
Effects of Remimazolam Anesthesia with Two Induction Doses on Hemodynamics and Recovery Profile in Older Patients: Comparison with Propofol Anesthesia
 , ,
, ,
Abstract
:1. Introduction
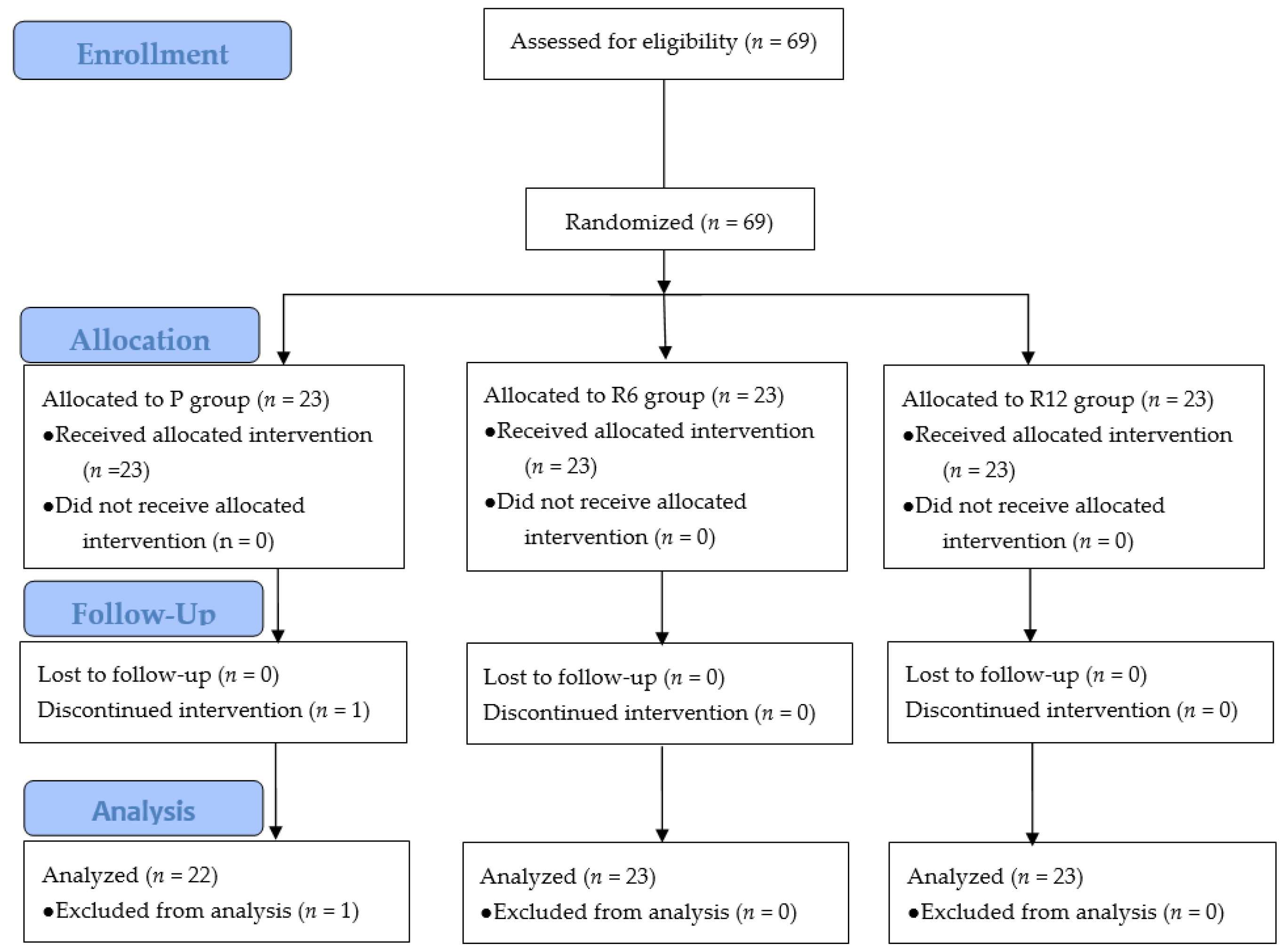
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salmasi, V.; Maheshwari, K.; Yang, D.; Mascha, E.J.; Singh, A.; Sessler, D.I.; Kurz, A. Relationship between Intraoperative Hypotension, Defined by Either Reduction from Baseline or Absolute Thresholds, and Acute Kidney and Myocardial Injury after Noncardiac Surgery: A Retrospective Cohort Analysis. Anesthesiology 2017, 126, 47–65. [Google Scholar] [CrossRef]
- Wesselink, E.M.; Kappen, T.H.; Torn, H.M.; Slooter, A.J.C.; van Klei, W.A. Intraoperative hypotension and the risk of postoperative adverse outcomes: A systematic review. Br. J. Anaesth. 2018, 121, 706–721. [Google Scholar] [CrossRef] [Green Version]
- Murabito, P.; Astuto, M.; Sanfilippo, F.; La Via, L.; Vasile, F.; Basile, F.; Cappellani, A.; Longhitano, L.; Distefano, A.; Li Volti, G. Proactive Management of Intraoperative Hypotension Reduces Biomarkers of Organ Injury and Oxidative Stress during Elective Non-Cardiac Surgery: A Pilot Randomized Controlled Trial. J. Clin. Med. 2022, 11, 392. [Google Scholar] [CrossRef]
- Sneyd, J.R.; Rigby-Jones, A.E. New drugs and technologies, intravenous anaesthesia is on the move (again). Br. J. Anaesth. 2010, 105, 246–254. [Google Scholar] [CrossRef] [Green Version]
- Sun, X.; Zhang, X.; Bo, Q.; Meng, T.; Lei, Z.; Li, J.; Hou, Y.; Yu, X.; Yu, J. Propofol reduced myocardial contraction of vertebrates partly by mediating the cyclic AMP-dependent protein kinase phosphorylation pathway. Toxicology 2016, 365, 59–66. [Google Scholar] [CrossRef]
- Phillips, A.T.; Deiner, S.; Mo Lin, H.; Andreopoulos, E.; Silverstein, J.; Levin, M.A. Propofol Use in the Elderly Population: Prevalence of Overdose and Association With 30-Day Mortality. Clin. Ther. 2015, 37, 2676–2685. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-H.; Fechner, J. Remimazolam—Current knowledge on a new intravenous benzodiazepine anesthetic agent. Korean J. Anesthesiol. 2022, 75, 307–315. [Google Scholar] [CrossRef]
- Sneyd, J.R.; Rigby-Jones, A.E. Remimazolam for anaesthesia or sedation. Curr. Opin. Anaesthesiol. 2020, 33, 506–511. [Google Scholar] [CrossRef]
- Doi, M.; Morita, K.; Takeda, J.; Sakamoto, A.; Yamakage, M.; Suzuki, T. Efficacy and safety of remimazolam versus propofol for general anesthesia: A multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J. Anesth. 2020, 34, 543–553. [Google Scholar] [CrossRef]
