
Incidence of Peri-Implantitis, Technical and Biological Complications of Single Implants Placed with Flap or Flapless Surgery—A 10–12-Year Case-Series

 , , and
, , and
Abstract
:1. Introduction
2. Aim
3. Material and Methods
3.1. Study Group
3.2. Clinical and Radiographic Evaluation
3.3. Statistical Analysis
4. Results
4.1. Study Group
4.2. Treatment Protocol
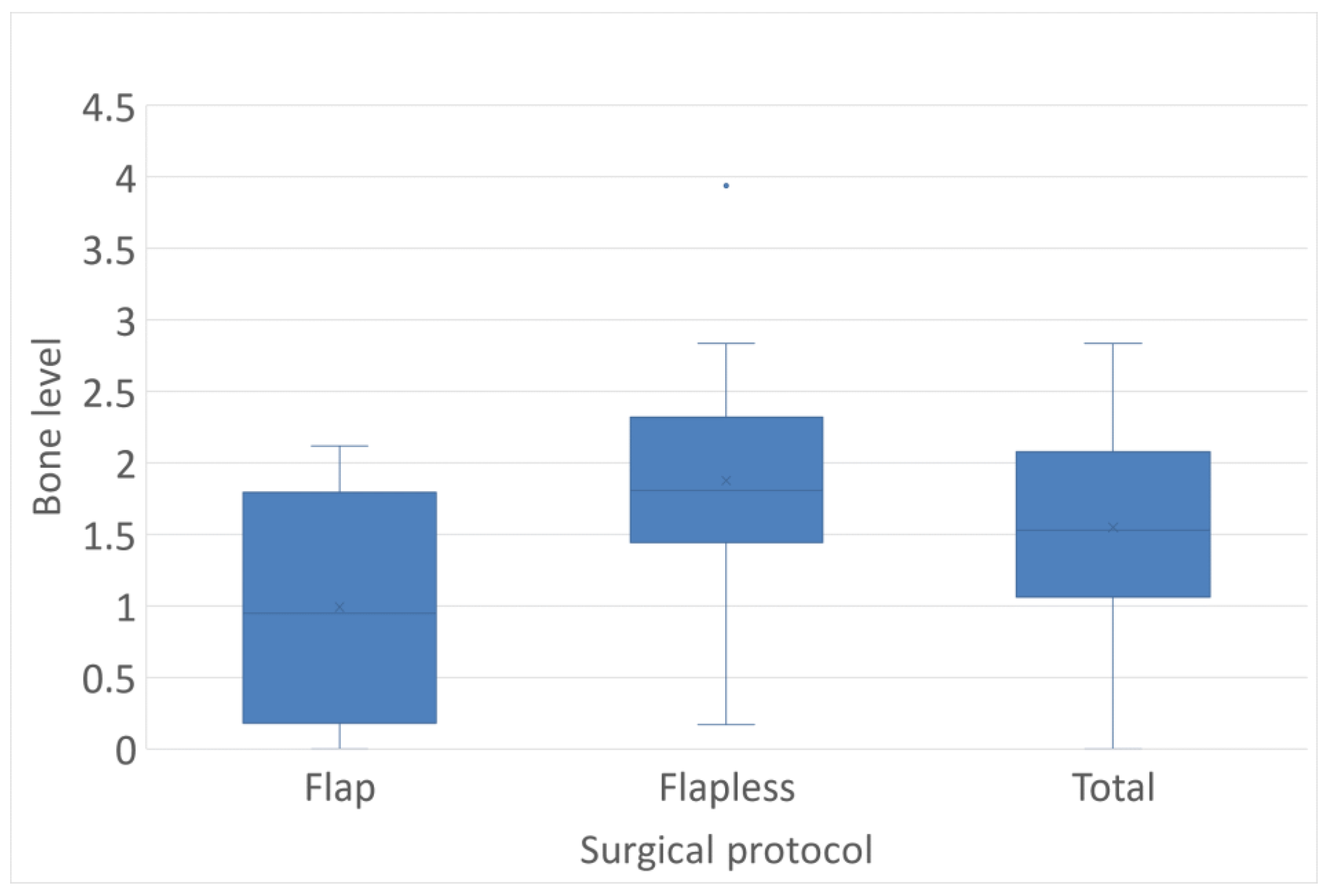
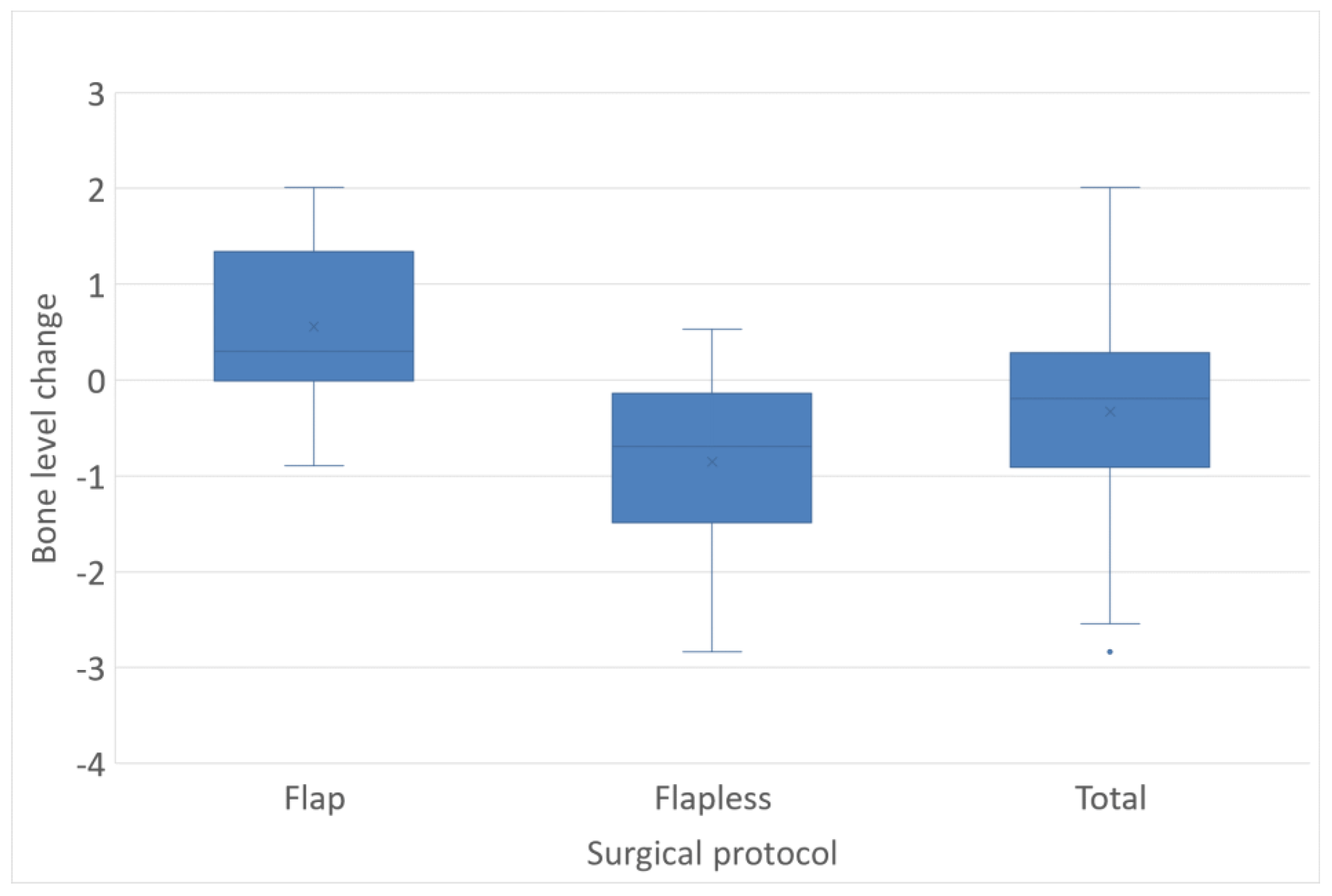
4.3. Bone Level
4.4. Clinical Outcomes
4.5. Peri-Implant Health and Peri-Implantitis
4.6. Complications
5. Discussions
Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buser, D.; Weber, H.P.; Lang, N.P. Tissue integration of non-submerged implants. 1-year results of a prospective study with 100 ITI hollow-cylinder and hollow-screw implants. Clin. Oral Implant. Res. 1990, 1, 33–40. [Google Scholar] [CrossRef]
- Buser, D.; Mericske-Stern, R.; Bernard, J.P.; Behneke, A.; Behneke, N.; Hirt, H.P.; Belser, U.C.; Lang, N.P. Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a prospective multi-center study with 2359 implants. Clin. Oral Implant. Res. 1997, 8, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, I.; Randow, K.; Nilner, K.; Petersson, A. Some clinical and radiographical features of submerged and non-submerged titanium implants. A 5-year follow-up study. Clin. Oral Implant. Res. 1997, 8, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Collaert, B.; De Bruyn, H. Comparison of Branemark fixture integration and short-term survival using one-stage or two-stage surgery in completely and partially edentulous mandibles. Clin. Oral Implant. Res. 1998, 9, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Schenk, R.K.; Steinemann, S.; Fiorellini, J.P.; Fox, C.H.; Stich, H. Influence of surface characteristics on bone integration of titanium implants. A histomorphometric study in miniature pigs. J. Biomed. Mater. Res. 1991, 25, 889–902. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Schmid, B.; Belser, U.C.; Lussi, A.; Buser, D. Early loading of non-submerged titanium implants with a sandblasted and acid-etched surface. 5-year results of a prospective study in partially edentulous patients. Clin. Oral Implant. Res. 2005, 16, 631–638. [Google Scholar] [CrossRef]
- Cochran, D.L.; Buser, D.; Ten Bruggenkate, C.M.; Weingart, D.; Taylor, T.M.; Bernard, J.P.; Peters, F.; Simpson, J.P. The use of reduced healing times on ITI implants with a sandblasted and acid-etched (SLA) surface: Early results from clinical trials on ITI SLA implants. Clin. Oral Implant. Res. 2002, 13, 144–153. [Google Scholar] [CrossRef]
