
Managing Vulvodynia with Central Sensitization: Challenges and Strategies

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
- a.
- Localized: vestibulodynia (pain in vaginal vestibule), clitoridynia (pain in clitoris); generalized; or mixed (localized and generalized).
- b.
- Provoked: insertional, contact; spontaneous (no contact); or mixed (provoked and spontaneous).
- c.
- Onset: primary (present from the first sexual contact or insertion of a tampon) or secondary (present after a period of asymptomatic sexual contact).
- d.
- Temporal pattern: intermittent, persistent (if symptoms have lasted more than 3 months and persist), constant, immediate (during physical contact), delayed (symptoms appear later).
2.2. Data Assessed
2.3. Exploratory Procedures or Pain-Mapping Method
2.3.1. An S2–S4 Neurological Examination
- Cotton swab testing of the S2–S4 dermatome and vestibule: the absence of signs and symptoms during the physical examination confirms the integrity of the C fibers.
- Clitoris, bulbospongiosus, and perineal reflexes: an evaluation of the motor response of the terminal branches of the pudendal nerve is conducted by gently touching the labium minus lateral to the clitoris, the perineum, and the clitoris with a cotton swab, and the normal motor activity at S2–S4 is indicated by anal sphincter contraction.
- Tinel’s sign in the sciatic spine area: to evaluate the third segment of the pudendal nerve, pain is reproduced with transrectal compression of the third segment of the PN (Tinel sign) in the sciatic spine and Alcock’s canal.
- Tinel’s sign at the clitoris: to evaluate the dorsal nerve of the clitoris, the clitoris is compressed to locate painful spots.
2.3.2. Exploration of the Pelvic Girdle
2.3.3. Exploration of Pelvic Floor Muscles
- Levator ani muscle (LAM): assessment of painful palpation of the pubococcygeus muscle.
- Obturator internus muscle (OIM): contracture of the OIM with flexion and external rotation of the hip in the supine decubitus position and transgluteal examination of OIM segments—pelvic (ischium), medium (midpoint between trochanter and coccyx), and gluteal (hip).
- Piriformis muscle (PM): simultaneous hip external rotation and abdominal flexion is encouraged to reproduce the pain. PM is palpated transgluteally five centimeters above the OIM middle segment.
2.4. Protocols for Vulvodynia Treatment
- Patients with provoked vulvodynia could be prescribed:
- ▪
- Pelvic floor physiotherapy, including 30–40 min of intravaginal and external perineal massage (along the OIM, EAM, and PM), thermotherapy, and biofeedback techniques such as the use of vibrators and vaginal dilators to use during the session and at home. If lack of response or partial response to the described techniques was experienced, transcutaneous electrical nerve stimulation (TENS) was used 2 times a week for 20 min each session, and the electrodes were applied to the labia majora in a V-shape.
- ▪
- Topical lidocaine (5% lidocaine clorhidrate gel, 3–4 applications/24 h).
- ▪
- Vaginal diazepam (5 mg diazepam ovules, 1 ovule/48 h).
- Patients with spontaneous vulvodynia could be prescribed:
- ▪
- Neuromodulators such as tricyclic depressants (amitriptyline, 25 mg/24 h) and serotonin and noradrenaline reuptake inhibitors (duloxetine, 30–60 mg/24 h).
- ▪
- Anticonvulsants (gabapentin, 300 mg/8 h and pregabalin, 75 mg/12 h).
- ▪
- Minimally invasive neuromodulation (MIN) techniques (infiltration of impar ganglion, pudendal nerve, and 100 units of onabotulinum toxin A, pulsed radiofrequency (PRF) of sacral roots and pudendal nerve).
- All types of vulvodynia could be prescribed:
- ▪
- Psychological therapy (normally cognitive behavioral) for treatment of stress and the response to pain when a psychological component to pain was identified.
- ▪
- Hygienic–dietary and behavioral measures, such as vulvar hygiene, lubrication, and use of vaginal dilators.
