
Adherence and Persistence to Biological Drugs for Psoriasis: Systematic Review with Meta-Analysis

 , ,
, ,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Selection Process
2.4. Data Extraction Process
2.5. Study Risk of Bias Assessment
2.6. Effect Measures
2.7. Synthesis Methods
3. Results
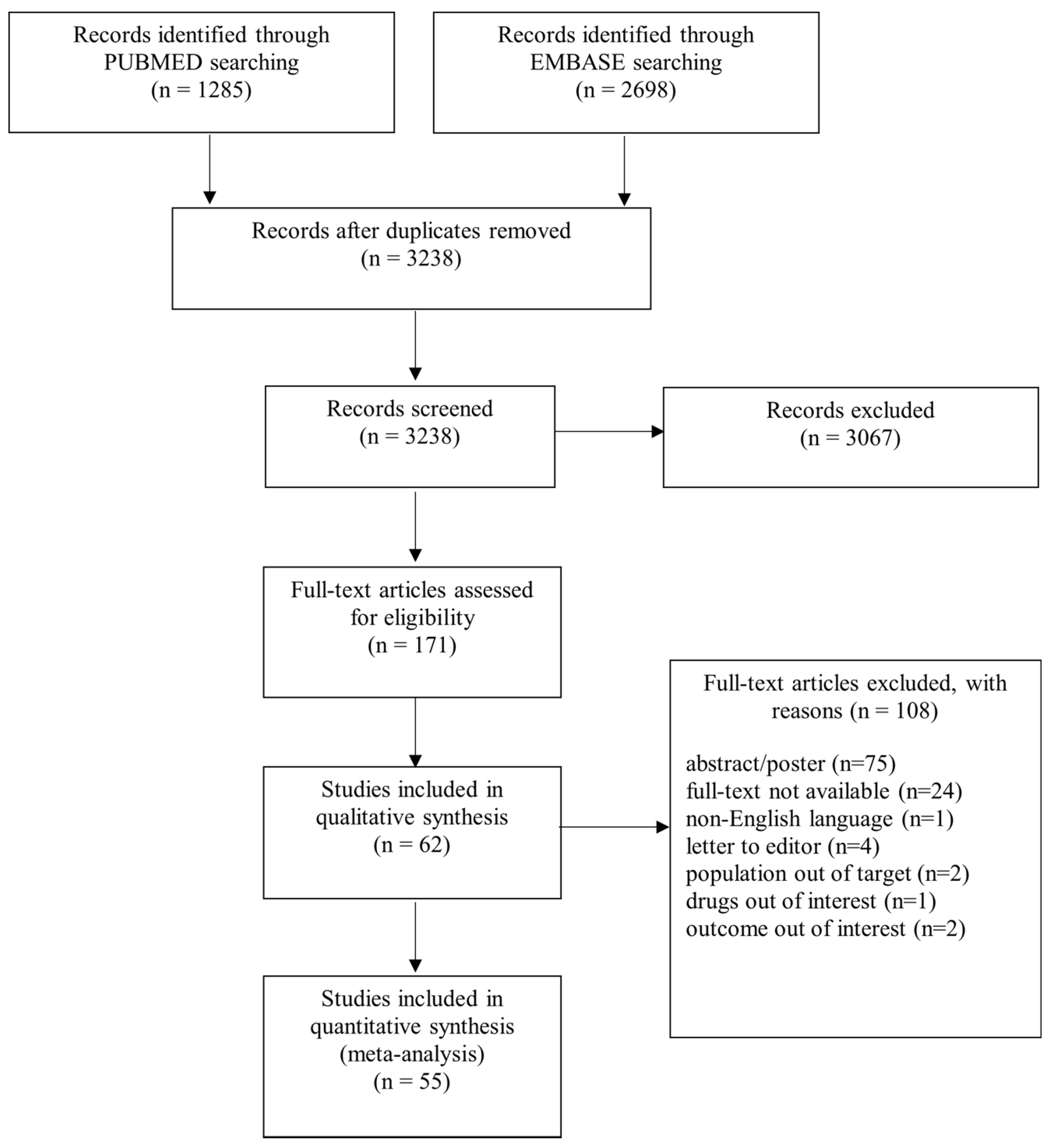
3.1. Systematic Review
3.2. Risk of Bias in Studies
3.3. Results of Synthesis
3.3.1. Adherence
3.3.2. Persistence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parisi, R.; Iskandar, I.Y.K.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.M.; Ashcroft, D.M. National, regional, and worldwide epidemiology of psoriasis: Systematic analysis and modelling study. BMJ 2020, 369, m1590. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Kishimoto, M.; Sugai, J.; Komine, M.; Ohtsuki, M. Risk factors for the development of psoriasis. Int. J. Mol. Sci. 2019, 20, 4347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, T.; Takahashi, H.; Kawada, A.; Iizuka, H.; Nakagawa, H. Epidemiological survey from 2009 to 2012 of psoriatic patients in Japanese Society for Psoriasis Research. J. Dermatol. 2018, 45, 251–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhosle, M.J.; Kulkarni, A.; Feldman, S.R.; Balkrishnan, R. Quality of life in patients with psoriasis. Health Qual. Life Outcomes 2006, 4, 35. [Google Scholar] [CrossRef] [Green Version]
- Silva, L.C.R.; Ortigosa, L.C.M.; Benard, G. Anti-TNF-α agents in the treatment of immune-mediated inflammatory diseases: Mechanisms of action and pitfalls. Immunotherapy 2010, 2, 817–833. [Google Scholar] [CrossRef]
- Giunta, A.; Ventura, A.; Chimenti, M.S.; Bianchi, L.; Esposito, M. Spotlight on ixekizumab for the treatment of moderate-to-severe plaque psoriasis: Design, development, and use in therapy. Drug Des. Devel. Ther. 2017, 2017, 1643–1651. [Google Scholar] [CrossRef] [Green Version]
- Ergen, E.N.; Yusuf, N. Inhibition of interleukin-12 and/or interleukin-23 for the treatment of psoriasis: What is the evidence for an effect on malignancy? Exp. Dermatol. 2018, 27, 737–747. [Google Scholar] [CrossRef]
- Belinchón, I.; Rivera, R.; Blanch, C.; Comellas, M.; Lizán, L. Adherence, satisfaction and preferences for treatment in patients with psoriasis in the European union: A systematic review of the literature. Patient Prefer. Adherence 2016, 10, 2357–2367. [Google Scholar] [CrossRef] [Green Version]
- De Vera, M.A.; Mailman, J.; Galo, J.S. Economics of Non-Adherence to Biologic Therapies in Rheumatoid Arthritis. Curr. Rheumatol. Rep. 2014, 16, 460. [Google Scholar] [CrossRef]
- Aleshaki, J.S.; Cardwell, L.A.; Muse, M.E.; Feldman, S.R. Adherence and resource use among psoriasis patients treated with biologics. Expert Rev. Pharm. Outcomes Res. 2018, 18, 609–617. [Google Scholar] [CrossRef]
- Hoy, D.; Brooks, P.; Woolf, A.; Blyth, F.; March, L.; Bain, C.; Baker, P.; Smith, E.; Buchbinder, R. Assessing risk of bias in prevalence studies: Modification of an existing tool and evidence of interrater agreement. J. Clin. Epidemiol. 2012, 65, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, A.F.; Choi, A.S.; Le, Q.T.; Ko, D.T.; Han, J.K.; Park, S.S.; Jackevicius, C.A. Real-World Adherence and Persistence to Direct Oral Anticoagulants in Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e005969. [Google Scholar] [CrossRef] [PubMed]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dávila-Seijo, P.; Dauden, E.; Carretero, G.; Ferrandiz, C.; Vanaclocha, F.; Gómez-García, F.-J.; Herrera-Ceballos, E.; De la Cueva-Dobao, P.; Belinchón, I.; Sánchez-Carazo, J.-L.; et al. Survival of classic and biological systemic drugs in psoriasis: Results of the BIOBADADERM registry and critical analysis. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1942–1950. [Google Scholar] [CrossRef]
- Gniadecki, R.; Bang, B.; Bryld, L.E.; Iversen, L.; Lasthein, S.; Skov, L. Comparison of long-term drug survival and safety of biologic agents in patients with psoriasis vulgaris. Br. J. Dermatol. 2015, 172, 244–252. [Google Scholar] [CrossRef]
- Yeung, H.; Wan, J.; Van Voorhees, A.S.; Callis Duffin, K.; Krueger, G.G.; Kalb, R.E.; Weisman, J.D.; Sperber, B.R.; Brod, B.A.; Schleicher, S.M.; et al. Patient-reported reasons for the discontinuation of commonly used treatments for moderate to severe psoriasis. J. Am. Acad. Dermatol. 2013, 68, 64–72. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Luo, Y.; Lv, C.; Zheng, X.; Zhu, W.; Chen, X.; Shen, M.; Kuang, Y. Nonadherence to Treatment and Patient-Reported Outcomes of Psoriasis During the COVID-19 Epidemic: A Web-Based Survey. Patient Prefer. Adherence 2020, 14, 1403–1409. [Google Scholar] [CrossRef]
