
Effect of an Electronic Alert System on Hepatitis B Virus Reactivation in Patients Receiving Immunosuppressive Drug Therapy

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Reagents
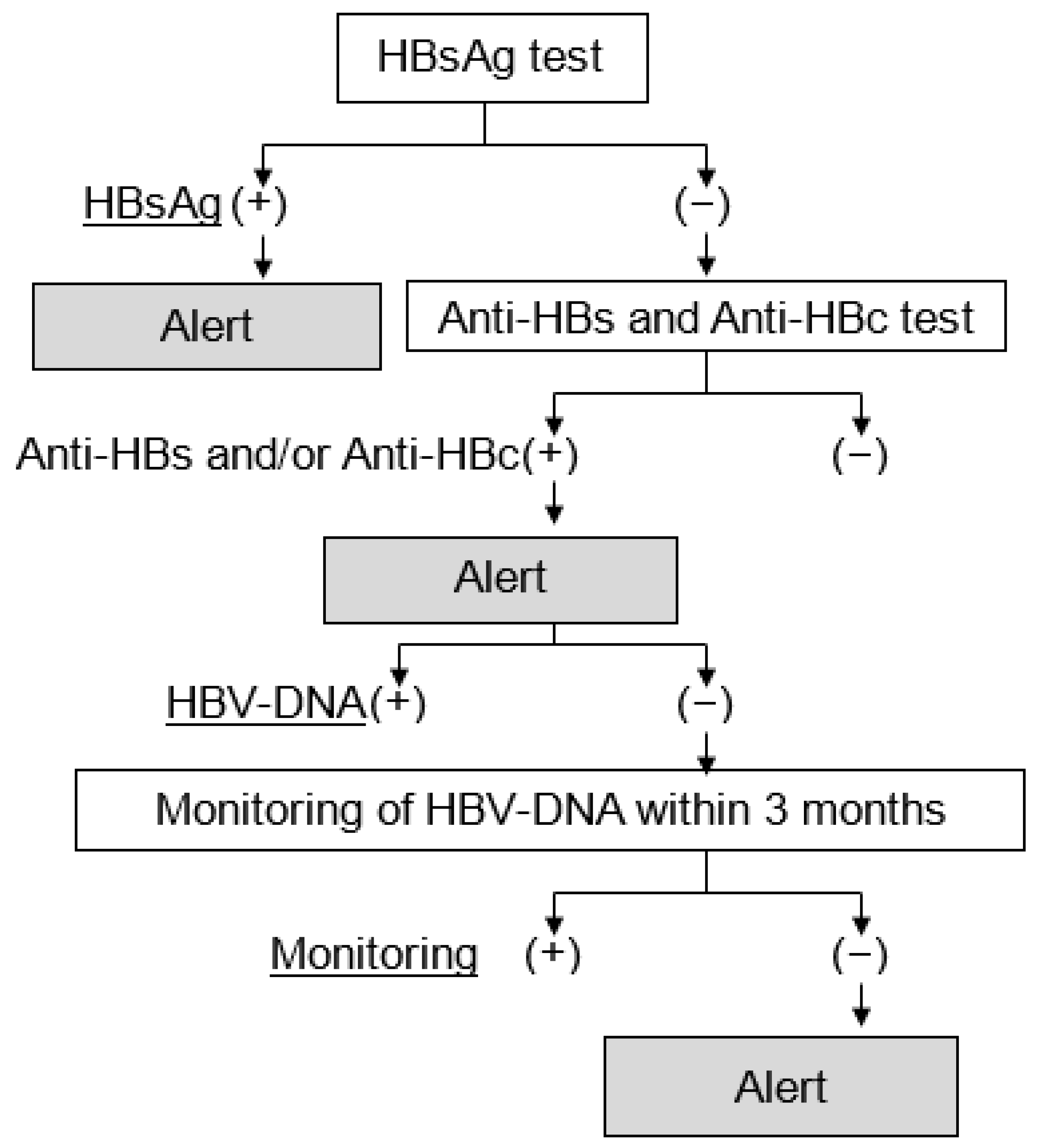
2.3. The Electronic Alert System for HBVr
2.4. Statistical Analysis
3. Results
3.1. Clinical Background before and after the Introduction of the Alert System
3.2. Effect of the Alert System on HBV-DNA Measurement Rates
3.3. Two Cases of HBV-Reactivation in Patients with HBV-Remission Phase
3.4. HBV-DNA Measurement Rates before and after the Introduction of the System in Patients Undergoing Chemotherapy
3.5. HBV-DNA Measurement Rates before and after the Introduction of the System in Patients Undergoing other Immunosuppressive Therapies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herrscher, C.; Roingeard, P.; Blanchard, E. Hepatitis B virus entry into cells. Cells 2020, 9, 1486. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.L.; Ratziu, V.; Yuen, M.F.; Poynard, T. Viral hepatitis B. Lancet 2003, 362, 2089–2094. [Google Scholar] [CrossRef]
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.T.; Krause, G.; Ott, J.J. Estimations of worldwide prevalence of chronic hepatitis B virus infection: A systematic review of data published between 1965 and 2013. Lancet 2015, 386, 1546–1555. [Google Scholar] [CrossRef]
- Liang, T.J. Hepatitis B: The virus and disease. Hepatology 2009, 49, S13–S21. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Hepatitis B. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 22 April 2022).
- McMahon, B.J. Natural history of chronic hepatitis B. Clin. Liver Dis. 2010, 14, 381–396. [Google Scholar] [CrossRef]
- Likhitsup, A.; Lok, A.S. Understanding the natural history of hepatitis B virus infection and the new definitions of cure and the endpoints of clinical trials. Clin. Liver Dis. 2019, 23, 401–416. [Google Scholar] [CrossRef]
- Toyoda, H.; Leong, J.; Landis, C.; Atsukawa, M.; Watanabe, T.; Huang, D.Q.; Liu, J.; Quek, S.X.Z.; Ishikawa, T.; Arai, T.; et al. Treatment and renal outcomes up to 96 weeks after tenofovir alafenamide switch from tenofovir disoproxil fumarate in routine practice. Hepatology 2021, 74, 656–666. [Google Scholar] [CrossRef]
- Dienstag, J.L. Benefits and risks of nucleoside analog therapy for hepatitis B. Hepatology 2009, 49, S112–S121. [Google Scholar] [CrossRef]
- Nassal, M. HBV cccDNA: Viral persistence reservoir and key obstacle for a cure of chronic hepatitis B. Gut 2015, 64, 1972–1984. [Google Scholar] [CrossRef] [Green Version]
- Yeo, W.; Johnson, P.J. Diagnosis, prevention and management of hepatitis B virus reactivation during anticancer therapy. Hepatology 2006, 43, 209–220. [Google Scholar] [CrossRef]
