
Candidacy for Cochlear Implantation in Prelingual Profoundly Deaf Adult Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Auditory Performance and Communication Evaluations
2.3. Statistical Analysis
3. Results
3.1. Population
3.2. Cochlear Implant Outcomes
3.3. Analysis of Preoperative Factors
3.4. Benefits of Bilateralisation in the Case of Sequential Cochlear Implantation
4. Discussion
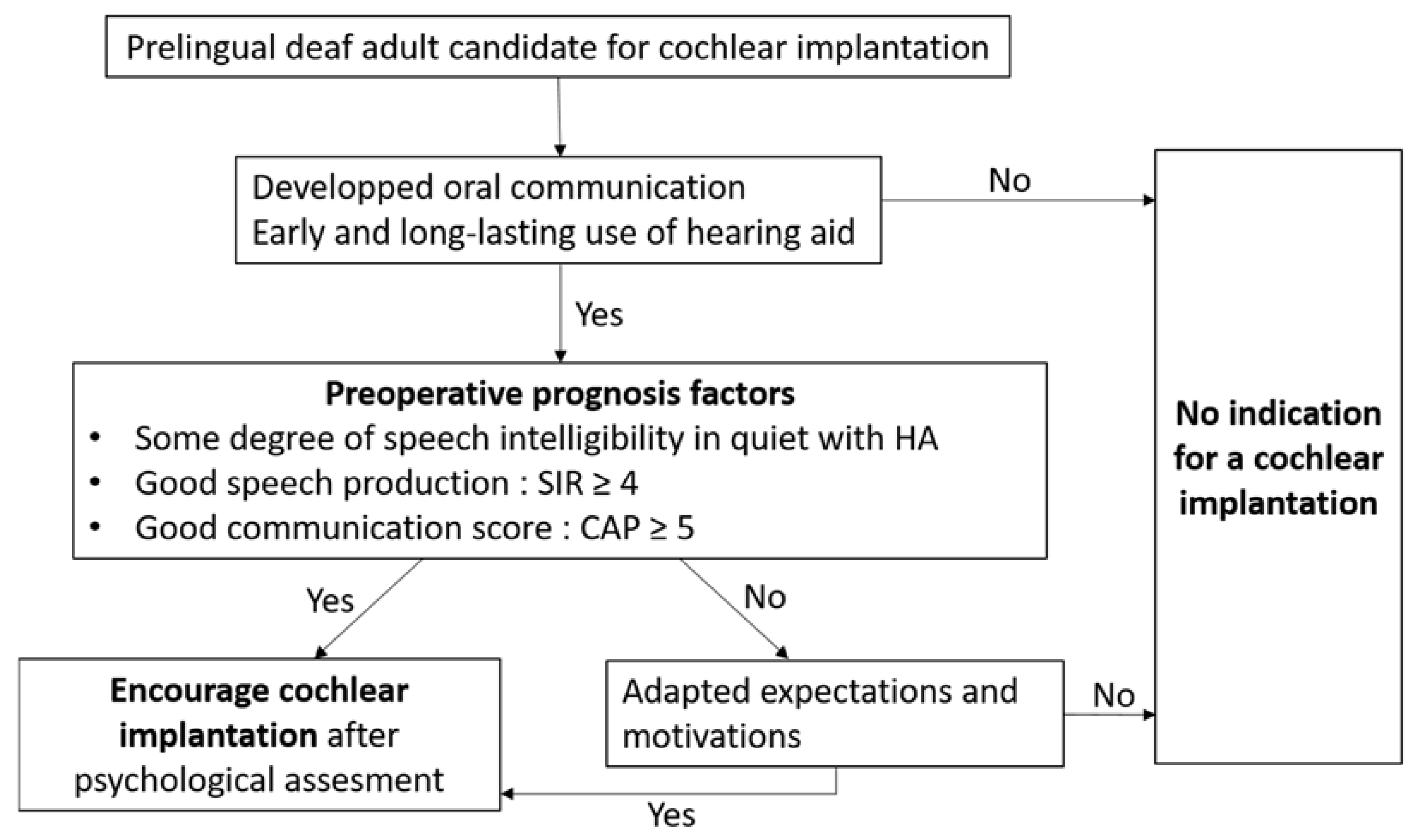
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lenarz, M.; Sönmez, H.; Joseph, G.; Büchner, A.; Lenarz, T. Long-Term Performance of Cochlear Implants in Postlingually Deafened Adults. Otolaryngol.-Head Neck Surg. 2012, 147, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Gaylor, J.M.; Raman, G.; Chung, M.; Lee, J.; Rao, M.; Lau, J.; Poe, D.S. Cochlear implantation in adults: A systematic review and meta-analysis. JAMA Otolaryngol.-Head Neck Surg. 2013, 139, 265–272. [Google Scholar] [CrossRef]
- McRackan, T.R.; Bauschard, M.; Hatch, J.L.; Franko-Tobin, E.; Droghini, H.R.; Nguyen, S.A.; Dubno, J.R. Meta-analysis of quality-of-life improvement after cochlear implantation and associations with speech recognition abilities. Laryngoscope 2018, 128, 982–990. [Google Scholar] [CrossRef] [PubMed]
- Black, J.; Hickson, L.; Black, B.; Perry, C. Prognostic indicators in paediatric cochlear implant surgery: A systematic literature review. Cochlear Implant. Int. 2011, 12, 67–93. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Torres, I.; Madrid-Cánovas, S.; Blanco-Montañez, G. Sensitive periods and language in cochlear implant users. J. Child Lang. 2016, 43, 479–504. [Google Scholar] [CrossRef]
- HAS. Le Traitement de la Surdité par Implants Cochléaires ou du Tronc Cérébral; HAS: Paris, France, 2012. [Google Scholar]
- Simon, F.; Roman, S.; Truy, E.; Barone, P.; Belmin, J.; Blanchet, C.; Borel, S.; Charpiot, A.; Coez, A.; Deguine, O.; et al. Guidelines (short version) of the French society of otorhinolaryngology (SFORL) on pediatric cochlear implant indications. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, 136, 385–391. [Google Scholar] [CrossRef]
- Kumar, R.S.; Mawman, D.; Sankaran, D.; Melling, C.; O’Driscoll, M.; Freeman, S.M.; Lloyd, S.K.W. Cochlear implantation in early deafened, late implanted adults: Do they benefit? Cochlear Implant. Int. 2016, 17, 22–25. [Google Scholar] [CrossRef]