- Bergman, M.; Patel, P.; Chen, N.; Jing, Y.; Saffore, C.D. Evaluation of Adherence and Persistence Differences Between Adalimumab Citrate-Free and Citrate Formulations for Patients with Immune-Mediated Diseases in the United States. Rheumatol. Ther. 2020, 8, 109–118. [Google Scholar] [CrossRef]
- Marshall, J.K.; Bessette, L.; Shear, N.H.; Lebovic, G.; Glass, J.; Millson, B.; Gaetano, T.; Gazel, S.; Latour, M.G.; Laliberté, M.-C.; et al. Canada’s Study of Adherence Outcomes in Patients Receiving Adalimumab: 3-year Results from the COMPANION Study. Clin. Ther. 2018, 40, 1024–1032. [Google Scholar] [CrossRef] [Green Version]
- Ichiyama, S.; Ito, M.; Funasaka, Y.; Abe, M.; Nishida, E.; Muramatsu, S.; Nishihara, H.; Kato, H.; Morita, A.; Imafuku, S.; et al. Assessment of medication adherence and treatment satisfaction in Japanese patients with psoriasis of various severities. J. Dermatol. 2018, 45, 727–731. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Foster, S.A.; Comer, B.S.; Lin, C.-Y.; Malatestinic, W.; Burge, R.; Goldblum, O. Real-world health outcomes in adults with moderate-to-severe psoriasis in the United States: A population study using electronic health records to examine patient-perceived treatment effectiveness, medication use, and healthcare resource utilization. BMC Dermatol. 2018, 18, 4. [Google Scholar] [CrossRef] [PubMed]
- Bhosle, M.J.; Feldman, S.R.; Camacho, F.T.; Timothy Whitmire, J.; Nahata, M.C.; Balkrishnan, R. Medication adherence and health care costs associated with biologics in Medicaid-enrolled patients with psoriasis. J. Dermatolog. Treat. 2006, 17, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Clemmensen, A.; Spon, M.; Skov, L.; Zachariae, C.; Gniadecki, R. Responses to ustekinumab in the anti-TNF agent-naïve vs. anti-TNF agent-exposed patients with psoriasis vulgaris. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 1037–1040. [Google Scholar] [CrossRef] [PubMed]
- Conesa-Nicolás, E.; García-Lagunar, M.H.; Núñez-Bracamonte, S.; García-Simón, M.S.; Mira-Sirvent, M.C. Persistence of secukinumab in patients with psoriasis, psoriatic arthritis, and ankylosing spondylitis. Farm. Hosp. 2020, 45, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Degli Esposti, L.; Sangiorgi, D.; Perrone, V.; Radice, S.; Clementi, E.; Perone, F.; Buda, S. Adherence and resource use among patients treated with biologic drugs: Findings from BEETLE study. Clinicoecon. Outcomes Res. 2014, 6, 401–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dommasch, E.D.; Lee, M.P.; Joyce, C.J.; Garry, E.M.; Gagne, J.J. Drug utilization patterns and adherence in patients on systemic medications for the treatment of psoriasis: A retrospective, comparative cohort study. J. Am. Acad. Dermatol. 2018, 79, 1061–1068.e1. [Google Scholar] [CrossRef]
- Doshi, J.A.; Takeshita, J.; Pinto, L.; Li, P.; Yu, X.; Rao, P.; Viswanathan, H.N.; Gelfand, J.M. Biologic therapy adherence, discontinuation, switching, and restarting among patients with psoriasis in the US Medicare population. J. Am. Acad. Dermatol. 2016, 74, 1057–1065.e4. [Google Scholar] [CrossRef] [Green Version]
- Egeberg, A.; Bryld, L.E.; Skov, L. Drug survival of secukinumab and ixekizumab for moderate-to-severe plaque psoriasis. J. Am. Acad. Dermatol. 2019, 81, 173–178. [Google Scholar] [CrossRef]
- Esposito, M.; Gisondi, P.; Cassano, N.; Ferrucci, G.; Del Giglio, M.; Loconsole, F.; Giunta, A.; Vena, G.A.; Chimenti, S.; Girolomoni, G. Survival rate of antitumour necrosis factor-α treatments for psoriasis in routine dermatological practice: A multicentre observational study. Br. J. Dermatol. 2013, 169, 666–672. [Google Scholar] [CrossRef]
- Esposito, M.; Gisondi, P.; Cassano, N.; Babino, G.; Cannizzaro, M.V.; Ferrucci, G.; Chimenti, S.; Giunta, A. Treatment adherence to different etanercept regimens, continuous vs. intermittent, in patients affected by plaque-type psoriasis. Drug Dev. Res. 2014, 75 (Suppl. 1), S31–S34. [Google Scholar] [CrossRef]
