0.002), hospital stay (MD: −0.32; 95% CI: −0.53, −0.10; days; p = 0.004), and overall complication rate (OR: 0.52; 95% CI: 0.32, 0.85; p = 0.009), respectively. Conversely, no difference was found between groups in terms of number of transfusions, EBL, and Clavien–Dindo complications ≥ 2 (Figure 2). At final pathological report, no diagnosis of malignant tumor and different rate of solitary adenoma vs. hyperplasia was observed between groups (90% vs. 10% in mi-PA and 81% vs. 19% in mi-TA; OR 1.55; 95% CI: 1.01, 2.38; p = 0.04).
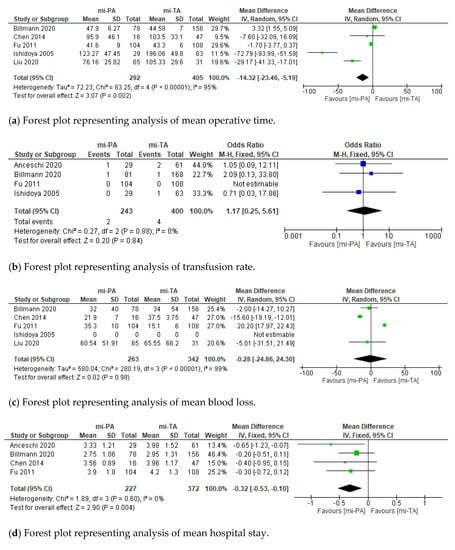
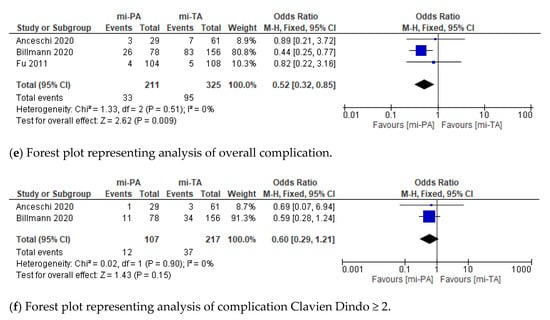
Figure 2.
