
Sinus Lift Associated with Leucocyte-Platelet-Rich Fibrin (Second Generation) for Bone Gain: A Systematic Review

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
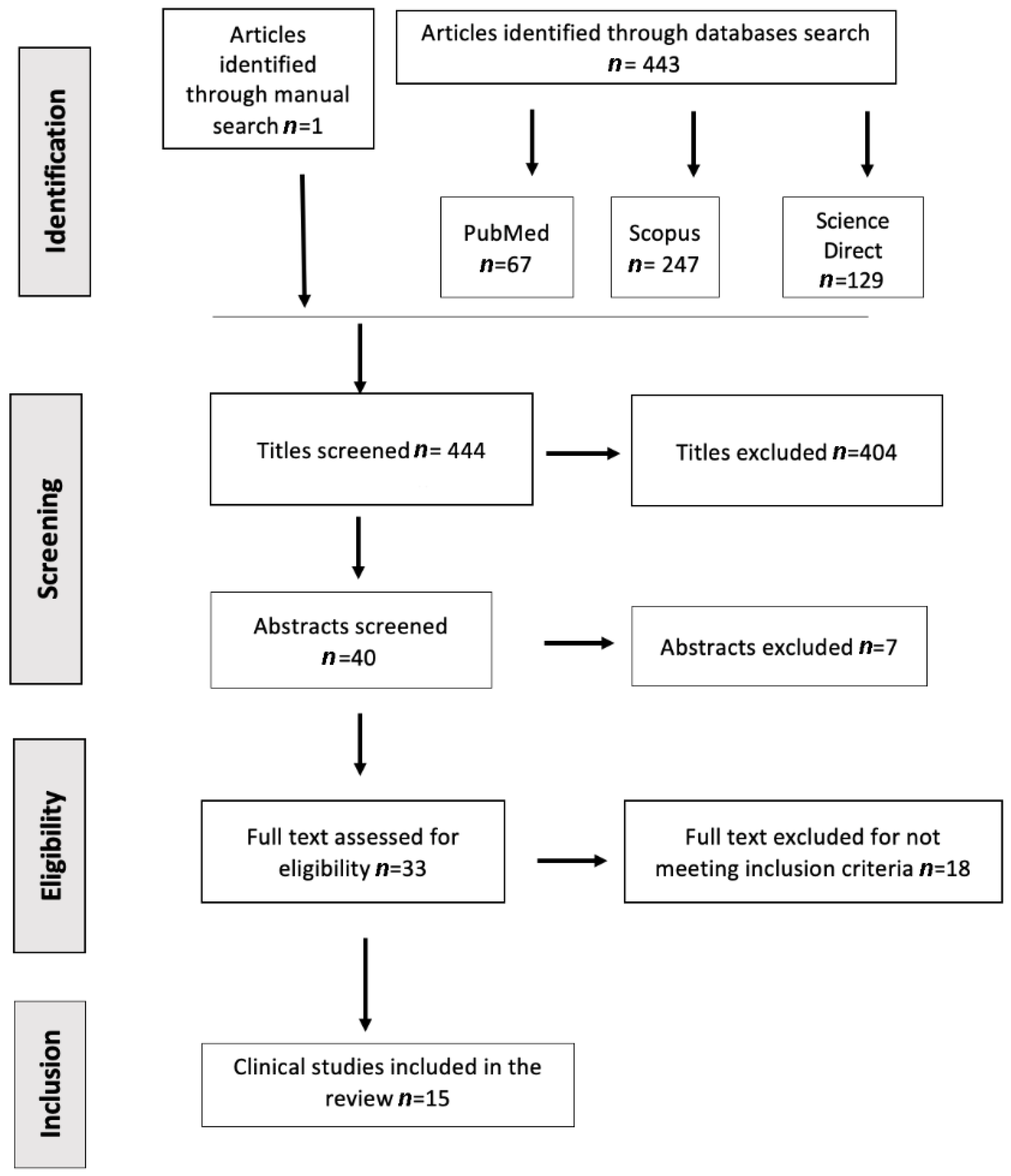
2. Materials and Methods
2.1. Focused Question
2.2. Information Sources and Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Quality Assessment and Risk of Bias
3. Results
3.1. Studies Characteristics
3.2. Quality Assessment and Risk of Bias
3.3. Total Patients, Age, and Amount of Surgeries
3.4. Follow-Up
3.5. Surgical Approach and Residual Bone Height
3.6. Membrane Perforation and Implant Failure
3.7. Biomaterials Association
3.7.1. PRF as the Sole Biomaterial
3.7.2. PRF with Allograft
3.7.3. PRF with Xenografts
3.7.4. PRF with Synthetic Bone Graft
3.8. New Bone Formation
3.9. Implant Stability Quotient (ISQ)
4. Discussion
4.1. PRF and Other Biomaterials
4.2. Only PRF Inserted
4.3. Implant Stability Quotient (ISQ)
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACP | autologous platelet concentrates |
| β-TCP | Beta-tricalcium phosphate |
| CGF | Concentrated growth factor |
| FDBA | Freeze-dried bone allograft |
| IGF | Insulin-like growth factor |
| ISQ | Implant Stability Quotient |
| L-PRF | Leucocyte and platelet-rich fibrin |
| NOS | Newcastle-Ottawa Scale |
| PDGF | platelet-derived growth factor |
| PRF | platelet-rich fibrin |
| PRGF | Platelet-rich in growth factors |
| RFA | Resonance frequency analysis |
| TGF-α | Transforming growth factor-beta |
| VEGF | Vascular endothelial growth factor |
References
- Ahmed, T.A.E.; Dare, E.V.; Hincke, M. Fibrin: A versatile scaffold for tissue engineering applications. Tissue Eng. Part B Rev. 2008, 14, 199–215. [Google Scholar] [CrossRef] [PubMed]
- Carrao, V.; De Matteis, I. Maxillary sinus bone augmentation techniques. Oral Maxillofac. Surg. Clin. N. Am. 2015, 27, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Atalay, B. Sinus lifting and leucocyte- and platelet-rich fibrin. In Challenging Issues on Paranasal Sinuses; IntechOpen: London, UK, 2019. [Google Scholar]
- Harduin-Couto, M.; Gonçalves, A.O.; Rizzato, M.; Oliveira, E.R.; Fisher-Trindade, H.; Fernandes, G.V.O. Endoscopic analysis of alterations in sinus floor elevation approaching the summers technique and immediate implant: A clinical trial with 10 years follow-up. Int. J. Sci. Dent. 2022, 58, 77–96. [Google Scholar]
- Bennardo, F.; Barone, S.; Vocaturo, C.; Nucci, L.; Antonelli, A.; Giudice, A. Usefulness of Magnetic Mallet in Oral Surgery and Implantology: A Systematic Review. J. Pers. Med. 2022, 12, 108. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Rosano, G.; Taschieri, S. Implant survival rates after maxillary sinus augmentation. Eur. J. Oral Sci. 2008, 116, 497–506. [Google Scholar] [CrossRef]
- Watanabe, T.; Isobe, K.; Suzuki, T.; Kawabata, H.; Nakamura, M.; Tsukioka, T.; Okudera, T.; Okudera, H.; Uematsu, K.; Okuda, K.; et al. An evaluation of the accuracy of the subtraction method used for determining platelet counts in advanced platelet-rich fibrin and concentrated growth factor preparations. Dent. J. 2017, 5, 7. [Google Scholar] [CrossRef] [Green Version]