- Kraaijenga, V.J.C.; Smit, A.L.; Stegeman, I.; Smilde, J.J.M.; van Zanten, G.A.; Grolman, W. Factors that influence outcomes in cochlear implantation in adults, based on patient-related characteristics—A retrospective study. Clin. Otolaryngol. 2016, 41, 585–592. [Google Scholar] [CrossRef]
- Arisi, E.; Forti, S.; Pagani, D.; Todini, L.; Torretta, S.; Ambrosetti, U.; Pignataro, L. Cochlear implantation in adolescents with prelinguistic deafness. Otolaryngol. Head Neck Surg. 2010, 142, 804–808. [Google Scholar] [CrossRef]
- Bosco, E.; Nicastri, M.; Ballantyne, D.; Viccaro, M.; Ruoppolo, G.; Maddalena, A.I.; Mancini, P. Long term results in late implanted adolescent and adult CI recipients. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 2611–2620. [Google Scholar] [CrossRef]
- Heywood, R.L.; Vickers, D.A.; Pinto, F.; Fereos, G.; Shaida, A. Assessment and outcome in non-traditional cochlear implant candidates. Audiol. Neurotol. 2017, 21, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Lammers, M.J.W.; Versnel, H.; Topsakal, V.; Zanten, G.A.V.; Grolman, W. Predicting performance and non-use in prelingually deaf and late-implanted cochlear implant users. Otol. Neurotol. 2018, 39, e436–e442. [Google Scholar] [CrossRef] [PubMed]
- Klop, W.M.C.; Briaire, J.J.; Stiggelbout, A.M.; Frijns, J.H.M. Cochlear implant outcomes and quality of life in adults with prelingual deafness. Laryngoscope 2007, 117, 1982–1987. [Google Scholar] [CrossRef] [PubMed]
- O’Gara, S.J.; Cullington, H.E.; Grasmeder, M.L.; Adamou, M.; Matthews, E.S. factors affecting speech perception improvement post implantation in congenitally deaf adults. Ear Hear. 2016, 37, 671–679. [Google Scholar] [CrossRef]
- Debruyne, J.; Janssen, M.; Brokx, J. Late cochlear implantation in early-deafened adults: A detailed analysis of auditory and self-perceived benefits. Audiol. Neurotol. 2018, 22, 364–376. [Google Scholar] [CrossRef] [PubMed]
- Duchesne, L.; Millette, I.; Bhérer, M.; Gobeil, S. Auditory performance and subjective benefits in adults with congenital or prelinguistic deafness who receive cochlear implants during adulthood. Cochlear Implant. Int. 2017, 18, 143–152. [Google Scholar] [CrossRef]
- Debruyne, J.; Janssen, A.; Brokx, J. Systematic review on late cochlear implantation in early-deafened adults and adolescents: Clinical effectiveness. Ear Hear. 2020, 41, 1417–1430. [Google Scholar] [CrossRef]