- Patients with vaginal atrophy could be prescribed:
- ▪
- Topical estradiol creams for menopausal women.
- ▪
- Ospemifene (60 mg/24 h).
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Data Assessed
3.3. Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bornstein, J.; Goldstein, A.T.; Stockdale, C.K.; Bergeron, S.; Pukall, C.; Zolnoun, D.; Coady, D. Consensus vulvar pain terminology committee of the International Society for the Study of Vulvovaginal Disease (ISSVD), the International Society for the Study of Women’s Sexual Health (ISSWSH), and the International Pelvic Pain Society (IPPS) 2015 ISSVD, ISSWSH and IPPS Consensus Terminology and Classification of Persistent Vulvar Pain and Vulvodynia. Obstet. Gynecol. 2016, 127, 745–751. [Google Scholar] [PubMed]
- Brotto, L.A.; Sadownik, L.A.; Thomson, S.; Dayan, M.; Smith, K.B.; Seal, B.N.; Moses, M.; Zhang, A. A Comparison of Demographic and Psychosexual Characteristics of Women with Primary versus Secondary Provoked Vestibulodynia. Clin. J. Pain 2014, 30, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Spadt, S.K.; Kingsberg, S. Vulvar Pain of Unknown Cause (Vulvodynia): Clinical Manifestations and Diagnosis. UpToDate. Available online: https://www.uptodate.com/contents/vulvar-pain-of-unknown-cause-vulvodynia-clinical-manifestations-and-diagnosis (accessed on 27 March 2023).
- Gómez, I.; Coronado, P.J.; Martín, C.M.; Alonso, R.; Guisasola-Campa, F.J. Study on the Prevalence and Factors Associated to Vulvodynia in Spain. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 240, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Wojcik, M.; Plagens-Rotman, K.; Merks, P.; Mizgier, M.; Kedzia, W.; Jarzabek-Bielecka, G. Visceral Therapy in Disorders of the Female Reproductive Organs. Ginekol. Pol. 2022, 93, 511–518. [Google Scholar] [CrossRef]
- Sadownik, L.A. Clinical Profile of Vulvodynia Patients. A prospective study of 300 patients. J. Reprod. Med. 2000, 45, 679–684. [Google Scholar]
- Levesque, A.; Riant, T.; Ploteau, S.; Rigaud, J.; Labat, J.-J. Convergences PP Network Clinical Criteria of Central Sensitization in Chronic Pelvic and Perineal Pain (Convergences PP Criteria): Elaboration of a Clinical Evaluation Tool Based on Formal Expert Consensus. Pain Med. 2018, 19, 2009–2015. [Google Scholar] [CrossRef]
- Woolf, C.J. Evidence for a Central Component of Post-Injury Pain Hypersensitivity. Nature 1983, 306, 686–688. [Google Scholar] [CrossRef]
- Woolf, C.J. Central Sensitization: Uncovering the Relation between Pain and Plasticity. Anesthesiology 2007, 106, 864. [Google Scholar] [CrossRef]
- Ji, R.-R.; Nackley, A.; Huh, Y.; Terrando, N.; Maixner, W. Neuroinflammation and Central Sensitization in Chronic and Widespread Pain. Anesthesiology 2018, 129, 343–366. [Google Scholar] [CrossRef]
- Origoni, M.; Leone Roberti Maggiore, U.; Salvatore, S.; Candiani, M. Neurobiological Mechanisms of Pelvic Pain. Biomed Res. Int. 2014, 2014, 903848. [Google Scholar] [CrossRef]
- Torres-Cueco, R.; Nohales-Alfonso, F. Vulvodynia—It Is Time to Accept a New Understanding from a Neurobiological Perspective. Int. J. Environ. Res. Public Health 2021, 18, 6639. [Google Scholar] [CrossRef] [PubMed]
- Matzumura-Kasano, J.P.; Gutiérrez-Crespo, H.F.; Zamudio-Eslava, L.A. Vulvodinia: Una Puesta Al Día. An. Fac. Med. 2018, 79, 53–59. [Google Scholar] [CrossRef]
- Shah, M.; Hoffstetter, S. Vulvodynia. Obstet. Gynecol. Clin. N. Am. 2014, 41, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Yunus, M.B. Central Sensitivity Syndromes: A New Paradigm and Group Nosology for Fibromyalgia and Overlapping Conditions, and the Related Issue of Disease versus Illness. Semin. Arthritis Rheum. 2008, 37, 339–352. [Google Scholar] [CrossRef]
- Pereira, A.; Fuentes, L.; Almoguera, B.; Chaves, P.; Vaquero, G.; Perez-Medina, T. Understanding the Female Physical Examination in Patients with Chronic Pelvic and Perineal Pain. J. Clin. Med. Res. 2022, 11, 7490. [Google Scholar] [CrossRef]
- Spadt, S.K.; Kingsberg, S. Vulvar Pain of Unknown Cause (Vulvodynia): Treatment. UpToDate. Available online: https://www.uptodate.com/contents/vulvar-pain-of-unknown-cause-vulvodynia-treatment (accessed on 27 March 2023).