- Rodella, L.F.; Favero, G.; Boninsegna, R.; Buffoli, B.; Labanca, M.; Scarì, G.; Sacco, L.; Batani, T.; Rezzani, R. Growth factors, CD34 positive cells, and fibrin network analysis in concentrated growth factors fraction. Microsc. Res. Tech. 2011, 74, 772–777. [Google Scholar] [CrossRef]
- Castro, A.B.; Meschi, N.; Temmerman, A.; Pinto, N.; Lambrechts, P.; Teughels, W.; Quirynen, M. Regenerative potential of leucocyte- and platelet-rich fibrin. Part B: Sinus floor elevation, alveolar ridge preservation and implant therapy. A systematic review. J. Clin. Periodontol. 2017, 44, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Schliephake, H. Clinical efficacy of growth factors to enhance tissue repair in oral and maxillofacial reconstruction: A systematic review. Clin. Implant Dent. Relat. Res. 2015, 17, 247–273. [Google Scholar] [CrossRef]
- Qiao, J.; An, N.; Ouyang, X. Quantification of growth factors in different platelet concentrates. Platelets 2017, 28, 774–778. [Google Scholar] [CrossRef]
- Aoki, N.; Kanayama, T.; Maeda, M.; Horii, K.; Miyamoto, H.; Wada, K.; Ojima, Y.; Tsuchimochi, T.; Shibuya, Y. Sinus augmentation by platelet-rich fibrin alone: A report of two cases with histological examinations. Case Rep. Dent. 2016, 2016, 2654645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonpieri, A.; Choukroun, J.; Corso, M.D.; Sammartino, G.; Ehrenfest, D.M.D. Simultaneous sinus-lift and implantation using microthreaded implants and leukocyte- and platelet-rich fibrin as sole grafting material: A six-year experience. Implant Dent. 2011, 20, 2–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anitua, E.; Aguirre, J.J.; Algorta, J.; Ayerdi, E.; Cabezas, A.I.; Orive, G.; Andia, I. Effectiveness of autologous preparation rich in growth factors for the treatment of chronic cutaneous ulcers. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 84, 415. [Google Scholar] [CrossRef] [PubMed]
- Fortunato, L.; Barone, S.; Bennardo, F.; Giudice, A. Regenerative surgery: Management of Facial Pyoderma Gangrenosum Using Platelet-Rich Fibrin: A Technical Report. J. Oral Maxillofac. Surg. 2018, 76, 1460–1463. [Google Scholar] [CrossRef]
- Sun, G.; Cao, L.; Li, H. Effects of platelet-rich fibrin combined with guided bone regeneration in the reconstruction of peri-implantitis bone defect. Am. J. Transl. Res. 2021, 13, 8397–8402. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Kempraj, J.; Sundaram, S.S.; Doss, G.P.T.; Nakeeran, K.P.; Raja, V.B.K.K. Maxillary sinus augmentation using xenograft and choukroun’s platelet-rich fibrin as grafting material: A radiological study. J. Maxillofac. Oral Surg. 2020, 1, 263–268. [Google Scholar] [CrossRef]
- Lei, L.; Yu, Y.; Han, J.; Shi, D.; Sun, W.; Zhang, D.; Chen, L. Quantification of growth factors in advanced platelet-rich fibrin and concentrated growth factors and their clinical efficacy as adjunctive to the GTR procedure in periodontal intrabony defects. J. Periodontol. 2020, 91, 462–472. [Google Scholar] [CrossRef]
