
Aberrant Structural Connectivity of the Triple Network System in Borderline Personality Disorder Is Associated with Behavioral Dysregulation

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. MRI Acquisition
2.3. MRI Preprocessing
2.3.1. Diffusion Tensor Images (DTI) Analysis
2.3.2. Structural 3D T1-Weighted Images Analysis
3. Statistical Analysis
4. Results
4.1. Demographical and Clinical Features of Participants
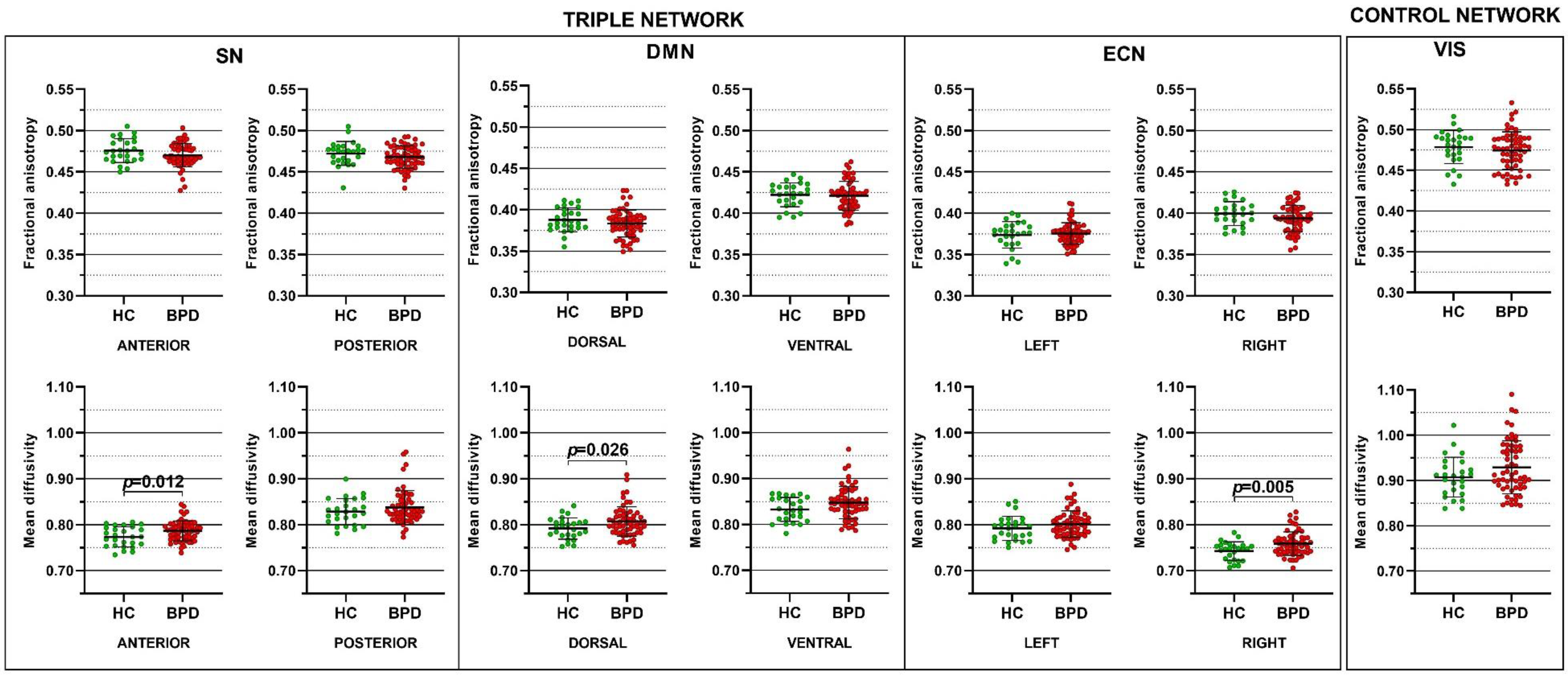
4.2. Mean Diffusivity Is Increased in the Triple Network System of BPD
4.3. WM Alterations Are Associated with Behavioral Dysregulation in BPD
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Menon, V. Large-scale brain networks and psychopathology: A unifying triple network model. Trends Cogn. Sci. 2011, 15, 483–506. [Google Scholar] [CrossRef] [PubMed]
- Doll, A.; Sorg, C.; Manoliu, A.; Meng, C.; Wöller, A.; Förstl, H.; Zimmer, C.; Wohlschläger, A.; Riedl, V. Shifted intrinsic connectivity of central executive and salience network in borderline personality disorder. Front. Hum. Neurosci. 2013, 7, 727. [Google Scholar] [CrossRef] [PubMed]
- Quattrini, G.; Pini, L.; Pievani, M.; Magni, L.R.; Lanfredi, M.; Ferrari, C.; Boccardi, M.; Bignotti, S.; Magnaldi, S.; Cobelli, M.; et al. Abnormalities in functional connectivity in borderline personality disorder: Correlations with metacognition and emotion dysregulation. Psychiatry Res. Neuroimaging 2019, 283, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Denny, B.T.; Fan, J.; Fels, S.; Galitzer, H.; Schiller, D.; Koenigsberg, H.W. Sensitization of the neural salience network to repeated emotional stimuli following initial habituation in patients with borderline personality disorder. Am. J. Psychiatry 2018, 175, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Sarkheil, P.; Ibrahim, C.N.; Schneider, F.; Mathiak, K.; Klasen, M. Aberrant functional connectivity profiles of brain regions associated with salience and reward processing in female patients with borderline personality disorder. Brain Imaging Behav. 2020, 14, 485–495. [Google Scholar] [CrossRef]
- Krauch, M.; Ueltzhöffer, K.; Brunner, R.; Kaess, M.; Hensel, S.; Herpertz, S.C.; Bertsch, K. Heightened Salience of Anger and Aggression in Female Adolescents with Borderline Personality Disorder—A Script-Based fMRI Study. Front. Behav. Neurosci. 2018, 12, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orth, L.; Zweerings, J.; Ibrahim, C.N.; Neuner, I.; Sarkheil, P. Altered functional connectivity during evaluation of self-relevance in women with borderline personality disorder. NeuroImage Clin. 2020, 27, 102324. [Google Scholar] [CrossRef] [PubMed]
- Malejko, K.; Neff, D.; Brown, R.C.; Plener, P.L.; Bonenberger, M.; Abler, B.; Graf, H. Neural signatures of social inclusion in borderline personality disorder versus non-suicidal self-injury. Brain Topogr. 2019, 32, 753–761. [Google Scholar] [CrossRef]