- Sullivan, D.; Vincenzi, G.; Feldman, S. Early loading of Osseotite implants 2 months after placement in the maxilla and mandible: A 5-year report. Int. J. Oral Maxillofac. Implant. 2005, 20, 905–912. [Google Scholar]
- De Bruyn, H.; Raes, S.; Ostman, P.O.; Cosyn, J. Immediate loading in partially and completely edentulous jaws: A review of the literature with clinical guidelines. Periodontol. 2000 2014, 66, 153–187. [Google Scholar] [CrossRef]
- Lazzara, R.J. Immediate implant placement into extraction sites: Surgical and restorative advantages. Int. J. Periodontics Restor. Dent. 1989, 9, 332–343. [Google Scholar]
- Jung, R.E.; Pjetursson, B.E.; Glauser, R.; Zembic, A.; Zwahlen, M.; Lang, N.P. A systematic review of the 5-year survival and complication rates of implant-supported single crowns. Clin. Oral Implant. Res. 2008, 19, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Zembic, A.; Pjetursson, B.E.; Zwahlen, M.; Thoma, D.S. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 2–21. [Google Scholar] [CrossRef] [PubMed]
- Raes, S.; Cosyn, J.; Noyelle, A.; Raes, F.; De Bruyn, H. Clinical Outcome After 8 to 10 Years of Immediately Restored Single Implants Placed in Extraction Sockets and Healed Ridges. Int. J. Periodontics Restor. Dent. 2018, 38, 337–345. [Google Scholar] [CrossRef]
- Jemt, T. Single-Implant Survival: More Than 30 Years of Clinical Experience. Int. J. Prosthodont. 2016, 29, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Dierens, M.; Vandeweghe, S.; Kisch, J.; Nilner, K.; De Bruyn, H. Long-term follow-up of turned single implants placed in periodontally healthy patients after 16–22 years: Radiographic and peri-implant outcome. Clin. Oral Implant. Res. 2012, 23, 197–204. [Google Scholar] [CrossRef]
- Bergenblock, S.; Andersson, B.; Furst, B.; Jemt, T. Long-term follow-up of CeraOne single-implant restorations: An 18-year follow-up study based on a prospective patient cohort. Clin. Implant Dent. Relat. Res. 2012, 14, 471–479. [Google Scholar] [CrossRef]
- Dierens, M.; De Bruyn, H.; Kisch, J.; Nilner, K.; Cosyn, J.; Vandeweghe, S. Prosthetic Survival and Complication Rate of Single Implant Treatment in the Periodontally Healthy Patient after 16 to 22 Years of Follow-Up. Clin. Implant Dent. Relat. Res. 2016, 18, 117–128. [Google Scholar] [CrossRef]
- Lang, N.P.; Berglundh, T. Working Group 4 of Seventh European Workshop on P. Periimplant diseases: Where are we now?--Consensus of the Seventh European Workshop on Periodontology. J. Clin. Periodontol. 2011, 38 (Suppl. 11), 178–181. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.-L. Peri-implantitis. J. Periodontol. 2018, 89, S267–S290. [Google Scholar] [CrossRef]
