Abstract
Chronic obstructive pulmonary disease (COPD) is associated with a poor prognosis in patients with non-small cell lung cancer (NSCLC). However, the impact of COPD treatment on the survival of patients with advanced NSCLC remains uncertain. We retrospectively investigated COPD patients among patients newly diagnosed with advanced NSCLC between September 2005 and August 2019 at a university hospital. The clinical characteristics, lung function, and survival outcomes were analyzed and compared between patients who did and did not receive COPD treatment. Among 221 patients with advanced NSCLC and COPD, 124 patients received treatment for COPD and 97 patients did not receive treatment for COPD. Forced expiratory volume in 1 s (FEV1) % predicted value was greater in the no-treatment group than in the COPD treatment group (p < 0.001). The median overall survival (OS) of the treatment group was 10.7 months, while that of the no-treatment group was 8.7 months (p = 0.007). In the multivariate analysis, COPD treatment was independently associated with improved OS (hazard ratio 0.71, 95% confidence interval 0.53–0.95, and p = 0.021). COPD treatment was associated with improved OS in patients with advanced NSCLC and COPD. Therefore, pretreatment spirometry and maximal treatment for COPD may offer a chance of optimal management for patients with advanced NSCLC.
1. Introduction
Lung cancer is the leading cause of cancer-related deaths worldwide. Chronic obstructive pulmonary disease (COPD) is an important comorbidity of lung cancer, sharing a common risk factor, i.e., cigarette smoking. Around 30–70% of lung cancer patients also have COPD [1,2,3]. COPD is associated with an increased risk during surgical resection, which offers the best prospect of long-term survival in patients with anatomically resectable non-small cell lung cancer (NSCLC) [4,5,6]. Even in the operable stage of NSCLC, patients with severe COPD generally cannot undergo surgery due to their high risk. Therefore, for patients with resectable NSCLC, spirometry is an essential test before surgery. Older smokers who have not experienced dyspnea, probably due to their habitual low activity, are often diagnosed with COPD for the first time as a result of spirometry during a pre-surgical examination for NSCLC. Several studies have reported that preoperative treatment with long-acting muscarinic antagonist (LAMA), long-acting β2-agonist (LABA), and/or inhaled corticosteroids (ICS), reduces the incidence of postoperative complications [7,8,9,10].
Similarly, in advanced NSCLC, several studies have reported that forced expiratory volume in 1 s (FEV1) less than 50% predicted or the presence of COPD were associated with mortality [11,12,13]. Because severity of airflow obstruction and acute exacerbations are predictors of mortality in COPD patients [14,15,16], improving these factors might also be important in patients with advanced NSCLC and COPD. Particularly, ICS has been associated with decreased mortality in COPD [17,18,19]. Nevertheless, few studies have investigated whether COPD treatment improves the survival of patients with advanced NSCLC.
The aim of the present study was to investigate the impact of COPD treatment on survival in patients with advanced NSCLC.
2. Materials and Methods
2.1. Study Population
We retrospectively investigated patients who were newly diagnosed with advanced NSCLC (inoperable stage IIIA to IV) between September 2005 and August 2019 at the Ewha Womans University Mokdong Hospital, Seoul, Korea (Figure 1). Among these, patients with spirometrically diagnosed COPD or patients who had already received treatment for COPD were included in the present study. The post-bronchodilator FEV1/forced vital capacity (FVC) < 0.7 was applied to define COPD. Patients were excluded if they had undergone surgical resection, did not have a histological diagnosis, were transferred to another hospital, or dropped out immediately after the diagnosis. We also excluded patients who harbored target mutations, such as epidermal growth factor receptor mutation and anaplastic lymphoma kinase rearrangement, and consequently received targeted therapies since they had a much better prognosis [20].
