
Addressing the Helper’s and Victim’s Gender Is Crucial in Schoolchildren Resuscitation Training—A Prospective, Educative Interventional Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Trial Registration
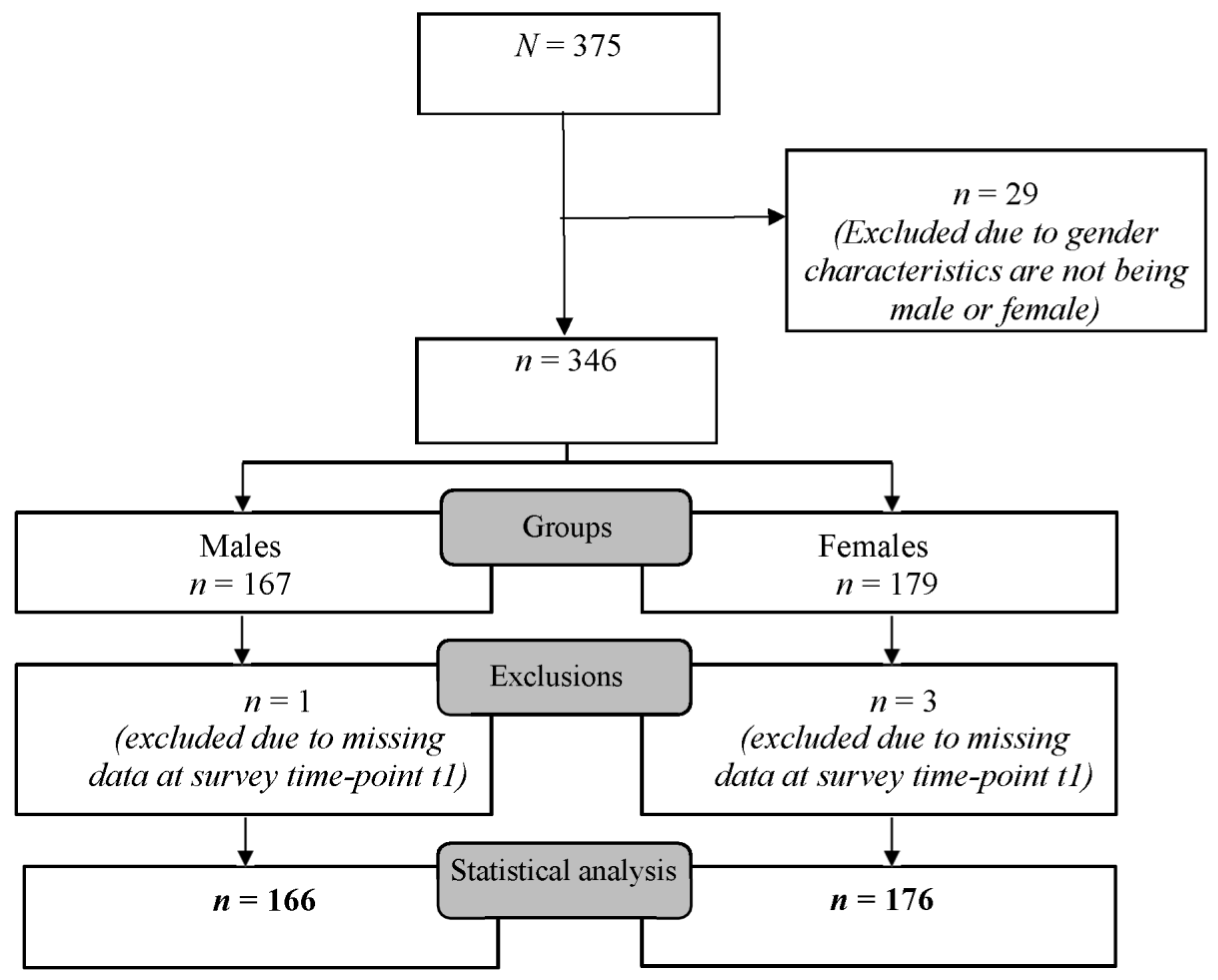
2.3. Study Population
2.4. Questionnaire
2.5. Intervention
2.6. Statistical Analysis
3. Results
3.1. Influence of Schoolchildren’s Gender on Their CPR Willingness
3.2. Influence of OHCA Victims’ Gender on the Willingness to Perform CPR in Schoolchildren before and after CPR Training
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CPR | Cardiopulmonary resuscitation |
| FG | Female group |
| MG | Male group |
| OHCA | Out-of-hospital cardiac arrest |
References
- Gräsner, J.T.; Lefering, R.; Koster, R.W.; Masterson, S.; Böttiger, B.W.; Herlitz, J.; Wnent, J.; Tjelmeland, I.B.; Ortiz, F.R.; Maurer, H.; et al. EuReCa ONE-27 Nations, ONE Europe, ONE Registry: A prospective one month analysis of out-of-hospital cardiac arrest outcomes in 27 countries in Europe. Resuscitation 2016, 105, 188–195. [Google Scholar] [CrossRef] [Green Version]
- Holmberg, M.; Holmberg, S.; Herlitz, J.; Swedish Cardiac Arrest, R. Factors modifying the effect of bystander cardiopulmonary resuscitation on survival in out-of-hospital cardiac arrest patients in Sweden. Eur. Heart J. 2001, 22, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, T.D.; Roe, D.J.; Cretin, S.; Spaite, D.W.; Larsen, M.P. Estimating effectiveness of cardiac arrest interventions: A logistic regression survival model. Circulation 1997, 96, 3308–3313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gräsner, J.T.; Wnent, J.; Herlitz, J.; Perkins, G.D.; Lefering, R.; Tjelmeland, I.; Koster, R.W.; Masterson, S.; Rossell-Ortiz, F.; Maurer, H.; et al. Survival after out-of-hospital cardiac arrest in Europe—Results of the EuReCa TWO study. Resuscitation 2020, 148, 218–226. [Google Scholar] [CrossRef]
- Kragholm, K.; Wissenberg, M.; Mortensen, R.N.; Fonager, K.; Jensen, S.E.; Rajan, S.; Lippert, F.K.; Christensen, E.F.; Hansen, P.A.; Lang-Jensen, T.; et al. Return to Work in Out-of-Hospital Cardiac Arrest Survivors: A Nationwide Register-Based Follow-Up Study. Circulation 2015, 131, 1682–1690. [Google Scholar] [CrossRef]
- Kragholm, K.; Wissenberg, M.; Mortensen, R.N.; Hansen, S.M.; Malta Hansen, C.; Thorsteinsson, K.; Rajan, S.; Lippert, F.; Folke, F.; Gislason, G.; et al. Bystander Efforts and 1-Year Outcomes in Out-of-Hospital Cardiac Arrest. N. Engl. J. Med. 2017, 376, 1737–1747. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.M.; Kragholm, K.; Pearson, D.A.; Tyson, C.; Monk, L.; Myers, B.; Nelson, D.; Dupre, M.E.; Fosbøl, E.L.; Jollis, J.G.; et al. Association of Bystander and First-Responder Intervention with Survival after Out-of-Hospital Cardiac Arrest in North Carolina, 2010–2013. JAMA 2015, 314, 255–264. [Google Scholar] [CrossRef]
