
Comparison of Surgical Outcomes between Trabeculectomy with Mitomycin C and Ahmed Valve Implantation with Mitomycin C in Eyes with Uveitic Glaucoma



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Outcome Measures
2.3. Surgical Procedures
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Surgical Success
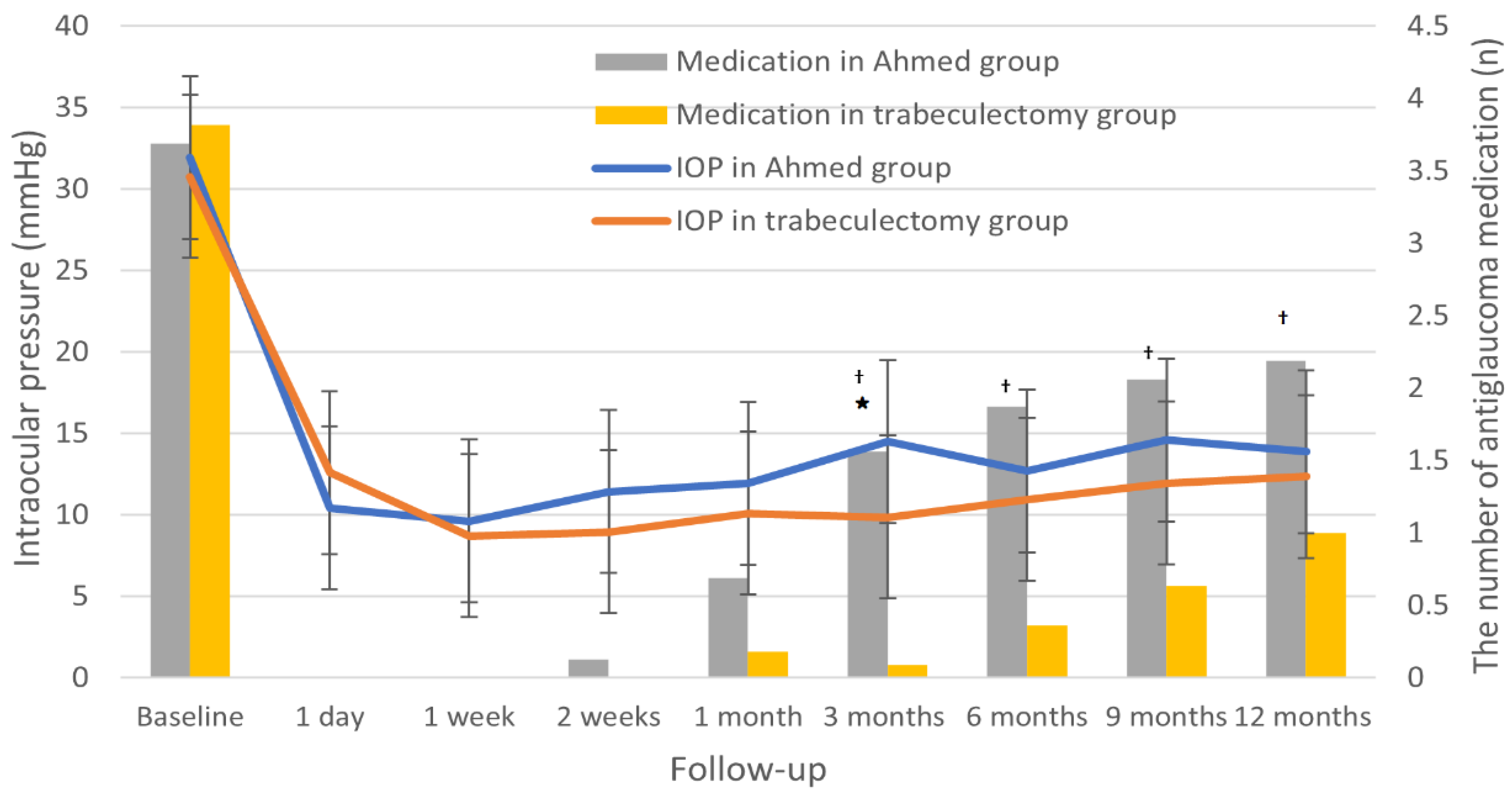
3.3. Intraocular Pressure and Number of Antiglaucoma Medications
3.4. Visual Acuity, Severity of Inflammation, and Corneal Endothelial Cell Density
3.5. Surgical Complications
3.6. Risk Factors Associated with Surgical Failure in Uveitic Glaucoma
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neri, P.; Azuara-Blanco, A.; Forrester, J.V. Incidence of glaucoma in patients with uveitis. J. Glaucoma 2004, 13, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Moorthy, R.S.; Mermoud, A.; Baerveldt, G.; Minckler, D.S.; Lee, P.P.; Rao, N.A. Glaucoma associated with uveitis. Surv. Ophthalmol. 1997, 41, 361–394. [Google Scholar] [CrossRef]
- Takahashi, T.; Ohtani, S.; Miyata, K.; Miyata, N.; Shirato, S.; Mochizuki, M. A clinical evaluation of uveitis-associated secondary glaucoma. Jpn. J. Ophthalmol. 2002, 46, 556–562. [Google Scholar] [CrossRef]
- Kalin-Hajdu, E.; Hammamji, K.; Gagne, S.; Harasymowycz, P. Outcome of viscodilation and tensioning of Schlemm’s canal for uveitic glaucoma. Can. J. Ophthalmol. 2014, 49, 414–419. [Google Scholar] [CrossRef]
- Sung, V.C.; Barton, K. Management of inflammatory glaucomas. Curr. Opin. Ophthalmol. 2004, 15, 136–140. [Google Scholar] [CrossRef]
- Iverson, S.M.; Bhardwaj, N.; Shi, W.; Sehi, M.; Greenfield, D.S.; Budenz, D.L.; Kishor, K. Surgical outcomes of inflammatory glaucoma: A comparison of trabeculectomy and glaucoma-drainage-device implantation. Jpn. J. Ophthalmol. 2015, 59, 179–186. [Google Scholar] [CrossRef]
- Zhou, M.; Wang, W.; Huang, W.; Zhang, X. Use of Mitomycin C to reduce the incidence of encapsulated cysts following ahmed glaucoma valve implantation in refractory glaucoma patients: A new technique. BMC Ophthalmol. 2014, 14, 107. [Google Scholar] [CrossRef] [Green Version]
- Papadaki, T.G.; Zacharopoulos, I.P.; Pasquale, L.R.; Christen, W.B.; Netland, P.A.; Foster, C.S. Long-term Results of Ahmed Glaucoma Valve Implantation for Uveitic Glaucoma. Am. J. Ophthalmol. 2007, 144, 62–69.e62. [Google Scholar] [CrossRef]
