
Combined Immunotherapy with Chemotherapy versus Bevacizumab with Chemotherapy in First-Line Treatment of Driver-Gene-Negative Non-Squamous Non-Small Cell Lung Cancer: An Updated Systematic Review and Network Meta-Analysis


Abstract
:1. Introduction
2. Material and Methods
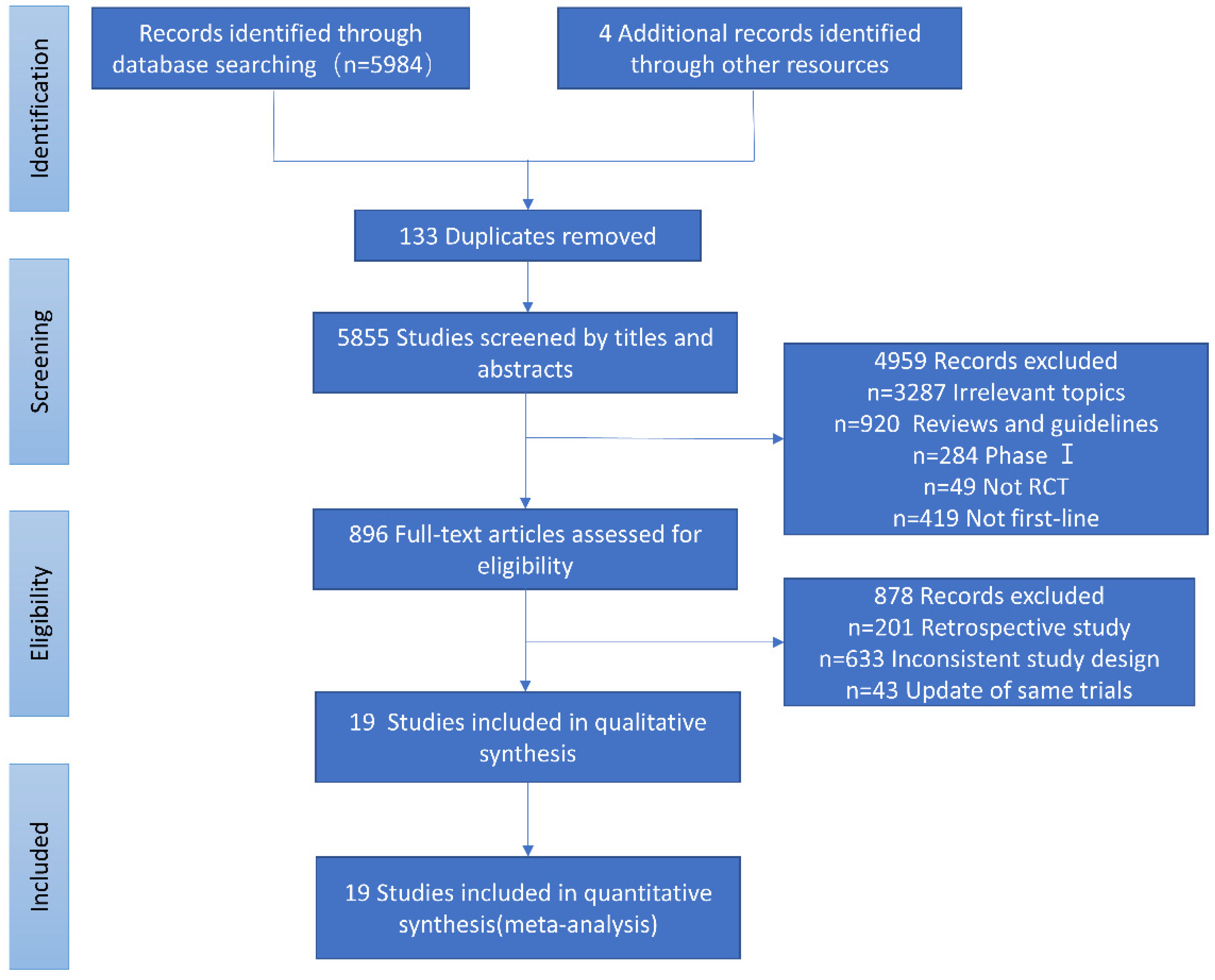
2.1. Literature Search and Selection
2.2. Data Extraction and Quality Assessment
2.3. Statistical Analysis
3. Results
3.1. Eligible Studies
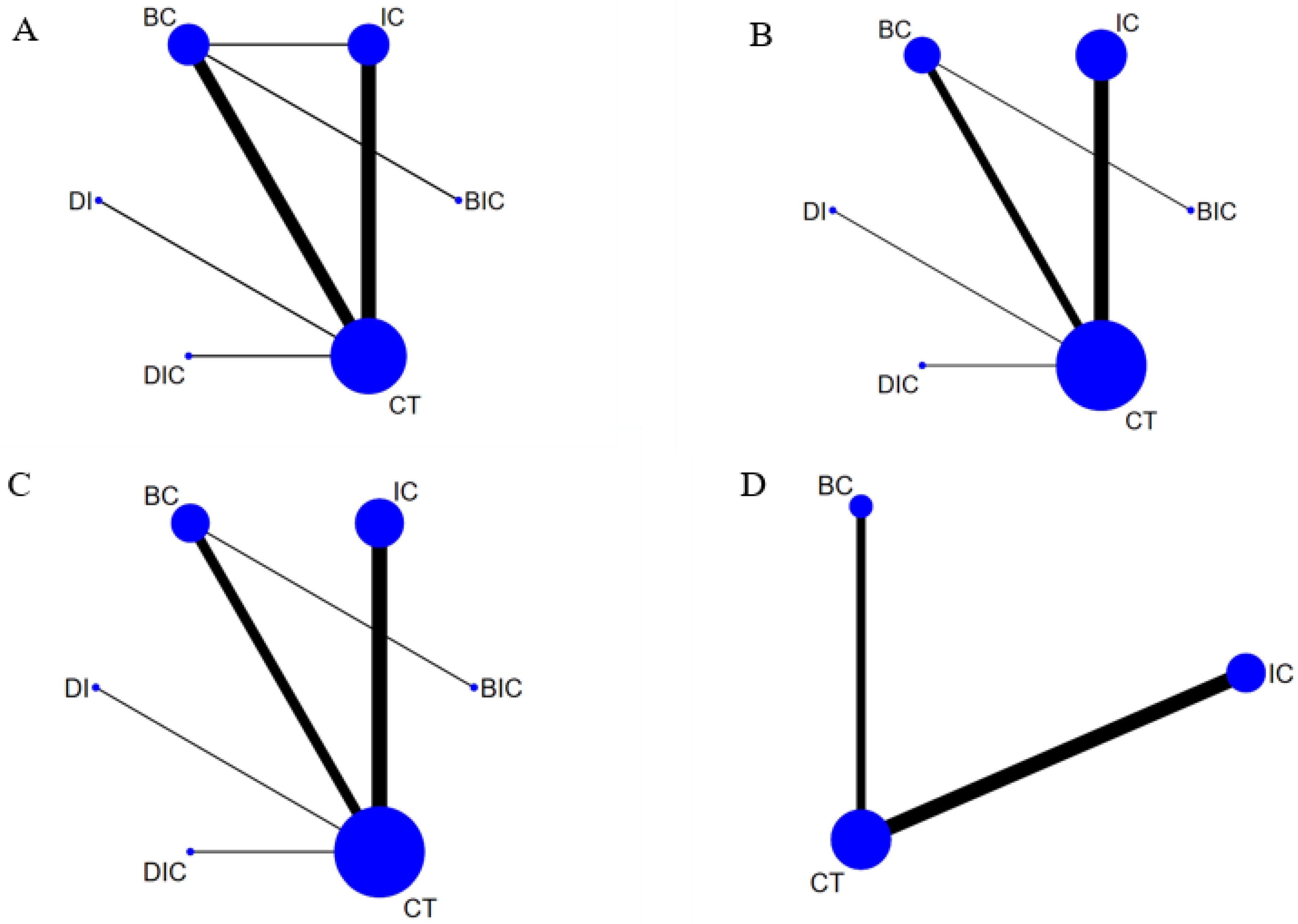
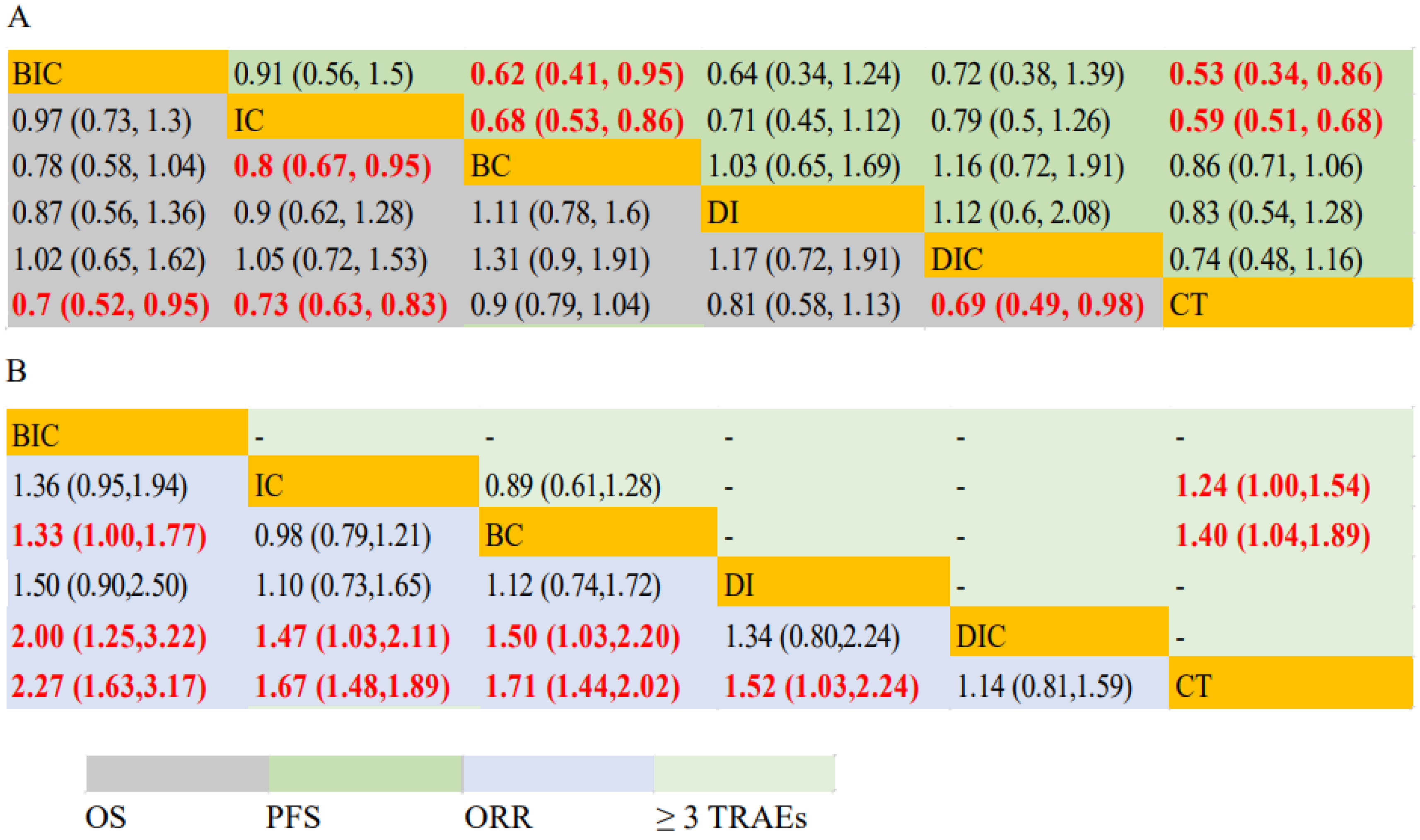
3.2. OS and PFS
3.3. ORR and Safety
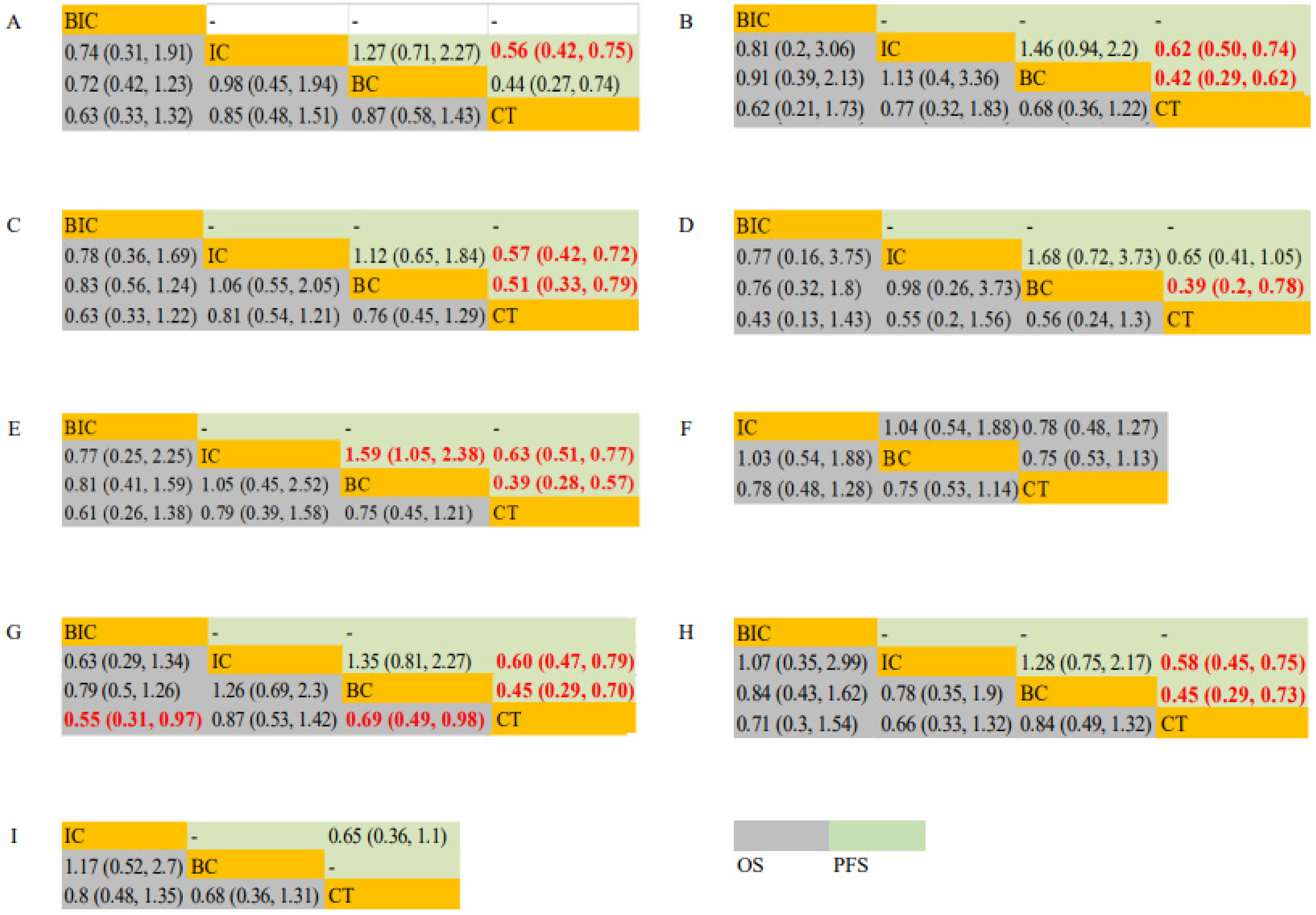
3.4. Subgroups of Various Clinicopathological Characteristics
3.5. Rank Probabilities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Five-Year Outcomes with Pembrolizumab versus Chemotherapy for Metastatic Non–Small-Cell Lung Cancer with PD-L1 Tumor Proportion Score ≥ 50%. J. Clin. Oncol. 2021, 39, 2339–2349. [Google Scholar] [CrossRef]
- Mok, T.S.K.; Wu, Y.-L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Herbst, R.S.; Giaccone, G.; De Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for First-Line Treatment of PD-L1–Selected Patients with NSCLC. N. Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef]
- Sezer, A.; Kilickap, S.; Gümüş, M.; Bondarenko, I.; Özgüroğlu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: A multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet 2021, 397, 592–604. [Google Scholar] [CrossRef]
- Ferrara, N.; Adamis, A.P. Ten years of anti-vascular endothelial growth factor therapy. Nat. Rev. Drug Discov. 2016, 15, 385–403. [Google Scholar] [CrossRef] [Green Version]
- Sul, J.; Blumenthal, G.M.; Jiang, X.; He, K.; Keegan, P.; Pazdur, R. FDA Approval Summary: Pembrolizumab for the Treatment of Patients with Metastatic Non-Small Cell Lung Cancer Whose Tumors Express Programmed Death-Ligand 1. Oncologist 2016, 21, 643–650. [Google Scholar] [CrossRef] [Green Version]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandler, A.; Gray, R.; Perry, M.C.; Brahmer, J.; Schiller, J.H.; Dowlati, A.; Lilenbaum, R.; Johnson, D.H. Paclitaxel–Carboplatin Alone or with Bevacizumab for Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2006, 355, 2542–2550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, C.; Wu, Y.