
Epidemiological Trends in Patients Undergoing Mitral Valve Transcatheter Edge-to-Edge Repair over the Last Decade: Functional vs. Structural Mitral Regurgitation



Abstract
:1. Introduction
2. Methodology
Statistical Analysis
3. Results
4. Hemodynamic Measurements
Trend Differences in Different Period (2010–2015 vs. 2016–2021)
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsen, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L. Scientific Document Committee of the European Association of Cardiovascular Imaging. Recommendations for the echocardiographic assessment of native valvular regurgitation: An executive summary from the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 611–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldman, T.; Kar, S.; Rinaldi, M.; Fail, P.; Hermiller, J.; Smalling, R.; Whitlow, P.L.; Gray, W.; Low, R.; Herrmann, H.C.; et al. EVEREST Investigators. Percutaneous mitral repair with the MitraClip system: Safety and midterm durability in the initial EVEREST (Endovascular Valve Edge-to-Edge REpair Study) cohort. J. Am. Coll. Cardiol. 2009, 54, 686–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidson, L.J.; Davidson, C.J. Transcatheter treatment of valvular heart disease: A review. JAMA 2021, 325, 2480–2494. [Google Scholar] [CrossRef] [PubMed]
- Harky, A.; Botezatu, B.; Kakar, S.; Ren, M.; Shirke, M.M.; Pullan, M. Mitral valve diseases: Pathophysiology and interventions. Prog. Cardiovasc. Dis. 2021, 67, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Lim, D.S.; Kar, S.; Spargias, K.; Kipperman, R.M.; O’Neill, W.W.; Ng, M.K.C.; Fam, N.P.; Walters, D.L.; Webb, J.G.; Smith, R.L.; et al. Transcatheter Valve Repair for Patients With Mitral Regurgitation: 30-Day Results of the CLASP Study. JACC Cardiovasc. Interv. 2019, 12, 1369–1378. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; et al. COAPT Investigators. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. N. Engl. J. Med. 2018, 379, 2307–2318. [Google Scholar] [CrossRef] [PubMed]
- Obadia, J.F.; Messika-Zeitoun, D.; Leurent, G.; Iung, B.; Bonnet, G.; Piriou, N.; Lefèvre, T.; Piot, C.; Rouleau, F.; Carrié, D.; et al. MITRA-FR Investigators. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. N. Engl. J. Med. 2018, 379, 2297–2306. [Google Scholar] [CrossRef] [PubMed]