- Feldman, S.R.; Zhao, Y.; Navaratnam, P.; Friedman, H.S.; Lu, J.; Tran, M.H. Patterns of medication utilization and costs associated with the use of etanercept, adalimumab, and ustekinumab in the management of moderate-to-severe psoriasis. J. Manag. Care Spec. Pharm. 2015, 21, 201–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldman, S.R.; Zhang, J.; Martinez, D.J.; Lopez-Gonzalez, L.; Marchlewicz, E.H.; Shrady, G.; Mendelsohn, A.M.; Zhao, Y. Real-world treatment patterns and healthcare costs of biologics and apremilast among patients with moderate-to-severe plaque psoriasis by metabolic condition status. J. Dermatolog. Treat. 2021, 32, 203–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blauvelt, A.; Shi, N.; Burge, R.; Malatestinic, W.N.; Lin, C.-Y.; Lew, C.R.; Zimmerman, N.M.; Goldblum, O.M.; Zhu, B.; Murage, M.J. Comparison of real-world treatment patterns among patients with psoriasis prescribed ixekizumab or secukinumab. J. Am. Acad. Dermatol. 2020, 82, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Ferrières, L.; Konstantinou, M.P.; Bulai Livideanu, C.; Hegazy, S.; Tauber, M.; Amelot, F.; Paul, C. Long-term continuation with secukinumab in psoriasis: Association with patient profile and initial psoriasis clearance. Clin. Exp. Dermatol. 2019, 44, e230–e234. [Google Scholar] [CrossRef]
- Gendelman, O.; Weitzman, D.; Rosenberg, V.; Shalev, V.; Chodick, G.; Amital, H. Characterization of adherence and persistence profile in a real-life population of patients treated with adalimumab. Br. J. Clin. Pharmacol. 2018, 84, 786–795. [Google Scholar] [CrossRef] [Green Version]
- Gniadecki, R.; Kragballe, K.; Dam, T.N.; Skov, L. Comparison of drug survival rates for adalimumab, etanercept and infliximab in patients with psoriasis vulgaris. Br. J. Dermatol. 2011, 164, 1091–1096. [Google Scholar] [CrossRef]
- Hendrix, N.; Marcum, Z.A.; Veenstra, D.L. Medication persistence of targeted immunomodulators for plaque psoriasis: A retrospective analysis using a U.S. claims database. Pharmacoepidemiol. Drug Saf. 2020, 29, 675–683. [Google Scholar] [CrossRef]
- Higa, S.; Devine, B.; Patel, V.; Baradaran, S.; Wang, D.; Bansal, A. Psoriasis treatment patterns: A retrospective claims study. Curr. Med. Res. Opin. 2019, 35, 1727–1733. [Google Scholar] [CrossRef] [Green Version]
- Howe, A.; Ten Eyck, L.; Dufour, R.; Shah, N.; Harrison, D.J. Treatment patterns and annual drug costs of biologic therapies across indications from the Humana commercial database. J. Manag. Care Spec. Pharm. 2014, 20, 1236–1244. [Google Scholar] [CrossRef] [Green Version]
- Hsu, D.Y.; Gniadecki, R. Patient Adherence to Biologic Agents in Psoriasis. Dermatology 2016, 232, 326–333. [Google Scholar] [CrossRef]
- Iskandar, I.Y.K.; Warren, R.B.; Lunt, M.; Mason, K.J.; Evans, I.; McElhone, K.; Smith, C.H.; Reynolds, N.J.; Ashcroft, D.M.; Griffiths, C.E.M. Differential Drug Survival of Second-Line Biologic Therapies in Patients with Psoriasis: Observational Cohort Study from the British Association of Dermatologists Biologic Interventions Register (BADBIR). J. Investig. Dermatol. 2018, 138, 775–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobi, A.; Rustenbach, S.J.; Augustin, M. Comorbidity as a predictor for drug survival of biologic therapy in patients with psoriasis. Int. J. Dermatol. 2016, 55, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Khalid, J.M.; Fox, K.M.; Globe, G.; Maguire, A.; Chau, D. Treatment patterns and therapy effectiveness in psoriasis patients initiating biologic therapy in England. J. Dermatolog. Treat. 2014, 25, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Blauvelt, A.; Shi, N.; Burge, R.; Malatestinic, W.N.; Lin, C.-Y.; Lew, C.R.; Zimmerman, N.M.; Goldblum, O.M.; Zhu, B.; Murage, M.J. Comparison of Real-World Treatment Patterns Among Psoriasis Patients Treated with Ixekizumab or Adalimumab. Patient Prefer. Adherence 2020, 14, 517–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Xie, L.; Wang, Y.; Vaidya, N.; Baser, O. Evaluating the Effect of Treatment Persistence on the Economic Burden of Moderate to Severe Psoriasis and/or Psoriatic Arthritis Patients in the U.S. Department of Defense Population. J. Manag. Care Spec. Pharm. 2018, 24, 654–663. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhou, H.; Cai, B.; Kahler, K.H.; Tian, H.; Gabriel, S.; Arcona, S. Group-based trajectory modeling to assess adherence to biologics among patients with psoriasis. Clinicoecon. Outcomes Res. 2014, 6, 197–208. [Google Scholar] [CrossRef] [Green Version]
- Magis, Q.; Jullien, D.; Gaudy-Marqueste, C.; Baumstark, K.; Viguier, M.; Bachelez, H.; Guibal, F.; Delaporte, E.; Karimova, E.; Montaudié, H.; et al. Predictors of long-term drug survival for infliximab in psoriasis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 96–101. [Google Scholar] [CrossRef]
- Mahlich, J.; Alba, A.; El Hadad, L.; Leisten, M.-K.; Peitsch, W.K. Drug Survival of Biological Therapies for Psoriasis Treatment in Germany and Associated Costs: A Retrospective Claims Database Analysis. Adv. Ther. 2019, 36, 1684–1699. [Google Scholar] [CrossRef]
- Malatestinic, W.; Nordstrom, B.; Wu, J.J.; Goldblum, O.; Solotkin, K.; Lin, C.-Y.; Kistler, K.; Fraeman, K.; Johnston, J.; Hawley, L.L.; et al. Characteristics and Medication Use of Psoriasis Patients Who May or May Not Qualify for Randomized Controlled Trials. J. Manag. Care Spec. Pharm. 2017, 23, 370–381. [Google Scholar] [CrossRef]