- Zhang, X.; Li, S.; Liu, J. Efficacy and safety of remimazolam besylate versus propofol during hysteroscopy: Single-centre randomized controlled trial. BMC Anesthesiol. 2021, 21, 156. [Google Scholar] [CrossRef]
- Liu, X.; Ding, B.; Shi, F.; Zhang, Y.; Liu, L.; Sha, Y.; Zhao, T. The Efficacy and Safety of Remimazolam Tosilate versus Etomidate-Propofol in Elderly Outpatients Undergoing Colonoscopy: A Prospective, Randomized, Single-Blind, Non-Inferiority Trial. Drug Des. Devel. Ther. 2021, 15, 4675–4685. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, X.; Zhang, Q.; Wang, Z.; Zhu, S. Application effects of remimazolam and propofol on elderly patients undergoing hip replacement. BMC Anesthesiol. 2022, 22, 118. [Google Scholar] [CrossRef]
- Guo, J.; Qian, Y.; Zhang, X.; Han, S.; Shi, Q.; Xu, J. Remimazolam tosilate compared with propofol for gastrointestinal endoscopy in elderly patients: A prospective, randomized and controlled study. BMC Anesthesiol. 2022, 22, 180. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Liu, T.; Zhang, Y.; Qi, D. Effect of remimazolam versus propofol sedation on the quality of recovery after colonoscopy: A randomised, controlled, noninferiority trial. Eur. J. Anaesthesiol. 2022, 39, 953–955. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, T.; Sento, Y.; Kamimura, Y.; Tsuji, T.; Kako, E.; Sobue, K. Remimazolam for induction of anesthesia in elderly patients with severe aortic stenosis: A prospective, observational pilot study. BMC Anesthesiol. 2021, 21, 306. [Google Scholar] [CrossRef] [PubMed]
- Sekiguchi, R.; Kinoshita, M.; Kawanishi, R.; Kakuta, N.; Sakai, Y.; Tanaka, K. Comparison of hemodynamics during induction of general anesthesia with remimazolam and target-controlled propofol in middle-aged and elderly patients: A single-center, randomized, controlled trial. BMC Anesthesiol. 2023, 23, 14. [Google Scholar] [CrossRef]
- Hino, H.; Matsuura, T.; Kihara, Y.; Tsujikawa, S.; Mori, T.; Nishikawa, K. Comparison between hemodynamic effects of propofol and thiopental during general anesthesia induction with remifentanil infusion: A double-blind, age-stratified, randomized study. J. Anesth. 2019, 33, 509–515. [Google Scholar] [CrossRef]
- Lu, K.; Wei, S.; Ling, W.; Wei, Y.; Ran, X.; Huang, H.; Wang, M.; Wei, N.; Liao, Y.; Qin, Z.; et al. Remimazolam versus propofol for deep sedation/anaesthesia in upper gastrointestinal endoscopy in elderly patients: A multicenter, randomized controlled trial. J. Clin. Pharm. Ther. 2022, 47, 2230–2236. [Google Scholar] [CrossRef]