Cumulative analysis of eligible studies comparing mi-PA vs. mi-TA in terms of (a) operative time, (b) transfusion rate, (c) blood loss, (d) hospital stay, (e) overall complication, and (f) Clavien–Dindo ≥ 2. IV = inverse variance; SD = standard deviation; CI = confidence interval; M–H = Mantel–Haenszel. Each studies is represented by a square incorporating confidence intervals represented by horizontal lines. The area of each square is proportional to the study’s weight in the meta-analysis. The meta-analysed measure of effect is plotted as a diamond with lateral points indicating confidence intervals.
3.3. Functional Outcomes
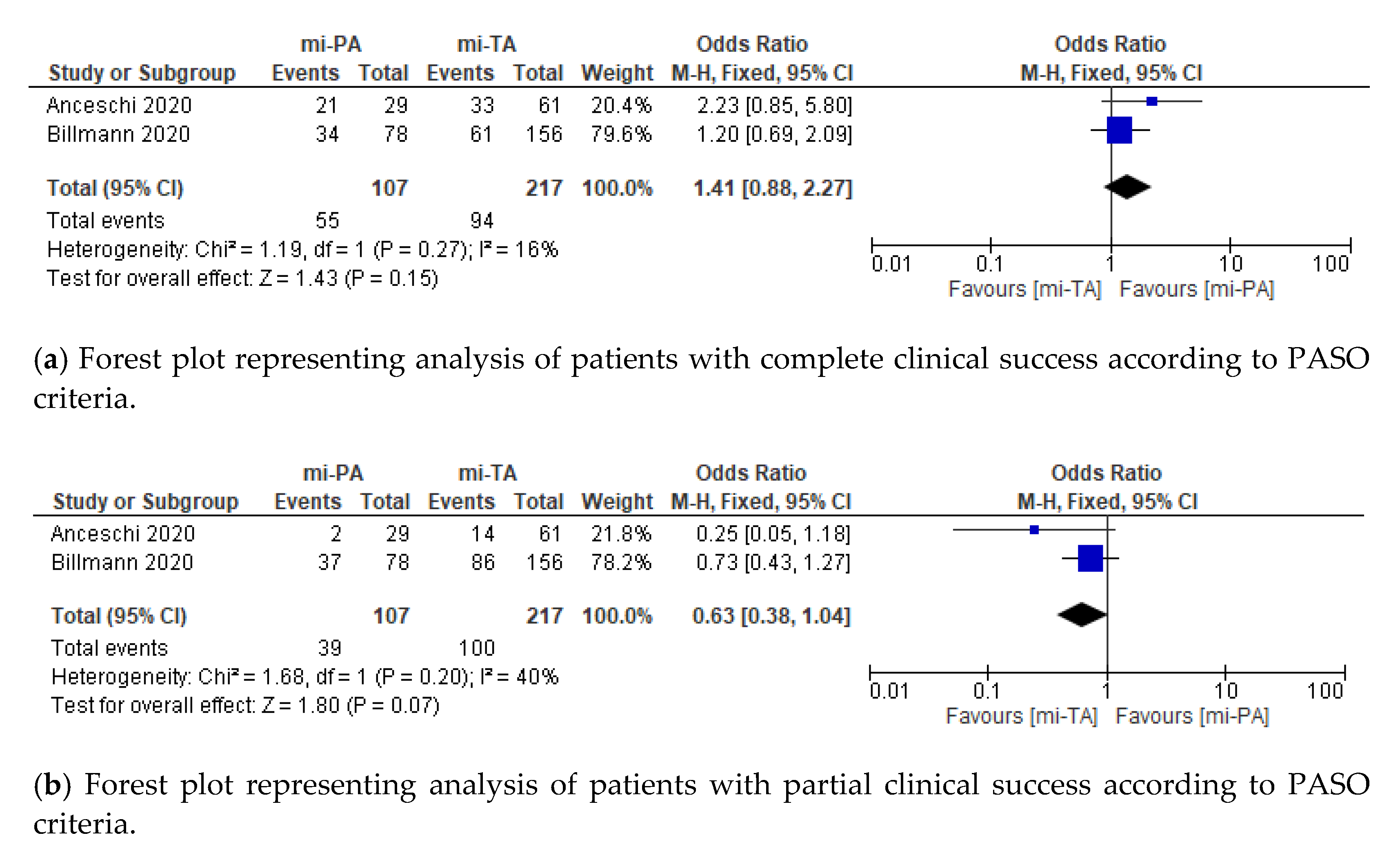