- Tomasi, C.; Derks, J. Clinical research of peri-implant diseases–quality of reporting, case definitions and methods to study incidence, prevalence and risk factors of peri-implant diseases. J. Clin. Periodontol. 2012, 39 (Suppl. 12), 207–223. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S313–S318. [Google Scholar] [CrossRef]
- Doornewaard, R.; Jacquet, W.; Cosyn, J.; De Bruyn, H. How do peri-implant biologic parameters correspond with implant survival and peri-implantitis? A critical review. Clin. Oral Implant. Res. 2018, 29 (Suppl. 18), 100–123. [Google Scholar] [CrossRef]
- Arisan, V.; Karabuda, C.Z.; Ozdemir, T. Implant surgery using bone- and mucosa-supported stereolithographic guides in totally edentulous jaws: Surgical and post-operative outcomes of computer-aided vs. standard techniques. Clin. Oral Implant. Res. 2010, 21, 980–988. [Google Scholar] [CrossRef]
- Fortin, T.; Bosson, J.L.; Isidori, M.; Blanchet, E. Effect of flapless surgery on pain experienced in implant placement using an image-guided system. Int. J. Oral Maxillofac. Implant. 2006, 21, 298–304. [Google Scholar]
- Sunitha, R.V.; Sapthagiri, E. Flapless implant surgery: A 2-year follow-up study of 40 implants. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, e237–e243. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Flapless versus Conventional Flapped Dental Implant Surgery: A Meta-Analysis. PLoS ONE 2014, 9, e100624. [Google Scholar] [CrossRef] [PubMed]
- Rocci, A.; Martignoni, M.; Gottlow, J. Immediate loading in the maxilla using flapless surgery, implants placed in predetermined positions, and prefabricated provisional restorations: A retrospective 3-year clinical study. Clin. Implant Dent. Relat. Res. 2003, 5 (Suppl. 1), 29–36. [Google Scholar] [CrossRef] [PubMed]
- De Bruyn, H.; Atashkadeh, M.; Cosyn, J.; van de Velde, T. Clinical outcome and bone preservation of single TiUnite implants installed with flapless or flap surgery. Clin. Implant Dent. Relat. Res. 2011, 13, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Van de Velde, T.; Glor, F.; De Bruyn, H. A model study on flapless implant placement by clinicians with a different experience level in implant surgery. Clin. Oral Implant. Res. 2008, 19, 66–72. [Google Scholar] [CrossRef]
- Brodala, N. Flapless surgery and its effect on dental implant outcomes. Int. J. Oral Maxillofac. Implant. 2009, 24, 118–125. [Google Scholar]
- Berdougo, M.; Fortin, T.; Blanchet, E.; Isidori, M.; Bosson, J.L. Flapless implant surgery using an image-guided system. A 1- to 4-year retrospective multicenter comparative clinical study. Clin. Implant Dent. Relat. Res. 2010, 12, 142–152. [Google Scholar] [CrossRef]
