Abstract
Background: Study aims to demonstrate single-institution two decades experience with lateral transperitoneal laparoscopic adrenalectomies. Methods: Retrospective study involved 991 operations grouped into 4 cohorts. Data was collected on the patients’ age, sex, side and size of the lesion, histopathological type, hormonal activity, conversion to open adrenalectomy, operating time, length of hospital stay, perioperative complications. Results: The operations were right-sided (n = 550), left-sided (n = 422), bilateral (n = 19). Mean tumor size was 41.9 mm. Histopathological examination revealed 442 adenomas, 191 nodular hyperplasias, 218 pheochromocytomas, 33 malignancies and 126 other lesions. 541 patients had hormonally active tumors. Mean operating time for unilateral laparoscopic adrenalectomy was 141 min. Mean length of hospital stay was 5.27 days. Intraoperative complications rate was 2.3%. Conversion rate was 1.5%. 54 of patients had 70 postoperative complications. Reoperation rate was 1%. Mortality rate was 0.1%. Statistically significant differences were found in all factors, apart from age, sex, side and size of the lesion, reoperations rate (p > 0.05). Conversions rate, complications rates, length of hospital stay were highest in the first group (p < 0.05). Operating time shortened in the first decade. Conclusions: Laparoscopic adrenalectomy is a safe procedure with negligible mortality. Conversions rate, perioperative complications rate, and length of hospital stay, significantly decreased over time.
1. Introduction
Although adrenal pathologies are rare, they are increasingly found incidentally as part of investigations for non-related reasons [1,2,3]. A variety of surgical approaches have been described to treat adrenal tumors, including open, endoscopic (laparoscopic, retroperitoneoscopic) and robotic methods [4,5]. The first laparoscopic adrenalectomy via a lateral transperitoneal approach was reported by Gagner et al. in 1992 [6]. Since then, the method became the standard approach in adrenal surgery due to its safety and feasibility [4,5].
Adrenal operations are uncommon in general surgical practice and the European Society of Endocrine Surgeons recommended that adrenalectomies should be performed in high-volume centers and established a minimum of 6 operations per year for a single center [4].
Contemporary evidence base on laparoscopic adrenalectomy consists mainly of reports on small series of patients. Larger datasets are distinctive for multi-institutional and national reports [7,8]. The largest single-institution case studies involve 400 to 650 patients [3,9,10,11,12,13]. Many factors affecting perioperative outcomes are discussed in the literature. Apart from surgeon experience, they include size of the tumour, histopathological type, hormonal activity, side of the lesion, sex of the patient [8,9,10,11,12,13].
The aim of this study is to demonstrate our single-institution, single-surgeon experience which spans over two decades and includes almost 1000 laparoscopic adrenalectomies performed via a lateral transperitoneal approach. We particularly focused to analyze patient outcomes with relation to evolving experience of the surgeon.
2. Materials and Methods
We retrospectively reviewed 991 laparoscopic adrenalectomies performed at a single academic medical center (Department of General, Vascular and Transplant Surgery, Medical University of Warsaw) between October 1997 to September 2017. Local Bioethics Committee approval for this research was obtained. All patients signed a written patients’ informed consent form for the operation.
Prior to surgery, all patients underwent endocrinological and anaesthesiological assessment. Pre-operative workup included hormonal evaluation and imaging (computed tomography, magnetic resonance imagery or positron emission tomography in selected cases), as well as pharmacological preparation when indicated.
Indications to laparoscopic adrenalectomy included: (1) hormonally active tumor measuring <80 mm in diameter on imaging, (2) non-functioning benign tumor measuring 40–80 mm in diameter, (3) non-functioning benign tumor measuring <40 mm in diameter, if rapid growth, focal changes of density, irregular shape or high density on Computed Tomography scans were observed, (4) metastases measuring <80 mm in diameter. Patients with tumors measuring >80 mm in diameter (hormonally active and non-functioning tumors, as well as metastases), primary malignant tumors, or if reoperation was needed, were offered open adrenalectomy. Patient who had non-functioning benign tumors measuring <40 mm in diameter were observed.
