1. Introduction
Abdominal aortic aneurysm (AAA), which is associated with hospitalization, morbidity, and mortality, is a significant public healthcare burden [
1]. Studies of the epidemiology of AAA in Western countries show that its incidence and mortality rates increased during the 20th century [
2,
3]. Because the repair of screen-detected large AAAs reduces peri-operative mortality rates [
4], several countries, including Sweden, the UK, the US, and Italy, have introduced cost-effective screening programs for AAA in men aged ≥65 years [
5,
6,
7]. Reports from Sweden, the UK, and the US indicate that both the prevalence of AAA and AAA-specific mortality have declined since 2000, indicating the benefits of these screening programs [
8].
To date, few studies have evaluated the incidence of and mortality from AAA in Korea, which currently lacks a screening program. Several studies have reported that the prevalence of AAA is lower in Asian than in Western populations. Large-scale population studies of the incidence of and mortality from AAA are needed, as they can provide insight into the burden of this disease, guide screening and risk prevention priorities and policies, and suggest treatment strategies. The National Health Insurance Service (NHIS) database in South Korea contains complete data on the diagnosis, treatment, and mortality of all residents of the country. Therefore, the aim of this study was to analyze the NHIS data to determine the incidence of AAA and its all-cause mortality from 2009 to 2018.
2. Materials and Methods
In this retrospective cross-sectional study, the NHIS database was searched to identify all Korean patients aged ≥50 years who underwent endovascular or open repair of an AAA between 2008 and 2019. Approval for data collection and publication was granted by the institutional review board (IRB No. 2020-1242) of the Asan Medical Centre, which waived the requirement for written informed consent because of the retrospective nature of this study. All procedures were performed in accordance with relevant guidelines and regulations.
The demographic characteristics of each patient aged ≥50 years with AAA were recorded, as were their International Classification of Disease, Tenth Revision (ICD-10), diagnosis codes, procedure codes, prescriptions, and survival as both inpatients and outpatients.
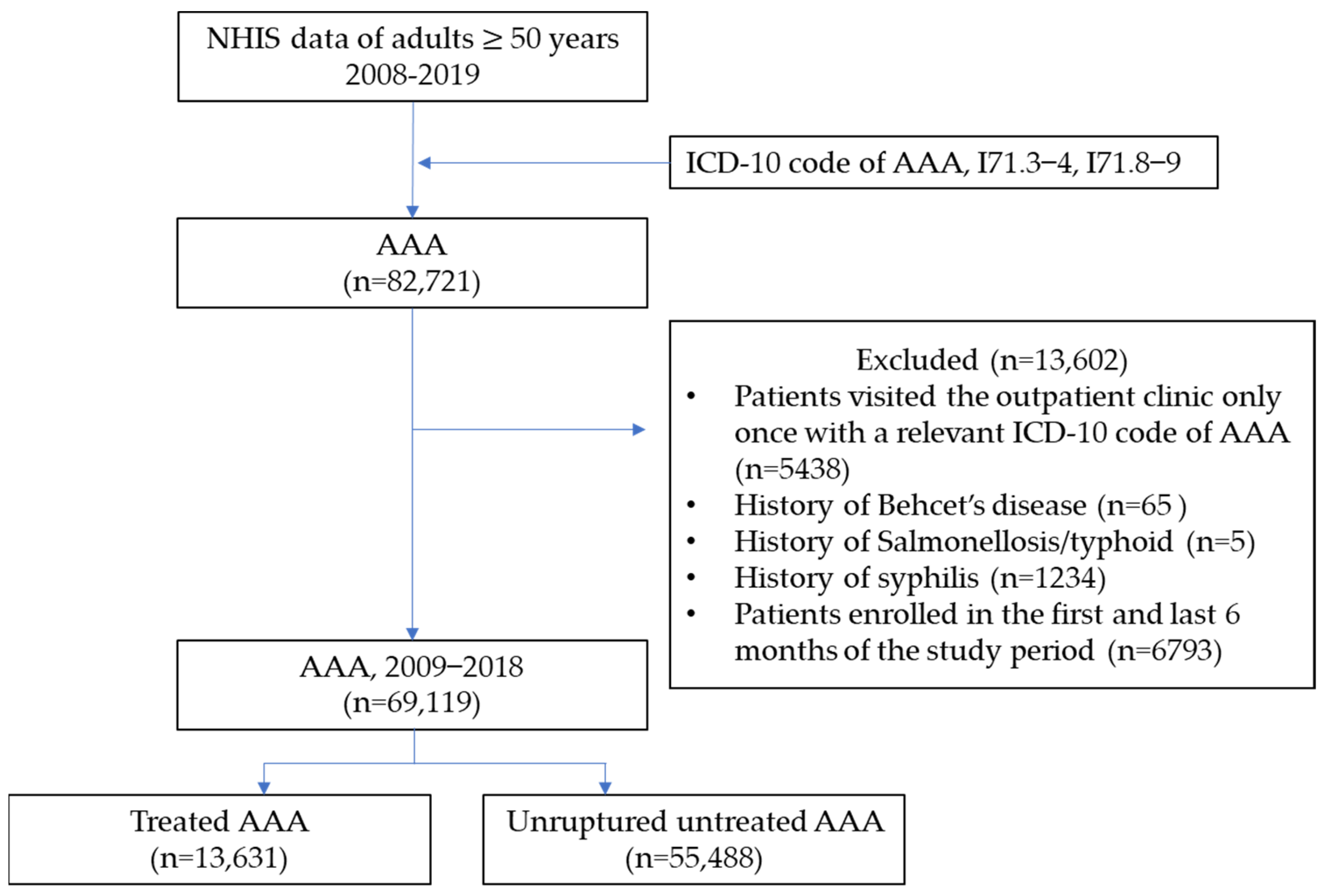
The study flow diagram is depicted in
Figure 1. Patients aged ≥50 years in the NHIS database who had been diagnosed with AAA (ICD-10 codes I71.3-4 and I71.8-71.9) between January 2008 and December 2019 were initially selected. Patients who had visited the outpatient clinic only once with a relevant ICD-10 code for AAA were excluded. Furthermore, to limit the study to patients with the degenerative type of AAA, those with Behcet’s disease (ICD-10 code M35.2) were excluded. The washout period was defined as the first and last years of the study period. The index date was defined as the first date of AAA diagnosis.
The main study outcomes were the incidence and mortality rates of AAA. The yearly incidence rate of AAA was calculated by dividing the number of patients newly diagnosed with AAA during each calendar year by the total number of patients at risk living in Korea during that calendar year. Exact confidence intervals for incidence were calculated using Ulm’s formula [
