
Assessment of Adherence to Insulin Injections among Diabetic Patients on Basal-Bolus Regimen in Primary and Secondary Healthcare Centers in Al-Jouf Region of Saudi Arabia; A Descriptive Analysis

 ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Adherence to Insulin Doses
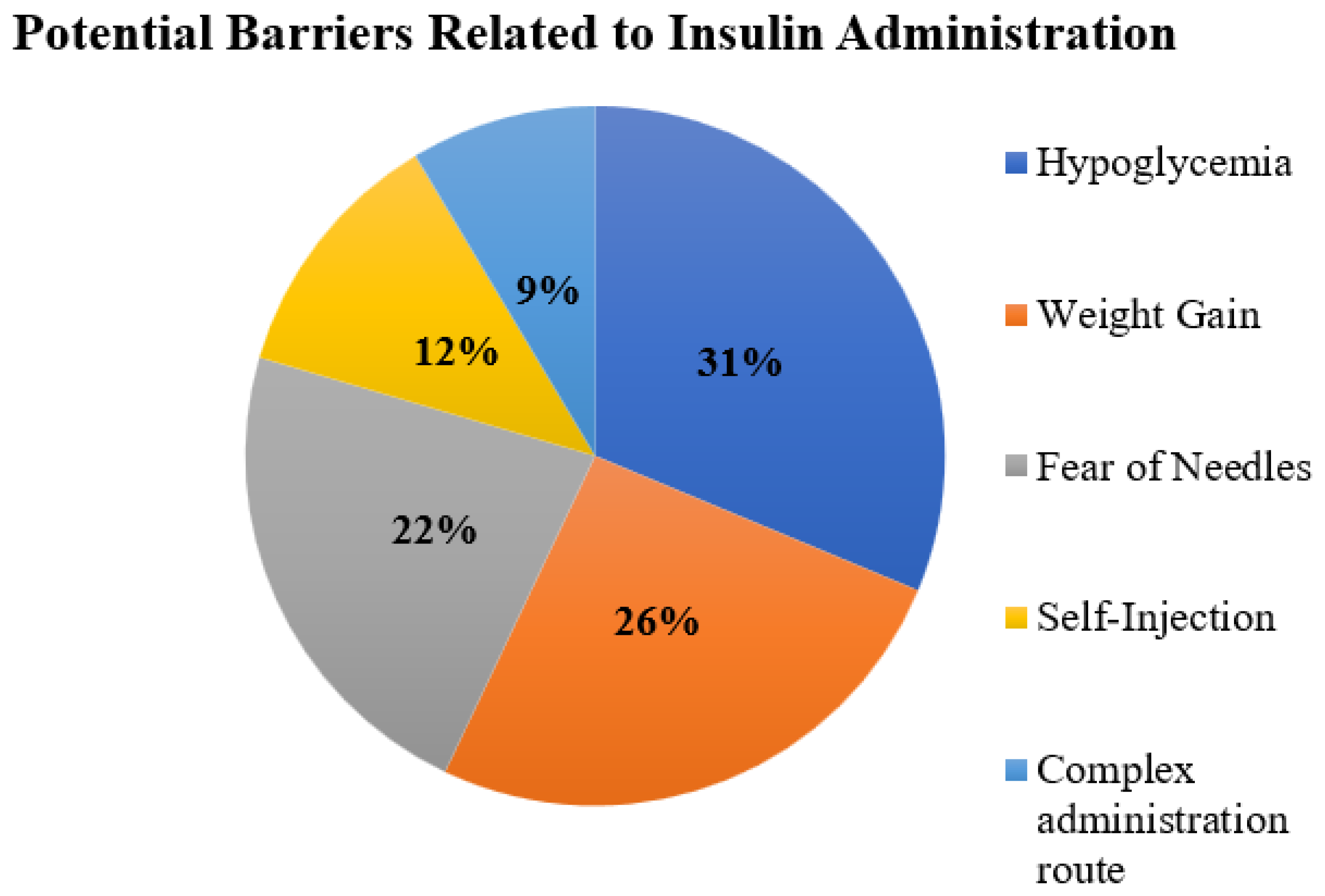
3.2. Self-Reported Barriers Experienced by the Patients during Insulin Administration
3.3. Difficulties among Diabetic Patients during Insulin Use
3.4. Self-Reported Factors Improving Adherence to Insulin Injections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kumar, R.; Saha, P.; Kumar, Y.; Sahana, S.; Dubey, A.; Prakash, O. A Review on Diabetes Mellitus: Type1 & Type2. World J. Pharm. Pharm. Sci. 2020, 9, 838–850. [Google Scholar]
- Chawla, A.; Chawla, R.; Jaggi, S. Microvasular and macrovascular complications in diabetes mellitus: Distinct or continuum? Indian J. Endocrinol. Metab. 2016, 20, 546. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Bullard, K.M.; Cowie, C.C.; Lessem, S.E.; Saydah, S.H.; Menke, A.; Geiss, L.S.; Orchard, T.J.; Rolka, D.B.; Imperatore, G. Prevalence of diagnosed diabetes in adults by diabetes type—United States, 2016. Morb. Mortal. Wkly. Rep. 2018, 67, 359. [Google Scholar] [CrossRef]
- Cole, J.B.; Florez, J.C. Genetics of diabetes mellitus and diabetes complications. Nat. Rev. Nephrol. 2020, 16, 377–390. [Google Scholar] [CrossRef]
- Mauricio, D.; Alonso, N.; Gratacòs, M. Chronic diabetes complications: The need to move beyond classical concepts. Trends Endocrinol. Metab. 2020, 31, 287–295. [Google Scholar] [CrossRef]
- Cahn, A.; Miccoli, R.; Dardano, A.; Del Prato, S. New forms of insulin and insulin therapies for the treatment of type 2 diabetes. Lancet Diabetes Endocrinol. 2015, 3, 638–652. [Google Scholar] [CrossRef]
- Harrison, L.B.; Adams-Huet, B.; Raskin, P.; Lingvay, I. β-cell function preservation after 3.5 years of intensive diabetes therapy. Diabetes Care 2012, 35, 1406–1412. [Google Scholar] [CrossRef]
- Wallace, T.M.; Matthews, D.R. Poor glycaemic control in type 2 diabetes: A conspiracy of disease, suboptimal therapy and attitude. Qjm 2000, 93, 369–374. [Google Scholar] [CrossRef]
- Mariye, T.; Girmay, A.; Birhanu, T.; Tasew, H.; Teklay, G.; Baraki, Z.; Gerensea, H.; Teklu, T.; Bezabeh, G. Adherence to insulin therapy and associated factors among patients with diabetes mellitus in public hospitals of Central Zone of Tigray, Ethiopia, 2018: A cross-sectional study. Pan Afr. Med. J. 2019, 33, 309. [Google Scholar] [CrossRef]
- Khan, A.R.; Lateef, Z.N.A.A.; Al Aithan, M.A.; Bu-Khamseen, M.A.; Al Ibrahim, I.; Khan, S.A. Factors contributing to non-compliance among diabetics attending primary health centers in the Al Hasa district of Saudi Arabia. J. Fam. Community Med. 2012, 19, 26. [Google Scholar] [CrossRef] [PubMed]