All operations were performed by the same primary surgeon (Prof. Maciej Otto) and his team via the lateral transperitoneal approach. The surgical method has been described previously by our team [14,15]. Open adrenalectomies were not analyzed in this study. Neither retroperitoneoscopic approach nor robotic method were implemented in our center and thus are not included in this report.
In order to control for the operating surgeon’s increasing experience, the patients were grouped into 4 equal cohorts depending on when they underwent the procedure. Each cohort contained a consecutive number of patients with the first cohort representing the earliest cases and the last cohort representing the latest cases in the study period. The time periods for each group are defined in Table 1 and Table 2.

Table 1.
Patient and tumor characteristics.
Table 2.
Perioperative outcomes.
Data were collected on the patients’ age, sex, side and size of the lesion, histopathological type, hormonal activity, conversion to open adrenalectomy, operating time, length of hospital stay, intra- and postoperative complications, reoperations, and mortality. The tumor size was obtained from the histopathology report. Operating time was measured from skin incision to skin closure. The postoperative complications were categorized using the Clavien-Dindo classification system [16].
Patients who underwent bilateral and adrenal-sparing laparoscopic adrenalectomy were included in the study, although they were excluded from the analysis of operating time. Patients who required conversion to open adrenalectomy or additional elective procedure performed (e.g., hernia repair/cholecystectomy) were also excluded from the analysis of operating time.
Statistical Analysis
The data were collected and stored using Microsoft Excel. Continuous variables were expressed as the mean, standard deviation (SD). Chi-square test and ANOVA were used to compare differences between the groups. Statistical significance was set at p-value < 0.05. Data were analyzed using STATISTICA 13.0 software.
3. Results
3.1. Patient and Tumor Characteristics
The study included a total of 991 laparoscopic adrenalectomies. Patient and tumor characteristics are summarized in Table 1. The mean (SD) age of the patients was 53 (14) years; n = 682 (68.8%) of the patients were female. With regards to the laterality, n = 550 had a right sided, and n = 422 had a left sided adrenalectomy. Bilateral adrenalectomy was performed in n = 19 patients. In 39 cases, an additional procedure was performed (cholecystectomy n = 29, hernia repair n = 10) concomitantly, during the same anesthetic time. The adrenal sparing procedure was performed in 21 patients. The mean (SD) size of the removed lesion was 41.9 (20) mm, range from 6 to 130 mm. Histopathological examination revealed 442 adenomas, 191 nodular hyperplasias, 218 pheochromocytomas, 33 malignancies and 126 other lesions. In all patients requiring bilateral adrenalectomies, tumors were histologically the same on both sides. Non-functioning lesions were identified in 450 patients, while 541 patients had hormones secreting lesions (n = 208 had catecholamine, n = 210 cortisol, n = 110 aldosterone, and n = 13 androgen).
3.2. Perioperative Data
Perioperative outcomes are outlined in Table 2. The mean (SD) operating time for unilateral laparoscopic adrenalectomy was 141 (47.1) min, range from 55 to 530 min. The mean (SD) length of hospital stay was 5.27 (4.68) days, range from 2 to 102 days. There were 23 (2.3%) intraoperative complications, with intraoperative bleeding being the most frequent one. Conversion to open adrenalectomy was performed in 15 (1.5%) patients. Indications for conversion are described in Table 3. Within the cohort, 54 (5.4%) patients experienced 70 postoperative complications. Postoperative blood transfusion was required in 41 patients (Clavien–Dindo = 2). Return to theatre was recorded in 10 patients, n = 7 cases had postoperative bleeding or hematoma, while n = 1 had a trocar-site herniation of the omentum, pancreatic fistula, and peritonitis each. Severe complications (Clavien–Dindo ≥ 3) were recorded in 1.6% of cases. Mortality was recorded in one patient (0.1%). A 73-year-old female with Cushing’s syndrome underwent right-sided laparoscopic adrenalectomy and was reoperated due to coagulopathy and bleeding (splenectomy was required). Postoperatively patient was hemodynamically unstable and required intensive care. Subsequently, another operation was carried out for peripancreatic fluid collection. Patient died due to multiorgan failure.