- Greif, R.; Lockey, A.; Breckwoldt, J.; Carmona, F.; Conaghan, P.; Kuzovlev, A.; Pflanzl-Knizacek, L.; Sari, F.; Shammet, S.; Scapigliati, A.; et al. European Resuscitation Council Guidelines 2021: Education for resuscitation. Resuscitation 2021, 161, 388–407. [Google Scholar] [CrossRef] [PubMed]
- Böttiger, B.W.; Van Aken, H. Kids save lives—Training school children in cardiopulmonary resuscitation worldwide is now endorsed by the World Health Organization (WHO). Resuscitation 2015, 94, A5–A7. [Google Scholar] [CrossRef]
- Isbye, D.L.; Rasmussen, L.S.; Ringsted, C.; Lippert, F.K. Disseminating cardiopulmonary resuscitation training by distributing 35,000 personal manikins among school children. Circulation 2007, 116, 1380–1385. [Google Scholar] [CrossRef] [PubMed]
- Bohn, A.; Van Aken, H.K.; Möllhoff, T.; Wienzek, H.; Kimmeyer, P.; Wild, E.; Döpker, S.; Lukas, R.P.; Weber, T.P. Teaching resuscitation in schools: Annual tuition by trained teachers is effective starting at age 10. A four-year prospective cohort study. Resuscitation 2012, 83, 619–625. [Google Scholar] [CrossRef]
- Lukas, R.P.; Van Aken, H.; Mölhoff, T.; Weber, T.; Rammert, M.; Wild, E.; Bohn, A. Kids save lives: A six-year longitudinal study of schoolchildren learning cardiopulmonary resuscitation: Who should do the teaching and will the effects last? Resuscitation 2016, 101, 35–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abelairas-Gomez, C.; Rodriguez-Nunez, A.; Casillas-Cabana, M.; Romo-Perez, V.; Barcala-Furelos, R. Schoolchildren as life savers: At what age do they become strong enough? Resuscitation 2014, 85, 814–819. [Google Scholar] [CrossRef]
- Böttiger, B.W.; Bossaert, L.L.; Castrén, M.; Cimpoesu, D.; Georgiou, M.; Greif, R.; Grünfeld, M.; Lockey, A.; Lott, C.; Maconochie, I.; et al. Kids Save Lives—ERC position statement on school children education in CPR.: “Hands that help—Training children is training for life”. Resuscitation 2016, 105, A1–A3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semeraro, F.; Greif, R.; Böttiger, B.W.; Burkart, R.; Cimpoesu, D.; Georgiou, M.; Yeung, J.; Lippert, F.; Lockey, A.S.; Olasveengen, T.M.; et al. European Resuscitation Council Guidelines 2021: Systems saving lives. Resuscitation 2021, 161, 80–97. [Google Scholar] [CrossRef]
- Wingen, S.; Schroeder, D.C.; Ecker, H.; Steinhauser, S.; Altin, S.; Stock, S.; Lechleuthner, A.; Hohn, A.; Böttiger, B.W. Self-confidence and level of knowledge after cardiopulmonary resuscitation training in 14 to 18-year-old schoolchildren: A randomised-interventional controlled study in secondary schools in Germany. Eur. J. Anaesthesiol. 2018, 35, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Blom, M.T.; Oving, I.; Berdowski, J.; van Valkengoed, I.G.M.; Bardai, A.; Tan, H.L. Women have lower chances than men to be resuscitated and survive out-of-hospital cardiac arrest. Eur. Heart J. 2019, 40, 3824–3834. [Google Scholar] [CrossRef] [PubMed]