- Qadir, I.; Salick, M.M.; Perveen, S.; Sharif, H. Mortality from isolated coronary bypass surgery: A comparison of the Society of Thoracic Surgeons and the EuroSCORE risk prediction algorithms. Interact. Cardiovasc. Thorac. Surg. 2012, 14, 258–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Öztürk, C.; Friederich, M.; Werner, N.; Nickenig, G.; Hammerstingl, C.; Schueler, R. Single-center five-year outcomes after interventional edge-to-edge repair of the mitral valve. Cardiol. J. 2021, 28, 215–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demir, O.M.; Ruffo, M.M.; Godino, C.; Ancona, M.; Ancona, F.; Stella, S.; Munafó, A.R.; Sisinni, A.; Agricola, E.; Colombo, A.; et al. Mid-Term clinical outcomes following percutaneous mitral valve edge-to-edge repair. J. Invasive Cardiol. 2020, 32, E313–E320. [Google Scholar] [PubMed]
- Buzzatti, N.; Denti, P.; Scarfò, I.S.; Giambuzzi, I.; Schiavi, D.; Ruggeri, S.; Castiglioni, A.; De Bonis, M.; La Canna, G.; Alfieri, O. Mid-term outcomes (up to 5 years) of percutaneous edge-to-edge mitral repair in the real-world according to regurgitation mechanism: A single-center experience. Catheter. Cardiovasc. Interv. 2019, 94, 427–435. [Google Scholar] [CrossRef]
- Polimeni, A.; Albanese, M.; Salerno, N.; Aquila, I.; Sabatino, J.; Sorrentino, S.; Leo, I.; Cacia, M.; Signorile, V.; Mongiardo, A.; et al. Predictors of outcomes in patients with mitral regurgitation undergoing percutaneous valve repair. Sci. Rep. 2020, 10, 17144. [Google Scholar] [CrossRef]
- Liu, X.H.; Shi, J.Y.; Feng, X.J.; Feng, D.C.; Wang, L.; Pang, H.Y.; Xie, H.Z.; Wang, F.F.; Hsu, J.; Jia, F.W.; et al. Short-term and 1-year outcomes after MitraClip therapy in functional versus degenerative mitral regurgitation patients: A systematic review and meta-analysis. J. Thorac. Dis. 2018, 10, 4156–4168. [Google Scholar] [CrossRef] [PubMed]
- Chiarito, M.; Pagnesi, M.; Martino, E.A.; Pighi, M.; Scotti, A.; Biondi-Zoccai, G.; Latib, A.; Landoni, G.; Mario, C.D.; Margonato, A.; et al. Outcome after percutaneous edge-to-edge mitral repair for functional and degenerative mitral regurgitation: A systematic review and meta-analysis. Heart 2018, 104, 306–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nita, N.; Schneider, L.; Dahme, T.; Markovic, S.; Keßler, M.; Rottbauer, W.; Tadic, M. Trends in transcatheter edge-to-edge mitral valve repair over a decade: Data from the MiTra ULM registry. Front. Cardiovasc. Med. 2022, 9, 850356. [Google Scholar] [CrossRef]