- Sampedro, F.; Aracil-Bolanos, I.; Carmona, I.; Farres, C.; Soler, J.; Schmidt, C.; Elices, M.; Pomarol-Clotet, E.; Salvador, R.; Vega, D.; et al. A Functional Connectivity Study to Investigate the Role of the Right Anterior Insula in Modulating Emotional Dysfunction in Borderline Personality Disorder. Psychosom. Med. 2022, 84, 64–73. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, A.; D’Souza, A.; Samson, A.C.; Carballedo, A.; Kerskens, C.; Frodl, T. Dysregulation between emotion and theory of mind networks in borderline personality disorder. Psychiatry Res. Neuroimaging 2015, 231, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Kluetsch, R.C.; Schmahl, C.; Niedtfeld, I.; Densmore, M.; Calhoun, V.D.; Daniels, J.; Kraus, A.; Ludaescher, P.; Bohus, M.; Lanius, R.A. Alterations in default mode network connectivity during pain processing in borderline personality disorder. Arch. Gen. Psychiatry 2012, 69, 993–1002. [Google Scholar] [CrossRef]
- Visintin, E.; De Panfilis, C.; Amore, M.; Balestrieri, M.; Wolf, R.C.; Sambataro, F. Mapping the brain correlates of borderline personality disorder: A functional neuroimaging meta-analysis of resting state studies. J. Affect. Disord. 2016, 204, 262–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soloff, P.H.; Abraham, K.; Ramaseshan, K.; Burgess, A.; Diwadkar, V.A. Hyper-modulation of brain networks by the amygdala among women with Borderline Personality Disorder: Network signatures of affective interference during cognitive processing. J. Psychiatr. Res. 2017, 88, 56–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wrege, J.; Carcone, D.; Lee, A.; Cane, C.; Lang, U.; Borgwardt, S.; Walter, M.; Ruocco, A. Attentional salience and the neural substrates of response inhibition in borderline personality disorder. Psychol. Med. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Van Den Heuvel, M.P.; Mandl, R.C.; Kahn, R.S.; Hulshoff Pol, H.E. Functionally linked resting-state networks reflect the underlying structural connectivity architecture of the human brain. Hum. Brain Mapp. 2009, 30, 3127–3141. [Google Scholar] [CrossRef] [PubMed]
- Straathof, M.; Sinke, M.R.; Dijkhuizen, R.M.; Otte, W.M. A systematic review on the quantitative relationship between structural and functional network connectivity strength in mammalian brains. J. Cereb. Blood Flow Metab. 2019, 39, 189–209. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Friston, K. Structural and functional brain networks: From connections to cognition. Science 2013, 342, 1238411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Bihan, D. Diffusion MRI: What water tells us about the brain. EMBO Mol. Med. 2014, 6, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.L.; Lee, J.E.; Lazar, M.; Field, A.S. Diffusion tensor imaging of the brain. Neurotherapeutics 2007, 4, 316–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lope-Piedrafita, S. Diffusion Tensor Imaging (DTI); Preclinical MRI; Springer: Berlin/Heidelberg, Germany, 2018; pp. 103–116. [Google Scholar]
- Grant, J.E.; Correia, S.; Brennan-Krohn, T.; Malloy, P.F.; Laidlaw, D.H.; Schulz, S.C. Frontal white matter integrity in borderline personality disorder with self-injurious behavior. J. Neuropsychiatry Clin. Neurosci. 2007, 19, 383–390. [Google Scholar] [CrossRef]
- Rüsch, N.; Weber, M.; Il’yasov, K.A.; Lieb, K.; Ebert, D.; Hennig, J.; van Elst, L.T. Inferior frontal white matter microstructure and patterns of psychopathology in women with borderline personality disorder and comorbid attention-deficit hyperactivity disorder. Neuroimage 2007, 35, 738–747. [Google Scholar] [CrossRef] [PubMed]
