
Double Balloon Catheter (Plus Oxytocin) versus Dinoprostone Vaginal Insert for Term Rupture of Membranes: A Randomized Controlled Trial (RUBAPRO)

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
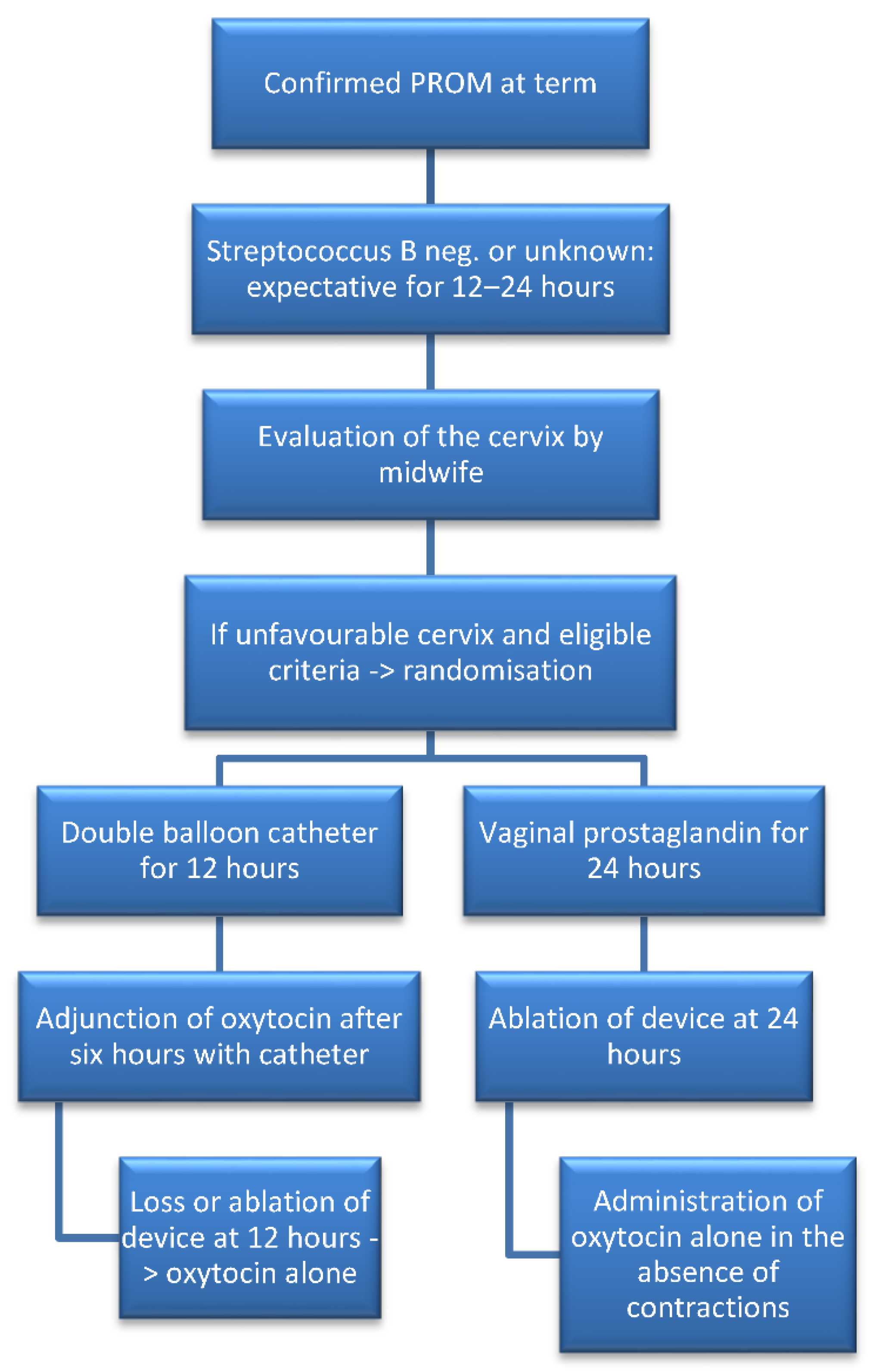
2.2. Study Procedures
2.3. Statistical Analysis and Sample Size Calculations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Senat, M.-V.; Schmitz, T.; Bouchghoul, H.; Diguisto, C.; Girault, A.; Paysant, S.; Sibiude, J.; Lassel, L.; Sentilhes, L. Term Prelabor Rupture of Membranes: CNGOF Guidelines for Clinical Practice—Short Text. Gynecol. Obstet. Fertil. Senol. 2020, 48, 15–18. [Google Scholar]
- Seaward, P.G.; Hannah, M.E.; Myhr, T.L.; Farine, D.; Ohlsson, A.; Wang, E.E.; Haque, K.; Weston, J.A.; Hewson, S.A.; Ohel, G.; et al. International multicentre term prelabor rupture of membranes study: Evaluation of predictors of clinical chorioamnionitis and postpartum fever in patients with prelabor rupture of membranes at term. Am. J. Obstet. Gynecol. 1997, 177, 1024–1029. [Google Scholar] [CrossRef]
- Hannah, M.E.; Ohlsson, A.; Farine, D.; Hewson, S.A.; Hodnett, E.D.; Myhr, T.L.; Wang, E.E.; Weston, J.A.; Willan, A.R. Induction of labor compared with expectant management for prelabor rupture of the membranes at term. N. Engl. J. Med. 1996, 334, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Huret, C.; Pereira, B.; Collange, V.; Delabaere, A.; Rouzaire, M.; Lemery, D.; Sapin, V.; Gallot, D. Premature rupture of membranes≥37 weeks of gestation: Predictive factors for labour onset within 24 hours. Gynecol. Obstet. Fertil. Senol. 2017, 45, 348–352. [Google Scholar] [PubMed]
- Sibiude, J. Term Prelabor Rupture of Membranes: CNGOF Guidelines for Clinical Practice—Timing of Labor Induction. Gynecol. Obstet. Fertil. Senol. 2020, 48, 35–47. [Google Scholar] [PubMed]
- Prelabor Rupture of Membranes: ACOG Practice Bulletin, Number 217. Obstet. Gynecol. 2020, 135, e80–e97. [CrossRef]