9]. Both crude and standardized incidence rates were calculated. The standardized incidence rates per 100,000 inhabitants were calculated by applying direct age and sex standardization to the Korean population in 2005 with data obtained from the Korean Statistical Information Service (
http://kosis.kr (accessed on 6 September 2021)). All-cause mortality rates, both crude and standardized, were calculated among patients with unruptured AAA. The rates were analyzed by 5-year age groups and different procedure types, including endovascular aneurysm repair (EVAR) and open surgical repair (OSR). Crude mortality rates were calculated by dividing the overall number of deaths in the at-risk AAA population each year (sum of person-years). Standardized mortality ratios (SMRs) were calculated by an indirect method and by determining the ratio of the number of observed deaths to the number of expected deaths, based on the sex- and age-specific general mortality rates during that calendar year in the total Korean population [
10]. The total numbers of expected deaths were calculated using Equation (1):
All statistical analyses were performed using SAS Enterprise guide version 7.1 software (SAS Institute Inc., Cary, NC, USA).
3. Results
3.1. Incidence
A search of the NHIS database identified 73,933 patients diagnosed with AAA from 2009 to 2018. The gender-specific annual incidences of AAA are shown in
Table 1. The overall incidence of AAA in adults aged ≥50 years during the study period was 37.5 per 100,000 population, 49.7 per 100,000 in men and 26.8 per 100,000 in women. The annual incidence of AAA in Korea increased from 32.33 per 100,000 persons in 2009 to 46.85 per 100,000 populations in 2018. Similarly, the annual incidence of AAA increased both in men and women, from 40.29 per 100,000 in 2008 to 63.40 per 100,000 in 2018 in men and from 25.50 per 100,000 in 2008 to 32.07 per 100,000 in 2018 in women. The incidence increased by approximately 2% to 4% every year from 2008 to 2019.
The standardized incidence of AAA also increased both in men and women, from 45.60 per 100,000 in 2008 to 64.46 per 100,000 in 2018 in men and from 22.70 per 100,000 in 2008 to 24.97 per 100,000 in 2018 in women. When compared with the crude incidence, the standardized incidence was slightly lower from 2012 to 2015 than in 2011 in men and from 2012 to 2017 than in 2011 in women. The increases in 2017 and 2018 were most pronounced both in men and women. The gender-specific annual incidence of AAA tended to increase both in patients aged <65 and ≥65 years (
Figure 2a,b). In 2018, the incidence of AAA in patients aged ≥65 years was 141.5 per 100,000 in men and 63.8 per 100,000 in women. The increased annual incidence of AAA was more apparent in patients aged ≥65 years than in those aged <65 years and in men than in women. The incidence in women aged <65 years was relatively constant, but slightly increased in women aged ≥65 years. In the later years of our study, the incidence peaked at age 80–84 years, but the incidence of AAA among patients aged 80 and above has shown an upward trend over time, resulting in a diverging incidence curve (
Figure 2c). The crude and standardized incidences of untreated AAA were higher than those of treated AAA, with the former showing increasing trends in the three most recent years (
Figure 3). The incidence of EVAR steadily increased during the study period, whereas the incidence of OSR remained constant.