- Becker, W.; Wikesjo, U.M.; Sennerby, L.; Qahash, M.; Hujoel, P.; Goldstein, M.; Turkyilmaz, I. Histologic evaluation of implants following flapless and flapped surgery: A study in canines. J. Periodontol. 2006, 77, 1717–1722. [Google Scholar] [CrossRef] [PubMed]
- Katsoulis, J.; Avrampou, M.; Spycher, C.; Stipic, M.; Enkling, N.; Mericske-Stern, R. Comparison of implant stability by means of resonance frequency analysis for flapless and conventionally inserted implants. Clin. Implant Dent. Relat. Res. 2012, 14, 915–923. [Google Scholar] [CrossRef]
- Jesch, P.; Jesch, W.; Bruckmoser, E.; Krebs, M.; Kladek, T.; Seemann, R. An up to 17-year follow-up retrospective analysis of a minimally invasive, flapless approach: 18 945 implants in 7783 patients. Clin. Implant. Dent. Relat. Res. 2018, 20, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Cannizzaro, G.; Soardi, E.; Pistilli, R.; Piattelli, M.; Corvino, V.; Felice, P. Posterior atrophic jaws rehabilitated with prostheses supported by 6 mm-long, 4 mm-wide implants or by longer implants in augmented bone. Preliminary results from a pilot randomised controlled trial. Eur. J. Oral Implantol. 2012, 5, 19–33. [Google Scholar] [PubMed]
- Naeini, E.N.; Dierens, M.; Atashkadeh, M.; De Bruyn, H. Long-term clinical outcome of single implants inserted flaplessly or conventionally. Clin. Implant Dent. Relat. Res. 2018, 20, 829–837. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Silness, J.; Löe, H. Periodontal Disease in Pregnancy II. Correlation Between Oral Hygiene and Periodontal Condition. Acta Odontol. Scand. 1964, 22, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Jemt, T. Regeneration of gingival papillae after single-implant treatment. Int. J. Periodontics Restor. Dent. 1997, 17, 326–333. [Google Scholar]
- De Rouck, T.; Eghbali, R.; Collys, K.; De Bruyn, H.; Cosyn, J. The gingival biotype revisited: Transparency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingiva. J. Clin. Periodontol. 2009, 36, 428–433. [Google Scholar] [CrossRef]
- Fewtrell, M.S.; Kennedy, K.; Singhal, A.; Martin, R.M.; Ness, A.; Hadders-Algra, M.; Koletzko, B.; Lucas, A. How much loss to follow-up is acceptable in long-term randomised trials and prospective studies? Arch. Dis. Child. 2008, 93, 458–461. [Google Scholar] [CrossRef] [PubMed]
- Campelo, L.D.; Camara, J.R. Flapless implant surgery: A 10-year clinical retrospective analysis. Int. J. Oral Maxillofac. Implant. 2002, 17, 271–276. [Google Scholar]