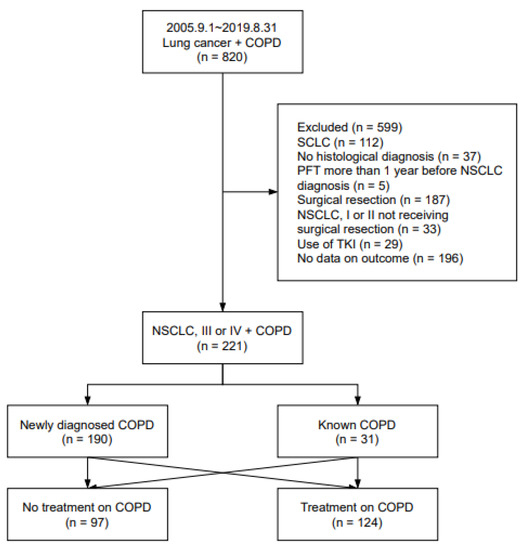
Figure 1.
Study design. COPD, chronic obstructive pulmonary disease; SCLC, small cell lung cancer; PFT, pulmonary function test; NSCLC, non-small cell lung cancer; TKI, tyrosine kinase inhibitor.
2.2. Data Collection and Assessment
Baseline clinical characteristics including age, sex, body mass index (BMI), smoking history, histological type, lung cancer stage, cancer treatment-related matters, and COPD treatment regimen were collected retrospectively using medical records. To diagnose COPD and determine the severity of airflow obstruction, spirometry performed within one year before and after the diagnosis of lung cancer was used.
The study subjects were divided into two groups according to whether they received COPD treatment or not. The COPD treatment group included patients who received inhaled therapy and/or theophylline. The no-treatment group included those who did not receive any treatment for COPD. The primary endpoint of the present study was to compare overall survival (OS) among these groups. In addition, we also investigated whether there was a difference in OS according to the COPD treatment regimens. OS was defined as the time from histologic diagnosis of NSCLC to death.
2.3. Statistical Analysis
The Pearson chi-square test or Fisher’s exact test was used to compare categorical variables, and the Student’s t-test was used to compare continuous variables. OS curves were plotted using the Kaplan–Meier method and were compared using a log-rank test. Hazard ratios (HRs) for univariate and multivariate survival analyses were calculated using the Cox proportional hazard model. All tests of significance were 2-sided, and differences among groups were considered significant when p < 0.05. All statistical analyses were performed using SPSS for Windows, version 27.0 (SPSS Inc., Chicago, IL, USA).
3. Results
3.1. Baseline Characteristics
A total of 221 patients with coexisting advanced NSCLC and COPD were included in the present study. Among these, 124 patients received COPD treatment and 97 patients did not receive COPD treatment. The baseline demographic and clinical characteristics of the patients are presented in Table 1. The mean age of the 221 patients was 70.7 ± 9.0 years old and 200 (90.5%) patients were men. There was a significant difference in lung cancer stage, where 61.9% of the no-treatment group had stage IV disease, while only 44.4% of the COPD treatment group had stage IV disease (p = 0.010). A total of 190 (86.0%) patients were newly diagnosed with COPD at the time of diagnosis of advanced NSCLC. A significantly higher proportion of patients in the no-treatment group were newly diagnosed COPD patients as compared with the COPD treatment group (99.0% vs. 75.8%, p < 0.001). In addition, the no-treatment group showed better baseline FVC, FEV1, and carbon monoxide diffusing capacity as compared with the COPD treatment group (Table 2). One hundred and five (84.7%) patients received inhalation therapy; triple therapy (ICS/LABA/LAMA) was the most commonly used regimen (45/124, 36.3%), followed by LAMA/LABA combination (22/124, 17.7%) and LAMA alone (20/124, 16.1%, Table 3).

Table 1.
Comparison of baseline characteristics by COPD treatment status.
Table 2.
Comparison of lung function by COPD treatment status.
Table 3.
Types of COPD treatment.