The number of procedures in all age groups increased from 2009 to 2018 (
Figure 4). The increases in EVAR were most apparent among men aged 75–79 years and women aged 80–84 years (
Figure 4a,b), whereas the numbers of OSR procedures increased in men in almost all age groups (
Figure 4c). However, the numbers of OSR procedures in most age groups of women peaked during the middle of the study period and then gradually decreased (
Figure 4d). Relative to men, the AAA procedure-age curve in women was shifted to the right by approximately 5 years.
3.2. Mortality
The crude all-cause mortality rates among patients with unruptured AAA were analyzed separately in treated and untreated patients. The crude all-cause mortality rate of patients with untreated AAA were 21.26/100 person-years in 2009 and 8.87/100 person-years in 2018, with decreasing trends observed both in men and women (
Table 2). The crude mortality rate was higher in men than in women. SMR was 5.91 in 2009 and 2.32 in 2018, and it was higher in men than in women.
The crude all-cause mortality rate in patients who underwent EVAR decreased from 2009 to 2012, remaining constant thereafter (
Figure 5a). The mortality rate for patients who underwent EVAR was higher among women than men during most of the study period (
Figure 5a,b). The crude all-cause mortality rate in patients who underwent OSR was lower in 2018 than in 2009 but varied during the interim (
Figure 5c). The difference in mortality rate between men and women who underwent OSR was smaller at the end of the study period (
Figure 5c,d).
4. Discussion
This nationwide study utilized data from the NHIS to estimate the incidence of AAA and mortality from the disease in Korea from 2009 to 2018. The incidence of AAA in Korea increased during this period for both men and women, with this increasing trend being most apparent in men aged ≥65 years. The incidence of major AAA requiring treatment also increased during the study period. In 2018, the incidence of AAA in subjects aged ≥50 year was 63.40 per 100,000 in men and 32.07 per 100,000 in women, with overall rates of 0.06% and 0.03%, respectively. Higher rates were observed in subjects aged ≥65 years, i.e., 0.14% in men and 0.06% in women. In 2009 and 2010, the incidence of AAA peaked in subjects aged 80–84 ages; in later years, however, the peak incidence was highest in subjects aged ≥85 years, a shift that may be due to the ageing of the Korean population.
Previous studies regarding the epidemiology of AAA in Western countries vary in the definition of AAA and/or the study population. The prevalence of AAA in these studies ranged from 1.3% to 8% [
11,
12,
13,
14,
15,
16], and the annual incidence of newly diagnosed AAA in screened populations ranged from 0.4% to 0.67% [
17,
18]. Although most Asian countries have not yet adopted a screening program for AAA, making it difficult to determine its exact prevalence, the incidence of AAA is generally thought to be lower in Asian than in Western populations [
19]. The incidence of AAA in the present study was much lower than previously reported, a finding likely due to differences in study populations. Because a screening program is not yet available in Korea, the incidence of AAA in the present study was calculated based on diagnosed patients in the NHIS database. The actual incidence of AAA in the general population is likely higher. However, even after accounting for missing patients due to the absence of screening, the incidence of AAA was much lower in the present study than in studies from Western countries, suggesting that this difference may be due, at least in part, to racial/ethnic differences. Accurate determination of the incidence of AAA in the general population, based on a screening program, may be required to evaluate the socioeconomic burden of AAA in Korea. As observed in
Figure 2c, a notable phenomenon emerges: the incidence of AAA among patients aged 80 and above has shown an upward trend over time, contrasting with its lower occurrence in the past. This can be attributed to the significant aging population in Korea, specifically with the increasing life expectancy. Consequently, it can be interpreted that the incidence of AAA is on the rise within the elderly demographic.