- Bao, N.; Jiang, Z.-X.; Coh, P.; Tao, L.-M. Long-term outcomes of uveitic glaucoma treated with Ahmed valve implant in a series of Chinese patients. Int. J. Ophthalmol. 2018, 11, 629–634. [Google Scholar] [CrossRef]
- Özdal, P.Ç.; Vianna, R.N.G.; Deschênes, J. Ahmed valve implantation in glaucoma secondary to chronic uveitis. Eye 2006, 20, 178–183. [Google Scholar] [CrossRef]
- Alvarado, J.A.; Hollander, D.A.; Juster, R.P.; Lee, L.C. Ahmed Valve Implantation with Adjunctive Mitomycin C and 5-Fluorouracil: Long-term Outcomes. Am. J. Ophthalmol. 2008, 146, 276–284.e272. [Google Scholar] [CrossRef]
- Iwao, K.; Inatani, M.; Seto, T.; Takihara, Y.; Ogata-Iwao, M.; Okinami, S.; Tanihara, H. Long-term outcomes and prognostic factors for trabeculectomy with mitomycin C in eyes with uveitic glaucoma: A retrospective cohort study. J. Glaucoma 2014, 23, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Novak-Laus, K.; Mandic, Z.; Ivekovic, R.; Korsic, J.; Tedeschi-Reiner, E.; Masnec-Paskvalin, S.; Bojic, L. Trabeculectomy with mitomycin C in glaucoma associated with uveitis. Coll. Antropol. 2005, 29 (Suppl. 1), 17–20. [Google Scholar] [PubMed]
- Carreño, E.; Villarón, S.; Portero, A.; Herreras, J.M.; Maquet, J.A.; Calonge, M. Surgical outcomes of uveitic glaucoma. J. Ophthalmic Inflamm. Infect. 2011, 1, 43–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, A.; Maruyama, K.; Yokoyama, Y.; Tsuda, S.; Ryu, M.; Nakazawa, T. Characteristics of uveitic glaucoma and evaluation of its surgical treatment. Clin. Ophthalmol. 2014, 8, 2383–2389. [Google Scholar] [CrossRef] [Green Version]
- Gil-Carrasco, F.; Salinas-VanOrman, E.; Recillas-Gispert, C.; Paczka, J.A.; Gilbert, M.; Arellanes-García, L. Ahmed valve implant for uncontrolled uveitic glaucoma. Ocul. Immunol. Inflamm. 1998, 6, 27–37. [Google Scholar] [CrossRef]
- Bettis, D.I.; Morshedi, R.G.; Chaya, C.; Goldsmith, J.; Crandall, A.; Zabriskie, N. Trabeculectomy With Mitomycin C or Ahmed Valve Implantation in Eyes With Uveitic Glaucoma. J. Glaucoma 2015, 24, 591–599. [Google Scholar] [CrossRef]