3.2. Overall Survival
The treatment group showed significantly improved median OS as compared with the no-treatment group (10.7 months, 95% confidence interval (CI) 8.3–13.0, vs. 8.7 months, 95% CI 7.5–9.9, p = 0.007, Figure 2A). We also investigated whether there was a difference in OS according to treatment regimens. The Kaplan–Meier survival curves revealed that all types of COPD treatment were associated with improved median OS. Patients who received inhalation therapy showed a median OS of 10.9 months, while the other patients had a median OS of 8.9 months (p = 0.021, Figure 2B). The use of ICS (12.2 months vs. 8.8 months, p = 0.006, Figure 2C) and theophylline (11.4 months vs. 8.7 months, p = 0.016, Figure 2D) also resulted in significantly improved OS versus the untreated patients.
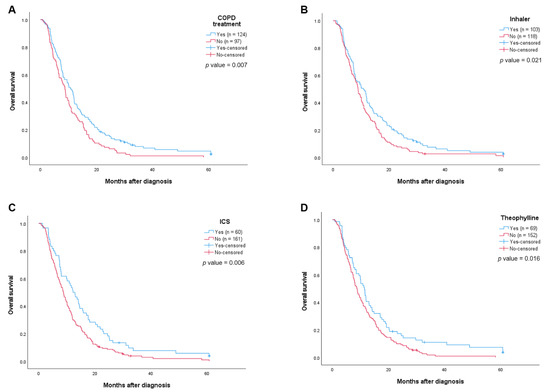
Figure 2.
Kaplan–Meier curves of overall survival of advanced NCSLC: (A) Overall survival curves by COPD treatment; (B) overall survival curves by use of inhaler; (C) overall survival curves by use of ICS; (D) overall survival curves by use of theophylline.
In subgroup analysis according to clinical stages, the median OS was significantly different according to COPD treatment status in stage III (12.0 months vs. 10.4 months, p = 0.032, Supplementary Figure S1A); however, there was no significant difference in stage IV (7.2 months vs. 6.6 months, p = 0.366, Supplementary Figure S1B).
Comparing OS according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification, on the one hand, the median OS of the COPD treatment group was significantly longer than that of the no-treatment group in GOLD 2 (11.8 months vs. 8.9 months, p = 0.007, Table 2). On the other hand, there was no significant difference in OS according to the presence or absence of COPD treatment in GOLD 1, GOLD 3, and GOLD 4 (Table 2).
In univariate analysis, sex, BMI, FEV1 less than 50% predicted, FVC, stage, chemotherapy, COPD treatment, inhaler use, ICS use, and theophylline-containing treatment were revealed as significant prognostic factors predicting OS (all p < 0.05). In the multivariate Cox regression analysis, men (HR 2.49, 95% CI 1.52–4.10, and p < 0.001) and stage IV disease (HR 1.94, 95% CI 1.44–2.62, and p < 0.001) were independent predictors of a worse OS, whereas higher BMI (HR 0.95, 95% CI 0.91–0.99, and p = 0.033), chemotherapy (HR 0.44, 95% CI 0.31–0.62, and p < 0.001), and COPD treatment (HR 0.71, 95% CI 0.53–0.95, and p = 0.021) were independent predictors of better OS (Table 4). When applying inhalation therapy or ICS instead of COPD treatment with the same variables, inhalation therapy (HR 0.72, 95% CI 0.54–0.97, and p = 0.029; Supplementary Table S1) and ICS were independent predictors of a better OS (HR 0.67, 95% CI 0.49–0.92, and p = 0.012; Supplementary Table S2). However, theophylline administration was not an independent predictor of OS (HR 0.79, 95% CI 0.58–1.08, and p = 0.135; Supplementary Table S3).
Table 4.
Clinical factors associated with overall survival.
4. Discussion
The current study demonstrated that COPD treatment was associated with improved OS in patients with advanced NSCLC, even though the COPD treatment group had worse baseline lung function than the no-treatment group. When OS was analyzed for each type of COPD treatment, inhalation therapy and the use of ICS were associated with improvements in OS.