- Carrasco, J.L.; Tajima-Pozo, K.; Díaz-Marsá, M.; Casado, A.; López-Ibor, J.J.; Arrazola, J.; Yus, M. Microstructural white matter damage at orbitofrontal areas in borderline personality disorder. J. Affect. Disord. 2012, 139, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Gan, J.; Yi, J.; Zhong, M.; Cao, X.; Jin, X.; Liu, W.; Zhu, X. Abnormal white matter structural connectivity in treatment-naïve young adults with borderline personality disorder. Acta Psychiatr. Scand. 2016, 134, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Whalley, H.C.; Nickson, T.; Pope, M.; Nicol, K.; Romaniuk, L.; Bastin, M.E.; Semple, S.I.; McIntosh, A.M.; Hall, J. White matter integrity and its association with affective and interpersonal symptoms in borderline personality disorder. NeuroImage Clin. 2015, 7, 476–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lischke, A.; Domin, M.; Freyberger, H.J.; Grabe, H.J.; Mentel, R.; Bernheim, D.; Lotze, M. Structural alterations in the corpus callosum are associated with suicidal behavior in women with borderline personality disorder. Front. Hum. Neurosci. 2017, 11, 196. [Google Scholar] [CrossRef] [PubMed]
- Quattrini, G.; Marizzoni, M.; Magni, L.R.; Magnaldi, S.; Lanfredi, M.; Rossi, G.; Frisoni, G.B.; Pievani, M.; Rossi, R. Whole-brain microstructural white matter alterations in borderline personality disorder patients. Personal. Ment. Health 2019, 13, 96–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ninomiya, T.; Oshita, H.; Kawano, Y.; Goto, C.; Matsuhashi, M.; Masuda, K.; Takita, F.; Izumi, T.; Inoue, A.; Higuma, H.; et al. Reduced white matter integrity in borderline personality disorder: A diffusion tensor imaging study. J. Affect. Disord. 2018, 225, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Grottaroli, M.; Delvecchio, G.; Bressi, C.; Moltrasio, C.; Soares, J.; Brambilla, P. Microstructural white matter alterations in borderline personality disorder: A minireview. J. Affect. Disord. 2020, 264, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Vandekerckhove, M.; Berens, A.; Wang, Y.; Quirin, M.; De Mey, J. Alterations in the fronto-limbic network and corpus callosum in borderline-personality disorder. Brain Cogn. 2020, 138, 103596. [Google Scholar] [CrossRef]
- Lei, X.; Zhong, M.; Zhang, B.; Yang, H.; Peng, W.; Liu, Q.; Zhang, Y.; Yao, S.; Tan, C.; Yi, J. Structural and functional connectivity of the anterior cingulate cortex in patients with borderline personality disorder. Front. Neurosci. 2019, 13, 971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossi, R.; Pievani, M.; Lorenzi, M.; Boccardi, M.; Beneduce, R.; Bignotti, S.; Borsci, G.; Cotelli, M.; Giannakopoulos, P.; Magni, L.R.; et al. Structural brain features of borderline personality and bipolar disorders. Psychiatry Res. Neuroimaging 2013, 213, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Sampedro, F.; Carmona I Farrés, C.; Soler, J.; Elices, M.; Schmidt, C.; Corripio, I.; Domínguez-Clavé, E.; Pomarol-Clotet, E.; Salvador, R.; Pascual, J.C. Structural brain abnormalities in borderline personality disorder correlate with clinical severity and predict psychotherapy response. Brain Imaging Behav. 2021, 15, 2502–2512. [Google Scholar] [CrossRef] [PubMed]
- Bøen, E.; Westlye, L.; Elvsåshagen, T.; Hummelen, B.; Hol, P.; Boye, B.; Andersson, S.; Karterud, S.; Malt, U. Regional cortical thinning may be a biological marker for borderline personality disorder. Acta Psychiatr. Scand. 2014, 130, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Soloff, P.H.; Pruitt, P.; Sharma, M.; Radwan, J.; White, R.; Diwadkar, V.A. Structural brain abnormalities and suicidal behavior in borderline personality disorder. J. Psychiatr. Res. 2012, 46, 516–525. [Google Scholar] [CrossRef] [Green Version]