- Ozan, O.; Turkyilmaz, I.; Yilmaz, B. A preliminary report of patients treated with early loaded implants using computerized tomography-guided surgical stents: Flapless versus conventional flapped surgery. J. Oral Rehabil. 2007, 34, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Becker, W.; Goldstein, M.; Becker, B.E.; Sennerby, L. Minimally invasive flapless implant surgery: A prospective multicenter study. Clin. Implant Dent. Relat. Res. 2005, 7 (Suppl. 1), S21–S27. [Google Scholar] [CrossRef] [PubMed]
- Sennerby, L.; Rocci, A.; Becker, W.; Jonsson, L.; Johansson, L.A.; Albrektsson, T. Short-term clinical results of Nobel Direct implants: A retrospective multicentre analysis. Clin. Oral Implant. Res. 2008, 19, 219–226. [Google Scholar] [CrossRef]
- Rousseau, P. Flapless and traditional dental implant surgery: An open, retrospective comparative study. J. Oral Maxillofac. Surg. 2010, 68, 2299–2306. [Google Scholar] [CrossRef]
- Lekholm, U.; Adell, R.; Lindhe, J.; Brånemark, P.I.; Eriksson, B.; Rockler, B.; Lindvall, A.-M.; Yoneyama, T. Marginal tissue reactions at osseointegrated titanium fixtures. (II) A cross-sectional retrospective study. Int. J. Oral Maxillofac. Surg. 1986, 15, 53–61. [Google Scholar] [CrossRef]
- Coli, P.; Christiaens, V.; Sennerby, L.; Bruyn, H. Reliability of periodontal diagnostic tools for monitoring peri-implant health and disease. Periodontol. 2000 2017, 73, 203–217. [Google Scholar] [CrossRef]
- Sanz, M.; Chapple, I.L. Working Group 4 of the VEWoP. Clinical research on peri-implant diseases: Consensus report of Working Group 4. J. Clin. Periodontol. 2012, 39 (Suppl. 12), 202–206. [Google Scholar] [CrossRef]
- Ramanauskaite, A.; Juodzbalys, G. Diagnostic Principles of Peri-Implantitis: A Systematic Review and Guidelines for Peri-Implantitis Diagnosis Proposal. J. Oral Maxillofac. Res. 2016, 7, e8. [Google Scholar] [CrossRef]
- Oh, T.J.; Yoon, J.; Misch, C.E.; Wang, H.L. The causes of early implant bone loss: Myth or science? J. Periodontol. 2002, 73, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Vandeweghe, S.; Cosyn, J.; Thevissen, E.; Van den Berghe, L.; De Bruyn, H. A 1-Year Prospective Study on Co-Axis® Implants Immediately Loaded with a Full Ceramic Crown. Clin. Implant. Dent. Relat. Res. 2012, 14, e126–e138. [Google Scholar] [CrossRef]
- Mombelli, A.; van Oosten, M.A.; Schurch, E., Jr.; Land, N.P. The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiol. Immunol. 1987, 2, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Adler, R.; Joss, A.; Nyman, S. Absence of bleeding on probing. An indicator of periodontal stability. J. Clin. Periodontol. 1990, 17, 714–721. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Lang, N.P. Antimicrobial treatment of peri-implant diseases. Int. J. Oral Maxillofac. Implant. 2004, 19, 128–139. [Google Scholar]