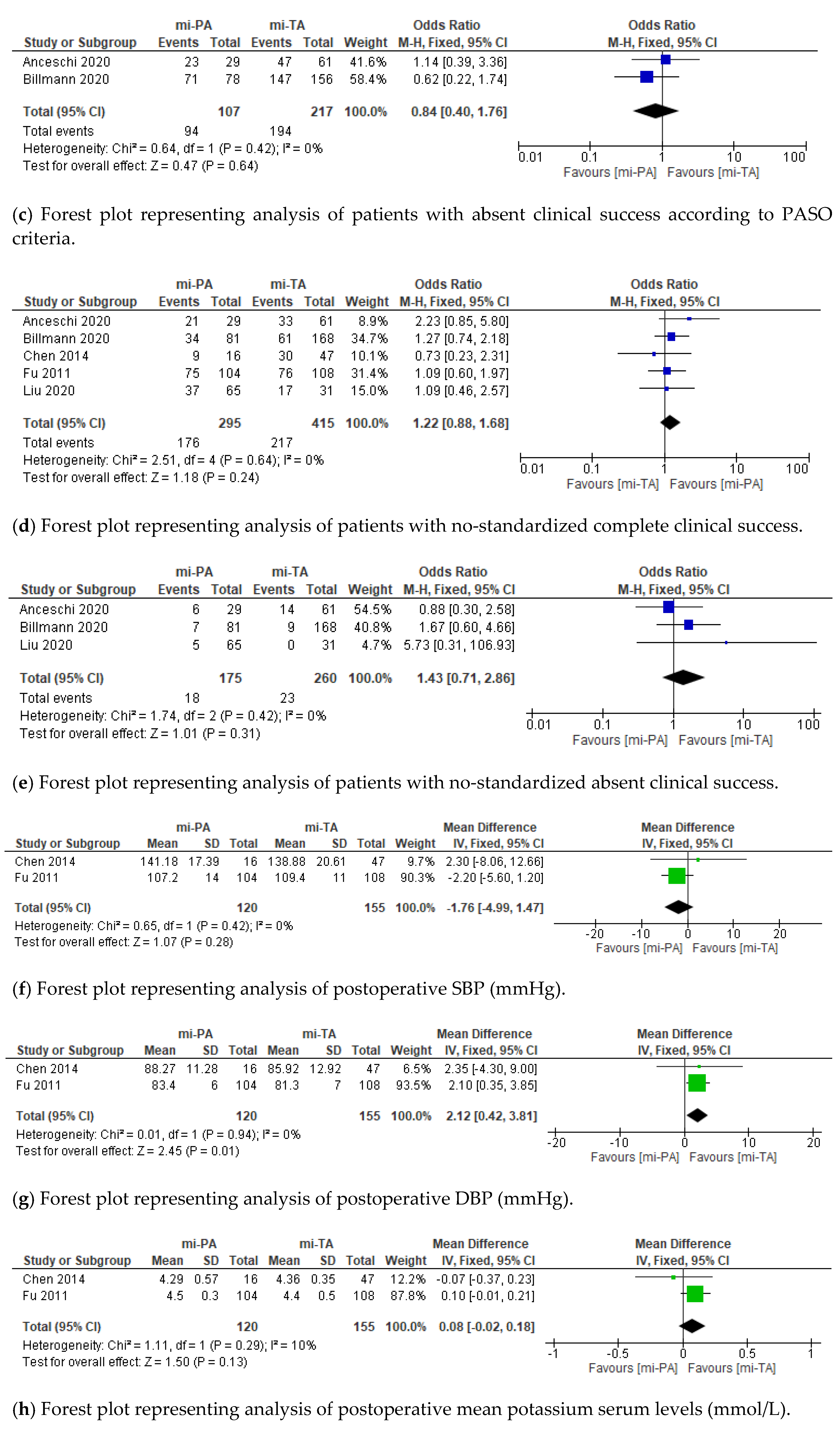
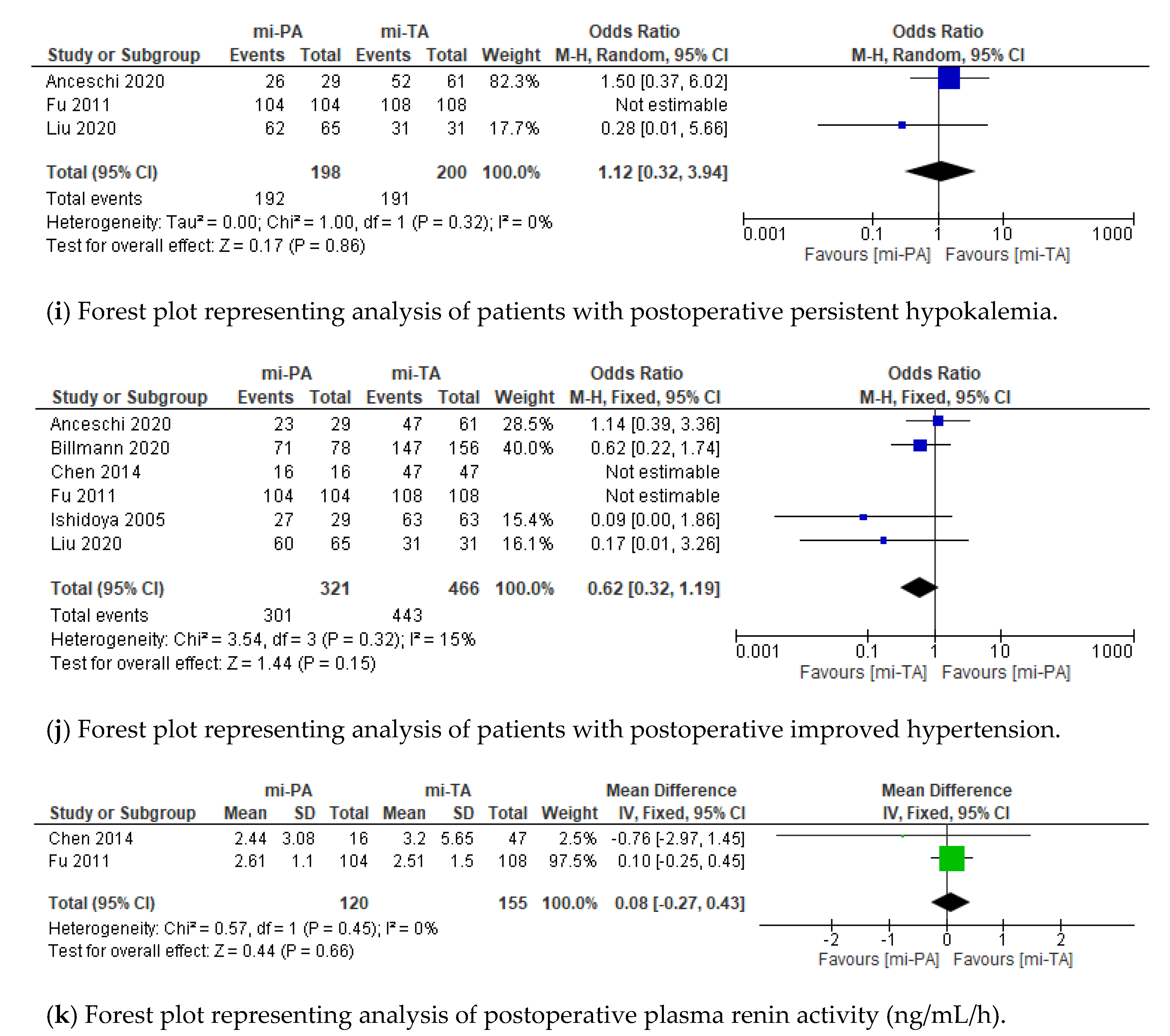
According to PASO criteria, complete, partial, and absent clinical success analyzed over 324 patients from two series showed no differences [10,36]. Moreover, similar results were found when considering no-standardized complete and absent clinical success over five studies for a total of 720 patients included [10,11,34,35,36]. No differences in persistence of postoperative hypokalemia and improvement in HTN were reported between mi-PA and mi-TA. Only two recurrences, confirmed by radiological and clinical investigation, respectively, were reported in the whole cohort (Figure 3).