- Debruyne, J.; Janssen, A.; Brokx, J. Systematic review on late cochlear implantation in early-deafened adults and adolescents: Predictors of performance. Ear Hear. 2020, 41, 1431–1441. [Google Scholar] [CrossRef]
- Hermann, R.; Lescanne, E.; Loundon, N.; Barone, P.; Belmin, J.; Blanchet, C.; Borel, S.; Charpiot, A.; Coez, A.; Deguine, O.; et al. French society of ENT (SFORL) guidelines. Indications for cochlear implantation in adults. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, 136, 193–197. [Google Scholar] [CrossRef]
- Kalafat, M.; Hugonot-Diener, L.; Poitrenaud, J. Standardisation et étalonnage français du “Mini-Mental State”, version GRECO. Rev. Neuropsychol. 2003, 13, 209–236. [Google Scholar]
- Archbold, S.; Lutman, M.; Marshall, D. Categories of auditory performance. Ann. Otol Rhinol Laryngol. Suppl. 1995, 166, 312–314. [Google Scholar] [PubMed]
- Cox, R.; Alexander, G. The abbreviated profile of hearing aid benefit. Ear Hear. 1995, 16, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.; Nikolopoulos, T.; Dyar, D.; O’Donoghue, G. Reliability of a rating scale for measuring speech intelligibility after pediatric cochlear implantation. Otol. Neurotol. 2001, 22, 631–633. [Google Scholar] [CrossRef] [PubMed]
- Rousset, A.; Dowell, R.; Leigh, J. Receptive language as a predictor of cochlear implant outcome for prelingually deaf adults. Int. J. Audiol. 2016, 55, S24–S30. [Google Scholar] [CrossRef] [PubMed]
- Caposecco, A.; Hickson, L.; Pedley, K. Cochlear implant outcomes in adults and adolescents with early-onset hearing loss. Ear Hear. 2012, 33, 209–220. [Google Scholar] [CrossRef]
- Craddock, L.; Cooper, H.; Riley, A.; Wright, T. Cochlear implants for pre-lingually profoundly deaf adults. Cochlear Implant. Int. 2016, 17, 26–30. [Google Scholar] [CrossRef]
- Yang, W.S.; Moon, I.S.; Kim, H.N.; Lee, W.S.; Lee, S.E.; Choi, J.Y. Delayed cochlear implantation in adults with prelingual severe-to-profound hearing loss. Otol. Neurotol. 2011, 32, 223–228. [Google Scholar] [CrossRef]
- Holden, L.K.; Au, D.; Finley, C.C.; Ph, D.; Firszt, J.B.; Timothy, A.; Brenner, C.; Potts, L.G.; Gotter, B.D.; Vanderhoof, S.S.; et al. Factors affecting open-set word recognition in adults with cochlear implants. Ear Hear. 2013, 34, 342–360. [Google Scholar] [CrossRef] [Green Version]