- Gaemperli, O.; Biaggi, P.; Gugelmann, R.; Osranek, M.; Schreuder, J.J.; Bühler, I.; Sürder, D.; Lüscher, T.F.; Felix, C.; Bettex, D.; et al. Real-time left ventricular pressure-volume loops during percutaneous mitral valve repair with the MitraClip system. Circulation 2013, 127, 1018–1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakkestrøm, R.; Banke, A.; Christensen, N.L.; Pecini, R.; Irmukhamedov, A.; Andersen, M.; Borlaug, B.A.; Møller, J.E. Hemodynamic characteristics in significant symptomatic and asymptomatic primary mitral valve regurgitation at rest and during exercise. Circ. Cardiovasc. Imaging 2018, 11, e007171. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structural MR (n = 354) | Functional MR (n = 563) | p | |
|---|---|---|---|
| Age (years) | 78 ± 9 | 77 ± 8 | 0.097 |
| Male (%) | 154 (44) | 230 (41) | 0.450 |
| BMI (kg/m2) | 25.7 ± 4.4 | 26.0 ± 5.0 | 0.461 |
| Systolic blood pressure (mmHg) | 126 ± 21 | 125 ± 20 | 0.162 |
| Diastolic blood pressure (mmHg) | 73 ± 11 | 71 ± 12 | 0.016 |
| NYHA class | 0.716 | ||
| III (%) | 262 (74) | 414 (73) | |
| IV (%) | 92 (26) | 149 (27) | |
| Interventions and surgeries | |||
| PCI (%) | 148 (42) | 273 (48) | 0.049 |
| CABG (%) | 54 (15) | 96 (17) | 0.588 |
| Mitral valve surgery (%) | 3 (1) | 3 (0.5) | 0.681 |
| TAVR (%) | 21 (6) | 38 (7) | 0.680 |
| Aortic valve surgery (%) | 21 (6) | 29 (5) | 0.601 |
| Comorbidities | |||
| CAD (%) | 225 (64) | 385 (68) | 0.110 |
| Previous MI (%) | 76 (21) | 142 (25) | 0.355 |
| Hypertension (%) | 286 (81) | 455 (81) | 1.00 |
| Dyslipidemia (%) | 208 (59) | 335 (60) | 0.836 |
| Diabetes (%) | 86 (24) | 175 (31) | 0.029 |
| Atrial fibrillation (%) | 215 (61) | 376 (67) | 0.064 |
| Peripheral artery disease (%) | 25 (7) | 56 (10) | 0.152 |
| COPD (%) | 38 (11) | 70 (12) | 0.463 |
| OSAS (%) | 18 (5) | 36 (6) | 0.473 |
| Peptic ulcer disease (%) | 7 (2) | 13 (2) | 0.820 |
| Renal failure (%) | 172 (49) | 280 (50) | 0.786 |
| Acute renal failure (%) | 20 (6) | 23 (4) | 0.336 |
| Hepatic cirrhosis (%) | 5 (1) | 7 (1) | 1.00 |
| Previous cancer (%) | 57 (16) | 99 (17) | 0.357 |
| Antiarrhythmia devices | |||
| CRT (%) | 28 (8) | 56 (10) | 0.408 |
| ICD (%) | 30 (8) | 93 (16.5) | <0.001 |
| Pacemaker (%) | 33 (9) | 51 (9) | 0.907 |
| Scores | |||
| Euro Score II | 7.5 ± 7.3 | 8.7 ± 8.4 | 0.024 |
| Therapy | |||
| ACEI (%) | 159 (45) | 248 (44) | 0.785 |
| ARB (%) | 101 (29) | 157 (28) | 0.821 |
| ARNI (%) | 17 (5) | 51 (9) | 0.001 |
| Beta-blockers (%) | 293 (83) | 497 (88) | 0.030 |
| Aldosterone antagonists (%) | 149 (43) | 271 (48) | 0.089 |