- Wójcik, M.; Szczepaniak, R.; Placek, K. Physiotherapy Management in Endometriosis. Int. J. Environ. Res. Public Health 2022, 19, 16148. [Google Scholar] [CrossRef]
- Wojcik, M.; Jarzabek-Bielecka, G.; Merks, P. The role of visceral therapy, Kegel’s muscle, core stability and diet in pelvic support disorders and urinary incontinence—Including sexological aspects and the role of physiotherapy and osteopathy. Ginekol. Pol. 2022, 93, 1018–1027. [Google Scholar] [CrossRef]
- Whitney, M.; Papermaster, A.E.; Baum, A.; Wright, M.L. Vulvodynia Is Not Associated with Concurrent Candidal Vaginitis. Women’s Health Rep. 2022, 3, 144–149. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, L.; Sturdivant, R.X. Applied Logistic Regression, 3rd ed.; John Wiley & Sons: New Jersey, NJ, USA, 2013. [Google Scholar]
- Reed, B.D.; Harlow, S.D.; Sen, A.; Legocki, L.J.; Edwards, R.M.; Arato, N.; Haefner, H.K. Prevalence and Demographic Characteristics of Vulvodynia in a Population-Based Sample. Am. J. Obstet. Gynecol. 2012, 206, 170.e1–170.e9. [Google Scholar] [CrossRef]
- Gumus, I.I.; Sarifakioglu, E.; Uslu, H.; Turhan, N.O. Vulvodynia: Case Report and Review of Literature. Gynecol. Obstet. Investig. 2008, 65, 155–161. [Google Scholar] [CrossRef]
- Pereira, A.; Pérez-Medina, T.; Rodríguez-Tapia, A.; Rutherford, S.; Millan, I.; Iglesias, E.; Ortiz-Quintana, L. Chronic Perineal Pain: Analyses of Prognostic Factors in Pudendal Neuralgia. Clin. J. Pain 2014, 30, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Patla, G.; Mazur-Bialy, A.I.; Humaj-Grysztar, M.; Bonior, J. Chronic Vulvar Pain and Health-Related Quality of Life in Women with Vulvodynia. Life 2023, 13, 328. [Google Scholar] [CrossRef] [PubMed]
- Pereira, G.M.V.; Marcolino, M.S.; Reis, Z.S.N.; Monteiro, M.V.D.C. A systematic review of drug treatment of vulvodynia: Evidence of a strong placebo effect. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 1216–1224. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographics | Overall N = 105 | CS N = 35 | No CS N = 70 | UA p | HR | CI 95% | MA p |