- Cosyn, J.; Thoma, D.S.; Hammerle, C.H.; De Bruyn, H. Esthetic assessments in implant dentistry: Objective and subjective criteria for clinicians and patients. Periodontol. 2000 2017, 73, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Benic, G.I.; Wolleb, K.; Sancho-Puchades, M.; Hammerle, C.H. Systematic review of parameters and methods for the professional assessment of aesthetics in dental implant research. J. Clin. Periodontol. 2012, 39 (Suppl. 12), 160–192. [Google Scholar] [CrossRef]
- Wood, D.L.; Hoag, P.M.; Donnenfeld, O.W.; Rosenfeld, L.D. Alveolar crest reduction following full and partial thickness flaps. J. Periodontol. 1972, 43, 141–144. [Google Scholar] [CrossRef]
- Stoupel, J.; Lee, C.T.; Glick, J.; Sanz-Miralles, E.; Chiuzan, C.; Papapanou, P.N. Immediate implant placement and provisionalization in the aesthetic zone using a flapless or a flap-involving approach: A randomized controlled trial. J. Clin. Periodontol. 2016, 43, 1171–1179. [Google Scholar] [CrossRef]
- Bashutski, J.D.; Wang, H.L.; Rudek, I.; Moreno, I.; Koticha, T.; Oh, T.J. Effect of flapless surgery on single-tooth implants in the esthetic zone: A randomized clinical trial. J. Periodontol. 2013, 84, 1747–1754. [Google Scholar] [CrossRef]
- Zhang, H.; Rokas, A.; Slot, J.C. Two different secondary metabolism gene clusters occupied the same ancestral locus in fungal dermatophytes of the arthrodermataceae. PLoS ONE 2012, 7, e41903. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Tan, K.; Lang, N.P.; Bragger, U.; Egger, M.; Zwahlen, M. A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. Clin. Oral Implant. Res. 2004, 15, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Muhlemann, S.; Zwahlen, M.; Hammerle, C.H.; Schneider, D. Cemented and screw-retained implant reconstructions: A systematic review of the survival and complication rates. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 163–201. [Google Scholar] [CrossRef] [PubMed]
- Millen, C.; Bragger, U.; Wittneben, J.G. Influence of prosthesis type and retention mechanism on complications with fixed implant-supported prostheses: A systematic review applying multivariate analyses. Int. J. Oral Maxillofac. Implant. 2015, 30, 110–124. [Google Scholar] [CrossRef] [PubMed]
- Linkevicius, T.; Puisys, A.; Vindasiute, E.; Linkeviciene, L.; Apse, P. Does residual cement around implant-supported restorations cause peri-implant disease? A retrospective case analysis. Clin. Oral Implant. Res. 2013, 24, 1179–1184. [Google Scholar] [CrossRef]
- Covani, U.; Cornelini, R.; Barone, A. Buccal bone augmentation around immediate implants with and without flap elevation: A modified approach. Int. J. Oral Maxillofac. Implant. 2008, 23, 841–846. [Google Scholar]
