
Prognostic Value of Characterizing Myocardial Tissue by Cardiac MRI with T1 Mapping in HFpEF Patients: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Literature Searching Strategy
2.3. Data Mining and Synthesis
2.4. Statistical Analysis
3. Results
3.1. Results of Literature Search
3.2. Baseline Characteristics of the Studies
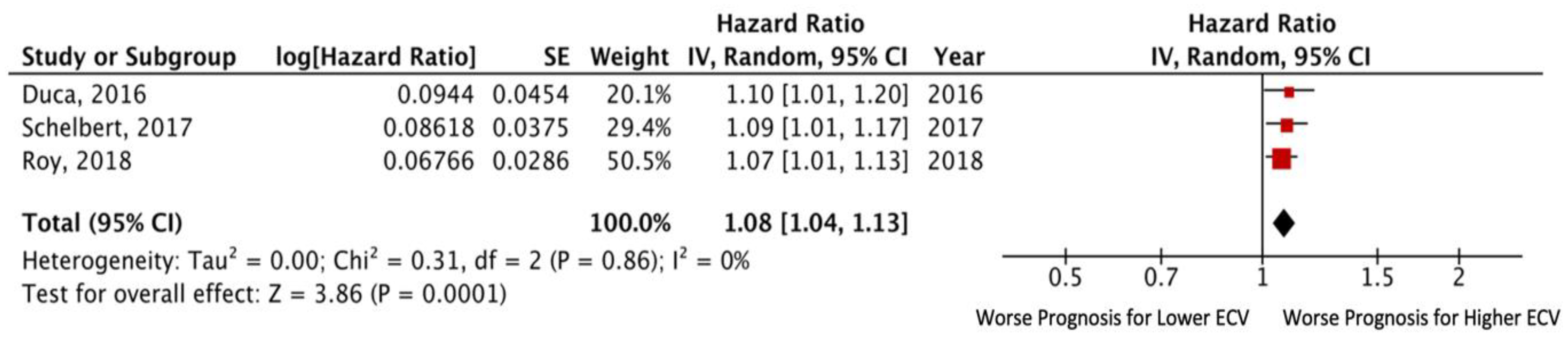
3.3. Extracellular Volume
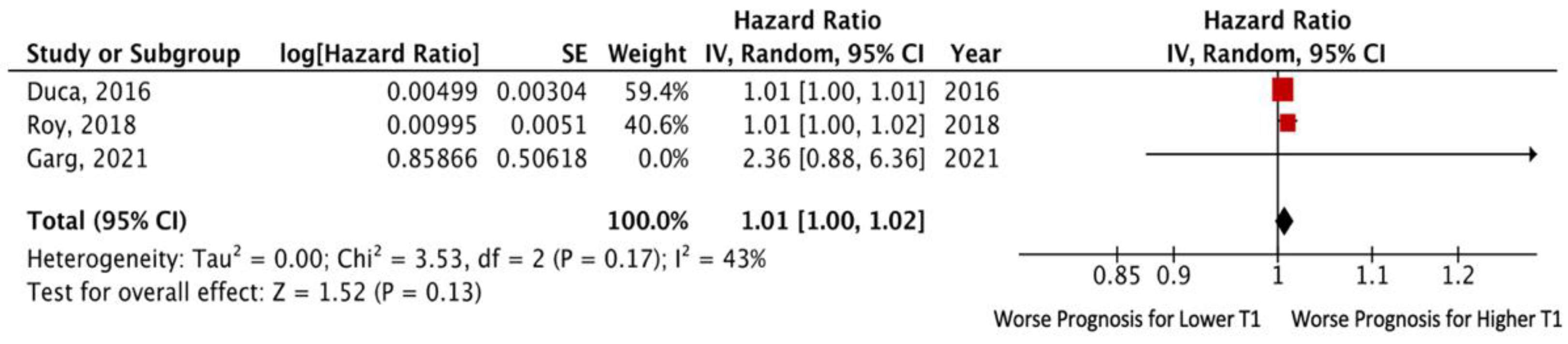
3.4. Native T1 Time
3.5. Postcontrast T1 Time
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Owan, T.E.; Hodge, D.O.; Herges, R.M.; Jacobsen, S.J.; Roger, V.L.; Redfield, M.M. Trends in Prevalence and Outcome of Heart Failure with Preserved Ejection Fraction. N. Engl. J. Med. 2006, 355, 251–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phan, T.T.; Shivu, G.N.; Abozguia, K.; Sanderson, J.E.; Frenneaux, M. The pathophysiology of heart failure with preserved ejection fraction: From molecular mechanisms to exercise haemodynamics. Int. J. Cardiol. 2012, 158, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.A.; Naish, J.; Bishop, P.; Coutts, G.; Clark, D.; Zhao, S.; Ray, S.G.; Yonan, N.; Williams, S.G.; Flett, A.S.; et al. Comprehensive Validation of Cardiovascular Magnetic Resonance Techniques for the Assessment of Myocardial Extracellular Volume. Circ. Cardiovasc. Imaging 2013, 6, 373–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iles, L.; Pfluger, H.; Phrommintikul, A.; Cherayath, J.; Aksit, P.; Gupta, S.N.; Kaye, D.M.; Taylor, A.J. Evaluation of Diffuse Myocardial Fibrosis in Heart Failure with Cardiac Magnetic Resonance Contrast-Enhanced T1 Mapping. J. Am. Coll. Cardiol. 2008, 52, 1574–1580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, J.C.; Messroghli, D.R.; Kellman, P.; Piechnik, S.K.; Robson, M.D.; Ugander, M.; Gatehouse, P.D.; Arai, A.; Friedrich, M.G.; Neubauer, S.; et al. Myocardial T1 mapping and extracellular volume quantification: A Society for Cardiovascular Magnetic Resonance (SCMR) and CMR Working Group of the European Society of Cardiology consensus statement. J. Cardiovasc. Magn. Reson. 2013, 15, 92. [Google Scholar] [CrossRef] [Green Version]