-L.; Chen, G.; Liu, X.; Zhu, Y.; Lu, S.; Feng, J.; He, J.; Han, B.; Wang, J.; et al. BEYOND: A Randomized, Double-Blind, Placebo-Controlled, Multicenter, Phase III Study of First-Line Carboplatin/Paclitaxel Plus Bevacizumab or Placebo in Chinese Patients with Advanced or Recurrent Nonsquamous Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2015, 33, 2197–2204. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; von Pawel, J.; Zatloukal, P.; Ramlau, R.; Gorbounova, V.; Hirsh, V.; Leighl, N.; Mezger, J.; Archer, V.; Moore, N.; et al. Overall survival with cisplatin–gemcitabine and bevacizumab or placebo as first-line therapy for nonsquamous non-small-cell lung cancer: Results from a randomised phase III trial (AVAiL). Ann. Oncol. 2010, 21, 1804–1809. [Google Scholar] [CrossRef]
- Leighl, N.B.; Zatloukal, P.; Mezger, J.; Ramlau, R.; Moore, N.; Reck, M.; Manegold, C. Efficacy and Safety of Bevacizumab-Based Therapy in Elderly Patients with Advanced or Recurrent Nonsquamous Non-small Cell Lung Cancer in the Phase III BO17704 Study (AVAiL). J. Thorac. Oncol. 2010, 5, 1970–1976. [Google Scholar] [CrossRef] [PubMed]
- Niho, S.; Kunitoh, H.; Nokihara, H.; Horai, T.; Ichinose, Y.; Hida, T.; Yamamoto, N.; Kawahara, M.; Shinkai, T.; Nakagawa, K.; et al. Randomized phase II study of first-line carboplatin-paclitaxel with or without bevacizumab in Japanese patients with advanced non-squamous non-small-cell lung cancer. Lung Cancer 2012, 76, 362–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zinner, R.G.; Obasaju, C.K.; Spigel, D.R.; Weaver, R.W.; Beck, J.T.; Waterhouse, D.M.; Modiano, M.R.; Hrinczenko, B.; Nikolinakos, P.G.; Liu, J.; et al. PRONOUNCE: Randomized, Open-Label, Phase III Study of First-Line Pemetrexed + Carboplatin Followed by Maintenance Pemetrexed versus Paclitaxel + Carboplatin + Bevacizumab Followed by Maintenance Bevacizumab in Patients ith Advanced Nonsquamous Non–Small-Cell Lung Cancer. J. Thorac. Oncol. 