- Chow, A.; Burkemper, B.; Varma, R.; Rodger, D.C.; Rao, N.; Richter, G.M. Comparison of surgical outcomes of trabeculectomy, Ahmed shunt, and Baerveldt shunt in uveitic glaucoma. J. Ophthalmic Inflamm Infect. 2018, 8, 9. [Google Scholar] [CrossRef] [Green Version]
- Ceballos, E.M.; Beck, A.D.; Lynn, M.J. Trabeculectomy with Antiproliferative Agents in Uveitic Glaucoma. J. Glaucoma 2002, 11, 189–196. [Google Scholar] [CrossRef]
- Cui, Q.N.; Hsia, Y.C.; Lin, S.C.; Stamper, R.L.; Rose-Nussbaumer, J.; Mehta, N.; Porco, T.C.; Naseri, A.; Han, Y. Effect of mitomycin c and 5-flurouracil adjuvant therapy on the outcomes of Ahmed glaucoma valve implantation. Clin. Exp. Ophthalmol. 2017, 45, 128–134. [Google Scholar] [CrossRef]
- Kook, M.S.; Yoon, J.; Kim, J.; Lee, M.S. Clinical results of Ahmed glaucoma valve implantation in refractory glaucoma with adjunctive mitomycin C. Ophthalmic Surg. Lasers 2000, 31, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Kesav, N.; Palestine, A.G.; Kahook, M.Y.; Pantcheva, M.B. Current management of uveitis-associated ocular hypertension and glaucoma. Surv. Ophthalmol. 2020, 65, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Jabs, D.A.; Nussenblatt, R.B.; Rosenbaum, J.T.; Standardization of Uveitis Nomenclature Working, G. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am. J. Ophthalmol. 2005, 140, 509–516. [Google Scholar] [CrossRef]
- Kee, C. Prevention of early postoperative hypotony by partial ligation of silicone tube in Ahmed glaucoma valve implantation. J. Glaucoma 2001, 10, 466–469. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.J.; Kong, Y.X.G.; Tao, L.W.; Lim, L.L.; Martin, K.R.; Green, C.; Ruddle, J.; Crowston, J.G. Surgical outcomes of trabeculectomy and glaucoma drainage implant for uveitic glaucoma and relationship with uveitis activity. Clin. Exp. Ophthalmol. 2017, 45, 472–480. [Google Scholar] [CrossRef] [Green Version]
- Almobarak, F.A.; Alharbi, A.H.; Morales, J.; Aljadaan, I. Intermediate and Long-term Outcomes of Mitomycin C-enhanced Trabeculectomy as a First Glaucoma Procedure in Uveitic Glaucoma. J. Glaucoma 2017, 26, 478–485. [Google Scholar] [CrossRef]
- Kaburaki, T.; Koshino, T.; Kawashima, H.; Numaga, J.; Tomidokoro, A.; Shirato, S.; Araie, M. Initial trabeculectomy with mitomycin C in eyes with uveitic glaucoma with inactive uveitis. Eye 2009, 23, 1509–1517. [Google Scholar] [CrossRef]