- Menter, A.; Papp, K.A.; Gooderham, M.; Pariser, D.M.; Augustin, M.; Kerdel, F.A.; Fakharzadeh, S.; Goyal, K.; Calabro, S.; Langholff, W.; et al. Drug survival of biologic therapy in a large, disease-based registry of patients with psoriasis: Results from the Psoriasis Longitudinal Assessment and Registry (PSOLAR). J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1148–1158. [Google Scholar] [CrossRef]
- Mercadal Orfila, G.; Ventayol Bosch, P.; Maestre Fullana, M.A.; Serrano López De Las Hazas, J.; Fernández Cortés, F.; Palomero Massanet, A.; García Álvarez, Á. Persistence and cost of biologic agents for psoriasis: Retrospective study in the Balearic Islands. Eur. J. Clin. Pharm. 2016, 18, 163–170. [Google Scholar]
- Mocanu, M.; Toader, M.-P.; Rezus, E.; Taranu, T. Aspects concerning patient adherence to anti-TNFα therapy in psoriasis: A decade of clinical experience. Exp. Ther. Med. 2019, 18, 4987–4992. [Google Scholar] [CrossRef] [PubMed]
- Murage, M.J.; Anderson, A.; Casso, D.; Oliveria, S.A.; Ojeh, C.K.; Muram, T.M.; Merola, J.F.; Zbrozek, A.; Araujo, A.B. Treatment patterns, adherence, and persistence among psoriasis patients treated with biologics in a real-world setting, overall and by disease severity. J. Dermatolog. Treat. 2019, 30, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Murage, M.J.; Gilligan, A.M.; Tran, O.; Goldblum, O.; Burge, R.; Lin, C.-Y.; Qureshi, A. Ixekizumab treatment patterns and healthcare utilization and costs for patients with psoriasis. J. Dermatolog. Treat. 2021, 32, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Bonafede, M.; Fox, K.M.; Watson, C.; Princic, N.; Gandra, S.R. Treatment patterns in the first year after initiating tumor necrosis factor blockers in real-world settings. Adv. Ther. 2012, 29, 664–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onsun, N.; Güneş, B.; Yabacı, A. Retention and survival rate of etanercept in psoriasis over 15 years and patient outcomes during the COVID-19 pandemic: The real-world experience of a single center. Dermatol. Ther. 2021, 34, e14623. [Google Scholar] [CrossRef]
- Pogácsás, L.; Borsi, A.; Takács, P.; Remenyik, É.; Kemény, L.; Kárpáti, S.; Holló, P.; Wikonkál, N.; Gyulai, R.; Károlyi, Z.; et al. Long-term drug survival and predictor analysis of the whole psoriatic patient population on biological therapy in Hungary. J. Dermatolog. Treat. 2017, 28, 635–641. [Google Scholar] [CrossRef] [Green Version]
- Ross, C.; Marshman, G.; Grillo, M.; Stanford, T. Biological therapies for psoriasis: Adherence and outcome analysis from a clinical perspective. Australas. J. Dermatol. 2016, 57, 137–140. [Google Scholar] [CrossRef]
- Ruiz-Villaverde, R.; Rodriguez-Fernandez-Freire, L.; Galán-Gutierrez, M.; Armario-HIta, J.C.; Martinez-Pilar, L. Drug survival, discontinuation rates, and safety profile of secukinumab in real-world patients: A 152-week, multicenter, retrospective study. Int. J. Dermatol. 2020, 59, 633–639. [Google Scholar] [CrossRef]
- Sbidian, E.; Mezzarobba, M.; Weill, A.; Coste, J.; Rudant, J. Persistence of treatment with biologics for patients with psoriasis: A real-world analysis of 16545 biologic-naïve patients from the French National Health Insurance database (SNIIRAM). Br. J. Dermatol. 2019, 180, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Sruamsiri, R.; Iwasaki, K.; Tang, W.; Mahlich, J. Persistence rates and medical costs of biological therapies for psoriasis treatment in Japan: A real-world data study using a claims database. BMC Dermatol. 2018, 18, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svedbom, A.; Dalén, J.; Mamolo, C.; Cappelleri, J.C.; Petersson, I.F.; Ståhle, M. Treatment patterns with topicals, traditional systemics and biologics in psoriasis—A Swedish database analysis. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Thorneloe, R.J.; Griffiths, C.E.M.; Emsley, R.; Ashcroft, D.M.; Cordingley, L. Intentional and Unintentional Medication Non-Adherence in Psoriasis: The Role of Patients’ Medication Beliefs and Habit Strength. J. Investig. Dermatol. 2018, 138, 785–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umezawa, Y.; Nobeyama, Y.; Hayashi, M.; Fukuchi, O.; Ito, T.; Saeki, H.; Nakagawa, H. Drug survival rates in patients with psoriasis after treatment with biologics. J. Dermatol. 2013, 40, 1008–1013. [Google Scholar] [CrossRef]