Table 3.
Indications for conversion to open surgery.
3.3. Evolution of Surgical Practice over Time
In the first year of practice, 3 cases were recorded. The number of operations was gradually increasing over time, and since 2002, 40–77 laparoscopic adrenalectomies were performed each year. The annual number of operations is shown in Figure 1.
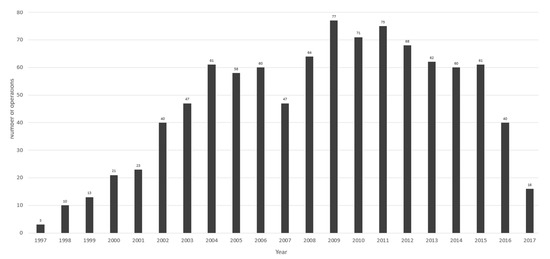
Figure 1.
Annual number of operations.
When comparing each cohort, there were no statistically significant differences between each group in terms of patient age, sex, side of lesion, size of lesion, reoperations rate (Table 1 and Table 2).
The mean operating time of unilateral laparoscopic adrenalectomy was longest in group 1 (154 min) and shortest in group 2 (122 min). In group 3 and 4 the mean operating time was 138 min and 153 min, respectively (p < 0.0001) (Table 2). The operating time was found gradually shorter in the first decade (groups 1, 2 and partially group 3) and then reached a plateau in the second decade (Figure 2). Conversions rate, intraoperative and postoperative complications rates as well as length of hospital stay were highest in the first group and significantly decreased in groups 2–4 (Table 2). There were 11 conversions in the first group, and reduced to two conversions in the second group and to one conversions in the subsequent groups (p = 0.0002). In addition, based on a view of annual performance, there is a reduction in conversion rate over time (Figure 3). Intraoperative complications developed in 11 cases in the first group and reduced to 4 cases in groups 2–4 (p = 0.002). The number of postoperative complications in groups 1–4 was 47, 5, 5, 13, respectively (p < 0.0001). Mean length of hospital stay decreased from 7 days in the first group to 4.8 and 4.6 days in groups 2–4 (p < 0.0001). The number of patients who underwent an adrenal sparing procedures significantly increased over time from one procedure in the first group to 9 procedures in the last group (p = 0.034) (Table 1).
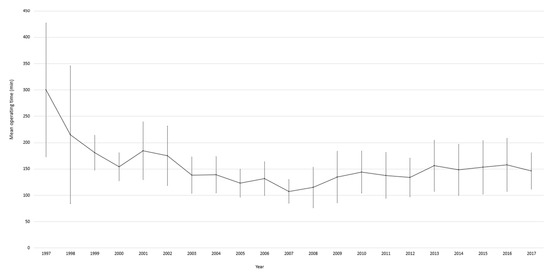
Figure 2.
Annual mean operating time of unilateral laparoscopic adrenalectomy (excluded: bilateral adrenalectomies, conversion to open surgery, adrenal-sparing procedures, additional procedures performed).
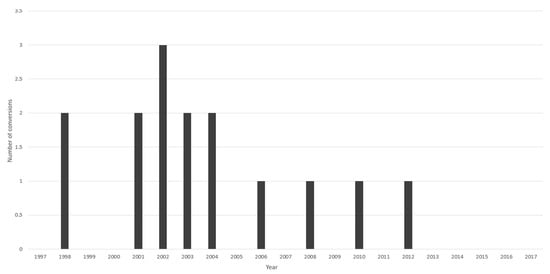
Figure 3.
Annual number of conversions to open surgery.