2015, 10, 134–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galetta, D.; Cinieri, S.; Pisconti, S.; Gebbia, V.; Morabito, A.; Borsellino, N.; Maiello, E.; Febbraro, A.; Catino, A.; Rizzo, P.; et al. Cisplatin/Pemetrexed Followed by Maintenance Pemetrexed versus Carboplatin/Paclitaxel/Bevacizumab Followed by Maintenance Bevacizumab in Advanced Nonsquamous Lung Cancer: The GOIM (Gruppo Oncologico Italia Meridionale) ERACLE Phase III Randomized Trial. Clin. Lung Cancer 2015, 16, 262–273. [Google Scholar] [CrossRef]
- Sheng, L.; Gao, J.; Xu, Q.; Zhang, X.; Huang, M.; Dai, X.; Li, S.; Liu, L. Selection of optimal first-line immuno-related therapy based on specific pathological characteristics for patients with advanced driver-gene wild-type non-small cell lung cancer: A systematic review and network meta-analysis. Ther. Adv. Med Oncol. 2021, 13, 17588359211018537. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Zhang, X.; Huang, M.; Dai, X.; Gao, J.; Li, S.; Sheng, L.; Huang, K.; Wang, J.; Liu, L. Comparison of Efficacy and Safety of Single and Double Immune Checkpoint Inhibitor-Based First-Line Treatments for Advanced Driver-Gene Wild-Type Non-Small Cell Lung Cancer: A Systematic Review and Network Meta-Analysis. Front. Immunol. 2021, 12, 731546. [Google Scholar] [CrossRef]
- Paz-Ares, L.G.; Ramalingam, S.S.; Ciuleanu, T.-E.; Lee, J.-S.; Urban, L.; Caro, R.B.; Park, K.; Sakai, H.; Ohe, Y.; Nishio, M.; et al. First-Line Nivolumab Plus Ipilimumab in Advanced NSCLC: 4-Year Outcomes From the Randomized, Open-Label, Phase 3 CheckMate 227 Part 1 Trial. J. Thorac. Oncol. 2021, 17, 289–308. [Google Scholar] [CrossRef] [PubMed]