- Garg, P.; Assadi, H.; Jones, R.; Bin Chan, W.; Metherall, P.; Thomas, R.; van der Geest, R.; Swift, A.J.; Al-Mohammad, A. Left ventricular fibrosis and hypertrophy are associated with mortality in heart failure with preserved ejection fraction. Sci. Rep. 2021, 11, 617. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- Mascherbauer, J.; Marzluf, B.A.; Tufaro, C.; Pfaffenberger, S.; Graf, A.; Wexberg, P.; Panzenböck, A.; Jakowitsch, J.; Bangert, C.; Laimer, D.; et al. Cardiac Magnetic Resonance Postcontrast T1 Time Is Associated with Outcome in Patients with Heart Failure and Preserved Ejection Fraction. Circ. Cardiovasc. Imaging 2013, 6, 1056–1065. [Google Scholar] [CrossRef] [Green Version]
- Duca, F.; Kammerlander, A.A.; Zotter-Tufaro, C.; Aschauer, S.; Schwaiger, M.L.; Marzluf, B.A.; Bonderman, D.; Mascherbauer, J. Interstitial Fibrosis, Functional Status, and Outcomes in Heart Failure with Preserved Ejection Fraction. Circ. Cardiovasc. Imaging 2016, 9, e005277. [Google Scholar] [CrossRef] [Green Version]
- Schelbert, E.B.; Fridman, Y.; Wong, T.C.; Abu Daya, H.; Piehler, K.M.; Kadakkal, A.; Miller, C.; Ugander, M.; Maanja, M.; Kellman, P.; et al. Temporal Relation between Myocardial Fibrosis and Heart Failure with Preserved Ejection Fraction: Association with Baseline Disease Severity and Subsequent Outcome. JAMA Cardiol. 2017, 2, 995–1006. [Google Scholar] [CrossRef]
- Roy, C.; Slimani, A.; De Meester, C.; Amzulescu, M.; Pasquet, A.; Vancraeynest, D.; Beauloye, C.; Vanoverschelde, J.-L.; Gerber, B.L.; Pouleur, A.-C. Associations and prognostic significance of diffuse myocardial fibrosis by cardiovascular magnetic resonance in heart failure with preserved ejection fraction. J. Cardiovasc. Magn. Reson. 2018, 20, 55. [Google Scholar] [CrossRef] [Green Version]
- Kanagala, P.; Cheng, A.S.; Singh, A.; Khan, J.N.; Gulsin, G.S.; Patel, P.; Gupta, P.; Arnold, J.R.; Squire, I.B.; Ng, L.L.; et al. Relationship between Focal and Diffuse Fibrosis Assessed by CMR and Clinical Outcomes in Heart Failure with Preserved Ejection Fraction. JACC Cardiovasc. Imaging 2019, 12, 2291–2301. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Du, Y.; Liu, Z.; Zhang, R.; Lin, X.; Ouyang, Y.; Chen, H. Triglyceride–Glucose Index and Extracellular Volume Fraction in Patients with Heart Failure. Front. Cardiovasc. Med. 2021, 8, 704462. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Sample Size | Study Design | Follow-Up (Months) | Magnetic Field Strength (Tesla) | Myocardial T1 Parameter | Events (n, %) | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Mascherbauer [9] | 2013 | 100 (63 *) | Prospective single-center study | 22.9 ± 5.0 | 1.5 T | T1 time | 16 (25.4%) | 13 patients were hospitalized for HF; 3 patients died |