- Mosnier, I.; Ferrary, E.; Aubry, K.; Bordure, P.; Bozorg-Grayeli, A.; Deguine, O.; Eyermann, C.; Franco-Vidal, V.; Godey, B.; Guevara, N.; et al. The French national cochlear implant registry (EPIIC): Cochlear implantation in adults over 65 years old. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2020, 137, S19–S25. [Google Scholar] [CrossRef]
- Lazard, D.S.; Giraud, A.L.; Gnansia, D.; Meyer, B.; Sterkers, O. Understanding the deafened brain: Implications for cochlear implant rehabilitation. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2012, 129, 98–103. [Google Scholar] [CrossRef]
- Debruyne, J.A.; Francart, T.; Janssen, A.M.L.; Douma, K.; Brokx, J.P.L. Fitting prelingually deafened adult cochlear implant users based on electrode discrimination performance. Int. J. Audiol. 2017, 56, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Santarelli, R.; De Filippi, R.; Genovese, E.; Arslan, E. Cochlear implantation outcome in prelingually deafened young adults: A speech perception study. Audiol. Neurotol. 2008, 13, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Cusumano, C.; Friedmann, D.R.; Fang, Y.; Wang, B.; Roland, J.T.; Waltzman, S.B. Performance plateau in prelingually and postlingually deafened adult cochlear implant recipients. Otol. Neurotol. 2017, 38, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Van Dijkhuizen, J.N.; Boermans, P.P.B.M.; Briaire, J.J.; Frijns, J.H.M. Intelligibility of the patient’s speech predicts the likelihood of cochlear implant success in prelingually deaf adults. Ear Hear. 2016, 37, e302–e310. [Google Scholar] [CrossRef] [PubMed]
- Lyness, C.R.; Woll, B.; Campbell, R.; Cardin, V. How does visual language affect crossmodal plasticity and cochlear implant success? Neurosci. Biobehav. Rev. 2013, 37, 2621–2630. [Google Scholar] [CrossRef] [Green Version]
- De Seta, D.; Nguyen, Y.; Vanier, A.; Ferrary, E.; Bebear, J.P.; Godey, B.; Robier, A.; Mondain, M.; Deguine, O.; Sterkers, O.; et al. Five-year hearing outcomes in bilateral simultaneously cochlear-implanted adult patients. Audiol. Neurotol. 2016, 21, 261–267. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | HL Etiology | HL Class at dg ¥ | Age at dg (Months) | Age at First HA (Months) | Duration without HA (Years) | Social Category | CAP | SIR | Communication † | Preoperative PTA (dB) | Type of Implantation | Age at CI (Years) | Year of First CI | CI Model | WSI at One Year (%) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CI Ear | Non-CI Ear | CI Ear | Non-CI Ear | |||||||||||||||