- van den Reek, J.M.P.A.; Tummers, M.; Zweegers, J.; Seyger, M.M.B.; van Lümig, P.P.M.; Driessen, R.J.B.; van de Kerkhof, P.C.M.; Kievit, W.; de Jong, E.M.G.J. Predictors of adalimumab drug survival in psoriasis differ by reason for discontinuation: Long-term results from the Bio-CAPTURE registry. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 560–565. [Google Scholar] [CrossRef]
- Bonafede, M.; Johnson, B.H.; Fox, K.M.; Watson, C.; Gandra, S.R. Treatment patterns with etanercept and adalimumab for psoriatic diseases in a real-world setting. J. Dermatolog. Treat. 2013, 24, 369–373. [Google Scholar] [CrossRef]
- Verma, L.; Mayba, J.N.; Gooderham, M.J.; Verma, A.; Papp, K.A. Persistency of Biologic Therapies for Plaque Psoriasis in 2 Large Community Practices. J. Cutan. Med. Surg. 2018, 22, 38–43. [Google Scholar] [CrossRef]
- Wu, B.; Muser, E.; Teeple, A.; Pericone, C.D.; Feldman, S.R. Treatment adherence and persistence of five commonly prescribed medications for moderate to severe psoriasis in a U.S. commercially insured population. J. Dermatolog. Treat. 2021, 32, 595–602. [Google Scholar] [CrossRef]
- Yiu, Z.Z.N.; Mason, K.J.; Hampton, P.J.; Reynolds, N.J.; Smith, C.H.; Lunt, M.; Griffiths, C.E.M.; Warren, R.B. Drug survival of adalimumab, ustekinumab and secukinumab in patients with psoriasis: A prospective cohort study from the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR). Br. J. Dermatol. 2020, 183, 294–302. [Google Scholar] [CrossRef] [Green Version]
- Zagni, E.; Colombo, D.; Fiocchi, M.; Perrone, V.; Sangiorgi, D.; Andretta, M.; De Sarro, G.; Nava, E.; Degli Esposti, L. Pharmaco-utilization of biologic drugs in patients affected by psoriasis, psoriatic arthritis and ankylosing spondylitis in an Italian real-world setting. Expert Rev. Pharm. Outcomes Res. 2020, 20, 491–497. [Google Scholar] [CrossRef]
- Zschocke, I.; Ortland, C.; Reich, K. Evaluation of adherence predictors for the treatment of moderate to severe psoriasis with biologics: The importance of physician-patient interaction and communication. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Carter, C.; Wilson, K.L.; Schenkel, B. Ustekinumab dosing, persistence, and discontinuation patterns in patients with moderate-to-severe psoriasis. J. Dermatolog. Treat. 2015, 26, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.A.; Hussain, F.; Lawson, L.G.; Ormerod, A.D. Factors affecting adherence to treatment of psoriasis: Comparing biologic therapy to other modalities. J. Dermatolog. Treat. 2013, 24, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Chastek, B.; Fox, K.M.; Watson, C.; Kricorian, G.; Gandra, S.R. Psoriasis treatment patterns with etanercept and adalimumab in a United States health plan population. J. Dermatolog. Treat. 2013, 24, 25–33. [Google Scholar] [CrossRef]
- Chastek, B.; White, J.; Van Voorhis, D.; Tang, D.; Stolshek, B.S. A Retrospective Cohort Study Comparing Utilization and Costs of Biologic Therapies and JAK Inhibitor Therapy Across Four Common Inflammatory Indications in Adult US Managed Care Patients. Adv. Ther. 2016, 33, 626–642. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.; Rupniewska, E.; Neighbors, M.; Singer, D.; Chiarappa, J.; Obando, C. Real-world evidence on adherence, persistence, switching and dose escalation with biologics in adult inflammatory bowel disease in the United States: A systematic review. J. Clin. Pharm. Ther. 2019, 44, 495–507. [Google Scholar] [CrossRef] [Green Version]
- Murage, M.J.; Tongbram, V.; Feldman, S.R.; Malatestinic, W.N.; Larmore, C.J.; Muram, T.M.; Burge, R.T.; Bay, C.; Johnson, N.; Clifford, S.; et al. Medication adherence and persistence in patients with rheumatoid arthritis, psoriasis, and psoriatic arthritis: A systematic literature review. Patient Prefer. Adherence 2018, 12, 1483–1503. [Google Scholar] [CrossRef] [Green Version]
- Lin, P.-T.; Wang, S.-H.; Chi, C.-C. Drug survival of biologics in treating psoriasis: A meta-analysis of real-world evidence. Sci. Rep. 2018, 8, 16068. [Google Scholar] [CrossRef] [Green Version]
- Mourad, A.I.; Gniadecki, R. Biologic Drug Survival in Psoriasis: A Systematic Review & Comparative Meta-Analysis. Front. Med. 2020, 7, 625755. [Google Scholar]
- Geale, K.; Lindberg, I.; Paulsson, E.C.; Wennerström, E.C.M.; Tjärnlund, A.; Noel, W.; Enkusson, D.; Theander, E. Persistence of biologic treatments in psoriatic arthritis: A population-based study in Sweden. Rheumatol. Adv. Pract. 2020, 4, rkaa070. [Google Scholar] [CrossRef]
- Warren, R.B.; Smith, C.H.; Yiu, Z.Z.N.; Ashcroft, D.M.; Barker, J.N.W.N.; Burden, A.D.; Lunt, M.; McElhone, K.; Ormerod, A.D.; Owen, C.M.; et al. Differential Drug Survival of Biologic Therapies for the Treatment of Psoriasis: A Prospective Observational Cohort Study from the British Association of Dermatologists Biologic Interventions Register (BADBIR). J. Investig. Dermatol. 2015, 135, 2632–2640. [Google Scholar] [CrossRef] [PubMed]