- Batais, M.A.; Schantter, P. Prevalence of unwillingness to use insulin therapy and its associated attitudes amongst patients with Type 2 diabetes in Saudi Arabia. Prim. Care Diabetes 2016, 10, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Alsayed, K.A.; Ghoraba, M.K. Assessment of diabetic patients’ adherence to insulin injections on basal-bolus regimen in diabetic care center in Saudi Arabia 2018: Cross sectional survey. J. Fam. Med. Prim. Care 2019, 8, 1964. [Google Scholar] [CrossRef] [PubMed]
- Nasruddin, A.Z.R.I.; Bachok, N.A.; Hassan, N.B.; Naing, N.N. Insulin adherence and associated factors in patients with type 2 diabetes mellitus treated in Klang primary health care centres. Malays. J. Med. Sci. MJMS 2021, 28, 76. [Google Scholar] [CrossRef]
- Gerada, Y.; Mengistu, Z.; Demessie, A.; Fantahun, A.; Gebrekirstos, K. Adherence to insulin self administration and associated factors among diabetes mellitus patients at Tikur Anbessa specialized hospital. J. Diabetes Metab. Disord. 2017, 16, 28. [Google Scholar] [CrossRef]
- Al Futaisi, A.; Alosali, M.; Al-Kazrooni, A.; Al-Qassabi, S.; Al-Gharabi, S.; Panchatcharam, S.; Al-Mahrezi, A.M. Assessing Barriers to Insulin Therapy among Omani Diabetic Patients Attending Three Main Diabetes Clinics in Muscat, Oman. Sultan Qaboos Univ. Med. J. 2022, 22, 525. [Google Scholar] [CrossRef]
- Yavuz, D.G.; Ozcan, S.; Deyneli, O. Adherence to insulin treatment in insulin-naïve type 2 diabetic patients initiated on different insulin regimens. Patient Prefer. Adherence 2015, 9, 1225–1231. [Google Scholar] [CrossRef]
- Alalhareth, S.M.Y.; Alyami, S.H.S.; Kuzman, M.H.H.; Kazman, M.M.H.; Al Hodisan, S.M.; Al Hadaisan, T.M.; Al Juraib, M.H.M.; Balhareth, F.H.M. Cardiovascular Diseases and Diabetes Mellitus in Saudi Arabia. Ann. Clin. Anal. Med. 2022, 10, 180–185. [Google Scholar]
- Al Hayek, A.A.; Robert, A.A.; Al Dawish, M.A.; Zamzami, M.M.; Sam, A.E.; Alzaid, A.A. Impact of an education program on patient anxiety, depression, glycemic control, and adherence to self-care and medication in Type 2 diabetes. J. Fam. Community Med. 2013, 20, 77. [Google Scholar] [CrossRef]
- Alanazi, F.; Gay, V.; Alturki, R. Poor Compliance of Diabetic Patients with AI-Enabled E-Health Self-Care Management in Saudi Arabia. Information 2022, 13, 509. [Google Scholar] [CrossRef]
- Al-Qahtani, S.M.; Shati, A.A.; Alqahtani, Y.A.; AlAsmari, A.A.; Almahdi, M.A.; Al Hassan, A.A.; Alhassany, A.M.; Shathan, R.A.; Aldosari, R.M.; AlQahtani, A.S.; et al. Factors affecting glycemic control among Saudi children with type 1 diabetes mellitus in Aseer region, southwestern Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 11558. [Google Scholar] [CrossRef] [PubMed]