- Rehermann, B.; Ferrari, C.; Pasquinelli, C.; Chisari, F.V. The hepatitis B virus persists for decades after patients’ recovery from acute viral hepatitis despite active maintenance of a cytotoxic T-lymphocyte response. Nat. Med. 1996, 2, 1104–1108. [Google Scholar] [CrossRef] [PubMed]
- Yeo, W.; Chan, P.K.; Zhong, S.; Ho, W.M.; Steinberg, J.L.; Tam, J.S.; Hui, P.; Leung, N.W.; Zee, B.; Johnson, P.J. Frequency of hepatitis B virus reactivation in cancer patients undergoing cytotoxic chemotherapy: A prospective study of 626 patients with identification of risk factors. J. Med. Virol. 2000, 62, 299–307. [Google Scholar] [CrossRef]
- Lok, A.S.; Liang, R.H.; Chiu, E.K.; Wong, K.L.; Chan, T.K.; Todd, D. Reactivation of hepatitis B virus replication in patients receiving cytotoxic therapy. Report of a prospective study. Gastroenterology 1991, 100, 182–188. [Google Scholar] [CrossRef]
- Calabrese, L.H.; Zein, N.N.; Vassilopoulos, D. Hepatitis B virus (HBV) reactivation with immunosuppressive therapy in rheumatic diseases: Assessment and preventive strategies. Ann. Rheum. Dis. 2006, 65, 983–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, E.; Urata, Y. Risk of hepatitis B reactivation in patients treated with tumor necrosis factor-α inhibitors. Hepatol. Res. 2012, 42, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Loomba, R.; Liang, T.J. Hepatitis B reactivation associated with immune suppressive and biological modifier therapies: Current concepts, management strategies, and future directions. Gastroenterology 2017, 152, 1297–1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, S.; Nakazono, K.; Murasawa, A.; Mita, Y.; Hata, K.; Saito, N.; Kikuchi, M.; Yoshida, K.; Nakano, M.; Gejyo, F. Development of fulminant hepatitis B (precore variant mutant type) after the discontinuation of low-dose methotrexate therapy in a rheumatoid arthritis patient. Arthritis Rheum. 2001, 44, 339–342. [Google Scholar] [CrossRef]
- Cheng, J.; Li, J.B.; Sun, Q.L.; Li, X. Reactivation of hepatitis B virus after steroid treatment in rheumatic diseases. J. Rheumatol. 2011, 38, 181–182. [Google Scholar] [CrossRef]
- Wei, L.; Ploss, A. Hepatitis B virus cccDNA is formed through distinct repair processes of each strand. Nat. Commun. 2021, 12, 1591. [Google Scholar] [CrossRef]
- Zoulim, F. New insight on hepatitis B virus persistence from the study of intrahepatic viral cccDNA. J. Hepatol. 2005, 42, 302–308. [Google Scholar] [CrossRef]