|---|---|---|---|---|---|---|---|
| Age, years, mean (range) | 40.9 (15–74) | 43.5 | 39.6 | 0.195 | - | - | - |
| Duration of pain, years, mean (range) | 3.7 (0.1–30) | 4.9 | 3.1 | 0.088 | 1.011 | 0.946–1.080 | 0.748 |
| PP score | |||||||
| Mean (range) | 4.1 (1–7) | 5.6 | 3.3 | - | - | - | - |
| Pain location, N | |||||||
| Multifocal | 43 (41.0%) | 13 (37.1%) | 30 (42.9%) | 0.132 | - | - | - |
| Vaginal pain | 18 (17.1%) | 6 (17.1%) | 12 (17.1%) | ||||
| Vulvar pain | 16 (15.2%) | 3 (8.6%) | 13 (18.6%) | ||||
| Vestibular pain | 13 (12.4%) | 6 (17.1%) | 7 (10.0%) | ||||
| Clitoral pain | 7 (6.7%) | 1 (2.9%) | 6 (8.6%) | ||||
| Perineal pain | 5 (4.8%) | 4 (11.4%) | 1 (1.4%) | ||||
| Urethral meatus | 2 (1.9%) | 1 (2.9%) | 1 (1.4%) | ||||
| Old obstetric scar | 1 (1.0%) | 1 (2.9%) | 0 (0%) | ||||
| Vulvodynia Type, N | |||||||
| GSV | 48 (45.3%) | 19 (54.3%) | 29 (41.4%) | 0.525 | - | - | - |
| LSV | 17 (16.0%) | 6 (17.1%) | 11 (15.7%) | ||||
| GPV | 18 (17.0%) | 5 (14.3%) | 13 (18.6%) | ||||
| LPV | 22 (20.8%) | 5 (14.3%) | 17 (24.3%) | ||||
| Comorbidities | 25 (23.8%) | 14 (40.0%) | 11 (15.7%) | 0.006 | 0.360 | 0.049–2.634 | 0.193 |
| Dyspareunia | 78 (74.3%) | 32 (91.4%) | 46 (65.7%) | 0.004 | 5.088 | 1.188–21.791 | 0.028 |
| Pain with micturition | 36 (34.3%) | 27 (77.1%) | 9 (12.9%) | <0.001 | 1.840 | 0.813–4.164 | 0.139 |
| Pain with defecation | 19 (18.1%) | 13 (37.1%) | 6 (8.6%) | <0.001 | 3.131 | 1.309–7.490 | 0.010 |
| Pain in pelvic trigger points | 100 (95.2%) | 35 (100%) | 65 (92.6%) | 0.125 | - | - | - |
| Demographics | GSV N = 48 | LSV N = 17 | GPV N = 18 | LPV N = 22 | UA p | HR | CI 95% | MA p |
|---|---|---|---|---|---|---|---|---|
| Age, years, mean | 47.4 | 40.0 | 38.8 | 29.1 | <0.001 | 0.989 | 0.961–1.019 | 0.478 |
| Duration of pain, years, mean | 3.8 | 2.6 | 4 | 4.2 | 0.807 | - | - | - |