4. Discussion
This study presents an analysis of almost 1000 laparoscopic adrenalectomies via lateral transperitoneal approach performed by a single surgeon over the 20 years. This is the largest published series describing experience with laparoscopic adrenalectomy in a single institution. Our study demonstrates an overall low rate of perioperative complications and a negligible mortality rate following laparoscopic adrenalectomy. Moreover, complications rate was demonstrated to reduce gradually over time and operating time was gradually reduced in the first decade of practice before reaching a plateau. The length of hospital stays also significantly decreased over time.
As a high-volume, national referral center, our institution performs about 50 laparoscopic adrenalectomies per year. It is in line with the consensus statement of the European Society of Endocrine Surgeons, stating that adrenal surgery should be performed in departments with at least 6 adrenalectomies per year, and at least 12 adrenalectomies per year—for management of adrenocortical cancer [4].
When comparing groups with regards to the tumor characteristics, we found statistically significant differences in histopathological type and hormonal activity (Table 1). The differences result from a small number of patients with malignant lesions and androgen-secreting tumors compared to other types, respectively.
There is controversy regarding the safety and feasibility of laparoscopic adrenalectomy as management for malignant lesions. The European guidelines recommend the open method as a standard technique [5,17]. In our center, suspected primarily malignant lesions as well as metastatic lesions measuring >80 mm in diameter, in preoperative assessment are managed with an open operation. In our series, the number of lesions found to be malignant during histopathological examination decreased over the study period, likely due to improvements in preoperative diagnostic tools [3,18]. Pędziwiatr et al., based on experience with 500 laparoscopic adrenalectomies, reported that the laparoscopic method can be a good alternative to open resection for the treatment of malignant adrenal tumors, when performed by an experienced team [10].
The mean operating time of unilateral laparoscopic adrenalectomy in our series was 141 min and decreased with increasing surgeon experience. In the literature, the mean operating time is reported to be between 83 and 240 min [3,7,8,9,10,11,12,13,19,20,21,22,23,24,25]. Apart from the operating surgeons’ experience, other factors may affect operating time and include: patient sex, obesity, tumor size, and presence of malignancy [10,19,25].
The overall rate of conversion to open surgery in our series was 1.5% and was significantly decreased over time. Other authors reported conversion rate ranging from 0.8% to 6.2%, although in majority of publications the conversion rate was more than 3.5% [3,8,9,10,12,13,19,20,21,22,25]. In our study, the most common indication for conversion to open surgery was suspicion of incomplete tumor resection and suspicion of malignancy (e.g., inferior vena cava infiltration). In a group of patients requiring conversion, the most common pathology was pheochromocytoma (60%) followed by malignancy (20%). Size could also be an important risk factor for conversion to open adrenalectomy, as mean size of the tumor requiring conversion in our series was 52 mm, whereas overall mean size of the removed tumor was 41.9 mm. Right sided tumors constituted 73% of all tumors requiring conversion to open adrenalectomy in our series. Factors defined as increasing risk for conversion vary in the literature, and involve pheochromocytoma, tumor size measuring > 50–80 mm, Body Mass Index > 24 kg/m2 [12,22,25,26].
Many authors have used Clavien–Dindo classification to describe the complication rates of laparoscopic adrenalectomy. The average rate of perioperative complications of laparoscopic adrenalectomy reported in the literature ranges from 0 to 15.5%, with bleeding being the most frequent one [3,7,8,9,10,11,12,13,20,21,22,23,25]. Postoperative complications occurred in 5.4% of patients in our study. The complications rate was found to reduce gradually over time, concomitant to the operating surgeon’s increasing experience. Within our patients, complications occur most frequently in patients who had pheochromocytoma and cortisol—secreting tumors. Battistella et al., in their 35 years of experience with 520 adrenalectomies reported zero peri-operative complications at 30-days and concluded that patients requiring adrenalectomy should be treated only in experienced centers [3]. Other authors report that factors associated with development of perioperative complications include: tumor size > 60 mm, American Society of Anesthesiology (ASA) class 3 or 4, presence of pheochromocytoma or cortisol-secreting adenoma, conversion to open/hand-assisted operation, and left-sided tumors [12,13,25].