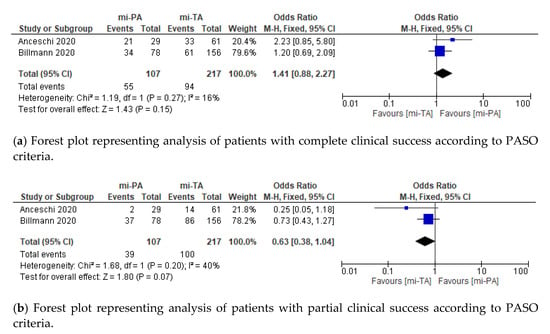
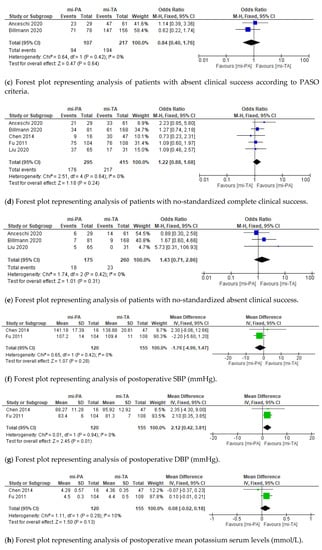
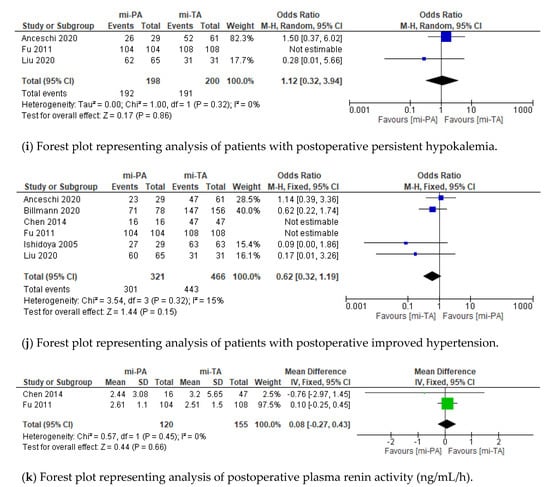
Figure 3.
Cumulative analysis of eligible studies comparing mi-PA vs. mi-TA in terms of (a) complete clinical success according to PASO criteria, (b) partial clinical success according to PASO criteria, (c) absent clinical success according to PASO criteria, (d) no-standardized complete clinical success, (e) no-standardized absent clinical success, (f) postoperative SBP, (g) postoperative DBP, (h) postoperative mean potassium serum levels, (i) postoperative persistent hypokalemia, (j) postoperative improved hypertension, and (k) postoperative plasma renin activity. IV = inverse variance; SD = standard deviation; CI = confidence interval; M-H = Mantel-Haenszel. Each studies is represented by a square incorporating confidence intervals represented by horizontal lines. The area of each square is proportional to the study’s weight in the meta-analysis. The meta-analysed measure of effect is plotted as a diamond with lateral points indicating confidence intervals.
4. Discussion
Nowadays, mi-TA represents the gold standard for uPHA over medical treatment [7]. Nonetheless, over the last decade, mi-PA has been increasingly adopted as an alternative surgical option for Conn’s syndrome, providing comparable outcomes with lesser incidence of cortisol replacement to mi-TA on the long run [19]. Despite this theoretical benefit, mi-PA remains currently underused due to lack of clear guidelines recommendation and granularity of available data [10]. Recently, Li et al. reported results of a pooled meta-analysis comparing PA vs. TA without providing a subgroup analysis accounting for different surgical techniques [20]. In this context, considering the growing interest towards robot-assisted adrenalectomy and the well-established role for laparoscopic adrenalectomy over years, we restricted our analysis to minimally-invasive adrenalectomy. Herein, we attempted to provide a more representative summary of current uPHA management among surgeons and urologists.
Our study showed interesting findings. Compared to mi-TA, among eligible studies, mi-PA showed a significant trend over reduced mean operative time, despite being within a large retrospective cohort; Walz et al. reported no significant differences in terms of this variable when considering all adrenal benign masses amenable of surgical treatment [14]. Additionally, in our study, mi-PA patients showed both lower mean hospital stay (MD: −0.32 days; p = 0.004) and lower rate of overall postoperative complication relative to mi-TA (15.6 vs. 29.2%; p = 0.009). Interestingly, when adopting a more comprehensive definition of perioperative complication (CD ≥ 2), we found no differences between mi-PA vs. mi-TA (11.2 vs. 17.1%; p = 0.15).
A major advantage of mi-PA over mi-TA may be represented by the decreased incidence of postoperative hypocortisolism. An increased rate of postoperative subclinical transient hypocortisolism after mi-TA was reported by Billman et al. (25.0% vs. 11.5% after mi-TA and mi-PA, respectively; p < 0.001) [36]. However, none of these patients needed permanent steroid replacement at median follow up of 24 months. This trend was also reported in prior series [11,34,35]. Conversely, a higher steroid replacement rate was reported by Anceschi et al., when compared mi-TA vs. mi-PA [10]. To date, available data suggest a negligible incidence of long-term steroid replacement after unilateral adrenalectomy for uPHA, irrespectively of the surgical approach (3–4.5%) [36].