| PP score | ||||||||
| Mean (range) | 4.4 | 4.0 | 3.7 | 3.8 | 0.859 | - | - | - |
| Pain location, N | <0.001 | 0.248 | ||||||
| Multifocal | 27 (56.3%) | 0 (0%) | 15 (83.3%) | 0 (0%) | 0.496 | 0.201–1.227 | ||
| Vaginal pain | 8 (16.7%) | 3 (17.6%) | 2 (11.1%) | 6 (27.3%) | 1.431 | 0.339–6.044 | ||
| Vulvar pain | 6 (12.5%) | 5 (29.4%) | 1 (5.6%) | 4 (18.2%) | - | - | ||
| Vestibular pain | 3 (6.3%) | 6 (35.3%) | 0 (0%) | 4 (18.2%) | 0.668 | 0.162–2.743 | ||
| Clitoral pain | 0 (0%) | 1 (5.9%) | 0 (0%) | 6 (27.3%) | 0.517 | 0.077–3.452 | ||
| Perineal pain | 3 (6.3%) | 1 (5.9%) | 0 (0%) | 1 (4.5%) | 1.460 | 0.354–6.028 | ||
| Urethral meatus | 1 (2.1%) | 0 (0%) | 0 (0%) | 1 (4.5%) | 2.886 | 0.499–16.692 | ||
| Old obstetric scar | 0 (0%) | 1 (5.9%) | 0 (0%) | 0 (0%) | - | - | ||
| CS | 19 (39.6%) | 6 (35.3%) | 5 (27.8%) | 5 (22.7%) | 0.525 | - | - | - |
| No CS | 29 (60.4%) | 11 (64.7%) | 13 (72.2%) | 17 (77.3%) | 0.525 | - | - | - |
| Comorbidities | 17 (35.4%) | 3 (17.6%) | 2 (11.1%) | 3 (13.6%) | 0.079 | 1.492 | 0.729–3.005 | 0.274 |
| Dyspareunia | 30 (62.5%) | 13 (76.5%) | 17 (94.4%) | 21 (95.5%) | 0.028 | 0.740 | 0.354–1.547 | 0.423 |
| Pain with micturition | 18 (37.5%) | 6 (35.2%) | 6 (33.3%) | 6 (27.3%) | 0.844 | - | - | - |
| Pain with defecation | 15 (31.3%) | 1 (5.9%) | 2 (11.1%) | 1 (4.5%) | 0.012 | 1.438 | 0.622–3.323 | 0.396 |
| Pain in pelvic trigger points | 47 (97.9%) | 17 (100%) | 15 (83.3%) | 21 (95.5%) | 0.065 | 0.119 | 0.019–0.728 | 0.006 |
| Demographics | Overall N = 105 | CS N = 35 | No CS N = 70 | UA p | HR | CI 95% | MA p |
|---|---|---|---|---|---|---|---|
| Number of previous treatments, mean (range) | 1.2 (0–7) | 1.3 | 1.1 | 0.369 | - | - | - |
| Number of prescribed treatments, mean (range) | 2.8 (0–10) | 3.4 | 2.4 | 0.018 | 0.847 | 0.714–1.004 | 0.056 |
| Prescribed treatment, N | 97 (92.4%) | 35 (100%) | 62 (88.6%) | 0.050 | 3.297 | 0.984–11.046 | 0.053 |