COPD is an important comorbidity for lung cancer patients. Therefore, several studies have investigated the relationship between COPD and the prognosis of lung cancer patients. In patients with inoperable NSCLC, FEV1 < 60% predicted or diffusing lung capacity < 60% predicted have both been associated with a worse prognosis [11,21]. FEV1 itself is a predictor of mortality, not only in COPD patients but also in the general population [14,22]. For patients with operable lung cancer, preoperative spirometry is essential, whereas spirometry may not be necessary for patients with inoperable lung cancer, particularly if they do not complain of respiratory symptoms, in which case clinicians are likely to focus only on lung cancer. Since physical activity usually decreases with age, patients with mild to moderate COPD, usually defined as FEV1 ≥ 50% predicted, do not experience or overlook their respiratory symptoms in many cases. In this study, 86% of patients with advanced NSCLC were diagnosed with COPD for the first time. Unfortunately, out of 190 patients with newly diagnosed COPD, only 94 (49%) patients were treated for their COPD. These results indicate that the identification of COPD through spirometry and active treatment for COPD is essential before treatment of their cancer.
As a result of comparing the OS with and without COPD treatment according to the GOLD classification, the OS of the COPD treatment group was significantly improved as compared with that of the no-treatment group in GOLD 2. In GOLD 1, GOLD 3, and GOLD 4, there was no difference in OS according to the presence or absence of COPD treatment. Since more than half of our study subjects belonged to the GOLD 2 stage (121/221) and the number of GOLD 1, GOLD 3, and GOLD 4 patients was relatively small, it is most likely that only GOLD 2 stage showed OS differences depending on the presence or absence of COPD treatment. However, similar to our study results, a study examining the effects of salmeterol/fluticasone propionate (SFC) according to the GOLD stage also showed that SFC significantly reduced mortality as compared with the placebo in GOLD 2 only [23].
In COPD patients, inhaled therapy, including LAMA, LABA, ICS, and combination therapy, have shown improvements in lung function, quality of life, and exacerbations [18,24,25,26]. However, the GOLD noted a lack of convincing evidence for a survival benefit with inhaled therapy in COPD. Recently, large randomized trials have shown a survival benefit of ICS-containing combination therapy over dual bronchodilator therapy with LAMA-LABA [18,19]. Interestingly, according to a nationwide study of COPD patients in Korea, ICS users appear to have a lower risk of lung cancer as compared with nonusers [27]. It is hypothesized that ICS, which reduces the risk of acute exacerbations through anti-inflammatory action in COPD patients, reduces the risk of lung cancer, a type of chronic inflammation. In this study, ICS was shown to prolong the survival of patients with advanced NSCLC. It is possible that the anti-inflammatory action of ICS inhibits cancer progression. There is also a report that ICS lowered the risk of coronary heart disease in COPD patients [28]. Therefore, the use of ICS may have had an effect on cardiovascular mortality in our study subjects. Since detailed information on the cause of death was not available for many of our subjects, it was not possible to evaluate whether inhaled therapy was associated with cancer progression or other fatal complications, such as exacerbation of COPD, pneumonia, and cardiovascular events. Inhaled therapy may have also influenced their performance status, which is a major factor in determining whether to treat lung cancer, and is itself an important prognostic factor in lung cancer patients [29].
In COPD patients, ICS increases the risk of pneumonia [30,31,32]. Pneumonia is one of the most life-threatening complications of lung cancer patients. However, previous studies have demonstrated consistent results that the use of ICS does not increase pneumonia-related mortality in COPD patients, and instead it is associated with decreased mortality in hospitalized pneumonia patients [17,33]. This might suggest a double effect of ICS, i.e., an immunosuppressive effect and an anti-inflammatory effect. ICS, which achieves locally high concentrations in the lung, upregulates the production of anti-inflammatory proteins and inhibits the transcription of proinflammatory cytokines and chemokines [34]. In a previous study of patients receiving cisplatin-containing chemotherapy, inhaled fluticasone reduced the incidence of delayed pulmonary toxicity [35]. Because there are also reports that different types of ICS have different impacts on the incidence of pneumonia, we need to make careful choices about ICS type and dose [31,36].