- Gregory, A.; Stapelfeldt, W.H.; Khanna, A.K.; Smischney, N.J.; Boero, I.J.; Chen, Q.; Stevens, M.; Shaw, A.D. Intraoperative Hypotension Is Associated with Adverse Clinical Outcomes After Noncardiac Surgery. Anesth. Analg. 2021, 132, 1654–1665. [Google Scholar] [CrossRef]
- Choi, J.Y.; Lee, H.S.; Kim, J.Y.; Han, D.W.; Yang, J.Y.; Kim, M.J.; Song, Y. Comparison of remimazolam-based and propofol-based total intravenous anesthesia on postoperative quality of recovery: A randomized non-inferiority trial. J. Clin. Anesth. 2022, 82, 110955. [Google Scholar] [CrossRef]
- Schüttler, J.; Eisenried, A.; Lerch, M.; Fechner, J.; Jeleazcov, C.; Ihmsen, H. Pharmacokinetics and Pharmacodynamics of Remimazolam (CNS 7056) after Continuous Infusion in Healthy Male Volunteers: Part I. Pharmacokinetics and Clinical Pharmacodynamics. Anesthesiology 2020, 132, 636–651. [Google Scholar] [CrossRef]
- Stöhr, T.; Colin, P.J.; Ossig, J.; Pesic, M.; Borkett, K.; Winkle, P.; Struys, M.; Schippers, F. Pharmacokinetic properties of remimazolam in subjects with hepatic or renal impairment. Br. J. Anaesth. 2021, 127, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, T.W.; Bruhn, J.; Radulescu, L.; Andresen, C.; Shafer, T.J.; Cohane, C.; Shafer, S.L. Pharmacodynamic interaction between propofol and remifentanil regarding hypnosis, tolerance of laryngoscopy, bispectral index, and electroencephalographic approximate entropy. Anesthesiology 2004, 100, 1353–1372. [Google Scholar] [CrossRef] [PubMed]
- Kern, S.E.; Xie, G.; White, J.L.; Egan, T.D. A response surface analysis of propofol-remifentanil pharmacodynamic interaction in volunteers. Anesthesiology 2004, 100, 1373–1381. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Chen, M.; Gu, F.; Chen, J.; Zhang, W.; Huang, Z.; Zhu, D.; Song, J.; Fang, J.; Yu, W.; et al. Comparison of Remimazolam-Flumazenil versus Propofol for Rigid Bronchoscopy: A Prospective Randomized Controlled Trial. J. Clin. Med. 2022, 12, 257. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| P Group (n = 22) | R6 Group (n = 23) | R12 Group (n = 23) | |
|---|---|---|---|
| Age, years | 68 (65–82) | 73 (65–86) | 72 (65–81) |
| Gender (M/F) | 11/11 | 12/11 | 17/6 |
| Height, cm | 160.9 ± 8.8 | 160.0 ±9.0 | 160.7 ± 8.2 |
| Weight, kg | 62.0 ± 12.0 | 61.0 ± 12.8 | 61.5 ± 9.9 |
| Body mass index, kg/m2 | 23.9 ± 3.3 | 23.8 ± 4.2 | 23.7 ± 2.8 |
| ASA physical status, I/II | 4/18 | 6/17 | 9/14 |
| Type of surgery | |||