- Jaam, M.; Ibrahim, M.I.M.; Kheir, N.; Awaisu, A. Factors associated with medication adherence among patients with diabetes in the Middle East and North Africa region: A systematic mixed studies review. Diabetes Res. Clin. Pract. 2017, 129, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Almaghaslah, D.; Abdelrhman, A.K.; AL-Masdaf, S.K.; Majrashi, L.M.; Matary, B.M.; Asiri, W.M.; Alqhatani, B.A. Factors contributing to non-adherence to insulin therapy among type 1 and type2 diabetes mellitus patients in Asser region, Saudi Arabia. Biomed. Res. 2018, 29, 2090–2095. [Google Scholar] [CrossRef]
- Davies, M.J.; Gagliardino, J.J.; Gray, L.J.; Khunti, K.; Mohan, V.; Hughes, R. Real-world factors affecting adherence to insulin therapy in patients with Type 1 or Type 2 diabetes mellitus: A systematic review. Diabet. Med. 2013, 30, 512–524. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Newson, R.S.; Liao, B.; Kennedy-Martin, T.; Battelino, T. Missed and mistimed insulin doses in people with diabetes: A systematic literature review. Diabetes Technol. Ther. 2021, 23, 844–856. [Google Scholar] [CrossRef] [PubMed]
- Harashima, S.-I.; Nishimura, A.; Inagaki, N. Attitudes of patients and physicians to insulin therapy in Japan: An analysis of the Global Attitude of Patients and Physicians in Insulin Therapy study. Expert Opin. Pharmacother. 2017, 18, 5–11. [Google Scholar] [CrossRef]
- Peyrot, M.; Barnett, A.H.; Meneghini, L.F.; Schumm-Draeger, P.M. Insulin adherence behaviours and barriers in the multinational Global Attitudes of Patients and Physicians in Insulin Therapy study. Diabet. Med. 2012, 29, 682–689. [Google Scholar] [CrossRef]
- Smythe, K.; Saw, M.; Mak, M.; Wong, V.W. Carbohydrate knowledge, lifestyle and insulin: An observational study of their association with glycaemic control in adults with type 1 diabetes. J. Hum. Nutr. Diet. 2018, 31, 597–602. [Google Scholar] [CrossRef]
- Al-Salmi, N.; Cook, P.; D’souza, M.S. Diet adherence among adults with type 2 diabetes mellitus: A concept analysis. Oman Med. J. 2022, 37, e361. [Google Scholar] [CrossRef]
- Olamoyegun, M.A.; Akinlade, A.T.; Ala, O.A. Audit of insulin prescription patterns and associated burden among diabetics in a tertiary health institution in Nigeria. Afr. Health Sci. 2018, 18, 852–864. [Google Scholar] [CrossRef]
- Peyrot, M.; Rubin, R.R.; Kruger, D.F.; Travis, L.B. Correlates of insulin injection omission. Diabetes Care 2010, 33, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Brod, M.; Rana, A.; Barnett, A.H. Adherence patterns in patients with type 2 diabetes on basal insulin analogues: Missed, mistimed and reduced doses. Curr. Med. Res. Opin. 2012, 28, 1933–1946. [Google Scholar] [CrossRef] [PubMed]
- Khan, Y.H.; Alzarea, A.I.; Alotaibi, N.H.; Alatawi, A.D.; Khokhar, A.; Alanazi, A.S.; Butt, M.H.; Alshehri, A.A.; Alshehri, S.; Alatawi, Y.; et al. Evaluation of Impact of a Pharmacist-Led Educational Campaign on Disease Knowledge, Practices and Medication Adherence for Type-2 Diabetic Patients: A Prospective Pre-and Post-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 10060. [Google Scholar] [CrossRef]