- Reddy, K.R.; Beavers, K.L.; Hammond, S.P.; Lim, J.K.; Falck-Ytter, Y.T. American Gastroenterological Association Institute guideline on the prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology 2015, 148, 215–219, quiz e216–e217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drafting Committee for Hepatitis Management Guidelines and the Japan Society of Hepatology. JSH Guidelines for the Management of Hepatitis B Virus Infection. Hepatol. Res. 2014, 44 (Suppl. S1), 1–58. [Google Scholar] [CrossRef] [PubMed]
- Remo, M.; Abraham, I.; Kankanala, V.; Chacra, W.; Danciu, O.C. Hepatitis B reactivation in a patient receiving chemotherapy for breast cancer: A case report. Anticancer Res. 2017, 37, 3791–3793. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Abe, K.; Fujita, M.; Okai, K.; Takahashi, A.; Ohira, H. Hepatitis B virus reactivation in a patient with nonalcoholic steatohepatitis 41 months after rituximab-containing chemotherapy. Intern. Med. 2019, 58, 375–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimond, C.; Negroiu, A.; Hughes, D.M.; Patel, J. Fatal hepatitis B reactivation in a patient receiving chemoradiation for cervical cancer. J. Oncol. Pharm. Pract. 2021, 27, 1296–1301. [Google Scholar] [CrossRef] [PubMed]
- Morales-Arraez, D.; Hernández-Guerra, M. Electronic alerts as a simple method for amplifying the yield of hepatitis C virus infection screening and diagnosis. Am. J. Gastroenterol. 2020, 115, 9–12. [Google Scholar] [CrossRef]
- Köksal, A.S.; Toka, B.; Eminler, A.T.; Hacıbekiroğlu, I.; Sunu, C.; Uslan, M.I.; Karabay, O.; Parlak, E. The efficacy of a computer alert programme for increasing HBV screening rates before starting immunosuppressive therapy. Acta Gastroenterol. Belg. 2019, 82, 279–284. [Google Scholar]
- Jasmine Bullard, A.; Cunningham, F.E.; Volpp, B.D.; Lowy, E.; Beste, L.A.; Heron, B.B.; Geraci, M.; Hammond, J.M.; LaPlant, K.; Stave, E.A.; et al. Preventing hepatitis B reactivation during anti-CD20 antibody treatment in the veterans health administration. Hepatol. Commun. 2018, 2, 1136–1146. [Google Scholar] [CrossRef]
- Sanagawa, A.; Kuroda, J.; Shiota, A.; Kito, N.; Takemoto, M.; Kawade, Y.; Esaki, T.; Kimura, K. Outcomes of the implementation of the computer-assisted HBView system for the prevention of hepatitis B virus reactivation in chemotherapy patients: A retrospective analysis. J. Pharm. Health Care Sci. 2015, 1, 29. [Google Scholar] [CrossRef] [Green Version]
- Svicher, V.; Salpini, R.; Malagnino, V.; Piermatteo, L.; Alkhatib, M.; Cerva, C.; Sarmati, L. New markers in monitoring the reactivation of hepatitis B virus infection in immunocompromised hosts. Viruses 2019, 11, 783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarmati, L.; Andreoni, M.; Antonelli, G.; Arcese, W.; Bruno, R.; Coppola, N.; Gaeta, G.B.; Galli, M.; Girmenia, C.; Mikulska, M.; et al. Recommendations for screening, monitoring, prevention, prophylaxis and therapy of hepatitis B virus reactivation in patients with haematologic malignancies and patients who underwent haematologic stem cell transplantation-a position paper. Clin. Microbiol. Infect. 