Despite the increased incidence, mortality rates decreased over time in both treated and untreated AAA patients in this study. Mortality from AAA in developed countries has decreased since the late 1990s [
20,
21]. AAA is associated with multiple risk factors, with tobacco smoking being the main modifiable risk factor for its development and rupture [
22]. The decrease in AAA correlated with reductions in cardiovascular risk factors, due in part to smoking cessation and treatment with cardiovascular drugs [
21,
23]. The mortality rate associated with the elective treatment of non-ruptured AAA has decreased in recent years [
24], due in part to improvements in the treatment or adoption of endovascular techniques [
25]. Similarly, the present study found that outcomes improved with the treatment of non-ruptured AAA. Moreover, the study found that reductions in mortality rates were greater in untreated AAA patients than in treated ones. This suggests that managing related diseases or risk factors for AAA may have a greater impact on mortality improvement than treating the AAA itself. As stated in the guidelines, identification of these factors will play a major role in improving the prognosis of patients with AAA [
26].
The major strength of this study was its complete coverage of the Korean population since incidence and mortality trends in patients with unruptured AAA were based on data from a compulsory national insurance system. Nevertheless, this study had several important limitations. Patients with ruptured AAA were not included because accurate statistics could not be obtained on out-of-hospital deaths or pre-hospital deaths with obscure diagnoses. The incidence of AAA in the general population could not be determined because of the absence of a screening program. Nevertheless, this study provided robust evidence of the incidence of and mortality from AAA in a large Asian population. Knowledge of these trends may help guide public health policies and implementation, including the introduction of AAA screening programs and increased focus on risk factor management and early intervention strategies.
5. Conclusions
In 2018, the incidence of AAA in Koreans aged ≥50 years was 0.06% in men and 0.03% in women, with increasing trends. Mortality rates have decreased over time both in treated and untreated AAA. The observed increase in incidence suggests a rising burden of AAA in the Korean population, particularly among men. The decreasing mortality rates may indicate improvements in the management and treatment of AAA over the study period. Further research and healthcare initiatives are warranted to address this public health concern and formulate appropriate strategies for the prevention, diagnosis, and treatment of AAA in Korea.
Author Contributions
Conceptualization: H.K. Data curation: H.K., T.-W.K., Y.-J.K. and S.K. Formal analysis: Y.-J.K. and S.K. Funding acquisition: T.-W.K. Investigation: H.K., J.G.G. and Y.H. Methodology: H.K. and Y.-J.K. Software: Y.-J.K. and S.K. Validation: Y.-P.C., J.G.G., Y.H. and S.A.L. Visualization: H.K. and Y.-J.K. Writing—original draft: H.K. Writing—review & editing: T.-W.K., Y.-P.C., J.G.G., Y.H. and S.A.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Asan Institute for Life Sciences and Corporate Relations of Asan Medical Center, Seoul, Korea.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Asan medical center (2020-1242).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of this study.
Data Availability Statement
The data that support the findings of this study are available from National Health Insurance Service of Korea, but restrictions apply to the availability of these data, which were used under license for the current study and so are not publicly available.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Sidloff, D.; Stather, P.; Dattani, N.; Bown, M.; Thompson, J.; Sayers, R.; Choke, E. Aneurysm global epidemiology study: Public health measures can further reduce abdominal aortic aneurysm mortality. Circulation 2014, 129, 747–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filipovic, M.; Goldacre, M.J.; Roberts, S.E.; Yeates, D.; Duncan, M.E.; Cook-Mozaffari, P. Trends in mortality and hospital admission rates for abdominal aortic aneurysm in England and Wales, 1979–1999. Br. J. Surg. 2005, 92, 968–975. [Google Scholar] [CrossRef] [PubMed]
- Lilienfeld, D.E.; Gunderson, P.D.; Sprafka, J.M.; Vargas, C. Epidemiology of aortic aneurysms: I. Mortality trends in the United States, 1951 to 1981. Arteriosclerosis 1987, 7, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Lindholt, J.S.; Norman, P.E. Meta-analysis of postoperative mortality after elective repair of abdominal aortic aneurysms detected by screening. Br. J. Surg. 2011, 98, 619–622. [Google Scholar] [CrossRef] [PubMed]
- Jacomelli, J.; Summers, L.; Stevenson, A.; Lees, T.; Earnshaw, J.J. Impact of the first 5 years of a national abdominal aortic aneurysm screening programme. Br. J. Surg. 2016, 103, 1125–1131. [Google Scholar] [CrossRef] [PubMed]
- Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Doubeni, C.A.; Epling, J.W., Jr.; Kubik, M.; Landefeld, C.S.; et al. Screening for Abdominal Aortic Aneurysm: US Preventive Services Task Force Recommendation Statement. JAMA 2019, 322, 2211–2218. [Google Scholar] [CrossRef] [Green Version]
- Wanhainen, A.; Hultgren, R.; Linné, A.; Holst, J.; Gottsäter, A.; Langenskiöld, M.; Smidfelt, K.; Björck, M.; Svensjö, S. Outcome of the Swedish Nationwide Abdominal Aortic Aneurysm Screening Program. Circulation 2016, 134, 1141–1148. [Google Scholar] [CrossRef]
- Choke, E.; Vijaynagar, B.; Thompson, J.; Nasim, A.; Bown, M.J.; Sayers, R.D. Changing Epidemiology of Abdominal Aortic Aneurysms in England and Wales. Circulation 2012, 125, 1617–1625. [Google Scholar] [CrossRef] [Green Version]
- Ulm, K. A simple method to calculate the confidence interval of a standardized mortality ratio (SMR). Am. J. Epidemiol. 1990, 131, 373–375. [Google Scholar] [CrossRef]
- Statistics Korea. Korean Standard Classification of Diseases and Causes of Death (KCD-6). Available online: https://kssc.kostat.go.kr:8443/ksscNew_web/ekssc/main/main.do (accessed on 6 September 2021).