- William, A.; Spitzer, M.S.; Doycheva, D.; Dimopoulos, S.; Leitritz, M.A.; Voykov, B. Comparison of ab externo trabeculotomy in primary open-angle glaucoma and uveitic glaucoma: Long-term outcomes. Clin. Ophthalmol. 2016, 10, 929–934. [Google Scholar] [CrossRef] [Green Version]
- Kanaya, R.; Kijima, R.; Shinmei, Y.; Shinkai, A.; Ohguchi, T.; Namba, K.; Chin, S.; Ishida, S. Surgical Outcomes of Trabeculectomy in Uveitic Glaucoma: A Long-Term, Single-Center, Retrospective Case-Control Study. J. Ophthalmol. 2021, 2021, 5550776. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristics | Ahmed Group (n = 16) | Trabeculectomy Group (n = 22) | p-Value |
|---|---|---|---|
| Age, yrs | 51.1 ± 17.2 | 47.2 ± 13.9 | 0.46 |
| Male, n (%) | 14 (87.5) | 17 (77.3) | 0.68 |
| Right eye, n (%) | 11 (68.8) | 9 (40.9) | 0.09 |
| Preoperative IOP, mmHg | 31.9 ± 9.9 | 30.8 ± 7.9. | 0.69 |
| Preoperative VA, logMAR | 0.60 ± 0.57 | 0.28 ± 0.30 | 0.03 |
| Preoperative inflammatory anterior chamber cell, n | 1.2 ± 1.2 | 0.8 ± 0.9 | 0.28 |
| Preoperative antiglaucoma medication, n | 3.7 ± 0.6 | 3.8 ± 0.4 | 0.69 |
| Preoperative corneal endothelial cell density, mm2 | 2036.9 ± 856.1 | 2263.0 ± 499.9 | 0.31 |
| Prior cataract surgery, n (%) | <0.001 | ||
| No | 3 (18.8) | 17 (77.3) | |
| Yes | 13 (81.3) | 5 (22.7) | |
| Duration of uveitis before surgery, m | 5.2 ± 3.4 | 5.4 ± 3.2 | 0.848 |
| Uveitis etiology, n (%) | 0.46 | ||
| Idiopathic | 12 (75.0) | 14 (63.6) | |
| Herpes simplex virus | 1 (6.3) | 3 (13.6) | |
| Cytomegalovirus | 0 | 2 (9.0) | |
| Posner Schlossman syndrome | 2 (12.5) | 1 (4.5) | |
| Ocular tuberculosis | 1 (6.3) | 0 | |
| Sarcoidosis | 0 | 1 (4.5) | |
| Behcet’s disease | 0 | 1 (4.5) |
| Rates | 6 Months | 12 Months | ||||
|---|---|---|---|---|---|---|
| Ahmed Group (n = 16) | Trabeculectomy Group (n = 22) | p-Value | Ahmed Group (n = 16) | Trabeculectomy Group (n = 22) | p-Value | |
| Complete success | 3 (18.8) | 18 (81.8) | <0.001 | 2 (12.5) | 11 (50.0) | 0.016 |
| Qualified success | 11 (68.8) | 1 (4.5) | <0.001 | 11 (68.8) | 7 (31.8) | 0.024 |
| Failure | 2 (12.5) | 3 (13.6) | 0.098 | 3 (18.8) | 4 (18.2) | 0.094 |