- Mallhi, T.H.; Liaqat, A.; Abid, A.; Khan, Y.H.; Alotaibi, N.H.; Alzarea, A.I.; Tanveer, N.; Khan, T.M. Multilevel engagements of pharmacists during the COVID-19 pandemic: The way forward. Front. Public Health 2020, 8, 561924. [Google Scholar] [CrossRef] [PubMed]
- Larkin, M.; Capasso, V.; Chen, C.L.; Mahoney, E.; Hazard, B.; Cagliero, E.; Nathan, D.M. Measuring Psychological Insulin Resistance: Barriers to Insulin Use. Diabetes 2007, 56, 511–517. [Google Scholar]
- Ross, S.A.; Tildesley, H.D.; Ashkenas, J. Barriers to effective insulin treatment: The persistence of poor glycemic control in type 2 diabetes. Curr. Med. Res. Opin. 2011, 27 (Suppl. S3), 13–20. [Google Scholar] [CrossRef] [PubMed]
- Shafie Pour, M.R.; Sadeghiyeh, T.; Hadavi, M.; Besharati, M.; Bidaki, R. The barriers against initiating insulin therapy among patients with diabetes living in Yazd, Iran. Diabetes Metab. Syndr. Obes. 2019, 12, 1349–1354. [Google Scholar] [CrossRef]
- Schaper, N.C.; Nikolajsen, A.; Sandberg, A.; Buchs, S.; Bøgelund, M. Timing of insulin injections, adherence, and glycemic control in a multinational sample of people with type 2 diabetes: A cross-sectional analysis. Diabetes Ther. 2017, 8, 1319–1329. [Google Scholar] [CrossRef]
- Evans, M.; Jensen, H.H.; Bøgelund, M.; Gundgaard, J.; Chubb, B.; Khunti, K. Flexible insulin dosing improves health-related quality-of-life (HRQoL): A time trade-off survey. J. Med. Econ. 2013, 16, 1357–1365. [Google Scholar] [CrossRef]
- Groleau, D.; Evans, M.; Jensen, H.H.; Bøgelund, M.; Gundgaard, J.; Chubb, B.; Khunti, K. Flexible Insulin Dosing Improves Health-Related Quality of Life (HRQoL): A Time Trade-off Survey. Can. J. Diabetes 2013, 37, S38–S39. [Google Scholar] [CrossRef]
- Abu Hassan, H.; Tohid, H.; Mohd Amin, R.; Long Bidin, M.B.; Muthupalaniappen, L.; Omar, K. Factors influencing insulin acceptance among type 2 diabetes mellitus patients in a primary care clinic: A qualitative exploration. BMC Fam. Pract. 2013, 14, 164. [Google Scholar] [CrossRef] [PubMed]
- Hayes, R.P.; Bowman, L.; Monahan, P.O.; Marrero, D.G.; McHorney, C.A. Understanding diabetes medications from the perspective of patients with type 2 diabetes. Diabetes Educ. 2006, 32, 404–414. [Google Scholar] [CrossRef] [PubMed]
- Brod, M.; Kongsø, J.H.; Lessard, S.; Christensen, T.L. Psychological insulin resistance: Patient beliefs and implications for diabetes management. Qual. Life Res. 2009, 18, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Allen, N.A.; Zagarins, S.E.; Feinberg, R.G.; Welch, G. Treating psychological insulin resistance in type 2 diabetes. J. Clin. Transl. Endocrinol. 2017, 7, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Nazar, C.M.J.; Bojerenu, M.M.; Safdar, M.; Marwat, J. Effectiveness of diabetes education and awareness of diabetes mellitus in combating diabetes in the United Kigdom: A literature review. J. Nephropharmacology 2016, 5, 110. [Google Scholar]