| Hygienic measures | 10 (9.5%) | 3 (8.6%) | 7 (10.0%) | - | - | - | |
| Gabapentin | 3 (2.9%) | 1 (2.9%) | 2 (2.9%) | 1.000 | - | - | - |
| Pregabalin | 11 (10.5%) | 5 (14.3%) | 6 (8.6%) | 1.000 | - | - | - |
| Duloxetine | 11 (10.5%) | 2 (5.7%) | 9 (12.6%) | 0.500 | - | - | - |
| Amitriptyline | 52 (49.5%) | 21 (60.0%) | 31 (44.3%) | 0.329 | - | - | - |
| Intravaginal diazepam | 32 (30.5%) | 12 (34.3%) | 20 (28.6%) | 0.129 | - | - | - |
| Topical lidocaine | 49 (46.7%) | 28 (46.7%) | 21 (60.0%) | 0.549 | - | - | - |
| Minimally invasive neuromodulation | 33 (31.4%) | 17 (48.5%) | 16 (22.9%) | 0.007 | 1.121 | 0.518–2.429 | 0.771 |
| Psychological therapy | 17 (16.2%) | 10 (28.6%) | 7 (10.0%) | 0.015 | 0.863 | 0.308–2.423 | 0.780 |
| Physiotherapy | 75 (71.4%) | 25 (71.4%) | 50 (71.4%) | 1.000 | - | - | - |
| Physiotherapy, number sessions attended | 3.9 (0–24) | 4.3 | 3.8 | 0.657 | - | - | - |
| Diazepam N = 32 | Lidocaine N = 49 | Amitryptiline N = 52 | Anticonvulsant N = 14 | MIN N = 33 | Psych. N = 17 | Physiotherapy N = 75 | |
|---|---|---|---|---|---|---|---|
| Type, p | 0.049 | 0.077 | <0.001 | 0.221 | 0.021 | 0.831 | 0.733 |
| GSV | 20 (62.5%) | 17 (34.7%) | 31 (59.6%) | 8 (57.1%) | 22 (66.7%) | 7 (41.2%) | 33 (44.0%) |
| LSV | 1 (3.1%) | 9 (18.4%) | 13 (25.0%) | 4 (28.6%) | 5 (15.2%) | 4 (23.5%) | 14 (18.7%) |
| GPV | 5 (15.6%) | 8 (16.3%) | 2 (3.8%) | 1 (7.1%) | 3 (9.1%) | 3 (17.6%) | 13 (17.3%) |
| LPV | 6 (18.7%) | 15 (30.6%) | 6 (11.5%) | 1 (7.1%) | 3 (9.1%) | 3 (17.6%) | 15 (20.0%) |
| Pain location, p | 0.237 | 0.005 | 0.093 | 0.917 | 0.417 | 0.080 | 0.502 |
| Multifocal | 16 (50.0%) | 14 (28.6%) | 19 (36.5%) | 6 (42.9%) | 17 (51.5%) | 8 (47.1%) | 30 (40%) |
| Vaginal pain | 7 (21.9%) | 7 (14.3%) | 6 (11.5%) | 1 (7.1%) | 3 (9.1%) | 2 (11.8%) | 12 (16%) |
| Vulvar pain | 3 (9.4%) | 9 (18.4%) | 9 (17.3%) | 3 (17.6%) | 5 (15.2%) | 0 (0%) | 12 (16%) |