- Awad, M.M.; Gadgeel, S.M.; Borghaei, H.; Patnaik, A.; Yang, J.C.-H.; Powell, S.F.; Gentzler, R.D.; Martins, R.G.; Stevenson, J.P.; Altan, M.; et al. Long-Term Overall Survival From KEYNOTE-021 Cohort G: Pemetrexed and Carboplatin with or without Pembrolizumab as First-Line Therapy for Advanced Nonsquamous NSCLC. J. Thorac. Oncol. 2020, 16, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Gadgeel, S.; Rodríguez-Abreu, D.; Speranza, G.; Esteban, E.; Felip, E.; Dómine, M.; Hui, R.; Hochmair, M.J.; Clingan, P.; Powell, S.F.; et al. Updated Analysis from KEYNOTE-189: Pembrolizumab or Placebo Plus Pemetrexed and Platinum for Previously Untreated Metastatic Nonsquamous Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2020, 38, 1505–1517. [Google Scholar] [CrossRef]
- Zhou, C.; Chen, G.; Huang, Y.; Zhou, J.; Lin, L.; Feng, J.; Wang, Z.; Shu, Y.; Shi, J.; Hu, Y.; et al. Camrelizumab plus carboplatin and pemetrexed versus chemotherapy alone in chemotherapy-naive patients with advanced non-squamous non-small-cell lung cancer (CameL): A randomised, open-label, multicentre, phase 3 trial. Lancet Respir. Med. 2021, 9, 305–314. [Google Scholar] [CrossRef]
- Yang, Y.; Sun, J.; Wang, Z.; Fang, J.; Yu, Q.; Han, B.; Cang, S.; Chen, G.; Mei, X.; Yang, Z.; et al. Updated Overall Survival Data and Predictive Biomarkers of Sintilimab Plus Pemetrexed and Platinum as First-Line Treatment for Locally Advanced or Metastatic Nonsquamous NSCLC in the Phase 3 ORIENT-11 Study. J. Thorac. Oncol. 2021, 16, 2109–2120. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Wang, Z.; Fang, J.; Yu, Q.; Han, B.; Cang, S.; Chen, G.; Mei, X.; Yang, Z.; Ma, R.; et al. Efficacy and Safety of Sintilimab Plus Pemetrexed and Platinum as First-Line Treatment for Locally Advanced or Metastatic Nonsquamous NSCLC: A Randomized, Double-Blind, Phase 3 Study (Oncology pRogram by InnovENT anti-PD-1-11). J. Thorac. Oncol. 2020, 15, 1636–1646. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lu, S.; Yu, X.; Hu, Y.; Sun, Y.; Wang, Z.; Zhao, J.; Yu, Y.; Hu, C.; Yang, K.; et al. Tislelizumab Plus Chemotherapy vs. Chemotherapy Alone as First-line Treatment for Advanced Squamous Non-Small-Cell Lung Cancer: A Phase 3 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef] [PubMed]