- Finke, S.R.; Schroeder, D.C.; Ecker, H.; Wingen, S.; Hinkelbein, J.; Wetsch, W.A.; Köhler, D.; Böttiger, B.W. Gender aspects in cardiopulmonary resuscitation by schoolchildren: A systematic review. Resuscitation 2018, 125, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Perman, S.M.; Shelton, S.K.; Knoepke, C.; Rappaport, K.; Matlock, D.D.; Adelgais, K.; Havranek, E.P.; Daugherty, S.L. Public Perceptions on Why Women Receive Less Bystander Cardiopulmonary Resuscitation Than Men in Out-of-Hospital Cardiac Arrest. Circulation 2019, 139, 1060–1068. [Google Scholar] [CrossRef]
- Kanstad, B.K.; Nilsen, S.A.; Fredriksen, K. CPR knowledge and attitude to performing bystander CPR among secondary school students in Norway. Resuscitation 2011, 82, 1053–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greif, R.; Lockey, A.S.; Conaghan, P.; Lippert, A.; De Vries, W.; Monsieurs, K.G.; Ballance, J.H.; Barelli, A.; Biarent, D.; Bossaert, L.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 10. Education and implementation of resuscitation. Resuscitation 2015, 95, 288–301. [Google Scholar] [CrossRef] [Green Version]
- German Resuscitation Council. Recommended Curriculum to Teach and Train Resuscitation to School Children in Germany. Available online: https://www.grc-org.de/downloads/GRC-school_curriculum_ATEE_12-10_JB.pdf (accessed on 17 February 2022).
- Pivač, S.; Skela-Savič, B.; Gradišek, P. Effects of Cardiopulmonary Resuscitation with Automated External Defibrillator Training among Schoolchildren in Slovenia: A Pre- and Post-test Cohort Study. Zdr Varst. 2021, 60, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Blewer, A.L.; Ibrahim, S.A.; Leary, M.; Dutwin, D.; McNally, B.; Anderson, M.L.; Morrison, L.J.; Aufderheide, T.P.; Daya, M.; Idris, A.H.; et al. Cardiopulmonary Resuscitation Training Disparities in the United States. J. Am. Heart Assoc. 2017, 6, e006124. [Google Scholar] [CrossRef] [PubMed]
- Mosca, L.; Mochari-Greenberger, H.; Dolor, R.J.; Newby, L.K.; Robb, K.J. Twelve-year follow-up of American women’s awareness of cardiovascular disease risk and barriers to heart health. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 120–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, C.E.; Wilkins, M.S.; Davies, J.M.; Caird, J.K.; Hallihan, G.M. Does the sex of a simulated patient affect CPR? Resuscitation 2015, 86, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Rücker, G.; Salomon Holtz, A.; Scharr, G.; Podbielski, A.; Devide, A. Current Test Results of Resuscitation Manikins Suitable for School Classes: Rostocker Simulationsanlage und Notfallausbildungszentrum (RoSaNa). Available online: https://rosana.med.uni-rostock.de/index.php?id=486 (accessed on 17 February 2022).