| 1 | F | Unknown | S | 12 | 12 | 12 | 1 | 7 | 5 | 5 | O | 115 | 114 | Unilateral | 29 | 2019 | CI522 | 100 |
| 2 | F | Unknown | P | 24 | 24 | 24 | 2 | 7 | 7 | 5 | O | 102.5 | 99 | Bilateral seq. | 22 | 2010 | Ci512 | 90 |
| 3 | M | Cnx 26 | P | 24 | 24 | 24 | 2 | 7 | NR | 5 | O | 120 | 111 | Bilateral seq. | 26 | 2015 | CI24RE | 80 |
| 4 | F | Unknown | S | 24 | 24 | 24 | 2 | 7 | 5 | 5 | O | 99 | 98 | Unilateral | 39 | 2014 | CI24RE | 70 |
| 5 | F | Cnx 26 | P | 12 | 12 | 12 | 1 | 6 | 6 | 5 | O | 99 | 99 | Unilateral | 16 | 2013 | CI24RE | 70 |
| 6 | M | Cnx 26 | S | 12 | 60 | 60 | 5 | 4 | 5 | 4 | O | 115 | 104 | Unilateral | 52 | 2018 | CI522 | 70 |
| 7 | F | IUI | P | 1 | 3 | 3 | 0 | 7 | 4 | 5 | O | 115 | 102.5 | Bilateral seq. | 45 | 2013 | Ci522 | 70 |
| 8 | F | Unknown | S | 24 | 24 | 24 | 2 | 6 | 5 | 5 | O | 109 | 99 | Bilateral seq. | 30 | 2012 | Med-El Flex31 | 60 |
| 9 | M | Meningitis | S | 3 | 96 | 144 | 8 | 1 | 5 | 4 | O | 105 | 105 | Bilateral sim. | 47 | 2018 | Neuro ZTI Evo | 60 |
| 10 | F | Cnx 26 | P | 16 | 16 | 16 | 1 | 7 | 6 | 5 | O | 102 | 96 | Unilateral | 32 | 2012 | CI24RE | 50 |
| 11 | F | Genetic | S | 40 | 40 | 40 | 3 | 7 | 5 | 4 | O + S | 109 | 112 | Bilateral seq. | 27 | 2012 | CI422 | 50 |
| 12 | F | IUI | P | 9 | 9 | 9 | 5 | 2 | 2 | 2 | O + S | 117 | 111 | Bilateral sim. | 20 | 2007 | Med-El | 50 |
| 13 | M | Cnx 26 | S | 15 | 16 | 16 | 1 | 7 | 5 | 4 | O | 111 | 109 | Unilateral | 32 | 2018 | CI522 | 50 |
| 14 | F | Unknown | P | 24 | 24 | 24 | 2 | 7 | 5 | 5 | O | 109 | 99 | Unilateral | 27 | 2018 | Ci522 | 50 |
| 15 | M | Unknown | S | 18 | 18 | 18 | 1.5 | 7 | 3 | 5 | O | 97.5 | 95 | Unilateral | 20 | 2013 | Ci422 | 50 |
| 16 | M | Unknown | S | 9 | 9 | 9 | 1 | 7 | 3 | 5 | O | 111 | 99 | Unilateral | 31 | 2013 | Ci422 | 40 |
| 17 | F | Cnx 26 | S | 6 | 6 | 6 | 0 | 7 | 5 | 5 | O | 116 | 108 | Bilateral sim. | 39 | 2016 | Ci512 | 40 |
| 18 | F | Cnx 26 | P | 45 | 167 | 45 | 14 | 7 | NR | NR | O + S | 114 | 115 | Unilateral | 45 | 2004 | Ci24CA | 30 |
| 19 | M | Unknown | P | 18 | 18 | 18 | 1 | 6 | 5 | 4 | O | 99 | 91 | Unilateral | 21 | 2012 | Ci24RE | 30 |
