

A Novel Irrigation System to Reduce Heat Generation during Guided Implantology: An In Vitro Study
 ,
, 
 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition for 3D Planning
2.2. Study Groups
2.3. Surgical Guide Design and Manufacture
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vermeulen, J. The Accuracy of Implant Placement by Experienced Surgeons: Guided vs Freehand Approach in a Simulated Plastic Model. Int. J. Oral Maxillofac. Implants 2017, 32, 617–624. [Google Scholar] [CrossRef]
- Misir, A.F.; Sumer, M.; Yenisey, M.; Egrioglu, E. Effect of surgical drill guide on heat generated from implant drilling. J. Oral Maxillofac. Surg. 2009, 67, 2663–2668. [Google Scholar] [CrossRef]
- Migliorati, M.; Amorfini, L.; Signori, A.; Barberis, F.; Silvestrini, B.A.; Benedicenti, S. Internal bone temperature change during guided surgery preparations for dental implants: An in vitro study. Int. J. Oral Maxillofac. Implants 2013, 28, 1464–1469. [Google Scholar] [CrossRef] [Green Version]
- dos Santos, P.L.; Pereira Queiroz, T.; Margonar, R.; Gomes de Souza Carvalho, A.C.; Betoni Jr, W.; Rodrigues Rezende, R.R.; dos Santos, P.H.; Garcia, R., Jr. Evaluation of bone heating, drill deformation, and drill doughiness after implant osteotomy: Guided surgery and classic drilling procedure. Int. J. Oral Maxillofac. Implants 2014, 29, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piattelli, A.; Piattelli, M.; Mangano, C.; Scarano, A. A histologic evaluation of eight cases of failed dental implants: Is bone overheating the most probable cause? Biomaterials 1998, 19, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, A.R.; Albrektsson, T.; Albrektsson, B. Heat caused by drilling cortical bone: Temperature measured in vivo in patients and animals. Acta Orthopaedica Scandinavica 1984, 55, 629–631. [Google Scholar] [CrossRef] [PubMed]
- Sener, B.C.; Dergin, G.; Gursoy, B.; Kelesoglu, E.; Slih, I. Effects of irrigation temperature on heat control in vitro at different drilling depths. Clin. Oral Implants Res. 2009, 20, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Strbac, G.D.; Unger, E.; Donner, R.; Bijak, M.; Watzek, G.; Zechner, W. Thermal effects of a combined irrigation method during implant site drilling. A standardized in vitro study using a bovine rib model. Clin. Oral Implants Res. 2012, 25, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Stocchero, M.; Jinno, Y.; Toia, M.; Ahmad, M.; Papia, E.; Yamaguchi, S.; Becktor, J.P. Intraosseous temperature change during installation of dental implants with two different surfaces and different drilling protocols: An in vivo study in sheep. J. Clin. Medicine 2019, 8, 1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Wu, J.; Zhang, J.; Peng, W.; Liao, W. Numerical and Experimental Analyses on the Temperature Distribution in the Dental Implant Preparation Area when Using a Surgical Guide. J. Prosthodont. 2016, 27, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Teich, S.; Bocklet, M.; Evans, Z.; Gutmacher, Z.; Renne, W. 3D printed implant surgical guides with internally routed irrigation for temperature reduction during osteotomy preparation: A pilot study. J. Esthet. Restor. Dent 2022, 34, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Alevizakos, V.; Mitov, G.; Von See, C. Guided implant placement using an internally cooling surgical template: A technical note. J. Oral Implantol. 2020, 46, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Stocchero, M.; Sivolella, S.; Brunello, G.; Zoppello, A.; Cavallin, F.; Biasetto, L. Bone temperature variation using a 3D-Printed surgical guide with internal irrigation. Appl. Sci. 2021, 11, 2588. [Google Scholar] [CrossRef]