- Toffler, M.; Toscano, N.; Holtzclaw, D. Osteotome-mediated sinus floor elevation using only platelet-rich fibrin: An early report on 110 patients. Implant Dent. 2010, 19, 447–456. [Google Scholar] [CrossRef] [Green Version]
- Anitua, E.; Prado, R.; Orive, G. Bilateral sinus elevation evaluating plasma rich in growth factors technology: A report of five cases. Clin. Implant Dent. Relat. Res. 2012, 14, 51–60. [Google Scholar] [CrossRef]
- Cho, Y.S.; Hwang, K.G.; Jun, S.H.; Tallarico, M.; Kwon, A.M.; Park, C.J. Radiologic comparative analysis between saline and platelet-rich fibrin filling after hydraulic transcrestal sinus lifting without adjunctive bone graft: A randomized controlled trial. Clin. Oral Implant. Res. 2020, 31, 1087–1093. [Google Scholar] [CrossRef] [PubMed]
- Pichotano, E.C.; de Molon, R.S.; de Souza, R.V.; Austin, R.S.; Marcantonio, E.; Zandim-Barcelos, D.L. Evaluation of L-PRF combined with deproteinized bovine bone mineral for early implant placement after maxillary sinus augmentation: A randomized clinical trial. Clin. Implant Dent. Relat. Res. 2019, 21, 253–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kılıç, S.C.; Güngörmüş, M.; Parlak, S.N. Histologic and histomorphometric assessment of sinus-floor augmentation with beta-tricalcium phosphate alone or in combination with pure-platelet-rich plasma or platelet-rich fibrin: A randomized clinical trial. Clin. Implant Dent. Relat. Res. 2017, 19, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Gassling, V.; Purcz, N.; Braesen, J.H.; Will, M.; Gierloff, M.; Behrens, E.; Açil, Y.; Wiltfang, J. Comparison of two different absorbable membranes for the coverage of lateral osteotomy sites in maxillary sinus augmentation: A preliminary study. J. Craniomaxillofac. Surg. 2013, 41, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Nizam, N.; Eren, G.; Akcalı, A.; Donos, N. Maxillary sinus augmentation with leukocyte and platelet-rich fibrin and deproteinized bovine bone mineral: A split-mouth histological and histomorphometric study. Clin. Oral Implant. Res. 2018, 29, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Olgun, E.; Ozkan, S.Y.; Atmaca, H.T.; Yalim, M.; Hendek, M.K. Comparison of the clinical, radiographic, and histological effects of titanium-prepared platelet rich fibrin to allograft materials in sinus-lifting procedures. J. Investig. Clin. Dent. 2018, 9, e12347. [Google Scholar] [CrossRef]
- Tatullo, M.; Marrelli, M.; Cassetta, M.; Pacifici, A.; Stefanelli, L.V.; Scacco, S.; Dipalma, G.; Pacifici, L.; Inchingolo, F. Platelet rich fibrin (P.R.F.) in reconstructive surgery of atrophied maxillary bones: Clinical and histological evaluations. Int. J. Med. Sci. 2012, 9, 872–880. [Google Scholar] [CrossRef]
- Aoki, N.; Maeda, M.; Kurata, M.; Hirose, M.; Ojima, Y.; Wada, K.; Shibuya, Y. Sinus floor elevation with platelet-rich fibrin alone: A Clinical retrospective study of 1-7 years. J. Clin. Exp. Dent. 2018, 10, e984–e991. [Google Scholar] [CrossRef]
- Pichotano, E.C.; de Molon, R.S.; de Paula, L.G.F.; de Souza, R.V.; Marcantonio, E.; Zandim-Barcelos, D.L. Early placement of dental implants in maxillary sinus grafted with leukocyte and platelet-rich fibrin and deproteinized bovine bone mineral. J. Oral Implantol. 2018, 44, 199–206. [Google Scholar] [CrossRef]