| Nasal | 8 (36) | 5 (23) | 7 (32) |
| Throat | 5 (32) | 8 (36) | 6 (27) |
| Urology | 7 (23) | 7 (32) | 8 (36) |
| Hepatobiliary | 1 (5) | 2 (9) | 1 (5) |
| Breast | 1 (5) | 1 (5) | 1 (5) |
| P Group (n = 22) | R6 Group (n = 23) | R12 Group (n = 23) | p-Value | |
|---|---|---|---|---|
| LoC time, s | 56.7 ± 15.5 † | 90.6 ± 13.7 *,‡ | 66.7 ± 18.5 † | <0.001 |
| LoC dose, mg/kg | 90.9 ± 16.0 | 12.2 ± 10.6 | 15.2 ± 5.1 | NA |
| Injection pain | 8 (36) | 0 (0) * | 0 (0) * | <0.001 |
| Total infused dose, mg/kg | 7.9 ± 2.6 | 0.9 ± 0.37 | 1.1 ± 0.4 | <0.001 |
| Total remifentanil dose, µg/kg | 7.6 ± 3.3 | 5.9 ± 4.0 | 6.8 ± 3.3 | 0.265 |
| Surgery time, min | 42.0 ± 23.6 | 32.8 ± 18.8 | 35.7 ± 21.6 | 0.342 |
| Anesthesia time, min | 77.0 ± 24.9 | 63.9 ± 19.0 | 77.2 ± 31.5 | 0.139 |
| Eye opening time, min | 10.0 ±3.1 | 13.0 ± 6.1 | 12.3 ± 4.2 | 0.095 |
| Extubation time, min | 11.0 ± 3.1 | 13.9 ± 5.9 | 13.2 ± 4.3 | 0.102 |
| Emergence cough, 0/1/2/3 | 6/12/3/1 | 8/11/2/2 | 7/8/2/6 | 0.684 |
| Fluid, mL | 304.5 ± 158.8 | 280.4 ± 138.8 | 279.5 ± 199.2 | 0.853 |
| Blood loss, mL | 187.5 ± 170.6 | 113.8 ± 85.8 | 112.9 ± 131.9 | 0.464 |
| P Group (n = 22) | R6 Group (n = 23) | R12 Group (n = 23) | p-Value | |
|---|---|---|---|---|
| MAP decrease, mmHg | 43.8 ± 13.8 | 39.2 ± 14.3 | 39.2 ± 13.5 | 0.443 |
| Vasoactive drugs, n | 12 | 4 * | 7 | 0.029 * |
| Ephedrine, n | 11 | 4 | 5 | |
| Phenylephrine, n | 0 | 0 | 0 | |
| Glycopyrrolate, n | 1 | 1 | 2 | |
| Atropine, n | 0 | 0 | 1 | |
| Dose of ephedrine, mg | 3 (0–6) | 0 (0–0) * | 0 (0–0) | 0.034 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, T.K.; Kwak, H.J.; Jung, W.S.; Choi, G.B.; Park, S.Y.; Kim, J.Y. Effects of Remimazolam Anesthesia with Two Induction Doses on Hemodynamics and Recovery Profile in Older Patients: Comparison with Propofol Anesthesia. J. Clin. Med. 2023, 12, 5285. https://doi.org/10.3390/jcm12165285
Kim TK, Kwak HJ, Jung WS, Choi GB, Park SY, Kim JY. Effects of Remimazolam Anesthesia with Two Induction Doses on Hemodynamics and Recovery Profile in Older Patients: Comparison with Propofol Anesthesia. Journal of Clinical Medicine. 2023; 12(16):5285. https://doi.org/10.3390/jcm12165285
Chicago/Turabian StyleKim, Tae Kwang, Hyun Jeong Kwak, Wol Seon Jung, Gyu Bin Choi, Sung Yong Park, and Jong Yeop Kim. 2023. "Effects of Remimazolam Anesthesia with Two Induction Doses on Hemodynamics and Recovery Profile in Older Patients: Comparison with Propofol Anesthesia" Journal of Clinical Medicine 12, no. 16: 5285. https://doi.org/10.3390/jcm12165285