| Vestibular pain | 2 (6.3%) | 12 (24.5%) | 9 (17.3%) | 2 (11.8%) | 5 (15.2%) | 2 (11.8%) | 8 (10.7%) |
| Clitoral pain | 1 (3.1%) | 3 (6.1%) | 5 (9.6%) | 1 (7.1%) | 1 (3.0%) | 1 (5.9%) | 5 (6.7%) |
| Perineal pain | 3 (9.4%) | 1 (2.0%) | 1 (1.9%) | 1 (7.1%) | 2 (6.1%) | 2 (11.8%) | 5 (6.7%) |
| Urethral meat. | 0 (0%) | 2 (4.1%) | 2 (3.8%) | 0 (0%) | 0 (0%) | 1 (5.9%) | 2 (2.7%) |
| Old obstet. scar | 0 (0%) | 1 (2.0%) | 1 (3.8%) | 0 (0%) | 0 (0%) | 1 (5.9%) | 1 (1.3%) |
| Comorbidities, p | 0.236 | 0.444 | 0.861 | 0.261 | 0.290 | 0.115 | 0.346 |
| 10 (31.3%) | 10 (20.4%) | 12 (23.1%) | 5 (35.7%) | 10 (30.3%) | 7 (41.2%) | 16 (21.3%) | |
| Dyspareunia, p | 0.912 | 0.245 | 0.012 | 0.511 | 0.466 | 0.764 | 0.104 |
| 24 (75.0%) | 39 (79.6%) | 33 (63.5%) | 12 (85.7%) | 23 (69.7%) | 12 (70.6%) | 59 (78.7%) | |
| Pain with micturition, p | 0.631 | <0.001 | 0.303 | 0.193 | 0.390 | 0.082 | 0.659 |
| 10 (31.3%) | 25 (51.0%) | 21 (40.4%) | 7 (50.0%) | 13 (39.4%) | 9 (52.9%) | 25 (33.3%) | |
| Pain with defecation, p | 0.022 | 0.002 | 0.446 | 0.069 | 0.022 | 0.508 | 0.691 |
| 10 (31.3%) | 3 (6.1%) | 8 (15.4%) | 6 (35.2%) | 10 (30.3%) | 4 (23.5%) | 13 (17.3%) | |
| Pain in pelvic trigger points, p | 0.639 | 0.662 | 1.000 | 1.000 | 0.322 | 1.000 | 0.622 |
| 30 (93.8%) | 46 (93.9%) | 50 (96.2%) | 14 (100%) | 33 (100%) | 16 (94.1%) | 72 (96%) | |
| CS, p | 0.549 | 0.050 | 0.129 | 0.543 | 0.007 | 0.015 | 1.000 |
| 12 (37.5%) | 21 (42.9%) | 21 (40.3%) | 6 (42.9%) | 17 (51.5%) | 10 (58.8%) | 25 (33.3%) |
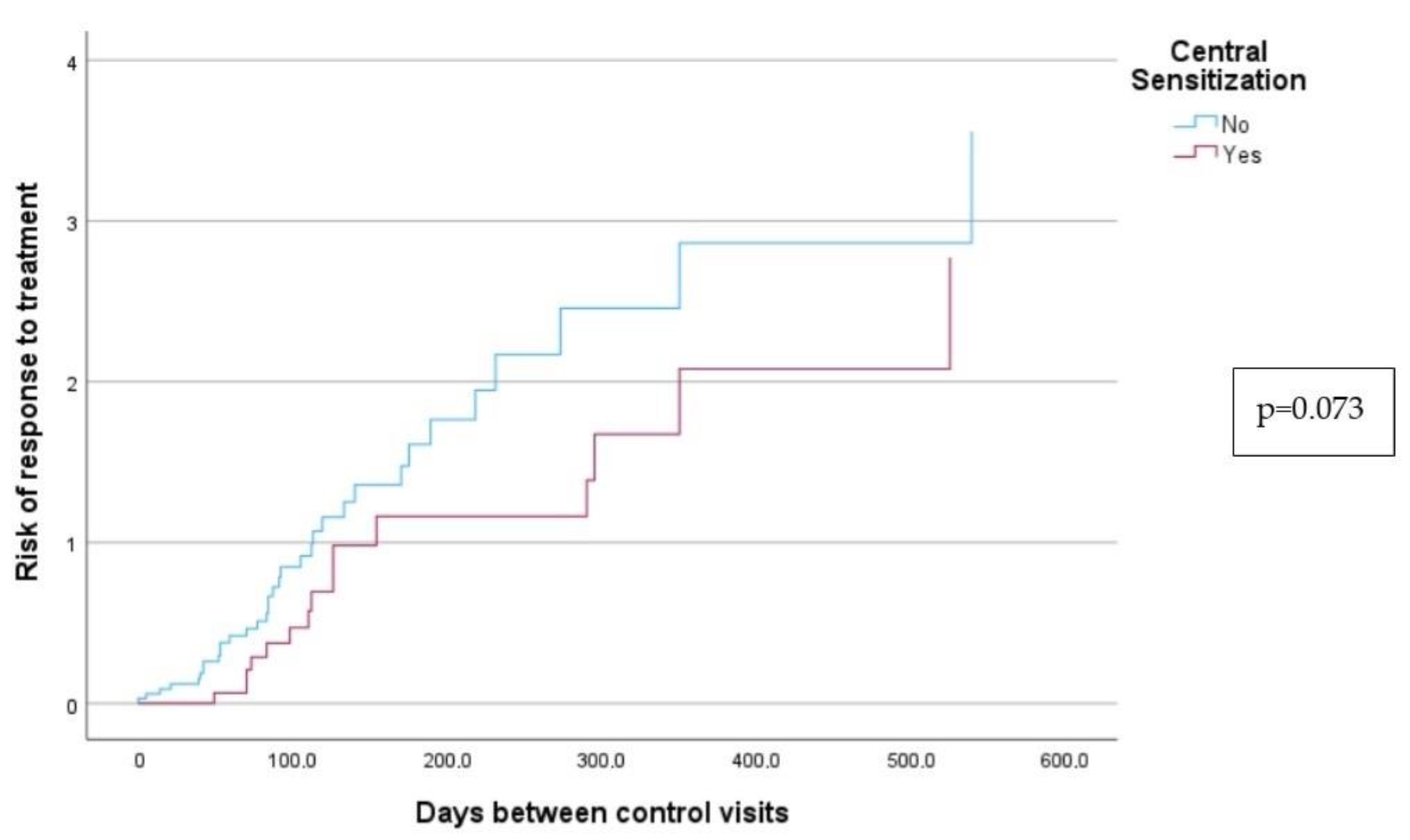
| Response to Treatment (N = 51) | Days until Response | ||||
|---|---|---|---|---|---|
| N (%) | Response (%) | p | Mean (Interval) | p | |
| CS (N = 28) | 16 (57.1%) | 60.9% | 0.073 | 293.4 (146.1–440.6) | 0.073 |
| No CS (N = 52) | 35 (67.3%) | 72.7% | 228.8 (114.8–342.7) | ||
| Pain with micturition (N = 31) | 18 (58%) | 64.4% | 0.273 | 272.6 (127–418.2) | 0.263 |
| No pain with micturition (N = 49) | 33 (67.3%) | 71.5% | 36 (124.3–347.6) | ||