| Duca [10] | 2016 | 117 | Prospective single-center study | 24.0 | 1.5 T | ECV, native T1 | 34 (29%) | 30 patients were hospitalized for HF; 4 patients died |
| Schelbert [11] | 2017 | 1174 (410 *) | Prospective single-center study | 22.8 | 1.5 T | ECV | 61 (14.9%) | 19 patients were hospitalized for HF; 48 patients died; 6 did both |
| Roy [12] | 2018 | 118 | Prospective single-center study | 11 ± 6 | 3.0 T | ECV Native myocardial T1 time (ms) | 43 (36.4%) | 32 patients were hospitalized for HF; 11 patients died |
| Kanagala [13] | 2019 | 232 | Prospective single-center study | 48.2 | 3.0 T | Native myocardial T1 time (ms), postcontrast myocardial T1 time (ms), ECV | 42 (18.1%) | 28 patients were hospitalized for HF; 14 patients died |
| Yang [14] | 2021 | 103 | Retrospective single-center study | 12.3 | 3.0 T | ECV | 39 (37.9%) | 39 patients reached the composite primary outcome |
| Garg [6] | 2021 | 86 | Retrospective single-center study | 38.4 | 1.5 T | Native T1 values (ms) | 27 (31%) | 27 patients reached the endpoint of all-cause mortality |
| Study | Age (Years) | Male Gender, Number (%) | LVEF | LGE Prevalence (%) | NYHA Functional Class III-IV (n, %) | Beta-Blockers (n, %) | ACE-I or ARB (n, %) | MRA (n, %) | Diuretics Other Than MRA (n, %) | NT-proBNP, pg/mL | LV Mass Index, g/m2 | E/E‘ Ratio | LAVI, ml/m2 | ECV |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mascherbauer, 2013 [9] | 70 ± 7 | 38 (40) | 64 ± 10 | - | - | - | - | - | - | 1343 ± 1178 | 59.5 ± 17.7 | - | - | - |
| Duca, 2016 [10] | 74 ± 8 | 36 (31) | 63 ± 10 | - | 71 (61) | - | - | - | - | 833 (396 to 1892) £ | 56.4 ± 13.2 | - | - | 29.3 ± 3.9 |
| Schelbert, 2017 [11] | 56 [44–66] | 637 (54) | - | 301 (25.6) | - | 255 (62) | 175 (43) | 176 (43) | - | - | - | - | - | |
| Roy, 2018 [12] | 78 ± 8 | 37 (31) | 64 ± 7 | 26 (22) | 53 (45) | 76 (64) | 76 (64) | 23 (19) | 94 (80) | 1747 (374 to 34,306) £ | 68 ± 15 | 18.1 ± 7.3 | 66 ± 29 | 32.9 ± 4.8 |
| Kanagala, 2019 [13] | 73 ± 8 | 67 (49) | 56 ± 6 | 49 (51) | 28 (29) | 68 (71) | 82 (85) | 31 (32) | 76 (79) | 144 [66–250] * | 51 ± 13 | 12.8 ± 4.8 | 54 ± 27 | 27.8 ± 4.6 |
| Yang, 2021 [14] | 58 ± 9 | 71 (69) | 49 [39–59] | 48 (46.6) | 71 (68.9) | 73 (70.9) | 81 (78.6) | 5723 [3259–8292] | 36.5 [33.4–39.6] | |||||
| Garg, 2021 [6] | 78 ± 9 | 52 (61) | 59 ± 12.4 | - | - | - | - | - | - | - | - | - | - | - |
| Study | CMR Mapping Parameters | Unadjusted HR | 95% CI | p | Adjusted HR | 95% CI | p | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Mascherbauer, 2013 [9] | Postcontrast T1 time (ms) | 0.99 | 0.98–0.99 | 0.01 | - | - | - | Hospitalization for heart failure or death from cardiovascular causes |