| Variables | Ahmed Group (n = 16) | Trabeculectomy Group (n = 22) | p-Value † | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | 6 Months | 1 Year | p-Value * | Baseline | 6 Months | 1 Year | p-Value * | ||
| VA, logMAR | 0.60 ± 0.57 | 0.67 ± 0.95 | 0.62 ± 0.83 | 0.78 | 0.28 ± 0.30 | 0.21 ± 0.27 | 0.23 ± 0.30 | 0.567 | 0.23 |
| Anterior chamber cell, n | 1.2 ± 1.2 | 0.8 ± 0.7 | 0.4 ± 0.5 | 0.019 | 0.8 ± 0.9 | 0.9 ± 1.1 | 0.6 ± 0.7 | 0.518 | 0.53 |
| Antiglaucoma medication, n | 3.7 ± 0.6 | 1.8 ± 1.1 | 2.2 ±1.1 | 0.001 | 3.8 ± 0.4 | 0.4 ± 0.8 | 1.0 ± 1.2 | <0.001 | 0.007 |
| Corneal endothelial cell density, mm2 | 2036.9 ± 856.1 | 1738.2 ± 471.9 | 1713.6 ± 541.6 | 0.004 | 2263.0 ± 499.9 | 2380.9 ± 439.7 | 2297.4 ± 616.0 | 0.881 | 0.012 |
| Ahmed Group (n = 16) | Trabeculectomy Group (n = 22) | p-Value | |
|---|---|---|---|
| No, n (%) | 11 (68.8) | 11 (50.0) | 0.682 |
| Yes, n (%) | 5 (31.3) | 11 (50.0) | |
| Acute hypotony | 2 (12.5) | 1 (4.5) | |
| Cystoid macular edema | 0 | 1 (4.5) | |
| Wound leakage | 1 (6.3) | 3 (13.6) | |
| Cataract progression | 1 (6.3) | 6 (27.3) | |
| Corneal decompensation | 1 (6.3) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.Y.; Kim, Y.H.; Kim, K.E.; Ahn, J. Comparison of Surgical Outcomes between Trabeculectomy with Mitomycin C and Ahmed Valve Implantation with Mitomycin C in Eyes with Uveitic Glaucoma. J. Clin. Med. 2022, 11, 1368. https://doi.org/10.3390/jcm11051368
Lee SY, Kim YH, Kim KE, Ahn J. Comparison of Surgical Outcomes between Trabeculectomy with Mitomycin C and Ahmed Valve Implantation with Mitomycin C in Eyes with Uveitic Glaucoma. Journal of Clinical Medicine. 2022; 11(5):1368. https://doi.org/10.3390/jcm11051368
Chicago/Turabian StyleLee, Seung Yeop, Yong Hyun Kim, Ko Eun Kim, and Jaehong Ahn. 2022. "Comparison of Surgical Outcomes between Trabeculectomy with Mitomycin C and Ahmed Valve Implantation with Mitomycin C in Eyes with Uveitic Glaucoma" Journal of Clinical Medicine 11, no. 5: 1368. https://doi.org/10.3390/jcm11051368
APA StyleLee, S. Y., Kim, Y. H., Kim, K. E., & Ahn, J. (2022). Comparison of Surgical Outcomes between Trabeculectomy with Mitomycin C and Ahmed Valve Implantation with Mitomycin C in Eyes with Uveitic Glaucoma. Journal of Clinical Medicine, 11(5), 1368. https://doi.org/10.3390/jcm11051368