- Benington, I.C.; Biagioni, P.A.; Briggs, J.; Sheridan, S.; Lamey, P.J. Thermal changes observed at implant sites during internal and external irrigation. Clin. Oral Implants Res. 2002, 13, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Davidson, S.R.H.; James, D.F. Measurement of thermal conductivity of bovine cortical bone. Medical Engin. Physics 2000, 22, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Barrak, I.; Joób-Fancsaly, Á.; Braunitzer, G.; Varga, E.; Boa, K.; Piffkó, J. Intraosseous heat generation during osteotomy was performed freehand and through a template with an integrated metal guide sleeve. Implant. Dent. 2018, 27, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Frösch, L.; Mukaddam, K.; Filippi, A.; Zitzmann, N.U.; Kühl, S. Comparison of heat generation between guided and conventional implant surgery for single and sequential drilling protocols-an in vitro study. Clin. Oral Implants Res. 2019, 30, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Boa, K.; Barrak, I.; Varga, E.; Joob-Fancsaly, A.; Varga, E.; Piffko, J. Intraosseous generation of heat during guided surgical drilling: An ex vivo study of the effect of the temperature of the irrigating fluid. Br. J. Oral Maxillofac. Surg. 2016, 54, 904–908. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A (Guide with Entry + Exit) | B (Guide with Entry Only) | C (External Handpiece) | D (Control) | ||
|---|---|---|---|---|---|
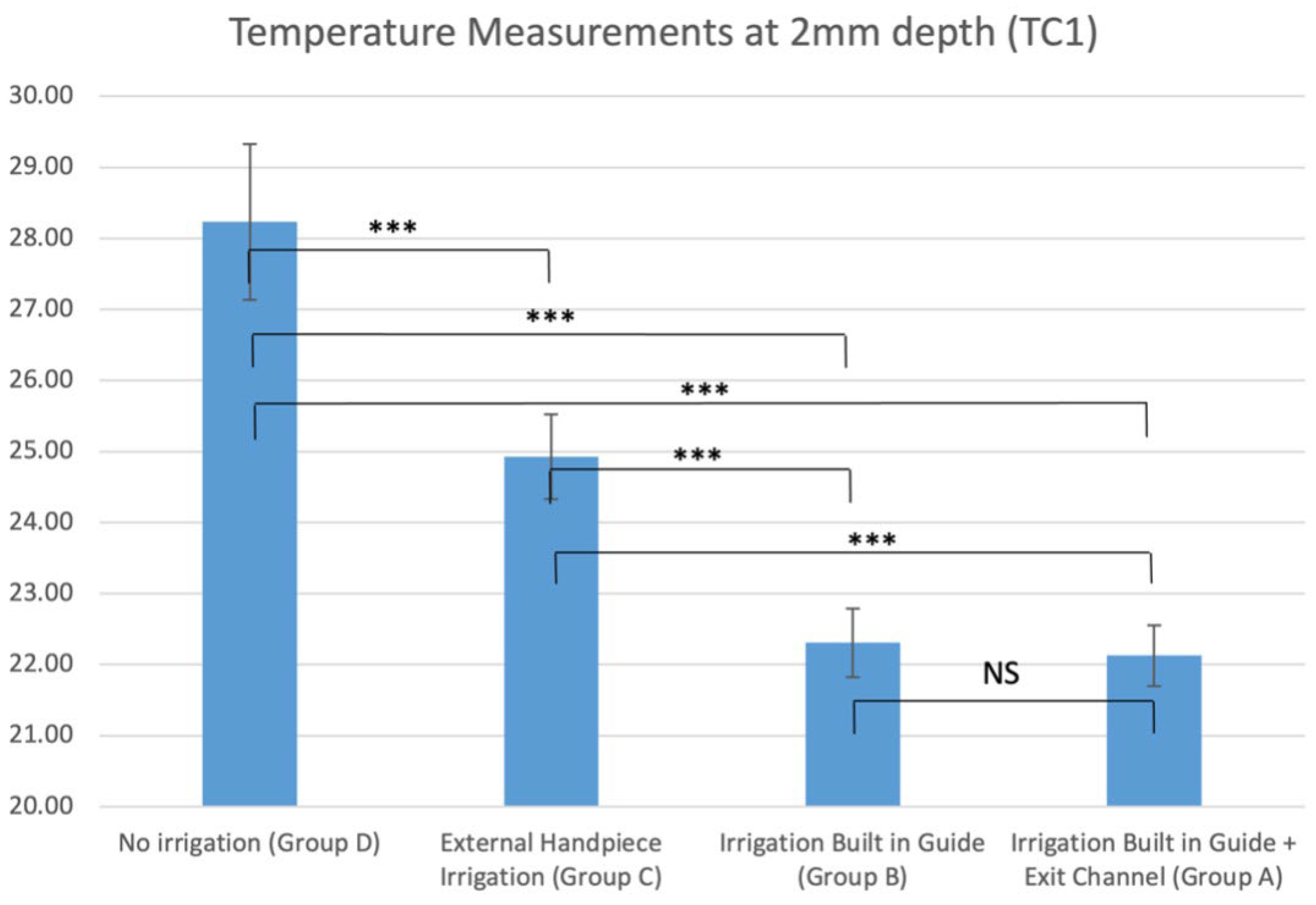
| TC1 | Mean | 22.1 °C | 22.3 °C | 24.9 °C | 28.2 °C |
| (2 mm depth) | StDev | 1.5 °C | 1.7 °C | 2.1 °C | 3.8 °C |
| Maximum | 33.9 °C | 45.9 °C | 47.2 °C | 51.4 °C | |
| TC2 | Mean | 21.4 °C | 22.1 °C | 23.7 °C | 27.2 °C |
| (6 mm depth) | StDev | 0.8 °C | 0.9 °C | 1.3 °C | 2.8 °C |
| Maximum | 28.9 °C | 27.5 °C | 36.9 °C | 52.6 °C |
| Groups in Comparison | TC1 (2 mm Depth) | TC2 (6 mm Depth) |
|---|---|---|
| A-B | 0.3897 | 0.0352 |
| A-C | 0.0005 | 0.0000 |
| A-D | 0.0000 | 0.0000 |
| B-C | 0.0013 | 0.0005 |
| B-D | 0.0000 | 0.0000 |
| C-D | 0.0073 | 0.0004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parvizi, S.; Cameron, A.; Tadakamadla, S.; Figueredo, C.M.S.; Reher, P. A Novel Irrigation System to Reduce Heat Generation during Guided Implantology: An In Vitro Study. J. Clin. Med. 2023, 12, 3944. https://doi.org/10.3390/jcm12123944
Parvizi S, Cameron A, Tadakamadla S, Figueredo CMS, Reher P. A Novel Irrigation System to Reduce Heat Generation during Guided Implantology: An In Vitro Study. Journal of Clinical Medicine. 2023; 12(12):3944. https://doi.org/10.3390/jcm12123944
Chicago/Turabian StyleParvizi, Somayeh, Andrew Cameron, Santosh Tadakamadla, Carlos Marcelo S. Figueredo, and Peter Reher. 2023. "A Novel Irrigation System to Reduce Heat Generation during Guided Implantology: An In Vitro Study" Journal of Clinical Medicine 12, no. 12: 3944. https://doi.org/10.3390/jcm12123944
APA StyleParvizi, S., Cameron, A., Tadakamadla, S., Figueredo, C. M. S., & Reher, P. (2023). A Novel Irrigation System to Reduce Heat Generation during Guided Implantology: An In Vitro Study. Journal of Clinical Medicine, 12(12), 3944. https://doi.org/10.3390/jcm12123944