- Depping, M.S.; Wolf, N.D.; Vasic, N.; Sambataro, F.; Thomann, P.A.; Wolf, R.C. Common and distinct structural network abnormalities in major depressive disorder and borderline personality disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2016, 65, 127–133. [Google Scholar] [CrossRef]
- Magni, L.R.; Carcione, A.; Ferrari, C.; Semerari, A.; Riccardi, I.; Lanfredi, M.; Pedrini, L.; Cotelli, M.; Bocchio, L.; Pievani, M.; et al. CLIMAMITHE Study group Neurobiological and clinical effect of metacognitive interpersonal therapy vs structured clinical model: Study protocol for a randomized controlled trial. BMC Psychiatry 2019, 19, 195. [Google Scholar] [CrossRef] [Green Version]
- Andersson, J.L.; Skare, S.; Ashburner, J. How to correct susceptibility distortions in spin-echo echo-planar images: Application to diffusion tensor imaging. Neuroimage 2003, 20, 870–888. [Google Scholar] [CrossRef]
- Andersson, J.L.; Sotiropoulos, S.N. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage 2016, 125, 1063–1078. [Google Scholar] [CrossRef] [Green Version]
- Figley, T.D.; Bhullar, N.; Courtney, S.M.; Figley, C.R. Probabilistic atlases of default mode, executive control and salience network white matter tracts: An fMRI-guided diffusion tensor imaging and tractography study. Front. Hum. Neurosci. 2015, 9, 585. [Google Scholar] [CrossRef] [Green Version]
- Figley, T.D.; Mortazavi Moghadam, B.; Bhullar, N.; Kornelsen, J.; Courtney, S.M.; Figley, C.R. Probabilistic white matter atlases of human auditory, basal ganglia, language, precuneus, sensorimotor, visual and visuospatial networks. Front. Hum. Neurosci. 2017, 11, 306. [Google Scholar] [CrossRef]
- Smith, S.M.; Jenkinson, M.; Johansen-Berg, H.; Rueckert, D.; Nichols, T.E.; Mackay, C.E.; Watkins, K.E.; Ciccarelli, O.; Cader, M.Z.; Matthews, P.M.; et al. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. Neuroimage 2006, 31, 1487–1505. [Google Scholar] [CrossRef] [PubMed]
- Andersson, J.L.; Jenkinson, M.; Smith, S. Non-linear registration, aka Spatial normalisation FMRIB technical report TR07JA2. FMRIB Anal. Group Univ. Oxf. 2007, 2, 1–21. [Google Scholar]
- Jenkinson, M.; Smith, S. A global optimisation method for robust affine registration of brain images. Med. Image Anal. 2001, 5, 143–156. [Google Scholar] [CrossRef]
- Backhausen, L.L.; Herting, M.M.; Buse, J.; Roessner, V.; Smolka, M.N.; Vetter, N.C. Quality control of structural MRI images applied using FreeSurfer—A hands-on workflow to rate motion artifacts. Front. Neurosci. 2016, 10, 558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischl, B.; Dale, A.M. Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc. Natl. Acad. Sci. USA 2000, 97, 11050–11055. [Google Scholar] [CrossRef] [Green Version]
- Thomas Yeo, B.; Krienen, F.M.; Sepulcre, J.; Sabuncu, M.R.; Lashkari, D.; Hollinshead, M.; Roffman, J.L.; Smoller, J.W.; Zöllei, L.; Polimeni, J.R.; et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J. Neurophysiol. 2011, 106, 1125–1165. [Google Scholar] [CrossRef] [PubMed]