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Dohan, D.M. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part V: Histologic evaluations of PRF effects on bone allograft maturation in sinus lift. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 299–303. [Google Scholar] [CrossRef]
- Batas, L.; Tsalikis, L.; Stavropoulos, A. PRGF as adjunct to DBB in maxillary sinus floor augmentation: Histological results of a pilot split-mouth study. Int. J. Implant Dent. 2019, 5, 14. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Tangl, S.; Huber, C.D.; Lin, Y.; Qiu, L.; Rausch-Fan, X. Effects of Choukroun’s platelet-rich fibrin on bone regeneration in combination with deproteinized bovine bone mineral in maxillary sinus augmentation: A histological and histomorphometric study. J. Cranio-Maxillofac. Surg. 2012, 40, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Wadhwani, C.P.K. (Ed.) Cementation in Dental Implantology; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Browaeys, H.; Bouvry, P.; De Bruyn, H. A literature review on biomaterials in sinus augmentation procedures. Clin. Implant Dent. Relat. Res. 2007, 9, 166–177. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Lin, Y.; Hu, X.; Zhang, Y.; Wu, H. A comparative study of platelet-rich fibrin (PRF) and platelet-rich plasma (PRP) on the effect of proliferation and differentiation of rat osteoblasts in vitro. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 707–713. [Google Scholar] [CrossRef]
- Chambrone, L.; Ortega, M.A.S.; Sukekava, F.; Rotundo, R.; Kalemaj, Z.; Buti, J.; Prato, G.P.P. Root coverage procedures for treating single and multiple recession-type defects: A Cochrane Systematic Review Updated. J. Periodontol. 2019, 90, 1399–1422. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; de Peppo, G.M.; Doglioli, P.; Sammartino, G. Slow release of growth factors and thrombospondin-1 in Choukroun’s platelet-rich fibrin (PRF): A gold standard to achieve for all surgical platelet concentrates technologies. Growth Factors 2009, 27, 63–69. [Google Scholar] [CrossRef]


{kind=link}
| #1 | P—In clinical studies with patients needing a maxillary sinus lift |
| ((“Sinus Floor Augmentation” [mesh Terms]) OR (“Sinus floor elevation) OR (Sinus lift)) | |
| #2 | I—Does the use of autologous concentrated platelets |
| ((“Platelet-Rich Fibrin” [mesh Terms]) OR (autologous concentrated platelets”) OR (Second generation; platelet concentrate) OR (L-PRF]) OR (PRF)) | |
| #3 | C—with or without the addition of other biomaterials |
| #4 | O—improve the clinical outcome associated with bone gain and density |
| Search combination | (#1 and #2) No combination was done with #3 and #4, since the preponderance of the papers on sinus elevation considers bone gain and density. The combination with keywords related to the outcome would further limit the results. |
| Filters | English, Humans, January 2006–August 2020, in vivo, Clinical Studies |
| Author/Year | Reason for Exclusion |
|---|---|
| Xin et al., 2020 | Data did not clear for evaluation |