- Girault, A. Term Prelabor Rupture of Membranes: CNGOF Guidelines for Clinical Practice—Methods for Inducing Labor. Gynecol. Obstet. Fertil. Senol. 2020, 48, 48–58. [Google Scholar] [PubMed]
- Kruit, H.; Tihtonen, K.; Raudaskoski, T.; Ulander, V.-M.; Aitokallio-Tallberg, A.; Heikinheimo, O.; Paavonen, J.; Rahkonen, L.; Kruit, H. Foley Catheter or Oral Misoprostol for Induction of Labor in Women with Term Premature Rupture of Membranes: A Randomized Multicenter Trial. Am. J. Perinatol. 2016, 33, 866–872. [Google Scholar]
- Amorosa, J.M.H.; Stone, J.; Factor, S.H.; Booker, W.; Newland, M.; Bianco, A. A randomized trial of Foley Bulb for Labor Induction in Premature Rupture of Membranes in Nulliparas (FLIP). Am. J. Obstet. Gynecol. 2017, 217, e1–e360. [Google Scholar] [CrossRef]
- Mackeen, A.D.; Durie, D.E.; Lin, M.; Huls, C.K.; Qureshey, E.; Paglia, M.J.; Sun, H.; Sciscione, A. Foley plus oxytocin compared with oxytocin for induction after membrane rupture: A randomized controlled trial. Obstet. Gynecol. 2018, 131, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, I.B.; Quiñones, J.N.; Durie, D.; Rust, J.; Smulian, J.C.; Scorza, W.E. Use of intracervical balloons and chorioamnionitis in term premature rupture of membranes. J. Matern.-Fetal Neonatal Med. 2016, 29, 967–971. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.M.; Lappen, J.R.; Gecsi, K.S.; Hackney, D.N. Cervical ripening balloon with and without oxytocin in multiparas: A randomized controlled trial. Am. J. Obstet. Gynecol. 2018, 219, e1–e294. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: https://www.cookmedical.com/data/resources/RH-D25085-FRCA-F_M3_1463771416666.pdf (accessed on 24 March 2020).
- Haute Autorité de Santé—Déclenchement Artificiel du Travail à Partir de 37 Semaines d’Aménorrhée. Available online: https://www.has-sante.fr/jcms/c_666473/fr/declenchement-artificiel-du-travail-a-partir-de-37-semaines-d-amenorrhee (accessed on 24 March 2020).