| Statins (%) | 227 (64) | 384 (68) | 0.249 |
| Laboratory | |||
| Creatinine (μmol/L) | 129 ± 72 | 131 ± 69 | 0.710 |
| GFR (ml/min/1.73 m2) | 49 ± 20 | 48 ± 19 | 0.248 |
| NT-pro-BNP (pg/mL) | 5191 ± 6381 | 5176 ± 6175 | 0.975 |
| Echocardiography | |||
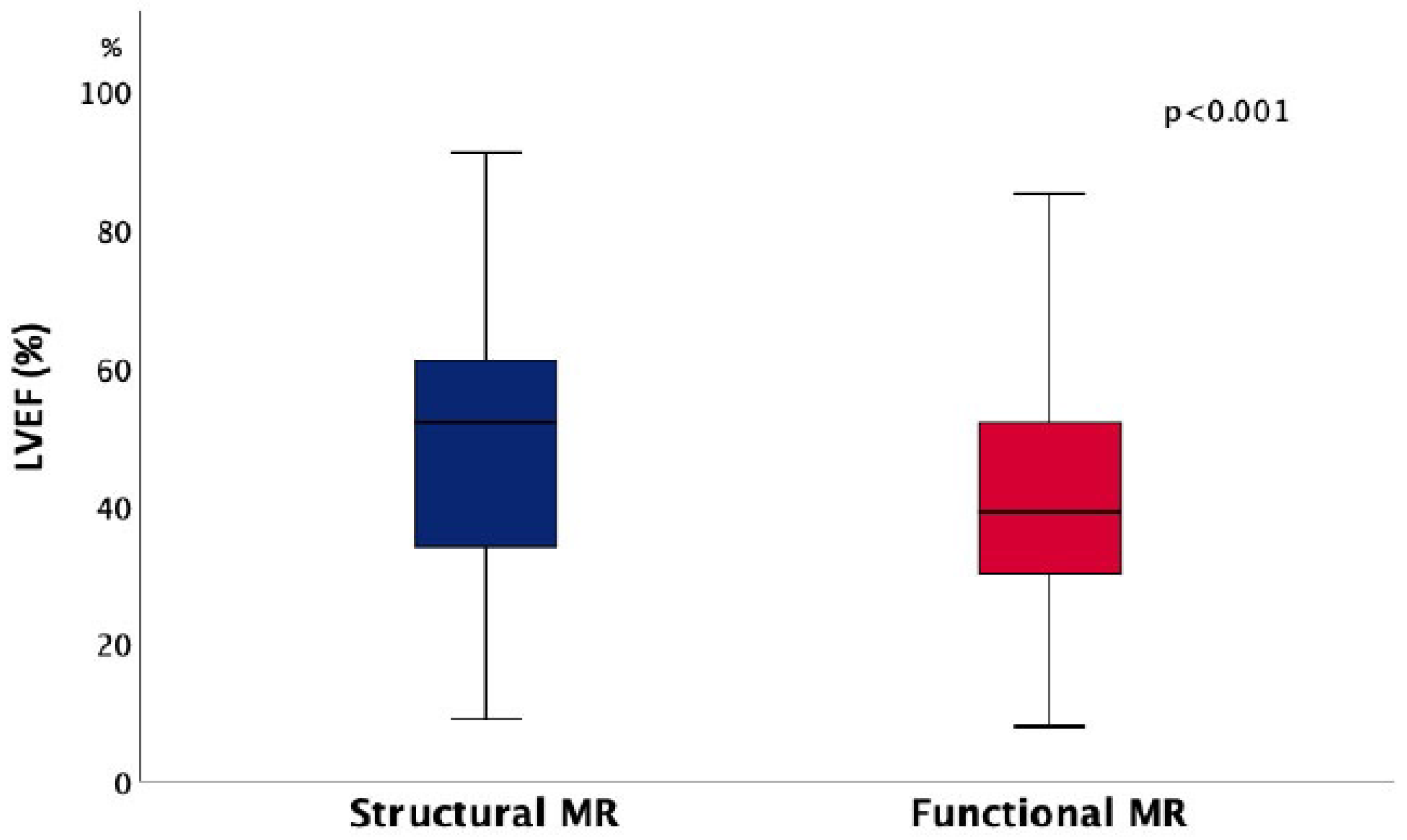
| LVEF (%) | 49 ± 18 | 41 ± 16 | <0.001 |
| LVEDD (mm) | 58 ± 11 | 61 ± 11 | 0.001 |
| LVESD (mm) | 41 ± 13 | 47 ± 13 | <0.001 |
| Interventricular septum thickness (mm) | 10.8 ± 2.4 | 11 ± 3.0 | 0.692 |
| LA (mm) | 55 ± 9 | 55 ± 9 | 0.306 |
| Intraprocedural results | |||
| MR severity after TEER | |||
| MR 1+ | 283 (80) | 473 (84) | 0.239 |
| MR 2+ | 60 (17) | 79 (14) | |
| MR 3+ | 11 (3) | 11 (2) | |
| Mitral stenosis (%) | 8 (2.2) | 13 (2.3) | 1.00 |
| Structural MR (n = 140) | Functional MR (n = 230) | p | |
|---|---|---|---|
| Heart rate (beat/min) | 72 ± 15 | 72 ± 16 | 0.868 |
| Mean RA pressure (mmHg) | 11 ± 6 | 11 ± 7 | 0.645 |
| Mean RV pressure (mmHg) | 21 ± 12 | 27 ± 14 | 0.049 |
| Systolic PA pressure (mmHg) | 52 ± 16 | 50 ± 15 | 0.189 |
| Diastolic PA pressure (mmHg) | 20 ± 9 | 20 ± 11 | 0.579 |
| Mean PA pressure (mmHg) | 35 ± 17 | 32 ± 11 | 0.095 |
| Mean PCWP (mmHg) | 23 ± 9 | 22 ± 9 | 0.303 |
| Mean LA pressure (mmHg) | 20 ± 8 | 19 ± 10 | 0.392 |
| LV end-systolic pressure (mmHg) | 124 ± 31 | 137 ± 35 | 0.284 |
| LV end-diastolic pressure (mmHg) | 20 ± 7 | 20 ± 9 | 0.937 |
| Systolic BP (mmHg) | 124 ± 32 | 127 ± 28 | 0.282 |
| Diastolic BP (mmHg) | 72 ± 18 | 64 ± 15 | 0.169 |
| Mean BP (mmHg) | 87 ± 21 | 87 ± 20 | 0.754 |
| SVR (dynes/seconds/cm−5) | 2265 ± 1680 | 1886 ± 1066 | 0.008 |
| PVR (dynes/seconds/cm−5) | 300 ± 235 | 300 ± 264 | 0.978 |
| Cardiac output (L/min) | 3.9 ± 1.2 | 3.8 ± 1.1 | 0.490 |
| Cardiac index (L/min/m2) | 2.1 ± 0.6 | 2.1 ± 0.5 | 0.672 |
| Oxygen saturation in aorta (%) | 90 ± 4 | 91 ± 4 | 0.270 |
| Oxygen saturation in PA (%) | 57 ± 10 | 57 ± 9 | 0.545 |
| 2010–2015 | 2016–2021 | 2010–2015 | 2016–2021 | |||
|---|---|---|---|---|---|---|
| Structural MR (n = 70) | Structural MR (n = 284) | p | Functional MR (n = 206) | Functional MR (n = 357) | p | |
| Age (years) | 77 ± 9 | 78 ± 8 | 0.723 | 77 ± 9 | 77 ± 8 | 0.845 |
| Male (%) | 25 (36) | 129 (34) | 0.178 | 79 (38) | 151 (42) | 0.374 |
| BMI (kg/m2) | 25.5 ± 4.1 | 25.8 ± 4.5 | 0.692 | 25.7 ± 4.5 | 26.1 ± 5.2 | 0.346 |
| Systolic blood pressure (mmHg) | 123 ± 20 | 127 ± 22 | 0.166 | 122 ± 20 | 126 ± 19 | 0.042 |