| Silberman et al., 2020 | Data does not meet inclusion criteria (focus on perforation) |
| Mohamadamin Damsaz et al., 2020 | Review, Data did not clear for evaluation |
| Xie et al., 2019 | Full text only available in Chinese |
| Wang et al., 2019 | Data does not meet inclusion criteria (focus on infection) |
| Chandra et al., 2019 | Data does not meet inclusion criteria (maxillary sinus) |
| Batas et al., 2019 | Focus on first-generation |
| Öncü et al., 2017 | Data does not meet inclusion criteria (focus on perforation) |
| Karaca et al., 2017 | Only the first generation of ACP discussed |
| Peker et al., 2016 | Data does not meet inclusion criteria (animal) |
| Anitua et al., 2016 | Report of immediate placement |
| Taschieri et al., 2015 | Only the first generation of ACP discussed |
| Tanaka et al., 2015 | Data does not meet inclusion criteria |
| Anitua et al., 2015 | Data mostly on short implants and first-generation |
| Troedhan et al., 2015 | Only anterior maxilla discussed |
| Amin Rahpeyma, 2014 | Only poster/abstract available |
| Inchingolo et al., 2010 | Full text not available |
| Meyer et al., 2009 | Full text only available in French |
| Author/Year | Type of Study | Inclusion Criteria for Each Included Article | Exclusion Criteria for Each Included Article |
|---|---|---|---|
| Cho et al., 2020 | Randomized control trial | Any healthy patient over the age of 18 has edentulism in the posterior maxilla and a decreased RABH, making the placement of implants longer than 8.5 mm unfeasible. | Systemic or local contraindications for implant placement include a history of untreated metabolic problems, smoking habits, bruxism, or uncontrolled periodontal disease, as determined on a cone-beam computed tomography (CBCT) scan and a residual bone height less than 5 mm. |
| Kempraj et al., 2020 | Clinical Study | Patients between 20 and 60 years old with severe maxillary atrophy in the sinus region less than 4 mm | Patients with uncontrolled systemic disorders, heavy smoking, alcohol or drug addiction, and uncontrolled periodontal disorders are at risk. |
| Pichotano et al., 2019 | A double-blinded, randomized controlled trial | Patients having a residual bone height of less than 4 mm who needed bilateral sinus floor augmentation for implant placement in the posterior maxillary area (based on CBCT) | Patients with poor general health, smokers or ex-smokers, alcoholics and drug addicts, irradiated patients, pregnancy, and bisphosphonate therapy Immunosuppressive drugs, blood platelet abnormalities, and chronic pain Patients with sinusitis or other pathology in the maxillary sinus With diabetes that is uncontrolled |
| Aoki et al., 2018 | Clinical Retrospective | Maxillary posterior tooth loss, good general health or manage medical conditions, implant placement by sinus floor elevation with PRF alone as the grafting material, informed consent granted, and follow-up visit performed at our facility following implant installation. | Not specified |
| Pichotano et al., 2018 | Case clinical report | One patient split-mouth, the patient reported no relevant medical history that could compromise bone healing, denied smoking, or used alcohol | Not specified |