Clinical success rate reported after surgery for uPHA remains controversial among series, ranging from 16% to 72% [38,39,40,41,42]. This wide variation highlights lack of consensus for defining clear success of adrenalectomy for PHA, irrespective of the surgical approach used [42]. In 2017, a collaborative international consortium (PASO) introduced a structured presentation of functional outcomes for adrenalectomy, establishing a comprehensive definition of complete, partial or absent clinical and biochemical success [27]. Several studies validated the greater accuracy of these new criteria in properly classifying postoperative functional results [41,42,43]. Nonetheless, Vorselaars et al. claimed that the use of high thresholds for definition of clinically relevant change in SBP, as well as the use of percentage, instead of absolute values, for evaluating daily-defined dose of medical treatment, represent the main drawbacks of these criteria [41]. To the best of our knowledge, only two published studies reported the comparison of clinical success between mi-PA and mi-TA according to PASO criteria [10,36]. We recorded comparable rate of complete, partial and absent clinical success between mi-PA and mi-TA according to PASO criteria (each p > 0.05). Interestingly, high rates of hypertension recovery (93.8% vs. 95.1%) with relevant postoperative SBP decrease (M.D. −39.44 vs. −43.39 mmHg, respectively) were recorded in mi-PA and mi-TA series, respectively. Since a relatively small decrease of SBP (≥10 mmHg) in HTN patients reduces by 13% the risk of all-cause mortality, these results support a theoretical benefit of both mi-TA and mi-PA in maintenance of SBP control, even if a complete clinical success may not be expectable [44,45].
Although the rate of absent clinical success was reported in two studies, data regarding its underlying etiology remain uncertain. For example, only three studies in the current SR investigated recurrence rate [11,34,36]. Overall, only two cases of recurrence in the mi-PA group were recorded. These findings reflect the low rate of recurrence after PA for Conn’s syndrome, as described in a recent meta-analysis (event rate 2%; 95% CI 1–5%) [18]. Moreover, Simforoosh et al. reported no cases of recurrence in seven patients treated by mi-PA for Conn’s syndrome at an extended follow-up (8 years) [33]. Furthermore, absence of malignant tumor at final pathological examination in all cases supports the use of mi-PA as a safe strategy for the treatment of patients with uPHA. Notably, a substantial number of uPHA patients treated with mi-PA vs. mi-TA harbored hyperplasia instead of APA (10% vs. 19%, respectively). Previous studies demonstrated that the presence of micronodules in the residual tissue after PA would expose patients to PHA recurrence [46,47]. Consequently, clinicians should carefully outweigh the benefit of adrenal sparing-surgery in this specific scenario.
Finally, in the current study a small amount of adrenalectomy was performed by robotic approach (3%). However, an increasing body of literature has addressed its potential benefit in terms of perioperative outcomes [16,48]. The advantages of robotic vs. laparoscopy technique [49], including its ancillary technology, such as near-infrared fluorescence imaging, may allow surgeons to better identify and excise adrenal masses, thus promoting the use of adrenal-sparing surgery [17,50,51,52].
This study is not devoid of limitations. Heterogeneity among eligible studies in preoperative evaluation and outcomes assessment represent intrinsic biases. For instance, preoperative adrenal vein sampling (AVS) was not routinely performed in all patients. Consequently, patients experiencing no complete clinical success might have a concomitant, functionally active, micro-nodule in the contralateral gland [53]. Finally, retrospective design, as well a limited follow-up, still precludes definitive conclusion on the non-inferiority of mi-PA vs. mi-TA for all evaluated endpoints. Notwithstanding these limitations, current literature support mi-PA as a safe surgical treatment for uPHA with mid-term functional outcomes comparable to mi-TA.
5. Conclusions
Adrenal-sparing techniques may provide patients affected by PHA with increased reserve of functional parenchyma. However, current findings may not be generalizable out of tertiary referral centers. Further evidence supported by either prospective series or multicentric RCTs are still required to determine those patients that might benefit mostly from either mi-PA or mi-TA for uPHA.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/jcm11051263/s1: Figure S1, Assessment of risk of bias according to ROBINS-I tool (a) and RoB 2 tool (b) as suggested by Cochrane handbook; Figure S2, Cumulative analysis of eligible studies comparing mi-PA vs. mi-TA in terms of (a) gender, (b) tumor side, (c) tumor size, (d) ASA 1-2, (e) ASA 3-4, (f) BMI, (g) surgical approach, (h) preoperative SPB, (i) preoperative DBP, (j) preoperative hypertension duration in years, (k) preoperative serum aldosterone, (l) preoperative renin activity and (m) serum potassium.