- West, H.; McCleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, H.J.; Kopp, H.-G.; Daniel, D.; McCune, S.; Mekhail, T.; et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef]
- Zhou, C.; Wang, Z.; Sun, Y.; Cao, L.; Ma, Z.; Wu, R.; Yu, Y.; Yao, W.; Wang, H.; Chen, J.; et al. MA13.07 GEMSTONE-302: A Phase 3 Study of Platinum-Based Chemotherapy with Placebo or Sugemalimab, a PD-L1 mAb, for metastatic NSCLC. J. Thorac. Oncol. 2021, 16, S926–S927. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.-E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): An international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.E.; Yu, X.; Salman, P.; Pluzanski, A.; Nagrial, A.; Havel, L.; Kowalyszyn, R.; Audigier-Valette, C.; Wu, Y.-L.; et al. Nivolumab (NIVO) plus platinum-doublet chemotherapy (chemo) vs. chemo as first-line (1L) treatment (tx) for advanced non-small cell lung cancer (aNSCLC): CheckMate 227-part 2 final analysis. Ann. Oncol. 2019, 30, 67–68. [Google Scholar]
- Rizvi, N.A.; Cho, B.C.; Reinmuth, N.; Lee, K.H.; Luft, A.; Ahn, M.J.; van den Heuvel, M.M.; Cobo, M.; Vicente, D.; Smolin, A.; et al. Durvalumab with or without Tremelimumab vs. Standard Chemotherapy in First-line Treatment of Metastatic Non-Small Cell Lung Cancer: The MYSTIC Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 661–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Wang, Z.; Wu, L.; Li, B.; Cheng, Y.; Li, X.; Wang, X.; Han, L.; Wu, X.; Fan, Y.; et al. MA13.08 CHOICE-01: A Phase 3 Study of Toripalimab versus Placebo in Combination with First-Line Chemotherapy for Advanced NSCLC. J. Thorac. Oncol. 2021, 16, S927–S928. [Google Scholar] [CrossRef]
- Gogishvili, M.; Melkadze, T.; Makharadze, T.; Giorgadze, D.; Dvorkin, M.; Penkov, K.; Laktionov, K.; Nemsadze, G.; Nechaeva, M.; Rozhkova, I.; et al. LBA51 EMPOWER-Lung 3: Cemiplimab in combination with platinum doublet chemotherapy for first-line (1L) treatment of advanced non-small cell lung cancer (NSCLC). Ann. Oncol. 2021, 32, S1328. [Google Scholar] [CrossRef]