| Nizam et al., 2018 | Prospective randomized clinical trial | Systemically healthy, age 21 years or older, implant therapy required in the bilateral posterior maxilla with a residual bone height of less than 5 mm, and periodontally healthy | Any systemic disease, use of any medications that could interfere with bone metabolism (i.e., corticosteroids, bisphosphonates), smoking, history of maxillary sinusitis or sinus surgery, history of reconstructive or previous implant surgery, and being edentulous for more than a year are all factors to consider. |
| Cömert Kılıç et al., 2017 | Randomized clinical trial | Age > 20 years, atrophic maxilla, previous posterior tooth loss, residual bone crest height = 7 mm or less on orthopantomography, and atrophic maxilla. | Had a maxillary sinus infection or hematologic, neurologic, or systemic problems, had radiotherapy or chemotherapy, had inflammatory or connective tissue illness, or had a malignant disease in the head and neck region. |
| Aoki et al., 2016 | A Clinical retrospective study | Case 1: good general health and non-smoker Case 2: no systemic pathology, smoker | Not specified |
| Gassling et al., 2013 | Randomized controlled study | Six healthy patients | Not specified |
| Tatullo et al., 2012 | Randomized clinical trial | A preoperative radiological and tomographic assessment revealed maxillary atrophy with a less than 5 mm remnant ridge. Due to toothlessness, anatomic-functional rehabilitation of the posterior maxilla is required. | Hemo-coagulative diseases Diabetes Incompetence/Immunological deficiency Previous head-neck radiation treatment Normal bone physiology anomalies Bisphosphonate-based treatments Smokers and ex-smokers would both be excluded |
| Zhang et al., 2012 | Clinical Study | Not specified | Blood platelet problems, aspirin therapy before surgery, viral and metabolic diseases, radiation, and acute and chronic maxillary sinus inflammation are all things to consider. |
| Toffler et al., 2010 | Clinical Study | Not specified | Not specified |
| Choukroun et al., 2006 | Histologic, clinical study | Thrombocyte concentrations in the blood are within normal limits, and there is no history of maxillary sinus irritation. Significant atrophy of the maxilla was discovered during the clinical examination and preoperative radiography. | Patients with immunologic disorders, uncontrolled diabetes, current chemo- or radiotherapy, or a history of drug misuse should not be considered. |
| Olgun et al., 2018 | Randomized clinical trial | Age ≥ 18 years Systemically healthy Non-smokers. Full-mouth plaque and bleeding score ≤15%; Presence of a residual crest height of <5 mm in the posterior maxilla as detected on X-rays. | Infectious and metabolic illnesses; Blood platelet abnormalities Chemotherapy or radiotherapy is still being administered. Chronic sinusitis in the maxillary sinuses is a common occurrence. Antibiotics and/or anti-inflammatory medicines are being taken. |