| Diastolic blood pressure (mmHg) | 72 ± 11 | 74 ± 11 | 0.141 | 70 ± 11 | 72 ± 12 | 0.088 |
| NYHA class | ||||||
| III (%) | 44 (63) | 218 (77) | 0.022 | 139 (67) | 274 (77) | 0.038 |
| IV (%) | 26 (37) | 66 (23) | 67 (33) | 82 (23) | ||
| Interventions and surgeries | ||||||
| PCI (%) | 24 (34) | 124 (44) | 0.177 | 94 (46) | 179 (50) | 0.336 |
| CABG (%) | 16 (23) | 38 (13) | 0.062 | 38 (18) | 58 (16) | 0.447 |
| Mitral valve surgery (%) | 1 (1) | 2 (1) | 0.485 | 2 (0.1) | 1 (0.2) | 0.558 |
| TAVR (%) | 3 (4) | 18 (6) | 0.777 | 10 (5) | 28 (8) | 0.222 |
| Aortic valve surgery (%) | 5 (7) | 16 (6) | 0.580 | 14 (7) | 15 (4) | 0.179 |
| Comorbidities | ||||||
| Previous MI (%) | 14 (20) | 62 (22) | 0.439 | 47 (23) | 95 (27) | 0.361 |
| CAD (%) | 49 (70) | 176 (62) | 0.208 | 151 (73) | 234 (66) | 0.070 |
| Hypertension (%) | 59 (84) | 227 (80) | 0.499 | 171 (83) | 284 (80) | 0.374 |
| Dyslipidemia (%) | 39 (56) | 169 (60) | 0.589 | 121 (59) | 214 (60) | 0.790 |
| Diabetes (%) | 20 (29) | 66 (23) | 0.354 | 60 (29) | 115 (32) | 0.508 |
| Atrial fibrillation (%) | 49 (70) | 166 (58) | 0.101 | 139 (67) | 237 (66) | 0.779 |
| Peripheral artery disease (%) | 7 (10) | 18 (6) | 0.299 | 20 (10) | 36 (10) | 1.00 |
| COPD (%) | 7 (10) | 31 (11) | 1.00 | 27 (13) | 43 (12) | 0.791 |
| OSAS (%) | 3 (4) | 15 (5) | 1.00 | 13 (6) | 23 (6) | 1.00 |
| Peptic ulcer disease (%) | 4 (6) | 3 (1) | 0.031 | 8 (4) | 5 (1) | 0.079 |
| Renal failure (%) | 37 (53) | 135 (48) | 0.505 | 117 (57) | 163 (46) | 0.011 |
| Acute renal failure (%) | 1 (1) | 19 (7) | 0.143 | 7 (3) | 16 (4) | 0.660 |
| Hepatic cirrhosis (%) | 2 (3) | 3 (10) | 0.257 | 1 (0.4) | 6 (2) | 0.432 |
| Previous cancer (%) | 10 (14) | 47 (17) | 0.720 | 36 (17) | 62 (17) | 0.974 |
| Antiarrhythmia devices | ||||||
| CRT (%) | 6 (8) | 22 (8) | 0.806 | 21 (10) | 33 (9) | 0.767 |
| ICD (%) | 10 (14) | 20 (7) | 0.058 | 45 (22) | 48 (13) | 0.013 |
| Pacemaker (%) | 8 (11) | 25 (9) | 0.494 | 22 (11) | 29 (8) | 0.361 |
| Scores | ||||||
| Euro Score II | 10.4 ± 9.9 | 6.8 ± 6.3 | <0.001 | 9.5 ± 8.3 | 8.3 ± 8.4 | 0.112 |
| Therapy | ||||||
| ACEI (%) | 38 (54) | 121 (43) | 0.107 | 112 (54) | 136 (38) | <0.001 |
| ARB (%) | 10 (14) | 91 (32) | 0.003 | 48 (23) | 109 (31) | 0.079 |
| ARNI (%) | - | 17 (6) | - | - | 51 (14.3) | - |
| Beta-blockers (%) | 57 (81) | 236 (83) | 0.723 | 182 (88) | 315 (88) | 1.00 |
| Aldosterone antagonists (%) | 24 (34) | 125 (44) | 0.140 | 93 (45) | 178 (50) | 0.294 |
| Statins (%) | 36 (51) | 191 (67) | 0.017 | 139 (67) | 245 (69) | 0.779 |