The overall mean length of hospital stay in our series was 5.27 days. When comparing the groups with regards to when they were performed, the length of stay gradually reduced from 7 days in the earliest cohort to 4.6 days in the most recent cohort. In the literature, mean length of hospital stays range between 1 and 12 days [3,7,8,9,10,11,12,13,14,20,21,22,23,25]. Factors associated with prolonged length of stay, discussed in the literature, include presence of postoperative complications, day of the week of operation (Thursday or Friday), use of drainage, pheochromocytoma, specimen size > 90 mm, age > 65 years, bilateral adrenalectomy, (ASA) class 3 or 4 [13,25,27,28].
The mortality rate in our series was 0.1%—this is comparable to other centers which quote a mortality ranging from 0% to 0.8%, emphasizing the overall safety of the laparoscopic adrenalectomy [9,10,13,22,23].
Limitations of this study are mostly related to its observational retrospective nature, as well as all operations being performed by the single surgeon and his team. Our Department is a national referral center. Postoperatively, many patients were followed up in their local hospitals, so our long term follow up data is partially incomplete and long-term outcomes were not analyzed. Another limitation is lack of data about the type of surgical equipment used during each operation. Development of technology over the two decades of practice could influence the outcomes. Moreover, information about the exact volume of intraoperative blood loss, Body Mass Index were not documented in available operating records.
5. Conclusions
This large single-center case series adds to the existing body of evidence on laparoscopic approach to adrenalectomy. Our data supports the safety and feasibility of the procedure and extends the evidence that laparoscopic adrenalectomy is a safe procedure with negligible mortality. Conversion and perioperative complication rate as well as length of hospital stay significantly decrease over time with increasing surgeon and institutional experience and excellent cooperation with endocrine and anesthesiology teams in perioperative care of patients undergoing laparoscopic adrenalectomy. We think that some lengthening of the operation time is acceptable if performed in order to achieve higher quality of surgery, reduce complications rate, maintain oncological margins and avoid conversion. Based on our material where all operations were performed by the same primary surgeon and his team, we can also conclude that gaining mastery in adrenalectomy can be very beneficial to the patients as above can assure very good outcomes.
Author Contributions
Conceptualization, M.D., J.D., J.S. and S.N.; methodology, M.D., J.D., J.S. and S.N.; formal analysis, M.D. and J.S.; data curation, M.D. and J.D.; writing—original draft preparation, M.D.; writing—review and editing, M.D., J.D., J.S. and S.N.; visualization, M.D. and J.S.; supervision, S.N.; project administration, M.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Medical University of Warsaw (protocol code AKBE/65/2019 and date of 18 February 2019).
Informed Consent Statement
Informed consent for operation was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to pay respect to Maciej Otto and his whole life work dedicated to patients with adrenal tumours.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hanna, F.W.F.; Hancock, S.; George, C.; Clark, A.; Sim, J.; Issa, B.G.; Powner, G.; Waldron, J.; Duff, C.J.; Lea, S.C.; et al. Adrenal Incidentaloma: Prevalence and Referral Patterns from Routine Practice in a Large UK University Teaching Hospital. J. Endocr. Soc. 2021, 6, bvab180. [Google Scholar] [CrossRef] [PubMed]