The present study has several limitations. First, it was a single-center study and not all patients with newly diagnosed advanced NSCLC had performed spirometry, therefore, there may have been selection bias. Second, it was not possible to investigate their performance status. Performance status is an important prognostic factor and may affect treatment decision making [37,38,39]. Nevertheless, BMI and undergoing cytotoxic chemotherapy might indirectly reflect their performance status, and these factors were adjusted for the analysis. Third, it is not clear why the no treatment group did not receive COPD treatment. As this study was a retrospective study, the respiratory symptoms of the study subjects were not evaluated. Nevertheless, the fact that the no treatment group had better lung function than the COPD treatment group strongly suggests the possibility of not receiving COPD treatment due to no respiratory symptoms. Even if a doctor tried to prescribe an inhalation drug, it is likely that a patient with no symptoms refused it. Fourth, although COPD is characterized by not fully reversible airflow obstruction, we were unable to evaluate whether lung function or dyspnea improved after treatment in the COPD treatment group. Fifth, although there was no statistically significant difference in the type of first-line chemotherapy between the two groups, the possibility that immune checkpoint inhibitors might affect the survival should be considered. In this study, four patients of the COPD treatment group received immune checkpoint inhibitors. Immune checkpoint inhibitors were administered as a second-line treatment to one patient and as a later line of treatment to three patients. These patients received two to four cycles of immune checkpoint inhibitors; however, there was no treatment response.
5. Conclusions
COPD treatment is associated with improved survival in patients with both advanced NSCLC and COPD. Additionally, this study showed that ICS and inhalation therapy are associated with improved OS. In patients with advanced NSCLC, finding COPD through spirometry before cancer treatment and treating the COPD as well as the lung cancer could improve survival.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/jcm11092391/s1, Figure S1: Overall survival curves stratified by COPD treatment in subgroup analysis according to clinical stages, stage III (A) and IV (B), Table S1: Clinical factors associated with overall survival (multivariate analysis when applying inhalation therapy instead of COPD treatment), Table S2: Clinical factors associated with overall survival (multivariate analysis when applying inhaled corticosteroids instead of COPD treatment), Table S3: Clinical factors associated with overall survival (multivariate analysis when applying theophylline instead of COPD treatment).
Author Contributions
H.J. had full access to all the data in the study and takes responsibility for the integrity of the data and accuracy of the analysis; J.H.L. and H.J. conceived and designed the study; all authors acquired the clinical data; H.J. conducted the statistical analysis; all authors analyzed and interpreted the data; H.J., S.P. and J.H.L. drafted the manuscript; all authors critically revised the manuscript for important intellectual content and approved the submitted version. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Research Foundation of Korea (NRF-2020R1A5A2019210). The funding source had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, and in the decision to publish the results.
Institutional Review Board Statement