| 20 | F | Cnx 26 | P | 9 | 9 | 9 | 1 | 7 | 5 | 3 | O + S | 112 | 108 | Bilateral seq. | 25 | 2012 | Ci24RE | 30 |
| 21 | M | Cnx 26 | P | 12 | 12 | 12 | 6 | 6 | NR | NR | O + S | 110 | 106 | Unilateral | 33 | 2007 | Digisonic SP | 20 |
| 22 | M | Unknown | S | 36 | 36 | 36 | 3 | 6 | 5 | 3 | O + S | 115 | 116 | Unilateral | 32 | 2008 | CI24RE | 20 |
| 23 | F | Unknown | P | 3 | 3 | 3 | 0 | 7 | 4 | 2 | O + S | 110 | 104 | Unilateral | 18 | 2011 | CI24RE | 20 |
| 24 | F | Cnx 26 | P | 12 | 12 | 12 | 1 | 6 | 5 | 4 | O + S | 110 | 105 | Bilateral seq. | 30 | 2015 | Ci422 | 10 |
| 25 | M | Genetic | S | 36 | 36 | 36 | 3 | 6 | 5 | 4 | O + S | 99 | 115 | Unilateral | 21 | 2014 | Digisonic SP | 10 |
| 26 | F | Cnx 26 | P | 24 | 24 | 24 | 2 | 7 | 3 | 4 | O + S | 110 | 107 | Unilateral | 24 | 2016 | Ci422 | 10 |
| 27 | M | Genetic | S | 46 | 46 | 46 | 4 | 6 | 5 | 5 | O | 115 | 110 | Bilateral seq. | 41 | 2010 | Ci24RE | 0 |
| 28 | M | Premature | S | 24 | 29 | 29 | 2 | 3 | 3 | 3 | O + C | 99 | 94 | Unilateral | 33 | 2011 | Med-El Ti100 | 0 |
| 29 | F | Genetic | P | 18 | 71 | 71 | 36 | 6 | 4 | 4 | O | 109 | 110 | Bilateral sim. | 43 | 2008 | Ci24RE | 0 |
| 30 | F | IUI | P | 46 | - | - | 30 | 1 | 1 | 1 | C | 111 | 100 | Bilateral sim. | 30 | 2013 | Digisonic SP | 0 |
| 31 | F | Unknown | P | 36 | 36 | 36 | 10 | 4 | 1 | 1 | S | 120 | 120 | Bilateral sim. | 23 | 2013 | Digisonic SP | 0 |
| 32 | F | Cnx 26 | S | 12 | 12 | 12 | 1 | 7 | 5 | 4 | O | 110 | 112 | Bilateral sim. | 41 | 2015 | Ci422 | 0 |
| 33 | M | Genetic | P | 36 | NR | NR | NR | 4 | 3 | 2 | O + S | 116 | 120 | Unilateral | 24 | 2019 | NeuroZTI Evo | 0 |
| 34 | F | IUI | P | 36 | 120 | 36 | 10 | 4 | 2 | 3 | O | 112 | 111 | Bilateral seq. | 55 | 2013 | Digisonic Evo | 0 |
| Poor Performers | Good Performers | |||||
|---|---|---|---|---|---|---|
| Preoperative | 1 Year Post-CI | p-Value | Preoperative | 1 Year Post-CI | p-Value | |
| Speech intelligibility | ||||||
| Disyllabic words | 4 ± 1.9 (0–30), n = 19 | 14 ± 3.4 (0–40), n = 19 | 0.052 ¥ | 11 ± 4.6 (0–50), n = 15 | 65 ± 4.1 (50–100), n = 15 | <0.0001 ¥ |
| Words in sentences | 2 ± 1.6 (0–14), n = 9 | 30 ± 8.6 (0–77), n = 12 | 0.13 ¥ | 20 ± 8.9 (0–92), n = 12 | 75 ± 6.7 (30–100), n = 14 | 0.001 ¥ |
| Sentences | 0 ± 0 (0–0), n = 9 | 15 ± 6.2 (0–60), n = 13 | 0.25 ¥ | 13 ± 7 (0–80), n = 12 | 64 ± 5.2 (33–100), n = 14 | 0.0007 ¥ |