- Johnson, M.; Cho, B.C.; Luft, A.; Alatorre-Alexander, J.; Geater, S.L.; Laktionov, K.; Vasiliev, A.; Trukhin, D.; Kim, S.; Ursol, G.; et al. Durvalumab +/− Tremelimumab plus Chemotherapy as First-line Treatment for mNSCLC: Results from the Phase 3 POSEIDON Study. J. Thorac. Oncol. 2021, 16, S844. [Google Scholar] [CrossRef]
- Socinski, M.A.; Nishio, M.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; et al. IMpower150 Final Overall Survival Analyses for Atezolizumab Plus Bevacizumab and Chemotherapy in First-Line Metastatic Nonsquamous NSCLC. J. Thorac. Oncol. 2021, 16, 1909–1924. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NCT Identifier Number | Published Year | First Author | Phase | Arm | Non-Squamous Patients with Survival Data | HR OS (95% CIs) | HR PFS (95% CIs) | ORR (n/N *) | ≥3 TRAEs (n/N *) | |
|---|---|---|---|---|---|---|---|---|---|---|
| ECOG4599 | NCT00021060 | 2006 | Sandler A, et al. | III | BCP | 417 | 0.79 (0.67 to 0.92) | 0.66 (0.57 to 0.77) | 133/381 | 251/427 |
| CP | 433 | - | - | 59/392 | 104/440 | |||||
| AVAiL | NCT00806923 | 2010 | Reck M, et al. | III | BCG | 351 | 1.03 (0.86 to 1.23) | 0.85 (0.73 to 1.00) | 121/351 | 274/329 |
| CG | 347 | - | - | 75/347 | 252/326 | |||||
| JO19907 | CTI-060338 | 2012 | Niho S, et al. | II | BCP | 117 | 0.99 (0.65 to 1.50) | 0.61 (0.42 to 0.89) | 71/121 | NA |
| CP | 58 | - | - | 18/58 | NA | |||||
| PRONOUNCE | NCT00948675 | 2015 | Zinner RG, et al. | III | BCP | 182 | 1.07 (0.83 to 1.36) | 1.06 (0.84 to 1.35) | 49/179 | NA |
| Pem + Cb | 179 | - | - | 43/182 | NA | |||||
| BEYOND | NCT01364012 | 2015 | Zhou C, et al. | III | BCP | 138 | 0.68 (0.50 to 0.93) | 0.40 (0.29 to 0.54) | 75/138 | 94/140 |
| CP | 138 | - | - | 36/138 | 83/134 | |||||
| ERACLE | NCT01303926 | 2015 | Galetta D, et al. | III | Cisplatin/Pemetrexed | 60 | 0.93 (0.60 to 1.42) | 0.79 (0.53 to 1.17) | 24/60 | 6/58 |
| BCP | 58 | - | - | 30/58 | 5/60 | |||||
| KEYNOTE-021G | NCT02039674 | 2016 | Langer C, et al. | II | Pembrolizumab + Pem + Cb | 60 | 0.71 (0.45 to 1.12) | 0.54 (0.35 to 0.83) | 35/60 | 23/60 |