- Mokabel, F.M.; Aboulazm, S.F.; Hassan, H.E.; Al-Qahtani, M.F.; Alrashedi, S.F.; Zainuddin, F.A. The efficacy of a diabetic educational program and predictors of compliance of patients with noninsulin-dependent (type 2) diabetes mellitus in Al-Khobar, Saudi Arabia. J. Fam. Community Med. 2017, 24, 164. [Google Scholar] [CrossRef]
- Alanazi, F.K.; Alotaibi, J.S.; Paliadelis, P.; Alqarawi, N.; Alsharari, A.; Albagawi, B. Knowledge and awareness of diabetes mellitus and its risk factors in Saudi Arabia. Saudi Med. J. 2018, 39, 981. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Frequency (n) | Proportion (%) |
|---|---|---|
| Age | ||
| 14–29 Years | 84 | 20.2 |
| 30–44 Years | 98 | 23.6 |
| 45–60 Years | 129 | 31.1 |
| >60 Years | 104 | 25.1 |
| Gender | ||
| Male | 201 | 48.4 |
| Female | 214 | 51.6 |
| Education Level | ||
| Illiterate—No Formal Education | 32 | 7.7 |
| Primary School | 61 | 14.7 |
| Secondary School | 61 | 14.7 |
| High School | 128 | 30.8 |
| Graduate | 104 | 25.1 |
| Postgraduate | 29 | 7.0 |
| Type of Diabetes Mellitus | ||
| Not Sure | 121 | 29.2 |
| T1DM | 88 | 21.2 |
| T2DM | 206 | 49.6 |
| Duration of Diabetes Mellitus | ||
| <2 Years | 56 | 13.5 |
| 2–5 Years | 109 | 26.3 |
| 6–10 Years | 129 | 31.1 |
| >10 Years | 121 | 29.2 |
| Follow-up Facilities | ||
| No Routine Follow up | 108 | 26.0 |
| Primary Healthcare | 69 | 16.6 |
| Int Med/Endocrine Govt Hosp | 196 | 47.2 |
| Private Hospitals/Clinics | 42 | 10.1 |
| Pattern of Follow-up for Diabetes Care in Last Year | ||
| Never Missed Follow-Up | 187 | 45.1 |
| Missed 1–2 Appointments | 89 | 21.4 |
| Missed > 2 Appointments | 45 | 10.8 |
| No Follow-up/Appointment Last Year | 94 | 22.7 |
| Diabetes control | ||
| Uncontrolled | 171 | 41.2 |
| Controlled | 244 | 58.8 |
| Presence of Chronic Diseases | ||
| Yes | 217 | 52.3 |
| No | 198 | 47.7 |
| Hypertension | ||
| Yes | 83 | 20.0 |
| No | 332 | 80.0 |
| Thyroid Disorders | ||
| Yes | 47 | 11.3 |
| No | 368 | 88.7 |
| Hyperlipidemia | ||
| Yes | 86 | 20.7 |
| No | 329 | 79.3 |
| Chronic Kidney Disease | ||
| Yes | 18 | 4.3 |
| No | 397 | 95.7 |
| Others Chronic Diseases | ||
| Yes | 26 | 6.3 |
| No | 389 | 93.7 |
| Overall (N = 415) | Patients with T1DM (n = 88) | Patients with T2DM (n = 206) | Patients Who Were Not Aware of Type of DM (n = 121) | p Values | |
|---|---|---|---|---|---|
| Do you forget to take insulin? | <0.001 | ||||
| Yes | 169 (40.7%) | 51 (58%) | 68 (33%) | 50 (41.3%) | |
| No | 246 (59.3%) | 37 (42%) | 138 (67%) | 71 (58.7%) | |
| How many doses do you miss in a week? | 0.012 | ||||
| I do not miss any dose | 246 (59.3%) | 37 (42%) | 138 (67%) | 71 (58.7%) | |