Author Contributions
R.S.F., conceptualization, investigation, data curation, and writing—original draft. U.A., writing—review and editing, methodology, data curation, and resources. A.T., investigation, data curation, and writing—original draft. E.B., data curation, validation, and formal analysis. F.P., software. A.M.B., resources and investigation. L.M., software, investigation, and formal analysis. R.M., resources, visualization, and data curation. G.T., writing—review & editing and supervision. A.C., conceptualization and supervision. L.L., writing—review & editing. T.C., data curation and supervision. C.L., writing—original draft and supervision. G.S., writing—review & editing and supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fuchs, F.D.; Whelton, P.K. High Blood Pressure and Cardiovascular Disease. Hypertension 2020, 75, 285–292. [Google Scholar] [CrossRef]
- Rossi, G.P. Primary Aldosteronism: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 74, 2799–2811. [Google Scholar] [CrossRef]
- Rossi, G.P.; Bernini, G.; Caliumi, C.; Desideri, G.; Fabris, B.; Ferri, C.; Ganzaroli, C.; Giacchetti, G.; Letizia, C.; Maccario, M.; et al. A Prospective Study of the Prevalence of Primary Aldosteronism in 1,125 Hypertensive Patients. J. Am. Coll. Cardiol. 2006, 48, 2293–2300. [Google Scholar] [CrossRef] [PubMed]
- Mulatero, P.; Stowasser, M.; Loh, K.C.; Fardella, C.E.; Gordon, R.D.; Mosso, L.; Gomez-Sanchez, C.E.; Veglio, F.; Young, W.F. Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J. Clin. Endocrinol. Metab. 2004, 89, 1045–1050. [Google Scholar] [CrossRef] [Green Version]
- Lim, P.O.; Rodgers, P.; Cardale, K.; Watson, A.D.; MacDonald, T.M. Potentially high prevalence of primary aldosteronism in a primary-care population. Lancet 1999, 353, 40. [Google Scholar] [CrossRef]
- Meng, Z.; Dai, Z.; Huang, K.; Xu, C.; Zhang, Y.-G.; Zheng, H.; Liu, T.-Z. Long-Term Mortality for Patients of Primary Aldosteronism Compared with Essential Hypertension: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2020, 11, 121. [Google Scholar] [CrossRef]
- Funder, J.W.; Carey, R.M.; Mantero, F.; Murad, M.H.; Reincke, M.; Shibata, H.; Stowasser, M.; Young, W.F. The management of primary aldosteronism: Case detection, diagnosis, and treatment: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2016, 101, 1889–1916. [Google Scholar] [CrossRef] [PubMed]
- Williams, T.A.; Reincke, M. Diagnosis and management of primary aldosteronism: The endocrine society guideline 2016 revisited. Eur. J. Endocrinol. 2018, 179, R19–R29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ball, M.W.; Hemal, A.K.; Allaf, M.E. International Consultation on Urological Diseases and European Association of Urology International Consultation on Minimally Invasive Surgery in Urology: Laparoscopic and robotic adrenalectomy. BJU Int. 2017, 119, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Anceschi, U.; Tuderti, G.; Fiori, C.; Zappalà, O.; Ferriero, M.C.; Brassetti, A.; Carrara, A.; Tirone, G.; De Concilio, B.; Celia, A.; et al. Minimally Invasive Partial versus Total Adrenalectomy for the Treatment of Primary Aldosteronism: Results of a Multicenter Series According to the PASO Criteria. Eur. Urol. Focus 2021, 7, 1418–1423. [Google Scholar] [CrossRef]
- Liu, J.H.; Wei, X.D.; Fu, C.C.; Li, Q.X.; Hou, J.Q.; Lv, J.X.; Huang, Y. Long-Term Results of Laparoscopic Partial Versus Total Adrenalectomy for Aldosterone Producing Adenoma. Urol. J. 2020, 17, 4981. [Google Scholar] [CrossRef]
- Jeschke, K.; Janetschek, G.; Peschel, R.; Schellander, L.; Bartsch, G.; Henning, K. Laparoscopic partial adrenalectomy in patients with aldosterone-producing adenomas: Indications, technique, and results. Urology 2003, 61, 69–72. [Google Scholar] [CrossRef]
- Nakada, T.; Kubota, Y.; Sasagawa, I.; Yagisawa, T.; Watanabe, M.; Ishigooka, M. Therapeutic Outcome of Primary Aldosteronism: Adrenalectomy versus Enucleation of Aldosterone-Producing Adenoma. J. Urol. 1995, 153, 1775–1780. [Google Scholar] [CrossRef]
- Walz, M.K.; Gwosdz, R.; Levin, S.L.; Alesina, P.F.; Suttorp, A.-C.; Metz, K.A.; Wenger, F.A.; Petersenn, S.; Mann, K.; Schmid, K.W. Retroperitoneoscopic adrenalectomy in Conn’s syndrome caused by adrenal adenomas or nodular hyperplasia. World J. Surg. 2008, 32, 847–853. [Google Scholar] [CrossRef]