| Anitua et al., 2012 | Clinical Study | All patients in the research had severe alveolar atrophy and a class D residual bone height. | Any local or systemic disorders can make the treatment ineffective. Perforation of the Schneiderian membrane. |
| Selection | Comparability | Outcome | Total Score | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Adequate Definition of Patient Cases | Representatives of Patient Cases | Selection of Controls | Definition of Controls | Control for Important or Additional Factors (Max of 2X) | Ascertainment of Exposure | Was Follow-Up Long Enough for Outcomes to Occur | Adequacy of Follow Up | ||
| Kempraj et al., 2020 | X | X | X | X | XX | X | X | X | 9 |
| Aoki et al., 2018 | X | X | X | X | X | X | X | X | 8 |
| Pichotano et al., 2018 | X | X | XX | X | X | X | 7 | ||
| Nizam et al., 2018 | X | X | X | X | X | X | X | X | 8 |
| Aoki et al., 2016 | X | X | X | X | X | X | 6 | ||
| Zhang et al., 2012 | X | X | X | X | X | X | X | 7 | |
| Anitua et al., 2012 | X | X | X | X | X | X | X | 7 | |
| Toffler et al., 2010 | X | X | X | X | XX | X | 7 | ||
| Choukroun et al., 2006 | X | X | X | X | XX | X | X | X | 9 |
| Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias | |
|---|---|---|---|---|---|---|---|
| Cho et al. 2020 | + | ? | ? | ? | + | + | + |
| Pichotano et al. 2019 | + | + | ? | + | + | + | ? |
| Olgun et al. 2018 | + | + | ? | − | + | + | + |
| Cömert Kılıç et al. 2017 | + | ? | ? | + | + | + | + |
| Gassling et al. 2013 | + | + | ? | + | + | + | ? |
| Tatullo et al.. 2012 | + | ? | − | − | + | + | + |
| Author/Year | Follow-Up | Surgical Approach | Residual Bone Height |
|---|---|---|---|
| Kempraj et al., 2020 | 3 months over 2 years | Mid-crestal incision | Less than 4 mm |
| Cho et al., 2020 | 1 year | Trans-crestal sinus lift | Over 5 mm |
| Pichotano et al.,2019 | 4, 8 months, and at implant placement and loading (time not specified) | Lateral window | Less than 4 mm |
| Pichotano et al., 2018 | 10 months | Lateral window | Not reported |
| Olgun et al., 2018 | 1 year | Balloon-lift technique | Less than 5 mm |
| Nizam et al., 2018 | 12 months after implant loading (18 months) | Lateral window | 2.53 mm |
| Aoki et al., 2018 | Average 3.43 years (1–7 years) | 54 implants were placed by trans-crestal approach and 15 by the lateral approach | Ranged from 0.56 mm to 9.60 mm |
| Cömert Kılıç et al., 2017 | 18 months 6month after surgery 12 months after loading | Modified Caldwell-Luc | Not reported |
| Aoki et al., 2016 | 24 months | Trans-crestal | Pt#1 2.7 mm pt#2 less than 2 mm |
| Zhang et al.,2012 | 6 months | Lateral window | Less than 5 mm |
| Tatullo et al., 2012 | 8 months | Tatum’s technique (lateral window) | Less than 5 mm |
| Gassling et al., 2013 | 1 year follow up after implant placement (17 months) | Lateral window | Less than 5 mm |
| Anitua et al., 2012 | 33 months | Lateral window | Less than 3 mm |
| Toffler et al., 2010 | 1 year | Trans-crestal | 4 to 8 mm |
| Choukroun et al., 2006 | 8 months | Lateral window | Not reported |
| Author/Year | PRF Alone | PRF + Bone Substitute | Only Bone Substitute |
|---|---|---|---|
| Kempraj et al., 2020 | YES | PRF + BIO-OSS® | N/A |
| Cho et al., 2020 | YES | N/A | N/A |