- Gianfagna, F.; Veronesi, G.; Tozzi, M.; Tarallo, A.; Borchini, R.; Ferrario, M.M.; Bertù, L.; Montonati, A.; Castelli, P.; Castelli, P.; et al. Prevalence of Abdominal Aortic Aneurysms in the General Population and in Subgroups at High Cardiovascular Risk in Italy. Results of the RoCAV Population Based Study. Eur. J. Vasc. Endovasc. Surg. 2018, 55, 633–639. [Google Scholar] [CrossRef] [Green Version]
- Lindholt, J.S.; Diederichsen, A.C.; Rasmussen, L.M.; Frost, L.; Steffensen, F.H.; Lambrechtsen, J.; Urbonaviciene, G.; Busk, M.; Egstrup, K.; Kristensen, K.L.; et al. Survival, Prevalence, Progression and Repair of Abdominal Aortic Aneurysms: Results from Three Randomised Controlled Screening Trials Over Three Decades. Clin. Epidemiol. 2020, 12, 95–103. [Google Scholar] [CrossRef] [Green Version]
- Norman, P.E.; Jamrozik, K.; Lawrence-Brown, M.M.; Le, M.T.; Spencer, C.A.; Tuohy, R.J.; Parsons, R.W.; Dickinson, J.A. Population based randomised controlled trial on impact of screening on mortality from abdominal aortic aneurysm. BMJ 2004, 329, 1259. [Google Scholar] [CrossRef] [Green Version]
- Scott, R.A.; Wilson, N.M.; Ashton, H.A.; Kay, D.N. Influence of screening on the incidence of ruptured abdominal aortic aneurysm: 5-year results of a randomized controlled study. Br. J. Surg. 1995, 82, 1066–1070. [Google Scholar] [CrossRef]
- Scott, R.A.P.; Bridgewater, S.G.; Ashton, H.A. Randomized clinical trial of screening for abdominal aortic aneurysm in women. Br. J. Surg. 2002, 89, 283–285. [Google Scholar] [CrossRef]
- Summers, K.L.; Kerut, E.K.; Sheahan, C.; Unruh, M.; Chawla, A.; Brooke, E.A.; Sheahan, M., III. Prevalence of Abdominal Aortic Aneurysms in the United States: Re-evaluating the Screening Guidelines. J. Vasc. Surg. 2019, 70, e89–e90. [Google Scholar] [CrossRef] [Green Version]
- Forsdahl, S.H.; Singh, K.; Solberg, S.; Jacobsen, B.K. Risk factors for abdominal aortic aneurysms: A 7-year prospective study: The Tromsø Study, 1994–2001. Circulation 2009, 119, 2202–2208. [Google Scholar] [CrossRef] [Green Version]
- Vardulaki, K.A.; Prevost, T.C.; Walker, N.M.; Day, N.E.; Wilmink, A.B.; Quick, C.R.; Ashton, H.A.; Scott, R.A. Incidence among men of asymptomatic abdominal aortic aneurysms: Estimates from 500 screen detected cases. J. Med. Screen. 1999, 6, 50–54. [Google Scholar] [CrossRef]
- Li, X.; Zhao, G.; Zhang, J.; Duan, Z.; Xin, S. Prevalence and trends of the abdominal aortic aneurysms epidemic in general population—A meta-analysis. PLoS ONE 2013, 8, e81260. [Google Scholar] [CrossRef]
- Buck, D.B.; Van Herwaarden, J.A.; Schermerhorn, M.L.; Moll, F.L. Endovascular treatment of abdominal aortic aneurysms. Nat. Rev. Cardiol. 2014, 11, 112–123. [Google Scholar] [CrossRef] [Green Version]
- Png, C.Y.M.; Wu, J.; Tang, T.Y.; Png, I.P.L.; Sheng, T.J.; Choke, E. Editor’s Choice—Decrease in Mortality from Abdominal Aortic Aneurysms (2001 to 2015): Is it Decreasing Even Faster? Eur. J. Vasc. Endovasc. Surg. 2021, 61, 900–907. [Google Scholar] [CrossRef]
- Ullery, B.W.; Hallett, R.L.; Fleischmann, D. Epidemiology and contemporary management of abdominal aortic aneurysms. Abdom. Radiol. 2018, 43, 1032–1043. [Google Scholar] [CrossRef] [PubMed]