2017, 23, 935–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusumoto, S.; Tanaka, Y.; Suzuki, R.; Watanabe, T.; Nakata, M.; Takasaki, H.; Fukushima, N.; Fukushima, T.; Moriuchi, Y.; Itoh, K.; et al. Monitoring of hepatitis B virus (HBV) DNA and risk of HBV reactivation in B-cell lymphoma: A prospective observational study. Clin. Infect. Dis. 2015, 61, 719–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Japan Society of Hepatology guidelines for the management of hepatitis C virus infection: 2019 update. Hepatol. Res. 2020, 50, 791–816. [CrossRef] [PubMed]
- Sarin, S.K.; Kumar, M.; Lau, G.K.; Abbas, Z.; Chan, H.L.; Chen, C.J.; Chen, D.S.; Chen, H.L.; Chen, P.J.; Chien, R.N.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef]
- Seto, W.K.; Chan, T.S.; Hwang, Y.Y.; Wong, D.K.; Fung, J.; Liu, K.S.; Gill, H.; Lam, Y.F.; Lie, A.K.; Lai, C.L.; et al. Hepatitis B reactivation in patients with previous hepatitis B virus exposure undergoing rituximab-containing chemotherapy for lymphoma: A prospective study. J. Clin. Oncol. 2014, 32, 3736–3743. [Google Scholar] [CrossRef]
- Koutsianas, C.; Thomas, K.; Vassilopoulos, D. Reactivation of hepatitis B virus infection in rheumatic diseases: Risk and management considerations. Ther. Adv. Musculoskelet. Dis. 2020, 12, 1759720x20912646. [Google Scholar] [CrossRef] [Green Version]
- Kusumoto, S.; Arcaini, L.; Hong, X.; Jin, J.; Kim, W.S.; Kwong, Y.L.; Peters, M.G.; Tanaka, Y.; Zelenetz, A.D.; Kuriki, H.; et al. Risk of HBV reactivation in patients with B-cell lymphomas receiving obinutuzumab or rituximab immunochemotherapy. Blood 2019, 133, 137–146. [Google Scholar] [CrossRef]
- Kusumoto, S.; Tanaka, Y.; Ueda, R.; Mizokami, M. Reactivation of hepatitis B virus following rituximab-plus-steroid combination chemotherapy. J. Gastroenterol. 2011, 46, 9–16. [Google Scholar] [CrossRef]
- Kumagai, K.; Takagi, T.; Nakamura, S.; Sawada, U.; Kura, Y.; Kodama, F.; Shimano, S.; Kudoh, I.; Nakamura, H.; Sawada, K.; et al. Hepatitis B virus carriers in the treatment of malignant lymphoma: An epidemiological study in Japan. Ann. Oncol. 1997, 8 (Suppl. S1), 107–109. [Google Scholar] [CrossRef]
- Lazarevic, I.; Banko, A.; Miljanovic, D.; Cupic, M. Immune-escape hepatitis B virus mutations associated with viral reactivation upon immunosuppression. Viruses 2019, 11, 778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanetti, A.R.; Tanzi, E.; Manzillo, G.; Maio, G.; Sbreglia, C.; Caporaso, N.; Thomas, H.; Zuckerman, A.J. Hepatitis B variant in Europe. Lancet 1988, 2, 1132–1133. [Google Scholar] [CrossRef]