- Kaur, P.; Pannu, H.S.; Malhi, A.K. Comprehensive Study of Continuous Orthogonal Moments—A Systematic Review. ACM Comput. Surv. 2019, 52, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Raebel, M.A.; Schmittdiel, J.; Karter, A.J.; Konieczny, J.L.; Steiner, J.F. Standardizing terminology and definitions of medication adherence and persistence in research employing electronic databases. Med. Care 2013, 51, S11–S21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahil, S.K.; Ezejimofor, M.C.; Exton, L.S.; Manounah, L.; Burden, A.D.; Coates, L.C.; de Brito, M.; McGuire, A.; Murphy, R.; Owen, C.M.; et al. Comparing the efficacy and tolerability of biologic therapies in psoriasis: An updated network meta-analysis. Br. J. Dermatol. 2020, 183, 638–649. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, L.M.; Malottki, K.; Sabry-Grant, C.; Yasmeen, N.; Wright, E.; Sohrt, A.; Borg, E.; Warren, R.B. Assessing the relative efficacy of interleukin-17 and interleukin-23 targeted treatments for moderate-to-severe plaque psoriasis: A systematic review and network meta-analysis of PASI response. PLoS ONE 2019, 14, e0220868. [Google Scholar] [CrossRef] [Green Version]
- Sbidian, E.; Chaimani, A.; Afach, S.; Doney, L.; Dressler, C.; Hua, C.; Mazaud, C.; Phan, C.; Hughes, C.; Riddle, D.; et al. Systemic pharmacological treatments for chronic plaque psoriasis: A network meta-analysis. Cochrane Database Syst. Rev. 2020, 1, CD011535. [Google Scholar] [CrossRef]
- Reich, K.; Burden, A.D.; Eaton, J.N.; Hawkins, N.S. Efficacy of biologics in the treatment of moderate to severe psoriasis: A network meta-analysis of randomized controlled trials. Br. J. Dermatol. 2012, 166, 179–188. [Google Scholar] [CrossRef]
- Kisielnicka, A.; Szczerkowska-Dobosz, A.; Nowicki, R. The influence of body weight of patients with chronic plaque psoriasis on biological treatment response. Adv. Dermatol. Allergol. Dermatol. Alergol. 2020, 37, 168–173. [Google Scholar] [CrossRef]
- Anghel, F.; Nitusca, D.; Cristodor, P. Body Mass Index Influence for the Personalization of the Monoclonal Antibodies Therapy for Psoriasis. Life 2021, 11, 1316. [Google Scholar] [CrossRef]
- Giunta, A.; Babino, G.; Ruzzetti, M.; Manetta, S.; Chimenti, S.; Esposito, M. Influence of body mass index and weight on etanercept efficacy in patients with psoriasis: A retrospective study. J. Int. Med. Res. 2016, 44, 72–75. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Facciorusso, A.; Singh, A.G.; Casteele, N.V.; Zarrinpar, A.; Prokop, L.J.; Grunvald, E.L.; Curtis, J.R.; Sandborn, W.J. Obesity and response to anti-tumor necrosis factor-α agents in patients with select immune-mediated inflammatory diseases: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0195123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yanaba, K.; Umezawa, Y.; Ito, T.; Hayashi, M.; Kikuchi, S.; Fukuchi, O.; Saeki, H.; Nakagawa, H. Impact of obesity on the efficacy of ustekinumab in Japanese patients with psoriasis: A retrospective cohort study of 111 patients. Arch. Dermatol. Res. 2014, 306, 921–925. [Google Scholar] [CrossRef]
- Di Lernia, V.; Tasin, L.; Pellicano, R.; Zumiani, G.; Albertini, G. Impact of body mass index on retention rates of anti-TNF-alfa drugs in daily practice for psoriasis. J. Dermatolog. Treat. 2012, 23, 404–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zweegers, J.; van den Reek, J.M.P.A.; van de Kerkhof, P.C.M.; Otero, M.E.; Kuijpers, A.L.A.; Koetsier, M.I.A.; Arnold, W.P.; Berends, M.A.M.; Weppner-Parren, L.; Ossenkoppele, P.M.; et al. Body mass index predicts discontinuation due to ineffectiveness and female sex predicts discontinuation due to side-effects in patients with psoriasis treated with adalimumab, etanercept or ustekinumab in daily practice: A prospective, comparative, long-. Br. J. Dermatol. 2016, 175, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Hansel, T.T.; Kropshofer, H.; Singer, T.; Mitchell, J.A.; George, A.J.T. The safety and side effects of monoclonal antibodies. Nat. Rev. Drug Discov. 2010, 9, 325–338. [Google Scholar] [CrossRef] [PubMed]
- Afif, W.; Loftus, E.V.J.; Faubion, W.A.; Kane, S.V.; Bruining, D.H.; Hanson, K.A.; Sandborn, W.J. Clinical utility of measuring infliximab and human anti-chimeric antibody concentrations in patients with inflammatory bowel disease. Am. J. Gastroenterol. 2010, 105, 1133–1139. [Google Scholar] [CrossRef]