- Nelissen, B.G.L.; Herwaarden, J.A.; Pasterkamp, G.; Moll, F.L.; Vaartjes, I. Shifting abdominal aortic aneurysm mortality trends in The Netherlands. J. Vasc. Surg. 2015, 61, 642–647.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberga, A.J.; Karthaus, E.G.; Wilschut, J.A.; de Bruin, J.L.; Akkersdijk, G.P.; Geelkerken, R.H.; Hamming, J.F.; Wever, J.J.; Verhagen, H.J.M.; van den Akker, P.J.; et al. Treatment Outcome Trends for Non-Ruptured Abdominal Aortic Aneurysms: A Nationwide Prospective Cohort Study. Eur. J. Vasc. Endovasc. Surg. 2022, 63, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Deery, S.E.; O’Donnell, T.F.X.; Pothof, A.B.; Bodewes, T.C.F.; Darling, J.D.; Shean, K.E.; Schermerhorn, M.L. Declining Mortality Rates From Abdominal Aortic Aneurysms Across All Age, Sex, and Racial Groups. J. Vasc. Surg. 2017, 66, e7. [Google Scholar] [CrossRef]
- Chaikof, E.L.; Dalman, R.L.; Eskandari, M.K.; Jackson, B.M.; Lee, W.A.; Mansour, M.A.; Mastracci, T.M.; Mell, M.; Murad, M.H.; Nguyen, L.L.; et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J. Vasc. Surg. 2018, 67, 2–77.e2. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Flow diagram. NHIS, National Health Insurance Service; AAA, abdominal aortic aneurysm; ICD, International Classification of Disease.
Figure 1.
Flow diagram. NHIS, National Health Insurance Service; AAA, abdominal aortic aneurysm; ICD, International Classification of Disease.
Figure 2.
Annual trend of incidence of abdominal aortic aneurysm (AAA) (per 100,000 persons) from 2009 to 2018 in patients aged (a) <65 years, and (b) ≥65 years. (c) Annual age-specific incidence of AAA. The gender-specific annual incidence of AAA tended to increase both in patients aged <65 and ≥65 years, and the age-specific incidence of AAA among patients aged 80 and above has shown an upward trend over time, resulting in a diverging incidence curve. ‘Total’ in panel (a,b) represents the combined data both for men and women.
Figure 2.
Annual trend of incidence of abdominal aortic aneurysm (AAA) (per 100,000 persons) from 2009 to 2018 in patients aged (a) <65 years, and (b) ≥65 years. (c) Annual age-specific incidence of AAA. The gender-specific annual incidence of AAA tended to increase both in patients aged <65 and ≥65 years, and the age-specific incidence of AAA among patients aged 80 and above has shown an upward trend over time, resulting in a diverging incidence curve. ‘Total’ in panel (a,b) represents the combined data both for men and women.
Figure 3.
Annual crude (a) and standardized (b) incidences (per 100,000 persons) from 2009 to 2018 of patients with abdominal aortic aneurysm who underwent endovascular aneurysm repair (EVAR), underwent open surgical repair (OSR), or were untreated. The incidence of EVAR steadily increased during the study period, whereas the incidence of OSR remained constant.
Figure 3.
Annual crude (a) and standardized (b) incidences (per 100,000 persons) from 2009 to 2018 of patients with abdominal aortic aneurysm who underwent endovascular aneurysm repair (EVAR), underwent open surgical repair (OSR), or were untreated. The incidence of EVAR steadily increased during the study period, whereas the incidence of OSR remained constant.
Figure 4.
Numbers of (a,c) men and (b,d) women who underwent (a,b) endovascular aneurysm repair (EVAR) and (c,d) open surgical repair (OSR) of abdominal aortic aneurysm by age group. The increases in EVAR were most apparent among men aged 75–79 years and women aged 80–84 years, whereas the numbers of OSR procedures increased in men in almost all age groups.