- Schroeder, D.C.; Ecker, H.; Wingen, S.; Semeraro, F.; Böttiger, B.W. “Kids Save Lives”-resuscitation training for schoolchildren: Systematic review. Anaesthesist 2017, 66, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Wingen, S.; Jeck, J.; Schroeder, D.C.; Wingen-Heimann, S.M.; Drost, R.; Böttiger, B.W. Facilitators and barriers for the implementation of resuscitation training programmes for schoolchildren: A systematic review. Eur. J. Anaesthesiol. 2021. [Google Scholar] [CrossRef]

{kind=link}
| Schoolchildren’s Characteristics | Sum | Male Group | Female Group | p-Value |
|---|---|---|---|---|
| Sex n = 342 | n (%) 342 (100.0) | n (%) 166 (48.5) | n (%) 176 (51.5) | |
| Age Median (IQR25–75) n = 342 | 12 (11–13) n (%) | 12 (11–13) n (%) | 12 (11–13) n (%) | 0.531 1 |
| 10 | 29 (8.5) | 12 (7.2) | 17 (9.7) | |
| 11 | 95 (27.8) | 54 (32.5) | 41 (23.2) | |
| 12 | 107 (31.3) | 48 (28.9) | 59 (33.5) | |
| 13 | 96 (28.1) | 43 (25.9) | 53 (30.1) | |
| 14 | 14 (4.1) | 8 (4.8) | 6 (3.4) | |
| 15 | 1 (0.3) | 1 (0.6) | 0 (0.0) | |
| Pre-knowledge in first aid n = 338 | 0.564 2 | |||
| Yes | 198 (58.6) | 95 (58.3) | 103 (58.9) | |
| No | 140 (41.4) | 68 (41.7) | 72 (41.1) | |
| Training method n = 342 | 0.833 2 | |||
| e-learning | 233 (68.1) | 114 (68.7) | 119 (67.6) | |
| Face-to-face | 109 (31.9) | 52 (31.3) | 57 (32.4) |
| Male Group n (%) | Female Group n (%) | p-Value | |
|---|---|---|---|
| n = 337 | 163 (48.4) | 174 (51.6) | |
| General CPR willingness (baseline; t0) | 0.0111,* | ||
| Yes | 145 (89.0) | 169 (97.1) | |
| No | 18 (11.0) | 5 (2.9) | |
| General CPR willingness (after training; t1) | 0.0381,* | ||
| Yes | 156 (95.7) | 172 (98.9) | |
| No | 7 (4.3) | 2 (1.1) | |
| Improvement of general CPR willingness (after CPR training; t1) | 0.0171,* | ||
| Yes | 13 (8.0) | 4 (2.3) | |
| No | 150 (92.0) | 170 (97.7) | |
| CPR Willingness | Male Group n = 166 | Female Group n = 174 | |||
|---|---|---|---|---|---|
| n = 340 | OHCA Victim Is… | OHCA Victim Is… | p-Value | ||
| Female n (%) | Male n (%) | Female n (%) | Male n (%) | ||
| Willingness to resuscitate (t0) (n;%) (yes) | 101 (60.8) | 121 (72.9) | 147 (84.5) | 120 (69.0) | 0.409 1 <0.001 1,* |
| Willingness to resuscitate (t1) (n;%) (yes) | 97 (58.4) | 109 (65.7) | 138 (79.3) | 120 (69.0) | 0.318 1 <0.001 1,* |
| Improvement in willingness to resuscitate (t1) (n;%) | 36 (21.7) | 28 (16.9) | 19 (10.9) | 33 (18.9) | 0.652 1 0.006 1,* |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wingen, S.; Ecker, H.; Schroeder, D.C.; Bartholme, B.; Böttiger, B.W.; Wetsch, W.A. Addressing the Helper’s and Victim’s Gender Is Crucial in Schoolchildren Resuscitation Training—A Prospective, Educative Interventional Trial. J. Clin. Med. 2022, 11, 2384. https://doi.org/10.3390/jcm11092384
Wingen S, Ecker H, Schroeder DC, Bartholme B, Böttiger BW, Wetsch WA. Addressing the Helper’s and Victim’s Gender Is Crucial in Schoolchildren Resuscitation Training—A Prospective, Educative Interventional Trial. Journal of Clinical Medicine. 2022; 11(9):2384. https://doi.org/10.3390/jcm11092384
Chicago/Turabian StyleWingen, Sabine, Hannes Ecker, Daniel C. Schroeder, Bérénice Bartholme, Bernd W. Böttiger, and Wolfgang A. Wetsch. 2022. "Addressing the Helper’s and Victim’s Gender Is Crucial in Schoolchildren Resuscitation Training—A Prospective, Educative Interventional Trial" Journal of Clinical Medicine 11, no. 9: 2384. https://doi.org/10.3390/jcm11092384
APA StyleWingen, S., Ecker, H., Schroeder, D. C., Bartholme, B., Böttiger, B. W., & Wetsch, W. A. (2022). Addressing the Helper’s and Victim’s Gender Is Crucial in Schoolchildren Resuscitation Training—A Prospective, Educative Interventional Trial. Journal of Clinical Medicine, 11(9), 2384. https://doi.org/10.3390/jcm11092384