- Devillard, E.; Delabaere, A.; Rouzaire, M.; Pereira, B.; Accoceberry, M.; Houllem, C.; Dejou-Bouillet, L.; Bouchet, P.; Gallot, D. Induction of labour in case of premature rupture of membranes at term with an unfavourable cervix: Protocol for a randomised controlled trial comparing double balloon catheter (+oxytocin) and vaginal prostaglandin (RUBAPRO) treatments. BMJ Open 2019, 9, e026090. [Google Scholar] [CrossRef]
- Mackeen, A.D.; Walker, L.; Ruhstaller, K.; Schuster, M.; Sciscione, A. Foley catheter vs prostaglandin as ripening agent in pregnant women with premature rupture of membranes. J. Am. Osteopath. Assoc. 2014, 114, 686–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suffecool, K.; Rosenn, B.M.; Kam, S.; Mushi, J.; Foroutan, J.; Herrera, K. Labor induction in nulliparous women with an unfavorable cervix: Double balloon catheter versus dinoprostone. J. Perinat. Med. 2014, 42, 213–218. [Google Scholar] [CrossRef]
- Wu, X.; Wang, C.; Li, Y.; Ouyang, C.; Liao, J.; Cai, W.; Zhong, Y.; Zhang, J.; Chen, H. Cervical dilation balloon combined with intravenous drip of oxytocin for induction of term labor: A multicenter clinical trial. Arch. Gynecol. Obstet. 2018, 297, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, L.T.; Gardner, B.; Rahman, M.; Schoen, C.; Connolly, K.A.; Hankins, G.D.; Saade, G.R.; Saad, A.F. Cervical Ripening Using Foley Balloon with or without Oxytocin: A Systematic Review and Meta-Analysis. Am. J. Perinatol. 2019, 36, 406–421. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.M.; Rayburn, W.F.; Smith, C.V. Patterns of uterine activity after intravaginal prostaglandin E2 during preinduction cervical ripening. Am. J. Obstet. Gynecol. 1991, 165 Pt 1, 1006–1009. [Google Scholar] [CrossRef]
- Pettker, C.M.; Pocock, S.B.; Smok, D.P.; Lee, S.M.; Devine, P.C. Transcervical foley catheter with and without oxytocin for cervical ripening: A randomized controlled trial. Obstet. Gynecol. 2008, 111, 1320–1326. [Google Scholar] [CrossRef] [PubMed]
- Wolff, K.; Swahn, M.L.; Westgren, M. Balloon catheter for induction of labor in nulliparous women with prelabor rupture of the membranes at term. Gynecol. Obstet. Investig. 1998, 46, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Kruit, H.; Tolvanen, J.; Eriksson, J.; Place, K.; Nupponen, I.; Rahkonen, L. Balloon catheter use for cervical ripening in women with term pre-labor rupture of membranes: A 5-year cohort study. Acta Obstet. Gynecol. Scand. 2020, 99, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Menon, R.; Taylor, B.D. Exploring Inflammatory Mediators in Fetal and Maternal Compartments during Human Parturition. Obstet. Gynecol. 2019, 134, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Menon, R.; Richardson, L.S. Preterm prelabor rupture of the membranes: A disease of the fetal membranes. Semin. Perinatol. 2017, 41, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Gibbins, J.; Thomson, A.M. Women’s expectations and experiences of childbirth. Midwifery 2001, 17, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Boyon, C.; Monsarrat, N.; Clouqueur, E.; Deruelle, P. Maturation cervicale: Y a-t-il un avantage à utiliser un double ballonnet pour le déclenchement du travail? Gynécol. Obstét. Fertil. 2014, 42, 674–680. [Google Scholar] [CrossRef]