Figure 4.
Numbers of (a,c) men and (b,d) women who underwent (a,b) endovascular aneurysm repair (EVAR) and (c,d) open surgical repair (OSR) of abdominal aortic aneurysm by age group. The increases in EVAR were most apparent among men aged 75–79 years and women aged 80–84 years, whereas the numbers of OSR procedures increased in men in almost all age groups.
Figure 5.
Annual (a,c) crude and (b,d) standardized mortality rates (per 100,000 persons) from 2009 to 2018 of patients with abdominal aortic aneurysm who underwent endovascular aneurysm repair (EVAR) (a,b) and open surgical repair (OSR) (c,d). The all-cause mortality rate in patients who underwent EVAR decreased from 2009 to 2012, remaining constant thereafter, and the all-cause mortality rate in patients who underwent OSR was lower in 2018 than in 2009.
Figure 5.
Annual (a,c) crude and (b,d) standardized mortality rates (per 100,000 persons) from 2009 to 2018 of patients with abdominal aortic aneurysm who underwent endovascular aneurysm repair (EVAR) (a,b) and open surgical repair (OSR) (c,d). The all-cause mortality rate in patients who underwent EVAR decreased from 2009 to 2012, remaining constant thereafter, and the all-cause mortality rate in patients who underwent OSR was lower in 2018 than in 2009.
Table 1.
Annual and standardized incidence rates (per 100,000 persons) of abdominal aortic aneurysm from 2009 to 2018.
Table 1.
Annual and standardized incidence rates (per 100,000 persons) of abdominal aortic aneurysm from 2009 to 2018.
| | No. of Patients | Population | Incidence (95% CI) | Standardised Incidence (95% CI) |
|---|
| Total | | | | |
| 2009 | 4390 | 13,580,019 | 32.33 (31.38, 33.30) | 68.30 (66.78, 69.83) |
| 2010 | 4748 | 14,263,364 | 33.29 (32.25, 34.25) | 70.59 (69.05, 72.16) |
| 2011 | 5387 | 14,966,440 | 35.99 (35.04, 36.97) | 76.07 (74.47, 77.69) |
| 2012 | 5655 | 15,637,721 | 36.16 (35.23, 37.12) | 75.72 (74.12, 77.34) |
| 2013 | 5658 | 16,240,030 | 34.84 (33.94, 35.76) | 72.20 (70.64, 73.78) |
| 2014 | 5786 | 16,818,677 | 34.40 (33.52, 35.3) | 69.98 (68.44, 71.53) |
| 2015 | 6185 | 17,416,450 | 35.51 (34.63, 36.41) | 71.18 (69.63, 72.75) |
| 2016 | 7257 | 17,994,515 | 40.33 (39.41, 41.27) | 79.94 (78.29, 81.60) |
| 2017 | 7725 | 18,572,007 | 41.59 (40.67, 42.53) | 81.74 (80.08, 83.42) |
| 2018 | 8993 | 19,193,790 | 46.85 (45.89, 47.83) | 89.43 (87.69, 91.19) |
| Men | | | | |
| 2009 | 2526 | 6,269,886 | 40.29 (38.73, 41.89) | 45.60 (44.36, 46.86) |
| 2010 | 2808 | 6,605,542 | 42.51 (40.95, 44.11) | 48.01 (46.74, 49.31) |
| 2011 | 3228 | 6,951,176 | 46.44 (44.85, 48.07) | 52.40 (51.07, 53.75) |
| 2012 | 3381 | 7,285,950 | 46.40 (44.85, 48.00) | 52.06 (50.73, 53.40) |
| 2013 | 3482 | 7,590,057 | 45.88 (44.36, 47.43) | 51.04 (49.73, 52.38) |
| 2014 | 3548 | 7,880,430 | 45.02 (43.55, 46.53) | 49.47 (48.18, 50.78) |
| 2015 | 3865 | 8,176,100 | 47.27 (45.79, 48.79) | 50.77 (49.46, 52.10) |
| 2016 | 4583 | 8,467,751 | 54.12 (52.57, 55.71) | 57.29 (55.90, 58.70) |
| 2017 | 5130 | 8,756,242 | 58.59 (56.99, 60.21) | 60.73 (59.30, 62.18) |
| 2018 | 5743 | 9,059,019 | 63.40 (61.77, 65.06) | 64.46 (62.98, 65.95) |
| Women | | | | |
| 2009 | 1864 | 7,310,133 | 25.50 (24.35, 26.68) | 22.70 (21.83, 23.59) |
| 2010 | 1940 | 7,657,823 | 25.33 (24.22, 26.49) | 22.58 (21.71, 23.47) |
| 2011 | 2159 | 8,015,264 | 26.94 (25.81, 28.10) | 23.67 (22.78, 24.58) |
| 2012 | 2274 | 8,351,771 | 27.23 (26.12, 28.37) | 23.66 (22.77, 24.57) |
| 2013 | 2176 | 8,649,974 | 25.16 (24.11, 26.24) | 21.16 (20.32, 22.02) |
| 2014 | 2238 | 8,938,248 | 25.04 (24.01, 26.10) | 20.51 (19.68, 21.36) |
| 2015 | 2320 | 9,240,351 | 25.11 (24.10, 26.15) | 20.42 (19.59, 21.26) |
| 2016 | 2674 | 9,526,765 | 28.07 (27.01, 29.15) | 22.64 (21.77, 23.54) |
| 2017 | 2595 | 9,815,766 | 26.44 (25.43, 27.47) | 21.01 (20.17, 21.87) |
| 2018 | 3250 | 10,134,772 | 32.07 (30.97, 33.19) | 24.97 (24.06, 25.91) |
Table 2.