| 1–2 doses | 65 (15.7%) | 22 (25%) | 24 (11.7%) | 19 (15.7%) | |
| 3–4 doses | 57 (13.7%) | 17 (19.3%) | 26 (12.6%) | 14 (11.6%) | |
| 5–6 doses | 26 (6.3%) | 8 (9.1%) | 9 (4.4%) | 9 (7.4%) | |
| Greater than 6 doses | 21 (5.1%) | 4 (4.5%) | 9 (4.4%) | 8 (6.6%) |
| Reasons for Missing Insulin Doses | Frequency (n) | Proportion (%) |
|---|---|---|
| Away from home | 61 | 36.1 |
| I cannot adhere to dietary regimen | 41 | 24.3 |
| Feeling embarrassed to take it in public | 40 | 23.7 |
| The time to take it is not appropriate | 31 | 18.3 |
| Forget | 26 | 15.4 |
| Took only when blood sugar is high | 22 | 13.0 |
| Time consuming | 17 | 10.1 |
| Regimen is complex | 15 | 8.9 |
| Fear of injection pain | 7 | 4.1 |
| Ran out of medication | 7 | 4.1 |
| Took only when felt sick | 4 | 2.4 |
| Factors | Frequency (n) | Proportion (%) |
|---|---|---|
| Minimize number of injections | ||
| Yes | 128 | 30.8 |
| No | 287 | 69.2 |
| Convenient time regimen | ||
| Yes | 123 | 29.6 |
| No | 292 | 70.4 |
| Confidence in taking medication in public | ||
| Yes | 93 | 22.4 |
| No | 322 | 77.6 |
| Belief in efficacy of the treatment | ||
| Yes | 41 | 9.9 |
| No | 374 | 90.1 |
| Social Support | ||
| Yes | 79 | 19.0 |
| No | 336 | 81.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsaidan, A.A.; Alsaidan, O.A.; Mallhi, T.H.; Khan, Y.H.; Alzarea, A.I.; Alanazi, A.S. Assessment of Adherence to Insulin Injections among Diabetic Patients on Basal-Bolus Regimen in Primary and Secondary Healthcare Centers in Al-Jouf Region of Saudi Arabia; A Descriptive Analysis. J. Clin. Med. 2023, 12, 3474. https://doi.org/10.3390/jcm12103474
Alsaidan AA, Alsaidan OA, Mallhi TH, Khan YH, Alzarea AI, Alanazi AS. Assessment of Adherence to Insulin Injections among Diabetic Patients on Basal-Bolus Regimen in Primary and Secondary Healthcare Centers in Al-Jouf Region of Saudi Arabia; A Descriptive Analysis. Journal of Clinical Medicine. 2023; 12(10):3474. https://doi.org/10.3390/jcm12103474
Chicago/Turabian StyleAlsaidan, Aseel Awad, Omar Awad Alsaidan, Tauqeer Hussain Mallhi, Yusra Habib Khan, Abdulaziz Ibrahim Alzarea, and Abdullah Salah Alanazi. 2023. "Assessment of Adherence to Insulin Injections among Diabetic Patients on Basal-Bolus Regimen in Primary and Secondary Healthcare Centers in Al-Jouf Region of Saudi Arabia; A Descriptive Analysis" Journal of Clinical Medicine 12, no. 10: 3474. https://doi.org/10.3390/jcm12103474
APA StyleAlsaidan, A. A., Alsaidan, O. A., Mallhi, T. H., Khan, Y. H., Alzarea, A. I., & Alanazi, A. S. (2023). Assessment of Adherence to Insulin Injections among Diabetic Patients on Basal-Bolus Regimen in Primary and Secondary Healthcare Centers in Al-Jouf Region of Saudi Arabia; A Descriptive Analysis. Journal of Clinical Medicine, 12(10), 3474. https://doi.org/10.3390/jcm12103474