- Cyranska-Chyrek, E.; Szczepanek-Parulska, E.; Olejarz, M.; Ruchala, M. Malignancy Risk and Hormonal Activity of Adrenal Incidentalomas in a Large Cohort of Patients from a Single Tertiary Reference Center. Int. J. Environ. Res. Public Health 2019, 16, 1872. [Google Scholar] [CrossRef] [PubMed]
- Battistella, E.; Ferrari, S.; Pomba, L.; Toniato, A. Adrenal surgery: Review of 35 years experience in a single centre. Surg. Oncol. 2021, 37, 101554. [Google Scholar] [CrossRef] [PubMed]
- Mihai, R.; Donatini, G.; Vidal, O.; Brunaud, L. Volume-outcome correlation in adrenal surgery-an ESES consensus statement. Langenbecks Arch. Surg. 2019, 404, 795–806. [Google Scholar] [CrossRef] [PubMed]
- Stefanidis, D.; Goldfarb, M.; Kercher, K.W.; Hope, W.W.; Richardson, W.; Fanelli, R.D. SAGES guidelines for minimally invasive treatment of adrenal pathology. Surg. Endosc. 2013, 27, 3960–3980. [Google Scholar] [CrossRef]
- Gagner, M.; Lacroix, A.; Bolté, E. Laparoscopic adrenalectomy in Cushing’s syndrome and pheochromocytoma. N. Engl. J. Med. 1992, 327, 1033. [Google Scholar] [CrossRef]
- Eichhorn-Wharry, L.I.; Talpos, G.B.; Rubinfeld, I. Laparoscopic versus open adrenalectomy: Another look at outcome using the Clavien classification system. Surgery 2012, 152, 1090–1095. [Google Scholar] [CrossRef]
- Alberici, L.; Paganini, A.M.; Ricci, C.; Balla, A.; Ballarini, Z.; Ortenzi, M.; Casole, G.; Quaresima, S.; Di Dalmazi, G.; Ursi, P.; et al. Development and validation of a preoperative “difficulty score” for laparoscopic transabdominal adrenalectomy: A multicenter retrospective study. Surg. Endosc. 2021, 36, 3549–3557. [Google Scholar] [CrossRef]
- Coste, T.; Caiazzo, R.; Torres, F.; Vantyghem, M.-C.; Carnaille, B.; Pattou, F.; Cao, C.D.; Douillard, C. Laparoscopic adrenalectomy by transabdominal lateral approach: 20 years of experience. Surg. Endosc. 2017, 31, 2743–2751. [Google Scholar] [CrossRef]
- Pędziwiatr, M.; Wierdak, M.; Ostachowski, M.; Natkaniec, M.; Białas, M.; Hubalewska-Dydejczyk, A.; Matłok, M.; Major, P.; Budzyński, P.; Migaczewski, M.; et al. Single center outcomes of laparoscopic transperitoneal lateral adrenalectomy—Lessons learned after 500 cases: A retrospective cohort study. Int. J. Surg. 2015, 20, 88–94. [Google Scholar] [CrossRef]
- Goitein, D.; Mintz, Y.; Gross, D.; Reissman, P. Laparoscopic adrenalectomy: Ascending the learning curve. Surg. Endosc. 2004, 18, 771–773. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gaujoux, S.; Bonnet, S.; Leconte, M.; Zohar, S.; Bertherat, J.; Bertagna, X.; Dousset, B. Risk factors for conversion and complications after unilateral laparoscopic adrenalectomy. Br. J. Surg. 2011, 98, 1392–1399. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Scholten, A.; Chomsky-Higgins, K.; Nwaogu, I.; Gosnell, J.E.; Seib, C.; Shen, W.T.; Suh, I.; Duh, Q.-Y. Risk Factors Associated with Perioperative Complications and Prolonged Length of Stay After Laparoscopic Adrenalectomy. JAMA Surg. 2018, 153, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Otto, M.; Szostek, G.; Nazarewski, S.; Borkowski, T.; Chudzinski, W.; Tolloczko, T. Laparoscopic operative technique for adrenal tumors. JSLS 2000, 4, 125–129. [Google Scholar] [PubMed]