- Carman, W.F.; Zanetti, A.R.; Karayiannis, P.; Waters, J.; Manzillo, G.; Tanzi, E.; Zuckerman, A.J.; Thomas, H.C. Vaccine-induced escape mutant of hepatitis B virus. Lancet 1990, 336, 325–329. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Before | After | p-Value | |
|---|---|---|---|
| Duration | August 2015 to July 2018 | October 2019 to April 2020 | |
| Number of patients | 4417 | 912 | |
| Patients who received chemotherapy | 2874 (65.1%) | 588 (64.5%) | 0.73 |
| Patients who received other immunosuppressive therapy | 1543 (34.9%) | 324 (35.5%) | |
| Gender (male/female) | 2039/2378 | 429/483 | 0.63 |
| Age (median, 95% CI) | 65 (59.5–60.6) | 66 (59.9–62.2) | 0.09 |
| HBsAg-positive patients | 42 (1.0%) | 9 (1.0 %) | 0.92 |
| HBsAg-negative patients | 4374 (99.0%) | 903 (99.0%) | |
| Patients with anti-HBs and/or anti-HBc | 917 (20.8%) | 219 (24.0%) | 0.03 |
| Patients with anti-HBs alone | 185 | 32 | |
| Patients with anti-HBc alone | 205 | 42 | |
| Patients with anti-HBs and anti-HBc | 527 | 145 | |
| HBV-remission patients | 704 (15.9%) | 188 (20.6%) | <0.01 |
| Before | After | p-Value | |
|---|---|---|---|
| HBsAg-positive patients | (n = 42) | (n = 9) | |
| Measurement for HBV-DNA | 35 | 8 | 0.68 |
| HBV-DNA-positive patients | 21 (60.0%) | 4 (50.0%) | 0.76 |
| HBsAg-negative patients | (n = 4374) | (n = 903) | |
| Patients with anti-HBs and/or anti-HBc | 917 | 219 | |
| Measurement for HBV-DNA before therapies | 705 (76.9%) | 188 (85.8%) | <0.01 |
| HBV-DNA-positive patients | 1 (0.1%) | 0 (0%) | 0.61 |
| HBV-remission patients with therapies | (n = 704) | (n = 188) | |
| Patients without HBV-DNA | 704 | 188 | |
| Monitoring of HBVDNA within 3 months after therapies | 305 (43.3%) | 104 (55.3%) | <0.01 |
| HBV-DNA-positive patients | 2 (0.7%) | 0 (0%) | 0.46 |
| Age | Gender | Background Disease | Treatment for Background Disease | Duration of Treatment [days] | Treatment for HBV | Pre-Anti-HBs [mIU/mL] | Pre-Anti-HBc [S/CO] | Post-HBV-DNA [log10 IU/mL] | Post-ALT [IU/L] |
|---|---|---|---|---|---|---|---|---|---|
| 76 | Male | Renal cell carcinoma | GC | 84 | TAF | 0.17 | 9.39 | 1.72 | 41 |
| 81 | Male | Bladder cancer | Low dose GC | 18 | ETV | 26.72 | 1.77 | 1.75 | 7 |
| Before | After | p-Value | |
| Number of patients who were tested | 2874 | 588 | |
| Gender (male/female) | 1477/1397 | 311/277 | 0.51 |
| Age (median, 95% CI) | 63 (63.2–64.1) | 65 (64.1–66.0) | 0.03 |
| Measurement of HBV-DNA. | |||
| Before | After | p-Value | |
| HBsAg-positive patients | (n = 32) | (n = 6) | |
| Measurement for HBV-DNA | 28 | 5 | 0.79 |