- Harding, F.A.; Stickler, M.M.; Razo, J.; DuBridge, R.B. The immunogenicity of humanized and fully human antibodies: Residual immunogenicity resides in the CDR regions. MAbs 2010, 2, 256–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loft, N.D.; Vaengebjerg, S.; Halling, A.-S.; Skov, L.; Egeberg, A. Adverse events with IL-17 and IL-23 inhibitors for psoriasis and psoriatic arthritis: A systematic review and meta-analysis of phase III studies. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1151–1160. [Google Scholar] [CrossRef]
- Matsui, T.; Umetsu, R.; Kato, Y.; Hane, Y.; Sasaoka, S.; Motooka, Y.; Hatahira, H.; Abe, J.; Fukuda, A.; Naganuma, M.; et al. Age-related trends in injection site reaction incidence induced by the tumor necrosis factor-α (TNF-α) inhibitors etanercept and adalimumab: The Food and Drug Administration adverse event reporting system, 2004–2015. Int. J. Med. Sci. 2017, 14, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Campi, P.; Benucci, M.; Manfredi, M.; Demoly, P. Hypersensitivity reactions to biological agents with special emphasis on tumor necrosis factor-alpha antagonists. Curr. Opin. Allergy Clin. Immunol. 2007, 7, 393–403. [Google Scholar] [CrossRef]
- Sfikakis, P.P.; Iliopoulos, A.; Elezoglou, A.; Kittas, C.; Stratigos, A. Psoriasis induced by anti-tumor necrosis factor therapy: A paradoxical adverse reaction. Arthritis Rheum. 2005, 52, 2513–2518. [Google Scholar] [CrossRef] [PubMed]
- Kerensky, T.A.; Gottlieb, A.B.; Yaniv, S.; Au, S. Etanercept: Efficacy and safety for approved indications. Expert Opin. Drug Saf. 2012, 11, 121–139. [Google Scholar] [CrossRef] [PubMed]
- Leman, J.; Burden, A. Treatment of severe psoriasis with infliximab. Ther. Clin. Risk Manag. 2008, 4, 1165–1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, E.J.; Beck, K.M.; Liao, W. Secukinumab in the treatment of psoriasis: Patient selection and perspectives. Psoriasis Auckl. 2018, 8, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, S.; Warren, R.B. Ixekizumab for the treatment of psoriasis: Up-to-date. Expert Opin. Biol. Ther. 2020, 20, 549–557. [Google Scholar] [CrossRef]
- Leonardi, C.L.; Kimball, A.B.; Papp, K.A.; Yeilding, N.; Guzzo, C.; Wang, Y.; Li, S.; Dooley, L.T.; Gordon, K.B. Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 76-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 1). Lancet 2008, 371, 1665–1674. [Google Scholar] [CrossRef]
- Ghosh, S.; Gensler, L.S.; Yang, Z.; Gasink, C.; Chakravarty, S.D.; Farahi, K.; Ramachandran, P.; Ott, E.; Strober, B.E. Ustekinumab Safety in Psoriasis, Psoriatic Arthritis, and Crohn’s Disease: An Integrated Analysis of Phase II/III Clinical Development Programs. Drug Saf. 2019, 42, 751–768. [Google Scholar] [CrossRef] [Green Version]
- Sandoval, L.F.; Huang, K.E.; Feldman, S.R. Adherence to ustekinumab in psoriasis patients. J. Drugs Dermatol. 2013, 12, 1090–1092. [Google Scholar]
- Chi, C.-C.; Wang, S.-H. Efficacy and cost-efficacy of biologic therapies for moderate to severe psoriasis: A meta-analysis and cost-efficacy analysis using the intention-to-treat principle. Biomed Res. Int. 2014, 2014, 862851. [Google Scholar] [CrossRef]
- Rouse, N.C.; Farhangian, M.E.; Wehausen, B.; Feldman, S.R. The cost-effectiveness of ustekinumab for moderate-to-severe psoriasis. Expert Rev. Pharm. Outcomes Res. 2015, 15, 877–884. [Google Scholar] [CrossRef]
- D’Souza, L.S.; Payette, M.J. Estimated cost efficacy of systemic treatments that are approved by the US Food and Drug Administration for the treatment of moderate to severe psoriasis. J. Am. Acad. Dermatol. 2015, 72, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Feldman, S.R.; Evans, C.; Russell, M.W. Systemic treatment for moderate to severe psoriasis: Estimates of failure rates and direct medical costs in a north-eastern US managed care plan. J. Dermatolog. Treat. 2005, 16, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Choi, C.W.; Choi, J.Y.; Kim, B.R.; Youn, S.W. Economic Burden Can Be the Major Determining Factor Resulting in Short-Term Intermittent and Repetitive Ustekinumab Treatment for Moderate-to-Severe Psoriasis. Ann. Dermatol. 2018, 30, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Sudharshan, L.; Hsu, M.-A.; Koenig, A.S.; Cappelleri, J.C.; Liu, W.F.; Smith, T.W.; Pasquale, M.K. Patient preferences associated with therapies for psoriatic arthritis: A conjoint analysis. Am. Health Drug Benefits 2018, 11, 408–416. [Google Scholar] [PubMed]
- Torres, T.; Puig, L.; Vender, R.; Lynde, C.; Piaserico, S.; Carrascosa, J.M.; Gisondi, P.; Daudén, E.; Conrad, C.; Mendes-Bastos, P.; et al. Drug Survival of IL-12/23, IL-17 and IL-23 Inhibitors for Psoriasis Treatment: A Retrospective Multi-Country, Multicentric Cohort Study. Am. J. Clin. Dermatol. 2021, 22, 567–579. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. of Studies (No. of Patients) | |