- Lebel, C.; Deoni, S. The development of brain white matter microstructure. Neuroimage 2018, 182, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Khundrakpam, B.S.; Lewis, J.D.; Zhao, L.; Chouinard-Decorte, F.; Evans, A.C. Brain connectivity in normally developing children and adolescents. Neuroimage 2016, 134, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, J.E.; Grohs, M.N.; Dewey, D.; Lebel, C. Global and regional white matter development in early childhood. Neuroimage 2019, 196, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Lisoni, J.; Miotto, P.; Barlati, S.; Calza, S.; Crescini, A.; Deste, G.; Sacchetti, E.; Vita, A. Change in core symptoms of borderline personality disorder by tDCS: A pilot study. Psychiatry Res. 2020, 291, 113261. [Google Scholar] [CrossRef] [PubMed]
- Wolkenstein, L.; Rombold-Bruehl, F.; Bingmann, T.; Sommer, A.; Kanske, P.; Plewnia, C. Challenging control over emotions in borderline personality disorder-a tDCS study. Neuropsychologia 2021, 156, 107850. [Google Scholar] [CrossRef] [PubMed]
- Molavi, P.; Aziziaram, S.; Basharpoor, S.; Atadokht, A.; Nitsche, M.A.; Salehinejad, M.A. Repeated transcranial direct current stimulation of dorsolateral-prefrontal cortex improves executive functions, cognitive reappraisal emotion regulation, and control over emotional processing in borderline personality disorder: A randomized, sham-controlled, parallel-group study. J. Affect. Disord. 2020, 274, 93–102. [Google Scholar] [PubMed]
- Schulze, L.; Grove, M.; Tamm, S.; Renneberg, B.; Roepke, S. Effects of transcranial direct current stimulation on the cognitive control of negative stimuli in borderline personality disorder. Sci. Rep. 2019, 9, 332. [Google Scholar] [CrossRef] [Green Version]
- Miniussi, C.; Harris, J.A.; Ruzzoli, M. Modelling non-invasive brain stimulation in cognitive neuroscience. Neurosci. Biobehav. Rev. 2013, 37, 1702–1712. [Google Scholar] [CrossRef] [Green Version]
- Boisseau, C.L.; Yen, S.; Markowitz, J.C.; Grilo, C.M.; Sanislow, C.A.; Shea, M.T.; Zanarini, M.C.; Skodol, A.E.; Gunderson, J.G.; Morey, L.C.; et al. Individuals with single versus multiple suicide attempts over 10 years of prospective follow-up. Compr. Psychiatry 2013, 54, 238–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yen, S.; Shea, M.T.; Sanislow, C.A.; Grilo, C.M.; Skodol, A.E.; Gunderson, J.G.; McGlashan, T.H.; Zanarini, M.C.; Morey, L.C. Borderline personality disorder criteria associated with prospectively observed suicidal behavior. Am. J. Psychiatry 2004, 161, 1296–1298. [Google Scholar] [CrossRef] [PubMed]
- Terzi, L.; Martino, F.; Berardi, D.; Bortolotti, B.; Sasdelli, A.; Menchetti, M. Aggressive behavior and self-harm in borderline personality disorder: The role of impulsivity and emotion dysregulation in a sample of outpatients. Psychiatry Res. 2017, 249, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Seeley, W.W.; Menon, V.; Schatzberg, A.F.; Keller, J.; Glover, G.H.; Kenna, H.; Reiss, A.L.; Greicius, M.D. Dissociable intrinsic connectivity networks for salience processing and executive control. J. Neurosci. 2007, 27, 2349–2356. [Google Scholar] [CrossRef] [PubMed]
- Menon, V.; Uddin, L.Q. Saliency, switching, attention and control: A network model of insula function. Brain Struct. Funct. 2010, 214, 655–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domes, G.; Schulze, L.; Herpertz, S.C. Emotion recognition in borderline personality disorder—A review of the literature. J. Personal. Disord. 2009, 23, 6–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bortolla, R.; Cavicchioli, M.; Fossati, A.; Maffei, C. Emotional Reactivity in Borderline Personality Disorder: Theoretical Considerations Based on a Meta-Analytic Review of Laboratory Studies. J. Personal. Disord. 2020, 34, 64–87. [Google Scholar] [CrossRef] [PubMed]