| HBV-DNA-positive patients | 16 (57.1%) | 1 (20.0%) | 0.12 |
| HBsAg-negative patients | (n = 2842) | (n = 582) | |
| Patients with anti-HBs and/or anti-HBc | 639 | 143 | 0.27 |
| Measurement for HBV-DNA before chemotherapy | 490 (76.7%) | 127 (88.8%) | <0.01 |
| HBV-DNA-positive patients | 1 (0.2%) | 0 (0%) | 0.61 |
| HBV-remission patients undergoing chemotherapy | (n = 489) | (n = 127) | |
| Patients without HBV-DNA | 489 | 127 | <0.01 |
| Monitoring of HBVDNA within 3 months after chemotherapy | 179 (36.6%) | 65 (51.2%) | <0.01 |
| HBV-DNA-positive patients | 2 (1.1%) | 0 (0%) | 0.39 |
| Before | After | p-Value | |
| Number of patients tested | 1543 | 324 | |
| Gender (male/female) | 562/981 | 118/206 | 0.99 |
| Age (median, 95% CI) | 59 (52.0–54.4) | 60 (51.6–56.7) | 0.70 |
| Measurement of HBV-DNA | |||
| Before | After | p-Value | |
| HBsAg-positive patients | (n = 10) | (n = 3) | |
| Measurement for HBV-DNA | 7 | 3 | 0.28 |
| HBV-DNA-positive patients | 5 (71.4%) | 3 (100%) | 0.30 |
| HBsAg-negative patients | (n = 1532) | (n = 321) | |
| Patients with anti-HBs and/or anti-HBc | 278 | 76 | 0.02 |
| Measurement for HBV-DNA | 215 (77.3%) | 61 (80.3%) | 0.59 |
| HBV-DNA-positive patients | 0 (0%) | 0 (0%) | N.A. |
| HBV-remission patients with therapies | (n = 215) | (n = 61) | |
| Patients without HBV-DNA | 215 | 61 | 0.59 |
| Monitoring of HBVDNA within 3 months after therapies | 126 (58.6%) | 39 (63.9%) | 0.45 |
| HBV-DNA-positive patients | 0 (0%) | 0 (0%) | N.A. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asai, A.; Hirai, S.; Yokohama, K.; Nishikawa, T.; Nishikawa, H.; Higuchi, K. Effect of an Electronic Alert System on Hepatitis B Virus Reactivation in Patients Receiving Immunosuppressive Drug Therapy. J. Clin. Med. 2022, 11, 2446. https://doi.org/10.3390/jcm11092446
Asai A, Hirai S, Yokohama K, Nishikawa T, Nishikawa H, Higuchi K. Effect of an Electronic Alert System on Hepatitis B Virus Reactivation in Patients Receiving Immunosuppressive Drug Therapy. Journal of Clinical Medicine. 2022; 11(9):2446. https://doi.org/10.3390/jcm11092446
Chicago/Turabian StyleAsai, Akira, Saho Hirai, Keisuke Yokohama, Tomohiro Nishikawa, Hiroki Nishikawa, and Kazuhide Higuchi. 2022. "Effect of an Electronic Alert System on Hepatitis B Virus Reactivation in Patients Receiving Immunosuppressive Drug Therapy" Journal of Clinical Medicine 11, no. 9: 2446. https://doi.org/10.3390/jcm11092446
APA StyleAsai, A., Hirai, S., Yokohama, K., Nishikawa, T., Nishikawa, H., & Higuchi, K. (2022). Effect of an Electronic Alert System on Hepatitis B Virus Reactivation in Patients Receiving Immunosuppressive Drug Therapy. Journal of Clinical Medicine, 11(9), 2446. https://doi.org/10.3390/jcm11092446