The study protocol was approved by the Institutional Review Board of the Ewha Womans University Hospital (IRB no. 2020-05-012). This study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Patient consent was waived because of the retrospective nature of the analysis.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We thank Hye Ah Lee (Clinical Trial Center, Ewha Womans University Mokdong Hospital) for her contribution to the statistical analysis and Eun Hwa Kang (Informatization department, Ewha Womans University Seoul Hospital) for her contribution to assessment of the patients’ clinical data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Loganathan, R.S.; Stover, D.E.; Shi, W.; Venkatraman, E. Prevalence of COPD in women compared to men around the time of diagnosis of primary lung cancer. Chest 2006, 129, 1305–1312. [Google Scholar] [CrossRef] [PubMed]
- Young, R.P.; Hopkins, R.J.; Christmas, T.; Black, P.N.; Metcalf, P.; Gamble, G. COPD prevalence is increased in lung cancer, independent of age, sex and smoking history. Eur. Respir. J. 2009, 34, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Collar, D.P.; Guerra, M.P.; Rodriguez, P.; Gotera, C.; Mahíllo-Fernández, I.; Peces-Barba, G.; Seijo, L.M. COPD is commonly underdiagnosed in patients with lung cancer: Results from the RECOIL study (retrospective study of COPD infradiagnosis in lung cancer). Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1033. [Google Scholar]
- Win, T.; Jackson, A.; Sharples, L.; Groves, A.; Wells, F.; Ritchie, A.; Laroche, C. Relationship between pulmonary function and lung cancer surgical outcome. Eur. Respir. J. 2005, 25, 594–599. [Google Scholar] [CrossRef]
- Greillier, L.; Thomas, P.; Loundou, A.; Doddoli, C.; Badier, M.; Auquier, P.; Barlési, F. Pulmonary function tests as a predictor of quantitative and qualitative outcomes after thoracic surgery for lung cancer. Clin. Lung Cancer 2007, 8, 554–561. [Google Scholar] [CrossRef]
- Zhai, R.; Yu, X.; Shafer, A.; Wain, J.C.; Christiani, D.C. The impact of coexisting COPD on survival of patients with early-stage non-small cell lung cancer undergoing surgical resection. Chest 2014, 145, 346–353. [Google Scholar] [CrossRef]
- Kobayashi, S.; Suzuki, S.; Niikawa, H.; Sugawara, T.; Yanai, M. Preoperative use of inhaled tiotropium in lung cancer patients with untreated COPD. Respirology 2009, 14, 675–679. [Google Scholar] [CrossRef]
- Nojiri, T.; Inoue, M.; Yamamoto, K.; Maeda, H.; Takeuchi, Y.; Nakagiri, T.; Shintani, Y.; Minami, M.; Sawabata, N.; Okumura, M. RETRACTED ARTICLE: Inhaled tiotropium to prevent postoperative cardiopulmonary complications in patients with newly diagnosed chronic obstructive pulmonary disease requiring lung cancer surgery. Surg. Today 2014, 44, 285–290. [Google Scholar] [CrossRef]
- Makino, T.; Otsuka, H.; Hata, Y.; Koezuka, S.; Azuma, Y.; Isobe, K.; Sugino, K.; Ebihara, S.; Homma, S.; Iyoda, A. Long-acting muscarinic antagonist and long-acting β2-agonist therapy to optimize chronic obstructive pulmonary disease prior to lung cancer surgery. Mol. Clin. Oncol. 2018, 8, 647–652. [Google Scholar] [CrossRef]
- Bölükbas, S.; Eberlein, M.; Eckhoff, J.; Schirren, J. Short-term effects of inhalative tiotropium/formoterol/budenoside versus tiotropium/formoterol in patients with newly diagnosed chronic obstructive pulmonary disease requiring surgery for lung cancer: A prospective randomized trial. Eur. J. Cardio-Thorac. Surg. 2011, 39, 995–1000. [Google Scholar] [CrossRef]
- Lee, J.H.; Song, E.M.; Sim, Y.S.; Ryu, Y.J.; Chang, J.H. Forced expiratory volume in one second as a prognostic factor in advanced non-small cell lung cancer. J. Thorac. Oncol. 2011, 6, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-y.; Choi, Y.J.; Seo, J.H.; Lee, S.Y.; Kim, J.S.; Kang, E.J. Pulmonary function is implicated in the prognosis of metastatic non-small cell lung cancer but not in extended disease small cell lung cancer. J. Thorac. Dis. 2019, 11, 4562. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.U.; Yeo, C.D.; Rhee, C.K.; Kang, H.S.; Park, C.K.; Kim, J.S.; Kim, J.W.; Kim, S.J.; Yoon, H.K.; Lee, S.H. Comparison of clinical characteristics and overall survival between spirometrically diagnosed chronic obstructive pulmonary disease (COPD) and non-COPD never-smoking stage I-IV non-small cell lung cancer patients. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 929. [Google Scholar] [CrossRef] [PubMed]