- Hartikainen, K.M. Emotion-Attention Interaction in the Right Hemisphere. Brain Sci. 2021, 11, 1006. [Google Scholar] [CrossRef] [PubMed]
- Ueltzhöffer, K.; Herpertz, S.C.; Krauch, M.; Schmahl, C.; Bertsch, K. Whole-brain functional connectivity during script-driven aggression in borderline personality disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 93, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Hampton, W.H.; Hanik, I.M.; Olson, I.R. Substance abuse and white matter: Findings, limitations, and future of diffusion tensor imaging research. Drug Alcohol Depend. 2019, 197, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Mori, S.; Wakana, S.; Van Zijl, P.C.; Nagae-Poetscher, L.M. MRI Atlas of Human White Matter; Elsevier: Amsterdam, The Netherlands, 2005. [Google Scholar]


{kind=link}
{kind=link}
| Demographic Features | BPD | HC | Test Value (df) | p Value |
|---|---|---|---|---|
| Age, years | 29.1 ± 7.7 | 28.9 ± 6.9 | U = 759.5 | 0.943 |
| Sex, females % | 88% | 81% | X2(1) = 0.808 | 0.369 |
| Education, years | 12.9 ± 3.1 | 17.3 ± 2.2 | U = 227.0 | <0.001 |
| Clinical features | ||||
| SCL-90-R | 181.0 ± 66.0 | 24.8 ± 19.3 | U = 4.0 | <0.001 |
| BIS-11 | 74.6 ± 12.0 | 54.8 ± 8.8 | t(81) = 7.422 | <0.001 |
| DERS | 125.3 ± 22.9 | 64.6 ± 11.7 | U = 12.0 | <0.001 |
| ZAN-BPD | 16.5 ± 5.1 | 2.1 ± 1.8 | U = 1.50 | <0.001 |
| STAXI-2 | ||||
| Anger/state | 23.9 ± 10.2 | 15.3 ± 0.6 | U = 218.5 | <0.001 |
| Anger/trait | 7.8 ± 10.6 | 2.9 ± 4.5 | U = 344.0 | <0.001 |
| Anger expression/out | 20.8 ± 4.7 | 14.4 ± 3.8 | U = 199.5 | <0.001 |
| Anger expression/in | 23.0 ± 4.6 | 16.3 ± 3.7 | t(81) = 6.430 | <0.001 |
| Anger control/out | 14.3 ± 4.2 | 19.9 ± 4.1 | t(81) = −5.570 | <0.001 |
| Anger control/in | 16.8 ± 4.4 | 23.3 ± 4.7 | t(81) = −6.155 | <0.001 |
| Anger expression/index | 60.1 ± 11.4 | 35.6 ± 11.9 | t(81) = 9.098 | <0.001 |
| CTQ | 62.9 ± 13.9 | 44.8 ± 3.5 | U = 82.5 | <0.001 |
| MAI | 32.5 ± 6.8 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quattrini, G.; Magni, L.R.; Lanfredi, M.; Pedrini, L.; Carcione, A.; Riccardi, I.; Corbo, D.; Gasparotti, R.; Rossi, R.; Pievani, M.; et al. Aberrant Structural Connectivity of the Triple Network System in Borderline Personality Disorder Is Associated with Behavioral Dysregulation. J. Clin. Med. 2022, 11, 1757. https://doi.org/10.3390/jcm11071757
Quattrini G, Magni LR, Lanfredi M, Pedrini L, Carcione A, Riccardi I, Corbo D, Gasparotti R, Rossi R, Pievani M, et al. Aberrant Structural Connectivity of the Triple Network System in Borderline Personality Disorder Is Associated with Behavioral Dysregulation. Journal of Clinical Medicine. 2022; 11(7):1757. https://doi.org/10.3390/jcm11071757
Chicago/Turabian StyleQuattrini, Giulia, Laura Rosa Magni, Mariangela Lanfredi, Laura Pedrini, Antonino Carcione, Ilaria Riccardi, Daniele Corbo, Roberto Gasparotti, Roberta Rossi, Michela Pievani, and et al. 2022. "Aberrant Structural Connectivity of the Triple Network System in Borderline Personality Disorder Is Associated with Behavioral Dysregulation" Journal of Clinical Medicine 11, no. 7: 1757. https://doi.org/10.3390/jcm11071757