| Pichotano et al., 2019 | NO | PRF + BIO-OSS® | BIO-OSS® |
| Pichotano et al., 2018 | NO | PRF + BIO-OSS® + COLLAGEN MEMBRANE | BIO-OSS® + COLLAGEN MEMBRANE |
| Olgun et al., 2018 | YES | N/A | N/A |
| Nizam et al., 2018 | NO | PRF + BIO-OSS® | BIO-OSS® |
| Aoki et al., 2018 | YES | N/A | N/A |
| Cömert Kılıç et al., 2017 | NO | PRF + β-TCP/PRP + β-TCP | β-TCP ALONE |
| Aoki et al., 2016 | YES | N/A | N/A |
| Gassling et al., 2013 | NO | PRF + CORTILOCANCELOUS BONE + BIO-OSS® | CORTILOCANCELOUS BONE + BIO-OSS® + COLLAGEN MEMBRANE |
| Zhang et al., 2012 | NO | PRF + BIO-OSS® | BIO-OSS® |
| Tatullo et al., 2012 | NO | PRF + BIO-OSS® | BIO-OSS® |
| Anitua et al., 2012 | NO | PRF + BIO-OSS® | BIO-OSS® |
| Toffler et al., 2010 | YES | N/A | N/A |
| Choukroun et al., 2006 | NO | PRF + FREEZE-DRIED BONE ALLOGRAFT | FREEZE-DRIED BONE ALLOGRAFT |
| Author | New Bone Formation |
|---|---|
| Kempraj et al., 2020 | PRF alone mean: 6.545 mm PRF + Bio-Oss® 12.636 mm |
| Cho et al., 2020 | 2.5 mm ± 1.2 mm (PRF) 1.7 ± 1.0 mm (control) |
| Pichotano et al., 2019 | PRF + DBBM 2.35 mm2 DBBM 1.58 mm2 |
| Pichotano et al., 2018 | Not reported |
| Olgun et al., 2018 | Test 16.58 mm (1.05) Control 17.28 mm (2.53) |
| Nizam et al., 2018 | Not reported |
| Aoki et al., 2018 | Not reported |
| Kılıç et al., 2017 | Mean of 33% in all groups |
| Aoki et al., 2016 | Not reported |
| Gassling et al., 2013 | PRF means 17% Collagen 17.2% |
| Zhang et al., 2012 | Test group 18.35% ± 6.62% Control group 12.95% ± 5.33% |
| Tatullo et al., 2012 | Not reported |
| Anitua et al., 2012 | 20–30% Test group 8% Control |
| Toffler et al., 2010 | Mean increase 3.5 mm (3.4–5 mm) |
| Choukroun et al., 2006 | Test group: 65% vital new bone 35% inert bone (4 months) Control group: 69% vital new bone 31% inert bone (8 months) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otero, A.I.P.; Fernandes, J.C.H.; Borges, T.; Nassani, L.; Castilho, R.d.M.; Fernandes, G.V.d.O. Sinus Lift Associated with Leucocyte-Platelet-Rich Fibrin (Second Generation) for Bone Gain: A Systematic Review. J. Clin. Med. 2022, 11, 1888. https://doi.org/10.3390/jcm11071888
Otero AIP, Fernandes JCH, Borges T, Nassani L, Castilho RdM, Fernandes GVdO. Sinus Lift Associated with Leucocyte-Platelet-Rich Fibrin (Second Generation) for Bone Gain: A Systematic Review. Journal of Clinical Medicine. 2022; 11(7):1888. https://doi.org/10.3390/jcm11071888
Chicago/Turabian StyleOtero, Ada Isis Pelaez, Juliana Campos Hasse Fernandes, Tiago Borges, Leonardo Nassani, Rogerio de Moraes Castilho, and Gustavo Vicentis de Oliveira Fernandes. 2022. "Sinus Lift Associated with Leucocyte-Platelet-Rich Fibrin (Second Generation) for Bone Gain: A Systematic Review" Journal of Clinical Medicine 11, no. 7: 1888. https://doi.org/10.3390/jcm11071888
APA StyleOtero, A. I. P., Fernandes, J. C. H., Borges, T., Nassani, L., Castilho, R. d. M., & Fernandes, G. V. d. O. (2022). Sinus Lift Associated with Leucocyte-Platelet-Rich Fibrin (Second Generation) for Bone Gain: A Systematic Review. Journal of Clinical Medicine, 11(7), 1888. https://doi.org/10.3390/jcm11071888