- Lim, S.E.L.; Tan, T.L.; Ng, G.Y.H.; Tagore, S.; Kyaw, E.E.P.; Yeo, G.S.H. Patient satisfaction with the cervical ripening balloon as a method for induction of labour: A randomised controlled trial. Singap. Med. J. 2018, 59, 419–424. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variable | Double Balloon Plus Oxytocine (n = 40) | Vaginal Dinoprostone Insert (n = 40) |
|---|---|---|
| Maternal age in y Median [IQR] | 27.5 [24.9–30.6] | 27.7 [25.4–30.4] |
| Parity | ||
| Nulliparous | 29 (72.5%) | 29 (72.5%) |
| Parous | 11 (27.5%) | 11 (27.5%) |
| Maternal prepregnancy BMI in kg/m² Median [IQR] | 23.3 [20.6–28.4] | 24.6 [22–27.3] |
| Associated pregnancy pathologies | 7 (17.5%) | 9 (22.5%) |
| Diabetes mellitus | 5 (12.5%) | 6 (15%) |
| HTN | 0 | 0 |
| Preeclampsia | 0 | 0 |
| IUGR | 0 | 0 |
| Other | 2 (5%) | 4 (10%) |
| Gestational age at PROM in w, Median [IQR] | 39.4 [38.2–40.4] | 39.3 [38.5–40.3] |
| Bishop score at randomization Mean ± SD | 3.5 ± 1.1 | 3.5 ± 1.3 |
| Variable | Double Balloon Plus Oxytocine (n = 40) | Vaginal Dinoprostone (n = 40) | p Value |
|---|---|---|---|
| Time PROM to IOL in h Median [IQR] | 25.9 [22.8–29.4] | 26.8 [24–29.4] | 0.46 |
| Time IOL—loss ou removal of device in h, Median [IQR] | 8.6 [5.0–12.0] | 13.0 [6.6–18.4] | 0.02 |
| Time IOL—active labor phase in h, Median [IQR] | 10 [6.8–12.5] | 13.4 [8–19.8] | 0.03 |
| Nulliparous | 10 [7.5–12.5] | 14.7 [9.7–23.6] | 0.03 |
| Parous | 9.4 [5.5–12.5] | 9.9 [4.3–15.3] | 0.60 |
| Time IOL—full dilatation in h Median [IQR] | 13.9 [11.8–18.3] | 16.6 [9.3–24] | 0.45 |
| Nulliparous | 14.5 [11.9–19] | 19.9 [13–29.5] | 0.06 |
| Parous | 12.3 [10.2–15.8] | 8.7 [4.9–16.6] | 0.22 |
| Time IOL—delivery, h Median [IQR] | 16.2 [14–19.4] | 20.2 [12–30.4] | 0.12 |
| Nulliparous | 17 [15.3–22] | 26.5 [15.5–33.6] | 0.006 |
| Parous | 12.6 [10.6–16.2] | 9.0 [4.9–16.8] | 0.19 |
| Time IOL—vaginal delivery, h Median [IQR] | 15.8 [13.8–18.9] | 17.8 [9.7–27.9] | 0.48 |
| Nulliparous | 16.3 [14.4–21] | 23.1 [14.4–33.6] | 0.06 |
| Parous | 12.6 [10.6–16.2] | 9.0 [4.9–16.8] | 0.19 |
| Rate of IOL—delivery <24 h | 36 (90%) | 23 (57.5%) | 0.001 |
| Nulliparous | 26 (89.6%) | 12 (41.4%) | 0.001 |
| Parous | 10 (90.9%) | 11 (100%) | 1.00 |
| Rate of IOL—vaginal delivery <24 h | 31 (88.5%) | 22 (66.6%) | 0.03 |
| Nulliparous | 21 (87.5%) | 11 (50%) | 0.01 |
| Parous | 10 (90.9%) | 11 (100%) | 1.00 |
| Variable | Double Balloon Plus Oxytocine (n = 40) | Vaginal Dinoprostone (n = 40) | p Value |
|---|---|---|---|
| Oxytocin use during labor in UI, Mean (± SD) | 2.74 ± 3.22 | 1.33 ± 1.73 | 0.002 |
| Abnormal FHR rate leading to: | |||
| Ripening device removal | 0 | 0 | 1.00 |
| Oxytocin discontinuation | 6 (15%) | 3 (7.5%) | 0.48 |
| Uterine hyperstimulation | 2 (5%) | 1 (2.5%) | 1.00 |
| Fever during labor | 1 (2.5%) | 1 (2.5%) | 1.00 |
| Epidural use | 40 (100%) | 38 (95%) | 0.49 |
| Delivery mode | 0.78 | ||
| Vaginal delivery | 35 | 33 | |
| Spontaneous | 30 (75%) | 27 (67.5%) | |
| Extraction | 5 (12.5%) | 6 (15%) | |
| Caesarean section | 5 (12.5%) | 7 (17.5%) | |
| Caesarean indications | 5 | 7 | |
| Failure of induction | 1 (20%) | 1 (14.5%) | |
| Failure of dilatation progress | 4 (80%) | 5 (71%) | |
| Nonreassuring FHR | 0 | 1 (14.5%) | |
| Postpartum hemorrhage * | 5 (12.5%) | 6 (15%) | 0.75 |