|---|---|
| Adherence | |
| MPR/PDC mean | |
| during a period of 12 months | 2 (4832) [27,53] |
| during a period of >12 months | 3 (6297) [22,33,44] |
| Good adherence | |
| MPR/PDC ≥ 80% | |
| during a period of 12 months | 6 (29,256) [25,26,27,49,53,68] |
| during a period of >12 months | 5 (11,516) [32,33,35,40,44] |
| Other definitions during different or not-specified periods a | 5 (4480) [21,46,63,71,73] |
| Persistence | |
| No discontinuation or gap a or switch | |
| during a period of <12 months | 2 (1179) [23,72] |
| during a period of 12 months | 24 (114,864) [24,27,28,31,37,38,39,43,45,48,49,51,53,54,55,60,61,62,64,65,66,68,74,75] |
| during a period of >12 months | 11 (24,246) [29,33,34,41,42,44,50,56,58,59,67,69] |
| during a not-specified period | 1 (84) [52] |
| Still on treatment | |
| after a period of <12 months | 1 (378) [25] |
| after a period of 12 months or more | 4 (2336) [30,36,47,57] |
| Other definitions during different or not-specified periods | 2 (13,714) [21,70] |
| No. of Studies | No. of Patients | Adherence, %, [CI 95%] | I2 | Q | p-Value for Heterogeneity within Strata | p-Value for Heterogeneity between Strata | |
|---|---|---|---|---|---|---|---|
| Overall | 16 | 45,252 | 61 [48; 73] | 99.7% | 5205.80 | 0 | |
| Study design | |||||||
| Cross-sectional | 3 | 753 | 85 [55; 100] | 98% | 89.03 | <0.0001 | 0.06 |
| Retrospective cohort | 13 | 44,499 | 54 [43; 66] | 100% | 4905.70 | <0.0001 | |
| Biological drug | |||||||
| ADA | 10 | 19,340 | 62 [47; 76] | 100.0% | 2263.54 | 0 | 0.04 |
| ETN | 8 | 11,376 | 50 [36; 65] | 100.0% | 1444.93 | <0.0001 | |
| INF | 3 | 650 | 63 [44; 80] | 94.0% | 33.15 | <0.0001 | |
| UST | 7 | 6179 | 72 [48; 91] | 99.0% | 1087.17 | <0.0001 | |
| IXE | 2 | 1291 | 46 [43; 48] | 0.0% | 0.28 | 0.5976 | |
| SECU | 3 | 2036 | 52 [35; 68] | 98.0% | 128.11 | <0.0001 | |
| Not specified | 5 | 4380 | 61 [33; 85] | 97.0% | 129.88 | <0.0001 | |
| Type of patient | |||||||
| Biological naïve | 6 | 33,301 | 52 [39; 65] | 99.8% | 3107.32 | 0 | 0.29 |
| Not specified | 12 | 12,912 | 63 [47; 78] | 99.1% | 1198.03 | <0.0001 | |
| No. of Studies | No. of Patients | Persistence, %, [CI 95%] | I2 | Q | p-Value for Heterogeneity within Strata | p-Value for Heterogeneity between Strata | |
|---|---|---|---|---|---|---|---|
| Overall | 46 | 156,801 | 63 [57; 68] | 100.0% | 19,429.06 | 0 | |
| Study design | |||||||
| Retrospective cohort | 42 | 146,657 | 62 [56; 68] | 100.0% | 16,496.95 | 0 | 0.07 |
| Prospective cohort | 4 | 10,144 | 71 [63; 77] | 96.1% | 76.69 | <0.001 | |
| Biological drug | |||||||
| ADA | 22 | 21,176 | 57 [50; 63] | 99.0% | 2428.85 | 0 | <0.001 |
| ETN | 19 | 12,914 | 53 [42; 65] | 99.0% | 2770.05 | 0 | |
| INF | 14 | 1465 | 64 [60; 68] | 56.0% | 29.85 | 0.0049 | |
| UST | 17 | 11,869 | 77 [70; 84] | 98.0% | 1045.48 | <0.001 | |
| IXE | 4 | 2155 | 70 [52; 85] | 98.0% | 176.12 | <0.001 | |
| SECU | 9 | 3053 | 72 [58; 84] | 99.0% | 585.42 | <0.001 | |
| Not specified | 12 | 90,014 | 55 [44; 66] | 100.0% | 9286.07 | 0 | |
| Type of patient | |||||||
| Biological naïve | 21 | 66,821 | 56 [49; 64] | 100.0% | 5408.54 | 0 | 0.05 |
| Biological experienced | 4 | 43,097 | 50 [35; 65] | 100.0% | 1638.78 | <0.001 | |
| Not specified | 25 | 46,583 | 67 [60; 74] | 100.0% | 5961.35 | 0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piragine, E.; Petri, D.; Martelli, A.; Janowska, A.; Dini, V.; Romanelli, M.; Calderone, V.; Lucenteforte, E. Adherence and Persistence to Biological Drugs for Psoriasis: Systematic Review with Meta-Analysis. J. Clin. Med. 2022, 11, 1506. https://doi.org/10.3390/jcm11061506
Piragine E, Petri D, Martelli A, Janowska A, Dini V, Romanelli M, Calderone V, Lucenteforte E. Adherence and Persistence to Biological Drugs for Psoriasis: Systematic Review with Meta-Analysis. Journal of Clinical Medicine. 2022; 11(6):1506. https://doi.org/10.3390/jcm11061506
Chicago/Turabian StylePiragine, Eugenia, Davide Petri, Alma Martelli, Agata Janowska, Valentina Dini, Marco Romanelli, Vincenzo Calderone, and Ersilia Lucenteforte. 2022. "Adherence and Persistence to Biological Drugs for Psoriasis: Systematic Review with Meta-Analysis" Journal of Clinical Medicine 11, no. 6: 1506. https://doi.org/10.3390/jcm11061506
APA StylePiragine, E., Petri, D., Martelli, A., Janowska, A., Dini, V., Romanelli, M., Calderone, V., & Lucenteforte, E. (2022). Adherence and Persistence to Biological Drugs for Psoriasis: Systematic Review with Meta-Analysis. Journal of Clinical Medicine, 11(6), 1506. https://doi.org/10.3390/jcm11061506