| Duca, 2016 [10] | ECV (%) | 1.132 | 1.049–1.222 | 0.001 | 1.099 | 1.005–1.201 | 0.038 | Hospitalization for heart failure or death from cardiovascular causes |
| Native myocardial T1 time (ms) | 1.005 | 0.999–1.011 | 0.103 | - | - | - | ||
| Schelbert, 2017 [11] | ECV (per 5% ECV increase) | 1.93 | 1.50–2.50 | < 0.001 | 1.52 | 1.05–2.21 | 0.03 | Hospitalization for heart failure or death from cardiovascular causes |
| ECV (per 1% ECV increase), | 1.14 | 1.08–1.20 | < 0.001 | 1.09 | 1.01–1.17 | 0.03 | ||
| Roy, 2018 [12] | ECV (%) | 1.07 | 1.01–1.12 | 0.015 | 1.07 * | 1.01–1.13 | 0.037 | Combination of all-cause mortality or the first hospitalization for heart failure |
| Native myocardial T1 time (ms) | 1.01 | 0.99–1.01 | 0.23 | - | - | - | ||
| Kanagala, 2019 [13] | ECV (%) | 1.519 | 1.076–2.145 | 0.018 | - | - | - | Death and/or hospitalization for heart failure |
| iECV (mL/m2) | 1.69 | 1.107–2.113 | 0.01 | |||||
| Yang, 2021 [14] | ECV fraction (every doubling) | 1.98 | 1.10–3.56 | 0.02 | 1.73 | 1.04–2.88 | 0.03 | All-cause mortality and heart failure hospitalization |
| Garg, 2021 [6] | Native myocardial T1 time (ms) | 2.36 | 0.88–6.38 | NR | - | - | - | All-cause mortality |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Golukhova, E.; Bulaeva, N.; Alexandrova, S.; Gromova, O.; Berdibekov, B. Prognostic Value of Characterizing Myocardial Tissue by Cardiac MRI with T1 Mapping in HFpEF Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 2531. https://doi.org/10.3390/jcm11092531
Golukhova E, Bulaeva N, Alexandrova S, Gromova O, Berdibekov B. Prognostic Value of Characterizing Myocardial Tissue by Cardiac MRI with T1 Mapping in HFpEF Patients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(9):2531. https://doi.org/10.3390/jcm11092531
Chicago/Turabian StyleGolukhova, Elena, Naida Bulaeva, Svetlana Alexandrova, Olga Gromova, and Bektur Berdibekov. 2022. "Prognostic Value of Characterizing Myocardial Tissue by Cardiac MRI with T1 Mapping in HFpEF Patients: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 9: 2531. https://doi.org/10.3390/jcm11092531
APA StyleGolukhova, E., Bulaeva, N., Alexandrova, S., Gromova, O., & Berdibekov, B. (2022). Prognostic Value of Characterizing Myocardial Tissue by Cardiac MRI with T1 Mapping in HFpEF Patients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(9), 2531. https://doi.org/10.3390/jcm11092531