| CAP | ||||||
| 1 | 2 | 0 | 0.015 ∞ | 0 | 0 | 0.0003 ∞ |
| 2 | 1 | 1 | 1 | 0 | ||
| 3 | 4 | 0 | 1 | 0 | ||
| 4 | 2 | 6 | 1 | 0 | ||
| 5 | 8 | 4 | 8 | 2 | ||
| 6 | 0 | 3 | 2 | 3 | ||
| 7 | 0 | 2 | 1 | 2 | ||
| 8 | 0 | 1 | 0 | 3 | ||
| 9 | 0 | 0 | 0 | 4 | ||
| Poor Performers (n = 4) | Good Performers (n = 5) | |||||
|---|---|---|---|---|---|---|
| Before the 2nd | 1 Year Post-2nd | p-Value | Before the 2nd | 1 Year Post-2nd | p-Value | |
| SI in quiet | ||||||
| Disyllabic words | 33 ± 16.5 (10–70), n = 4 | 50 ± 13.5 (30–90), n = 4 | 0.4 ¥ | 82 ± 11.1 (50–100), n = 5 | 88 ± 6.3 (70–100), n = 4 | 0.9 ¥ |
| Words in sentences | 48 ± 21.2 (0–94), n = 4 | 66 ± 13.0 (44–89), n = 3 | 0.9 ¥ | 83 ± 9.3 (51–100), n = 5 | 89 ± 10.5 (68–100), n = 3 | 0.7 ¥ |
| Sentences | 33 ± 17.7 (0–80), n = 4 | 49 ± 17.4 (20–80), n = 3 | 0.8 ¥ | 69 ± 13.6 (33–100), n = 5 | 80 ± 16.6 (47–100), n = 3 | 0.5 ¥ |
| SI in noise | ||||||
| Words in sentences | 25 ± 18.4 (0–78), n = 4 | 38 ± 14.4 (11–60), n = 3 | 0.9 ¥ | 55 ± 18.6 (3–91), n = 5 | 78 ± 11.7 (56–100), n = 4 | 0.1 ¥ |
| Sentences | 15 ± 15.0 (0–60), n = 4 | 20 ± 7.5 (7–33), n = 3 | 0.9 ¥ | 41 ± 17.4 (0–80), n = 5 | 62 ± 20.1 (27–100), n = 4 | 0.07 ¥ |
| APHAB | 45 ± 4.8 (33–57), n = 4 | 45 ± 4.7 (37–57), n = 4 | >0.9 ‡ | 48 ± 7.1 (33–67), n = 5 | 39 ± 8.6 (15–57), n = 4 | 0.6 ‡ |
| CAP | ||||||
| 5 | 1 | 1 | 0.8 ∞ | 1 | 0 | 0.09 ∞ |
| 6 | 0 | 0 | 1 | 0 | ||
| 7 | 0 | 1 | 1 | 0 | ||
| 8 | 2 | 1 | 1 | 2 | ||
| 9 | 1 | 1 | 1 | 2 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lahlou, G.; Daoudi, H.; Ferrary, E.; Jia, H.; De Bergh, M.; Nguyen, Y.; Sterkers, O.; Mosnier, I. Candidacy for Cochlear Implantation in Prelingual Profoundly Deaf Adult Patients. J. Clin. Med. 2022, 11, 1874. https://doi.org/10.3390/jcm11071874
Lahlou G, Daoudi H, Ferrary E, Jia H, De Bergh M, Nguyen Y, Sterkers O, Mosnier I. Candidacy for Cochlear Implantation in Prelingual Profoundly Deaf Adult Patients. Journal of Clinical Medicine. 2022; 11(7):1874. https://doi.org/10.3390/jcm11071874
Chicago/Turabian StyleLahlou, Ghizlene, Hannah Daoudi, Evelyne Ferrary, Huan Jia, Marion De Bergh, Yann Nguyen, Olivier Sterkers, and Isabelle Mosnier. 2022. "Candidacy for Cochlear Implantation in Prelingual Profoundly Deaf Adult Patients" Journal of Clinical Medicine 11, no. 7: 1874. https://doi.org/10.3390/jcm11071874