- Kaye, D.R.; Storey, B.B.; Pacak, K.; Pinto, P.A.; Linehan, W.M.; Bratslavsky, G. Partial adrenalectomy: Underused first line therapy for small adrenal tumors. J. Urol. 2010, 184, 18–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simone, G.; Anceschi, U.; Tuderti, G.; Misuraca, L.; Celia, A.; De Concilio, B.; Costantini, M.; Stigliano, A.; Minisola, F.; Ferriero, M.; et al. Robot-assisted Partial Adrenalectomy for the Treatment of Conn’s Syndrome: Surgical Technique, and Perioperative and Functional Outcomes. Eur. Urol. 2019, 75, 811–816. [Google Scholar] [CrossRef]
- Anceschi, U.; Simone, G. Reply to Franco Gaboardi, Guglielmo Mantica, and Nazareno Suardi’s Letter to the Editor re: Giuseppe Simone, Umberto Anceschi, Gabriele Tuderti, et al. Robot-assisted Partial Adrenalectomy for the Treatment of Conn’s Syndrome: Surgical Technique, and Perioperative and Functional Outcomes. Eur Urol 2019;75:811-6. Eur. Urol. 2019, 76, e144–e145. [Google Scholar] [CrossRef]
- Nagaraja, V.; Eslick, G.D.; Edirimanne, S. Recurrence and functional outcomes of partial adrenalectomy: A systematic review and meta-analysis. Int. J. Surg. 2015, 16, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Muth, A.; Ragnarsson, O.; Johannsson, G.; Wängberg, B. Systematic review of surgery and outcomes in patients with primary aldosteronism. Br. J. Surg. 2015, 102, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Li, K.-P.; Duan, X.; Yang, X.-S.; Huang, J.; Wu, T. Partial versus total adrenalectomy for the treatment of unilateral aldosterone-producing adenoma: A systematic review and meta-analysis. Updates Surg. 2021, 73, 2301–2313. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151. [Google Scholar] [CrossRef] [Green Version]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (Pico) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef]
- Frandsen, T.F.; Bruun Nielsen, M.F.; Lindhardt, C.L.; Eriksen, M.B. Using the full PICO model as a search tool for systematic reviews resulted in lower recall for some PICO elements. J. Clin. Epidemiol. 2020, 127, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; pp. 205–228. [Google Scholar]
- Phillips, B.; Ball, C.; Sackett, D. Levels of Evidence Andgrades of Recommendation; Oxford Centre for Evidence-based Medicine: Oxford, UK, 2009. [Google Scholar]
- Williams, T.A.; Lenders, J.W.M.; Mulatero, P.; Burrello, J.; Rottenkolber, M.; Adolf, C.; Satoh, F.; Amar, L.; Quinkler, M.; Deinum, J.; et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: An international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol. 2017, 5, 689–699. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- McGrath, S.; Zhao, X.F.; Steele, R.; Thombs, B.D.; Benedetti, A.; Levis, B.; Riehm, K.E.; Saadat, N.; Levis, A.W.; Azar, M.; et al. Estimating the sample mean and standard deviation from commonly reported quantiles in meta-analysis. Stat. Methods Med. Res. 2020, 29, 2520–2537. [Google Scholar] [CrossRef] [Green Version]
- Liao, C.-H.; Chung, S.-D.; Lai, M.-K.; Yu, H.-J.; Chueh, S.-C. Laparoscopic simultaneous bilateral partial and total adrenalectomy: A longer follow-up. BJU Int. 2009, 104, 1269–1273. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Liang, Y.; Lin, W.; Fu, G.-Q.; Ma, Z.-W. Surgical management of large adrenal tumors: Impact of different laparoscopic approaches and resection methods on perioperative and long-term outcomes. BMC Urol. 2018, 18, 31. [Google Scholar] [CrossRef] [Green Version]
- Balci, M.; Tuncel, A.; Aslan, Y.; Aykanat, C.; Berker, D.; Guzel, O. Laparoscopic Partial versus Total Adrenalectomy in Nonhereditary Unilateral Adrenal Masses. Urol. Int. 2020, 104, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Simforoosh, N.; Soltani, M.H.; Shemshaki, H.; Bonakdar Hashemi, M.; Dadpour, M.; Kashi, A.H. Symptom Resolution and Recurrence Outcomes after Partial versus Total Laparoscopic Adrenalectomy: 13 years of Experience with Medium-Long Term Follow up. Urol. J. 2020, 18, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Fu, B.; Zhang, X.; Wang, G.; Lang, B.; Ma, X.; Li, H.; Wang, B.; Shi, T.; Ai, X.; Zhou, H.; et al. Long-term results of a prospective, randomized trial comparing retroperitoneoscopic partial versus total adrenalectomy for aldosterone producing adenoma. J. Urol. 2011, 185, 1578–1582. [Google Scholar] [CrossRef]
- Chen, S.-F.; Chueh, S.-C.; Wang, S.-M.; Wu, V.-C.; Pu, Y.-S.; Wu, K.-D.; Huang, K.-H. Clinical outcomes in patients undergoing laparoscopic adrenalectomy for unilateral aldosterone producing adenoma: Partial versus total adrenalectomy. J. Endourol. 2014, 28, 1103–1106. [Google Scholar] [CrossRef]