- Van de Velde, T.; Sennerby, L.; De Bruyn, H. The clinical and radiographic outcome of implants placed in the posterior maxilla with a guided flapless approach and immediately restored with a provisional rehabilitation: A randomized clinical trial. Clin. Oral Implant. Res. 2010, 21, 1223–1233. [Google Scholar] [CrossRef]
- Al-Juboori, M.J.; Bin Abdulrahaman, S.; Jassan, A. Comparison of flapless and conventional flap and the effect on crestal bone resorption during a 12-week healing period. Dent. Implantol. Update 2012, 23, 9–16. [Google Scholar]
- Malo, P.; Nobre, M. Flap vs. flapless surgical techniques at immediate implant function in predominantly soft bone for rehabilitation of partial edentulism: A prospective cohort study with follow-up of 1 year. Eur. J. Oral Implantol. 2008, 1, 293–304. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Implant Position | Maxilla | Mandible | Total |
|---|---|---|---|
| Incisors | 15 | 2 | 17 |
| Canines | 3 | 0 | 3 |
| Premolars | 10 | 3 | 13 |
| Molars | 3 | 4 | 7 |
| Total | 31 | 9 | 40 |
| Implant Platform (mm) | Flap | Flapless | Total |
|---|---|---|---|
| NP (3.3) | 3 | 3 | 6 |
| RP (3.75–4.0) | 14 | 19 | 33 |
| WP (5) | 0 | 1 | 1 |
| Total | 16 | 22 | 40 |
| Implant Length (mm) | Flap | Flapless | Total |
|---|---|---|---|
| 10 | 1 | 2 | 3 |
| 11.5 | 1 | 3 | 4 |
| 13 | 4 | 8 | 12 |
| 15 | 15 | 5 | 20 |
| 18 | 0 | 1 | 1 |
| Total | 21 | 19 | 40 |
| Total Patient Group | Flap | Flapless | ||
|---|---|---|---|---|
| Number of implants | Follow-up | 40 | 19 | 21 |
| Bone level at follow-up (mm) | Mean (SD; range) | −1.26 (0.8; −4.1–0) | −1.49 (0.9; −4.1–0) | −1.04 (0.66; −2.3–0) |
| Bone loss (mm) | Mean (SD; range) | −0.33 (1.16; −2.84–2.02) | 0.56 (0.89; −0.9–2.02) | −0.85 (0.98; −2.84–0.53) |
| PPD (mm) | Mean (SD; range) | 3.26 (0.87; 1.83–5.33) | 3.32 (0.84; 2.17–4.83) | 3.19 (0.91; 1.83–5.33) |
| BOP | Mean (SD; range) | 0.19 (0.29; 0–1.5) | 0.15 (0.21; 0–0.75) | 0.22 (0.38; 0–1.5) |
| Gingival recession (mm) | Mean (SD; range) | 0.28 (0.52; 0–2) | 0.38 (0.60; 0–2) | 0.17 (0.45; 0–2) |
| Mesial Papilla Height (mm) | Mean (SD; range) | 3.67 (1.58; 0–8) | 3.58 (1.68; 0–8) | 3.76 (1.48; 0–6) |
| Distal Papilla Height (mm) | Mean (SD; range) | 2.69 (1.60; 0–6) | 3.05 (1.51; 0–6) | 2.33 (1.68; 0–5) |
| Bone Loss/Pocket Depth | ≤3 mm | >3 mm & ≤4 mm | >4 mm & ≤5 mm | >5 mm | Total |
|---|---|---|---|---|---|
| <0 mm (bone gain) | 4 (2; 6.3%) | 7 (2; 6.3%) | 4 (3; 9.4%) | 1 (1; 3.1%) | 16 (8; 25%) |
| ≤1 mm | 7 (3; 9.4%) | 2 (1; 3.1%) | 1 (1; 3.1%) | 10 (5; 15.6%) | |
| >1 ≤ 2 mm | 2 (0; 0%) | 1 (0; 0%) | 3 (0; 0%) | ||
| >2 ≤ 3 mm | 2 (0; 0%) | 2 (0; 0%) | |||