| Variable | Double Balloon Plus Oxytocine (n = 40) | Vaginal Dinoprostone (n = 40) | p Value |
|---|---|---|---|
| Birth weight, g Median [IQR] | 3152.5 [2922–3542] | 3275 [3047–3505] | 0.36 |
| 5-min Apgar score <7 | 2 (5%) | 1 (2.5%) | 1.00 |
| Umbilical artery pH Mean (±SD) | 7.23 ± 0.07 | 7.24 ± 0.08 | 0.44 |
| Umbilical artery BE Mean (±SD) | −4.10 ± 2.11 | −4.89 ± 2.95 | 0.19 |
| Lactates, mmol/L Mean (±SD) | 4.15 ± 1.84 | 4.22 ± 1.59 | 0.87 |
| NCIU Admission | 1 (2.5%) | 2 (5%) | 1.00 |
| Variable | Double Balloon Plus Oxytocine (n = 40) | Vaginal Dinoprostone (n = 40) | p Value |
|---|---|---|---|
| Clinical chorio-amnionitis | 0 | 1 (2.5%) | 1.00 |
| Bacteriological chorioamnionitis | 0 | 3 (7.5%) | 0.24 |
| Histological | 6 (15%) | 5 (12.5%) | 0.56 |
| chorio-amnionitis | |||
| funisitis | 3 | 0 | |
| Postpartum endometritis | 0 | 0 | |
| Materno-fetal infection | |||
| No | 38 (95%) | 39 (97.5%) | 1.00 |
| Probably | 1 (2.5%) | 1 (2.5%) | |
| Confirmed | 1 (2.5%) | 0 |
| Variable | Double Balloon Plus Oxytocine (n = 40) | Vaginal Dinoprostone (n = 40) | p Value |
|---|---|---|---|
| VASPI at insertion device, Mean (±SD) | 4.6 ± 2.8 | 2.9 ± 2.5 | 0.02 |
| Nulliparous | 4.7 ± 2.9 | 3.3 ± 2.6 | 0.07 |
| Parous | 3.6 ± 2.5 | 1.4 ± 1.5 | 0.13 |
| VASPI at H6, Mean (±SD) | 3.8 ± 2.9 | 5.8 ±2.9 | 0.04 |
| Nulliparous | 3.7 ± 2.9 | 5.6 ± 3.0 | 0.08 |
| Parous | 4.4 ± 2.7 | 7.0 ± 0.0 | 0.10 |
| VASPI at H12, Mean (±SD) | 2.5 ± 3.1 | 5.7 ± 2.9 | 0.008 |
| VASPI at H18, Mean (±SD) | 6.2 ± 1.3 | ||
| VASPI at H24, Mean (±SD) | 5.1 ± 4.1 | ||
| Acceptability | |||
| Yes | 37 (92.5%) | 36 (87.5%) | 0.84 |
| No | 3 (7.5%) | 3 (7.5%) | |
| No data | 0 | 1 (2.5%) (il manque 1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Devillard, E.; Petillon, F.; Rouzaire, M.; Pereira, B.; Accoceberry, M.; Houlle, C.; Dejou-Bouillet, L.; Bouchet, P.; Delabaere, A.; Gallot, D. Double Balloon Catheter (Plus Oxytocin) versus Dinoprostone Vaginal Insert for Term Rupture of Membranes: A Randomized Controlled Trial (RUBAPRO). J. Clin. Med. 2022, 11, 1525. https://doi.org/10.3390/jcm11061525
Devillard E, Petillon F, Rouzaire M, Pereira B, Accoceberry M, Houlle C, Dejou-Bouillet L, Bouchet P, Delabaere A, Gallot D. Double Balloon Catheter (Plus Oxytocin) versus Dinoprostone Vaginal Insert for Term Rupture of Membranes: A Randomized Controlled Trial (RUBAPRO). Journal of Clinical Medicine. 2022; 11(6):1525. https://doi.org/10.3390/jcm11061525
Chicago/Turabian StyleDevillard, Eric, Fanny Petillon, Marion Rouzaire, Bruno Pereira, Marie Accoceberry, Céline Houlle, Lydie Dejou-Bouillet, Pamela Bouchet, Amélie Delabaere, and Denis Gallot. 2022. "Double Balloon Catheter (Plus Oxytocin) versus Dinoprostone Vaginal Insert for Term Rupture of Membranes: A Randomized Controlled Trial (RUBAPRO)" Journal of Clinical Medicine 11, no. 6: 1525. https://doi.org/10.3390/jcm11061525
APA StyleDevillard, E., Petillon, F., Rouzaire, M., Pereira, B., Accoceberry, M., Houlle, C., Dejou-Bouillet, L., Bouchet, P., Delabaere, A., & Gallot, D. (2022). Double Balloon Catheter (Plus Oxytocin) versus Dinoprostone Vaginal Insert for Term Rupture of Membranes: A Randomized Controlled Trial (RUBAPRO). Journal of Clinical Medicine, 11(6), 1525. https://doi.org/10.3390/jcm11061525