| Pem + Cb | 63 | - | - | 21/63 | 20/63 | |||||
| IMpower130 | NCT02367781 | 2019 | West H, et al. | III | Atezolizumab + Nab-paclitaxel + carboplatin | 451 | 0.79 (0.64 to 0.98) | 0.64 (0.54 to 0.77) | 220/447 | 381/473 |
| Nab-paclitaxel+ carboplatin | 228 | - | - | 72/226 | 164/232 | |||||
| KEYNOTE-189 | NCT02578680 | 2020 | Gadgeel S, et al. | III | Pembrolizumab + Pemetrexed + Platinum | 410 | 0.56 (0.45 to 0.70) | 0.48 (0.40 to 0.58) | 197/410 | 291/410 |
| Pemetrexed + Platinum | 206 | - | - | 40/206 | 135/206 | |||||
| CheckMate 227 4year part1A i | NCT02477826 | 2020 | Hellmann MD, et al. | III | Nivolumab + Ipilimumab | 278 | 0.81 (0.67 to 0.99) | 0.83 (0.68 to 1.01) | 103/278 | NA |
| Chemotherapy | 279 | - | - | 91/279 | NA | |||||
| CheckMate 227 4year part1B ii | NCT02477826 | 2020 | Hellmann MD, et al. | III | Nivolumab + Ipilimumab | 134 | 0.69 (0.53 to 0.89) | 0.66 (0.51 to 0.87) | 53/134 | NA |
| Chemotherapy | 140 | - | - | 30/140 | NA | |||||
| CheckMate 227 4year part2 iii | NCT02477826 | 2020 | Hellmann MD, et al. | III | Nivolumab + chemotherapy | 270 | 0.69 (0.50 to 0.97) | 0.69 (0.50 to 0.97) | 130/270 | NA |
| Chemotherapy | 273 | - | - | 80/273 | NA | |||||
| IMpower132 | NCT02657434 | 2021 | Nishio M, et al. | III | APP | 292 | 0.86 (0.71 to 1.06) | 0.60 (0.49 to 0.72) | 137/292 | 159/292 |
| PP | 286 | - | - | 92/286 | 115/286 | |||||
| IMpower150 4 year update | NCT02366143 | 2021 | Socinski MA, et al. | III | ABCP | 350 | 0.80 (0.67 to 0.95) iv | 0.62 (0.52 to 0.74) | 224/350 | NA |
| ACP | 359 | 0.84(0.71 to 1.00) v | NA | NA | NA | |||||
| BCP | 338 | - | - | 159/331 | NA | |||||
| CheckMate 9LA 2-year update | NCT03215706 | 2021 | Reck M, et al. | III | Nivolumab + ipilimumab + platinum-doublet Chemotherapy | 248 | 0.69 (0.55 to 0.87) | 0.74 (0.60 to 0.92) | 82/246 | NA |
| Chemotherapy | 247 | - | - | 54/246 | NA | |||||
| CameL | NCT03134872 | 2021 | Zhou, et al. | III | Camrelizumab + Pem + Cb | 205 | 0.73 (0.53 to 1.02) | 0.60 (0.45 to 0.79) | 123/205 | NA |