- Billmann, F.; Billeter, A.; Thomusch, O.; Keck, T.; El Shishtawi, S.; Langan, E.A.; Strobel, O.; Müller-Stich, B.P. Minimally invasive partial versus total adrenalectomy for unilateral primary hyperaldosteronism-a retrospective, multicenter matched-pair analysis using the new international consensus on outcome measures. Surgery 2021, 169, 1361–1370. [Google Scholar] [CrossRef]
- Ishidoya, S.; Ito, A.; Sakai, K.; Satoh, M.; Chiba, Y.; Sato, F.; Arai, Y. Laparoscopic partial versus total adrenalectomy for aldosterone producing adenoma. J. Urol. 2005, 174, 40–43. [Google Scholar] [CrossRef]
- Proye, C.A.G.; Mulliez, E.A.R.; Carnaille, B.M.L.; Lecomte-Houcke, M.; Decoulx, M.; Wemeau, J.L.; Lefebvre, J.; Racadot, A.; Ernst, O.; Huglo, D.; et al. Essential hypertension: First reason for persistent hypertension after unilateral adrenalectomy for primary aldosteronism? Surgery 1998, 124, 1128–1133. [Google Scholar] [CrossRef] [PubMed]
- Rossi, G.P.; Bolognesi, M.; Rizzoni, D.; Seccia, T.M.; Piva, A.; Porteri, E.; Tiberio, G.A.M.; Giulini, S.M.; Agabiti-Rosei, E.; Pessina, A.C. Vascular remodeling and duration of hypertension predict outcome of adrenalectomy in primary aldosteronism patients. Hypertension 2008, 51, 1366–1371. [Google Scholar] [CrossRef] [Green Version]
- Steichen, O.; Zinzindohoué, F.; Plouin, P.F.; Amar, L. Outcomes of adrenalectomy in patients with unilateral primary aldosteronism: A review. Horm. Metab. Res. 2012, 44, 221–227. [Google Scholar] [CrossRef] [Green Version]
- Vorselaars, W.M.C.M.; van Beek, D.J.; Postma, E.L.; Spiering, W.; Borel Rinkes, I.H.M.; Valk, G.D.; Vriens, M.R.; Zarnegar, R.; Drake, F.T.; Duh, Q.Y.; et al. Clinical outcomes after surgery for primary aldosteronism: Evaluation of the PASO-investigators’ consensus criteria within a worldwide cohort of patients. Surgery 2019, 166, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Sellgren, F.; Koman, A.; Nordenström, E.; Hellman, P.; Hennings, J.; Muth, A. Outcomes after Surgery for Unilateral Dominant Primary Aldosteronism in Sweden. World J. Surg. 2020, 44, 561–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, B.S.; Turcu, A.F.; Nanba, A.T.; Hughes, D.T.; Cohen, M.S.; Gauger, P.G.; Auchus, R.J. Refining the Definitions of Biochemical and Clinical Cure for Primary Aldosteronism Using the Primary Aldosteronism Surgical Outcome (PASO) Classification System. World J. Surg. 2018, 42, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef] [Green Version]
- Brunström, M.; Carlberg, B. Association of blood pressure lowering with mortality and cardiovascular disease across blood pressure levels a systematic review and meta-analysis. JAMA Intern. Med. 2018, 178, 28–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Reincke, M.; Williams, T.A. Treatment of Unilateral PA by Adrenalectomy: Potential Reasons for Incomplete Biochemical Cure. Exp. Clin. Endocrinol. Diabetes 2019, 127, 100–108. [Google Scholar] [CrossRef] [Green Version]
- Ferriere, A.; Kerlan, V.; Tabarin, A. La chirurgie d’épargne surrénalienne: Du cortex à la médulla. Ann. Endocrinol. 2017, 78, S11–S20. [Google Scholar] [CrossRef]
- Brandao, L.F.; Autorino, R.; Laydner, H.; Haber, G.P.; Ouzaid, I.; De Sio, M.; Perdonà, S.; Stein, R.J.; Porpiglia, F.; Kaouk, J.H. Robotic versus laparoscopic adrenalectomy: A systematic review and meta-analysis. Eur. Urol. 2014, 65, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Merseburger, A.S.; Herrmann, T.R.W.; Shariat, S.F.; Kyriazis, I.; Nagele, U.; Traxer, O.; Liatsikos, E.N. EAU guidelines on robotic and single-site surgery in Urology. Eur. Urol. 2013, 64, 277–291. [Google Scholar] [CrossRef] [PubMed]
- Cacciamani, G.E.; Shakir, A.; Tafuri, A.; Gill, K.; Han, J.; Ahmadi, N.; Hueber, P.A.; Gallucci, M.; Simone, G.; Campi, R.; et al. Best practices in near-infrared fluorescence imaging with indocyanine green (NIRF/ICG)-guided robotic urologic surgery: A systematic review-based expert consensus. World J. Urol. 2020, 38, 883–896. [Google Scholar] [CrossRef] [PubMed]
- Manny, T.B.; Pompeo, A.S.; Hemal, A.K. Robotic partial adrenalectomy using indocyanine green dye with near-infrared imaging: The initial clinical experience. Urology 2013, 82, 738–742. [Google Scholar] [CrossRef] [PubMed]
- Colvin, J.; Zaidi, N.; Berber, E. The utility of indocyanine green fluorescence imaging during robotic adrenalectomy. J. Surg. Oncol. 2016, 114, 153–156. [Google Scholar] [CrossRef]
- Young, W.F.; Stanson, A.W.; Thompson, G.B.; Grant, C.S.; Farley, D.R.; Van Heerden, J.A. Role for adrenal venous sampling in primary aldosteronism. Surgery 2004, 136, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).