| >3 mm | 1 (0; 0%) | 1 (0; 0%) | |||
| Total | 15 | 11 | 5 | 1 | 32 (13; 40.6%) |
| Implant Number | Surgical Protocol F/FL | Crown Retention | Total No. Compl. | Technical Compl. | Biological Compl. | Aesthetic Compl. | Bone Loss | PPD |
|---|---|---|---|---|---|---|---|---|
| 2 | F | C | NR | 4.8 | ||||
| 5 | F | C | −0.17 | 2.5 | ||||
| 8 | F | C | 1 | 1 | −0.44 | 4.2 | ||
| 25 | F | C | 2 | 1 | 1 | −1.50 | 3.5 | |
| 14 | FL | C | 1 | 1 | −0.21 | 5.0 | ||
| 19 | FL | C | 0.18 | 2.0 | ||||
| 29 | FL | C | 5 | 4 | 1 | 2.55 | 2.2 | |
| 35 | FL | C | 0.23 | 2.7 | ||||
| 1 | F | S | −0.05 | 2.2 | ||||
| 4 | F | S | −1.14 | 3.8 | ||||
| 6 | F | S | NR | 2.7 | ||||
| 7 | F | S | 2 | 1 * | 1 | −2.02 | 4.5 | |
| 10 | F | S | NR | 3.2 | ||||
| 11 | F | S | NR | 3.7 | ||||
| 12 | F | S | 0.90 | 3.0 | ||||
| 16 | F | S | NR | 2.5 | ||||
| 17 | F | S | 3 | 1 | 1 | 1 | −0.09 | 2.8 |
| 22 | F | S | NR | 2.3 | ||||
| 24 | F | S | 3 | 3 | NR | 2.8 | ||
| 26 | F | S | 0.20 | 2.7 | ||||
| 39 | F | S | −2.05 | 4.0 | ||||
| 40 | F | S | −2.74 | 3.8 | ||||
| 43 | F | S | −1.28 | 4.7 | ||||
| 23 | FL | S | 2 | 1 | 1 | NR | 2.8 | |
| 27 | FL | S | −1.95 | 5.3 | ||||
| 30 | FL | S | 1 | 1 | 0.69 | 3.5 | ||
| 31 | FL | S | 1 | 1 | 0.59 | 2.3 | ||
| 32 | FL | S | 1 | 1 | 1.69 | 3.3 | ||
| 34 | FL | S | 1.28 | 2.7 | ||||
| 38 | FL | S | 1 | 1 | 0.76 | 3.5 | ||
| 41 | FL | S | 1 | 1 | 0.91 | 3.8 | ||
| 44 | FL | S | 2.09 | 3.3 | ||||
| 45 | FL | S | −0.53 | 3.8 | ||||
| 46 | FL | S | −1.01 | 3.7 | ||||
| 47 | FL | S | 0.11 | 1.8 | ||||
| 49 | FL | S | 2.84 | 2.8 | ||||
| 50 | FL | S | 1.20 | 2.7 | ||||
| 51 | FL | S | −0.28 | 3.7 | ||||
| 52 | FL | S | 0.39 | 2.8 | ||||
| 53 | FL | S | −1.42 | 2.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naeini, E.N.; Atashkadeh, M.; Jacquet, W.; D’Haese, J.; De Bruyn, H. Incidence of Peri-Implantitis, Technical and Biological Complications of Single Implants Placed with Flap or Flapless Surgery—A 10–12-Year Case-Series. J. Clin. Med. 2023, 12, 3668. https://doi.org/10.3390/jcm12113668
Naeini EN, Atashkadeh M, Jacquet W, D’Haese J, De Bruyn H. Incidence of Peri-Implantitis, Technical and Biological Complications of Single Implants Placed with Flap or Flapless Surgery—A 10–12-Year Case-Series. Journal of Clinical Medicine. 2023; 12(11):3668. https://doi.org/10.3390/jcm12113668
Chicago/Turabian StyleNaeini, Emitis Natali, Mandana Atashkadeh, Wolfgang Jacquet, Jan D’Haese, and Hugo De Bruyn. 2023. "Incidence of Peri-Implantitis, Technical and Biological Complications of Single Implants Placed with Flap or Flapless Surgery—A 10–12-Year Case-Series" Journal of Clinical Medicine 12, no. 11: 3668. https://doi.org/10.3390/jcm12113668