Annual crude and standardized mortality rates of patients with untreated unruptured abdominal aortic aneurysm from 2009 to 2018.
Table 2.
Annual crude and standardized mortality rates of patients with untreated unruptured abdominal aortic aneurysm from 2009 to 2018.
| | Observed Deaths | Person-Year | Crude Mortality per 100 Person-Years | Standardised Mortality Ratio (95% CI) |
|---|
| Total | | | | |
| 2009 | 611 | 2874.4 | 21.26 | 5.91 (5.45–6.40) |
| 2010 | 906 | 5946.9 | 15.23 | 4.28 (4.01–4.57) |
| 2011 | 1189 | 8968.3 | 13.26 | 3.77 (3.56–3.99) |
| 2012 | 1391 | 12,280.2 | 11.33 | 3.13 (2.97–3.30) |
| 2013 | 1562 | 15,079.2 | 10.36 | 2.92 (2.77–3.07) |
| 2014 | 1722 | 17,786.8 | 9.68 | 2.73 (2.60–2.86) |
| 2015 | 2007 | 20,450.1 | 9.81 | 2.68 (2.57–2.80) |
| 2016 | 2237 | 23,554.7 | 9.50 | 2.58 (2.47–2.69) |
| 2017 | 2367 | 26,903.5 | 8.80 | 2.36 (2.26–2.45) |
| 2018 | 2729 | 30,779.1 | 8.87 | 2.32 (2.23–2.40) |
| Men | | | | |
| 2009 | 332 | 1529.6 | 21.71 | 5.34 (4.78–5.94) |
| 2010 | 538 | 3150.7 | 17.08 | 4.24 (3.89–4.61) |
| 2011 | 725 | 4758.3 | 15.24 | 3.84 (3.57–4.13) |
| 2012 | 821 | 6469.1 | 12.69 | 3.14 (2.93–3.37) |
| 2013 | 902 | 7983.7 | 11.30 | 2.86 (2.68–3.06) |
| 2014 | 982 | 9462.5 | 10.38 | 2.66 (2.50–2.83) |
| 2015 | 1110 | 10,977.3 | 10.11 | 2.56 (2.41–2.72) |
| 2016 | 1297 | 12,813.0 | 10.12 | 2.57 (2.43–2.72) |
| 2017 | 1378 | 14,802.6 | 9.31 | 2.38 (2.26–2.51) |
| 2018 | 1610 | 17,220.4 | 9.35 | 2.35 (2.23–2.46) |
| Women | | | | |
| 2009 | 279 | 1344.8 | 20.75 | 6.79 (6.02–7.63) |
| 2010 | 368 | 2796.2 | 13.16 | 4.34 (3.91–4.81) |
| 2011 | 464 | 4210.0 | 11.02 | 3.65 (3.33–4.00) |
| 2012 | 570 | 5811.1 | 9.81 | 3.11 (2.86–3.38) |
| 2013 | 660 | 7095.6 | 9.30 | 2.99 (2.77–3.23) |
| 2014 | 740 | 8324.4 | 8.89 | 2.83 (2.63–3.04) |
| 2015 | 897 | 9472.8 | 9.47 | 2.85 (2.67–3.05) |
| 2016 | 940 | 10,741.7 | 8.75 | 2.59 (2.43–2.76) |
| 2017 | 989 | 12,100.9 | 8.17 | 2.32 (2.18–2.47) |
| 2018 | 1119 | 13,558.7 | 8.25 | 2.27 (2.14–2.41) |
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}