| Pem + Cb | 207 | - | - | 81/207 | NA | |||||
| RATIONALE 304 | NCT03663205 | 2021 | Lu S, et al. | III | Tislelizumab + chemotherapy | 222 | NA | 0.645 (0.46 to 0.902) | 128/223 | 141/205 |
| Chemotherapy | 110 | - | - | 41/111 | 97/207 | |||||
| ORIENT 11 | NCT03607539 | 2021 | Yang Y, et al. | III | Sintilimab + pemetrexed + platinum | 266 | NA | 0.49 (0.38 to 0.63) | 138/266 | 74/223 |
| Pemetrexed + platinum | 131 | - | - | 39/131 | 23/111 | |||||
| GEMSTONE-302 | NCT03789604 | 2021 | Zhou C, et al. | III | Sugemalimab + platinum-based chemotherapy | 191 | NA | 0.59 (0.45 to 0.79) | NA | NA |
| Platinum-based chemotherapy | 96 | NA | - | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chai, Y.; Wu, X.; Bai, H.; Duan, J. Combined Immunotherapy with Chemotherapy versus Bevacizumab with Chemotherapy in First-Line Treatment of Driver-Gene-Negative Non-Squamous Non-Small Cell Lung Cancer: An Updated Systematic Review and Network Meta-Analysis. J. Clin. Med. 2022, 11, 1655. https://doi.org/10.3390/jcm11061655
Chai Y, Wu X, Bai H, Duan J. Combined Immunotherapy with Chemotherapy versus Bevacizumab with Chemotherapy in First-Line Treatment of Driver-Gene-Negative Non-Squamous Non-Small Cell Lung Cancer: An Updated Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine. 2022; 11(6):1655. https://doi.org/10.3390/jcm11061655
Chicago/Turabian StyleChai, Yue, Xinyu Wu, Hua Bai, and Jianchun Duan. 2022. "Combined Immunotherapy with Chemotherapy versus Bevacizumab with Chemotherapy in First-Line Treatment of Driver-Gene-Negative Non-Squamous Non-Small Cell Lung Cancer: An Updated Systematic Review and Network Meta-Analysis" Journal of Clinical Medicine 11, no. 6: 1655. https://doi.org/10.3390/jcm11061655
APA StyleChai, Y., Wu, X., Bai, H., & Duan, J. (2022). Combined Immunotherapy with Chemotherapy versus Bevacizumab with Chemotherapy in First-Line Treatment of Driver-Gene-Negative Non-Squamous Non-Small Cell Lung Cancer: An Updated Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine, 11(6), 1655. https://doi.org/10.3390/jcm11061655