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; de Oca, M.M.; Mendez, R.A.; Plata, V.P.; Cabral, H.J. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.P.; Krishnan, J.A.; Lechtzin, N.; Diette, G.B. In-hospital mortality following acute exacerbations of chronic obstructive pulmonary disease. Arch. Intern. Med. 2003, 163, 1180–1186. [Google Scholar] [CrossRef] [PubMed]
- Price, L.C.; Lowe, D.; Hosker, H.; Anstey, K.; Pearson, M.; Roberts, C.M. UK National COPD Audit 2003: Impact of hospital resources and organisation of care on patient outcome following admission for acute COPD exacerbation. Thorax 2006, 61, 837–842. [Google Scholar] [CrossRef]
- Chen, D.; Restrepo, M.I.; Fine, M.J.; Pugh, M.J.V.; Anzueto, A.; Metersky, M.L.; Nakashima, B.; Good, C.; Mortensen, E.M. Observational study of inhaled corticosteroids on outcomes for COPD patients with pneumonia. Am. J. Respir. Crit. Care Med. 2011, 184, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Lipson, D.A.; Barnhart, F.; Brealey, N.; Brooks, J.; Criner, G.J.; Day, N.C.; Dransfield, M.T.; Halpin, D.M.; Han, M.K.; Jones, C.E. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N. Engl. J. Med. 2018, 378, 1671–1680. [Google Scholar] [CrossRef]
- Rabe, K.F.; Martinez, F.J.; Ferguson, G.T.; Wang, C.; Singh, D.; Wedzicha, J.A.; Trivedi, R.; St. Rose, E.; Ballal, S.; McLaren, J. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N. Engl. J. Med. 2020, 383, 35–48. [Google Scholar] [CrossRef]
- Lee, J.G.; Kim, H.C.; Choi, C.-M. Recent Trends of Lung Cancer in Korea. Tuberc. Respir. Dis. 2021, 84, 89. [Google Scholar] [CrossRef]
- Semrau, S.; Klautke, G.; Virchow, J.; Kundt, G.; Fietkau, R. Impact of comorbidity and age on the outcome of patients with inoperable NSCLC treated with concurrent chemoradiotherapy. Respir. Med. 2008, 102, 210–218. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Duong, M.; Islam, S.; Rangarajan, S.; Leong, D.; Kurmi, O.; Teo, K.; Killian, K.; Dagenais, G.; Lear, S.; Wielgosz, A. Mortality and cardiovascular and respiratory morbidity in individuals with impaired FEV1 (PURE): An international, community-based cohort study. Lancet Glob. Health 2019, 7, e613–e623. [Google Scholar] [CrossRef]
- Jenkins, C.R.; Jones, P.W.; Calverley, P.M.; Celli, B.; Anderson, J.A.; Ferguson, G.T.; Yates, J.C.; Willits, L.R.; Vestbo, J. Efficacy of salmeterol/fluticasone propionate by GOLD stage of chronic obstructive pulmonary disease: Analysis from the randomised, placebo-controlled TORCH study. Respir. Res. 2009, 10, 59. [Google Scholar] [CrossRef] [PubMed]
- Tashkin, D.P.; Celli, B.; Senn, S.; Burkhart, D.; Kesten, S.; Menjoge, S.; Decramer, M. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N. Engl. J. Med. 2008, 359, 1543–1554. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Papi, A.; Corradi, M.; Pavlišová, I.; Montagna, I.; Francisco, C.; Cohuet, G.; Vezzoli, S.; Scuri, M.; Vestbo, J. Single inhaler triple therapy versus inhaled corticosteroid plus long-acting β2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): A double-blind, parallel group, randomised controlled trial. Lancet 2016, 388, 963–973. [Google Scholar] [CrossRef]
- Papi, A.; Vestbo, J.; Fabbri, L.; Corradi, M.; Prunier, H.; Cohuet, G.; Guasconi, A.; Montagna, I.; Vezzoli, S.; Petruzzelli, S. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): A double-blind, parallel group, randomised controlled trial. Lancet 2018, 391, 1076–1084. [Google Scholar] [CrossRef]