| Laboratory | ||||||
| Creatinine (μmol/L) | 127 ± 54 | 130 ± 76 | 0.759 | 131 ± 64 | 131 ± 71 | 0.962 |
| GFR (mL/min/1.73 m2) | 50 ± 18 | 49 ± 21 | 0.884 | 47 ± 19 | 48 ± 19 | 0.676 |
| NT-pro-BNP (pg/mL) | 4549 ± 5158 | 5270 ± 6520 | 0.554 | 5892 ± 6509 | 4923 ± 6042 | 0.145 |
| Echocardiography | ||||||
| LVEF (%) | 50 ± 17 | 49 ± 18 | 0.721 | 43 ± 17 | 40 ± 15 | 0.096 |
| LVEDD (mm) | 57 ± 10 | 58 ± 11 | 0.714 | 62 ± 12 | 60 ± 11 | 0.032 |
| LVESD (mm) | 39 ± 12 | 42 ± 13 | 0.245 | 48 ± 15 | 47 ± 13 | 0.225 |
| Interventricular septum thickness (mm) | 10.9 ± 2.7 | 10.8 ± 2.3 | 0.944 | 10.6 ± 2.3 | 11.2 ± 3.3 | 0.287 |
| LA (mm) | 58 ± 12 | 54 ± 9 | 0.012 | 56 ± 9 | 55 ± 10 | 0.653 |
| Intraprocedural results | ||||||
| MR severity after TEER | ||||||
| MR 1+ | 53 (76) | 230 (81) | 0.326 | 165 (80) | 308 (86) | 0.126 |
| MR 2+ | 13 (18) | 47 (17) | 35 (17) | 44 (12) | ||
| MR 3+ | 4 (6) | 7 (2) | 6 (3) | 5 (1) | ||
| Mitral stenosis (%) | 3 (4) | 5 (2) | 0.196 | 7 (3) | 6 (2) | 0.245 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schneider, L.; Nita, N.; Dahme, T.; Markovic, S.; Keßler, M.; Rottbauer, W.; Tadic, M. Epidemiological Trends in Patients Undergoing Mitral Valve Transcatheter Edge-to-Edge Repair over the Last Decade: Functional vs. Structural Mitral Regurgitation. J. Clin. Med. 2022, 11, 1422. https://doi.org/10.3390/jcm11051422
Schneider L, Nita N, Dahme T, Markovic S, Keßler M, Rottbauer W, Tadic M. Epidemiological Trends in Patients Undergoing Mitral Valve Transcatheter Edge-to-Edge Repair over the Last Decade: Functional vs. Structural Mitral Regurgitation. Journal of Clinical Medicine. 2022; 11(5):1422. https://doi.org/10.3390/jcm11051422
Chicago/Turabian StyleSchneider, Leonhard, Nicoleta Nita, Tilman Dahme, Sinisa Markovic, Mirjam Keßler, Wolfang Rottbauer, and Marijana Tadic. 2022. "Epidemiological Trends in Patients Undergoing Mitral Valve Transcatheter Edge-to-Edge Repair over the Last Decade: Functional vs. Structural Mitral Regurgitation" Journal of Clinical Medicine 11, no. 5: 1422. https://doi.org/10.3390/jcm11051422
APA StyleSchneider, L., Nita, N., Dahme, T., Markovic, S., Keßler, M., Rottbauer, W., & Tadic, M. (2022). Epidemiological Trends in Patients Undergoing Mitral Valve Transcatheter Edge-to-Edge Repair over the Last Decade: Functional vs. Structural Mitral Regurgitation. Journal of Clinical Medicine, 11(5), 1422. https://doi.org/10.3390/jcm11051422