| Pain with defecation (N = 14) | 5 (35.7%) | 59.0% | 0.284 | 180.8 (116.6–245) | 0.447 |
| No pain with defecation (N = 66) | 46 (69.7%) | 70.1% | 244.7 (156.4–333) | ||
| Dyspareunia (N = 59) | 36 (61.0%) | 66.7% | 0.236 | 229.4 (139.9–318.4) | 0.211 |
| No dyspareunia (N = 21) | 15 (71.4%) | 74.7% | 283.4 (88.9–477.8) | ||
| Comorbidities (N = 59) | 35 (59.3%) | 66.4% | 0.213 | 237.1 (143.6–330.6) | 0.113 |
| No comorbidities (N = 21) | 16 (76.1%) | 74.7% | 246.8 (74.3–419.4) | ||
| Vulvodynia Type | 0.394 | 0.941 | |||
| GSV (N = 37) | 26 (70.2%) | 66.5% | 308.8 (205.2–412.4) | ||
| LSV (N = 12) | 7 (58.3%) | 73.6% | 327.7 (171.9–510.8) | ||
| GPV (N = 14) | 8 (57.1%) | 63.1% | 341.4 (163.7–378.3) | ||
| LPV (N = 17) | 9 (52.9%) | 78.9% | 271.0 (239.7–380.0) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rubal, C.; Pereira, A.; Sastre, L.C.; Pérez-Cejuela, B.A.; Gámiz, S.H.; Chaves, P.; Medina, T.P. Managing Vulvodynia with Central Sensitization: Challenges and Strategies. J. Clin. Med. 2023, 12, 3851. https://doi.org/10.3390/jcm12113851
Rubal C, Pereira A, Sastre LC, Pérez-Cejuela BA, Gámiz SH, Chaves P, Medina TP. Managing Vulvodynia with Central Sensitization: Challenges and Strategies. Journal of Clinical Medicine. 2023; 12(11):3851. https://doi.org/10.3390/jcm12113851
Chicago/Turabian StyleRubal, Cristina, Augusto Pereira, Laura Calles Sastre, Belén Almoguera Pérez-Cejuela, Sofía Herrero Gámiz, Pilar Chaves, and Tirso Pérez Medina. 2023. "Managing Vulvodynia with Central Sensitization: Challenges and Strategies" Journal of Clinical Medicine 12, no. 11: 3851. https://doi.org/10.3390/jcm12113851
APA StyleRubal, C., Pereira, A., Sastre, L. C., Pérez-Cejuela, B. A., Gámiz, S. H., Chaves, P., & Medina, T. P. (2023). Managing Vulvodynia with Central Sensitization: Challenges and Strategies. Journal of Clinical Medicine, 12(11), 3851. https://doi.org/10.3390/jcm12113851