- Lee, Y.M.; Kim, S.J.; Lee, J.H.; Ha, E. Inhaled corticosteroids in COPD and the risk of lung cancer. Int. J. Cancer 2018, 143, 2311–2318. [Google Scholar] [CrossRef]
- Shin, J.; Yoon, H.-Y.; Lee, Y.M.; Ha, E.; Lee, J.H. Inhaled corticosteroids in COPD and the risk for coronary heart disease: A nationwide cohort study. Sci. Rep. 2020, 10, 18973. [Google Scholar] [CrossRef]
- Simmons, C.P.; Koinis, F.; Fallon, M.T.; Fearon, K.C.; Bowden, J.; Solheim, T.S.; Gronberg, B.H.; McMillan, D.C.; Gioulbasanis, I.; Laird, B.J. Prognosis in advanced lung cancer—A prospective study examining key clinicopathological factors. Lung Cancer 2015, 88, 304–309. [Google Scholar] [CrossRef]
- Crim, C.; Dransfield, M.T.; Bourbeau, J.; Jones, P.W.; Hanania, N.A.; Mahler, D.A.; Vestbo, J.; Wachtel, A.; Martinez, F.J.; Barnhart, F. Pneumonia risk with inhaled fluticasone furoate and vilanterol compared with vilanterol alone in patients with COPD. Ann. Am. Thorac. Soc. 2015, 12, 27–34. [Google Scholar] [CrossRef]
- Yang, M.; Du, Y.; Chen, H.; Jiang, D.; Xu, Z. Inhaled corticosteroids and risk of pneumonia in patients with chronic obstructive pulmonary disease: A meta-analysis of randomized controlled trials. Int. Immunopharmacol. 2019, 77, 105950. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Park, Y.H.; Kang, D.R.; Lee, S.J.; Lee, M.K.; Kim, S.-H.; Yong, S.J.; Lee, W.-Y. Risk of pneumonia associated with inhaled corticosteroid in patients with chronic obstructive pulmonary disease: A Korean population-based study. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 3397. [Google Scholar] [CrossRef] [PubMed]
- de Molina, R.M.; Mortensen, E.; Restrepo, M.; Copeland, L.; Pugh, M.; Anzueto, A. Inhaled corticosteroid use is associated with lower mortality for subjects with COPD and hospitalised with pneumonia. Eur. Respir. J. 2010, 36, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P. Corticosteroid effects on cell signalling. Eur. Respir. J. 2006, 27, 413–426. [Google Scholar] [CrossRef] [PubMed]
- McGaughey, D.S.; Nikcevich, D.A.; Long, G.D.; Vredenburgh, J.J.; Rizzieri, D.; Smith, C.A.; Broadwater, G.; Loftis, J.S.; McDonald, C.; Morris, A.K. Inhaled steroids as prophylaxis for delayed pulmonary toxicity syndrome in breast cancer patients undergoing high-dose chemotherapy and autologous stem cell transplantation. Biol. Blood Marrow Transplant. 2001, 7, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Li, S.; Zhou, W.; Yang, X.; Li, J.; Cao, J. Risk of pneumonia with different inhaled corticosteroids in COPD patients: A meta-analysis. COPD J. Chronic Obstr. Pulm. Dis. 2020, 17, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Albain, K.S.; Crowley, J.J.; LeBlanc, M.; Livingston, R.B. Survival determinants in extensive-stage non-small-cell lung cancer: The Southwest Oncology Group experience. J. Clin. Oncol. 1991, 9, 1618–1626. [Google Scholar] [CrossRef]
- Di Maio, M.; Lama, N.; Morabito, A.; Smit, E.F.; Georgoulias, V.; Takeda, K.; Quoix, E.; Hatzidaki, D.; Wachters, F.M.; Gebbia, V. Clinical assessment of patients with advanced non-small-cell lung cancer eligible for second-line chemotherapy: A prognostic score from individual data of nine randomised trials. Eur. J. Cancer 2010, 46, 735–743. [Google Scholar] [CrossRef]
- Zukin, M.; Barrios, C.H.; Rodrigues Pereira, J.; De Albuquerque Ribeiro, R.; de Mendonça Beato, C.A.; do Nascimento, Y.N.; Murad, A.; Franke, F.A.; Precivale, M.; de Lima Araujo, L.H. Randomized phase III trial of single-agent pemetrexed versus carboplatin and pemetrexed in patients with advanced non–small-cell lung cancer and Eastern Cooperative Oncology Group performance status of 2. J. Clin. Oncol. 2013, 31, 2849–2853. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).