- Otto, M.; Dzwonkowski, J.; Jędrasik, M.; Ciąćka, T.; Górnicka, B.; Życińska, K.; Szmidt, J. Qualification and Operative Difficulties of Laparoscopic Adrenalectomy. Pol. J. Surg. 2010, 82, 38–46. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Gaujoux, S.; Mihai, R.; joint working group of ESES and ENSAT. European Society of Endocrine Surgeons (ESES) and European Network for the Study of Adrenal Tumours (ENSAT) recommendations for the surgical management of adrenocortical carcinoma. Br. J. Surg. 2017, 104, 358–376. [Google Scholar] [CrossRef]
- Bednarczuk, T.; Bolanowski, M.; Sworczak, K.; Górnicka, B.; Cieszanowski, A.; Otto, M.; Ambroziak, U.; Pachucki, J.; Kubicka, E.; Babińska, A.; et al. Adrenal incidentaloma in adults—Management recommendations by the Polish Society of Endocrinology. Endokrynol. Pol. 2016, 67, 234–258. [Google Scholar] [CrossRef]
- Natkaniec, M.; Dworak, J.; Pędziwiatr, M.; Pisarska, M.; Major, P.; Dembiński, M.; Winiarski, M.; Budzyński, A. Patients criteria determining difficulty of the laparoscopic lateral transperitoneal adrenalectomy. A retrospective cohort study. Int. J. Surg. 2017, 43, 33–37. [Google Scholar] [CrossRef]
- Conzo, G.; Gambardella, C.; Candela, G.; Sanguinetti, A.; Polistena, A.; Clarizia, G.; Patrone, R.; Di Capua, F.; Offi, C.; Musella, M.; et al. Single center experience with laparoscopic adrenalectomy on a large clinical series. BMC Surg. 2018, 18, 2. [Google Scholar] [CrossRef]
- Gumbs, A.A.; Gagner, M. Laparoscopic adrenalectomy. Best Pract. Res. Clin. Endocrinol. Metab. 2006, 20, 483–499. [Google Scholar] [CrossRef] [PubMed]
- Bittner, J.G., 4th; Gershuni, V.M.; Matthews, B.D.; Moley, J.F.; Brunt, L.M. Risk factors affecting operative approach, conversion, and morbidity for adrenalectomy: A single-institution series of 402 patients. Surg. Endosc. 2013, 27, 2342–2350. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.K.; Natarajan, B.; Pallati, P.K.; Gupta, H.; Sainath, J.; Fitzgibbons, R.J. Outcomes after laparoscopic adrenalectomy. Surg. Endosc. 2011, 25, 784–794. [Google Scholar] [CrossRef] [PubMed]
- Eto, M.; Harano, M.; Koga, H.; Tanaka, M.; Naito, S. Clinical outcomes and learning curve of a laparoscopic adrenalectomy in 103 consecutive cases at a single institute. Int. J. Urol. 2006, 13, 671–676. [Google Scholar] [CrossRef]
- Economopoulos, K.P.; Phitayakorn, R.; Lubitz, C.C.; Sadow, P.M.; Parangi, S.; Stephen, A.E.; Hodin, R.A. Should specific patient clinical characteristics discourage adrenal surgeons from performing laparoscopic transperitoneal adrenalectomy? Surgery 2016, 159, 240–248. [Google Scholar] [CrossRef]
- Shen, Z.J.; Chen, S.W.; Wang, S.; Jin, X.D.; Chen, J.; Zhu, Y.; Zhang, R.M. Predictive factors for open conversion of laparoscopic adrenalectomy: A 13-year review of 456 cases. J. Endourol. 2007, 21, 1333–1337. [Google Scholar] [CrossRef]
- Pisarska, M.; Dworak, J.; Natkaniec, M.; Małczak, P.; Przęczek, K.; Wysocki, M.; Major, P.; Radkowiak, D.; Budzyński, A.; Pędziwiatr, M. Risk factors for prolonged hospitalization in patients undergoing laparoscopic adrenalectomy. Videosurg. Other Miniinvasive Tech. 2018, 13, 141–147. [Google Scholar] [CrossRef]
- Rodríguez-Hermosa, J.I.; Delisau, O.; Planellas-Giné, P.; Cornejo, L.; Ranea, A.; Maldonado, E.; Fernández-Real, J.M.; Codina-Cazador, A. Factors associated with prolonged hospital stay after laparoscopic adrenalectomy. Updates Surg. 2021, 73, 693–702. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).